Ageing with HIV

{kind=link}
{kind=link}
Abstract
:1. Introduction
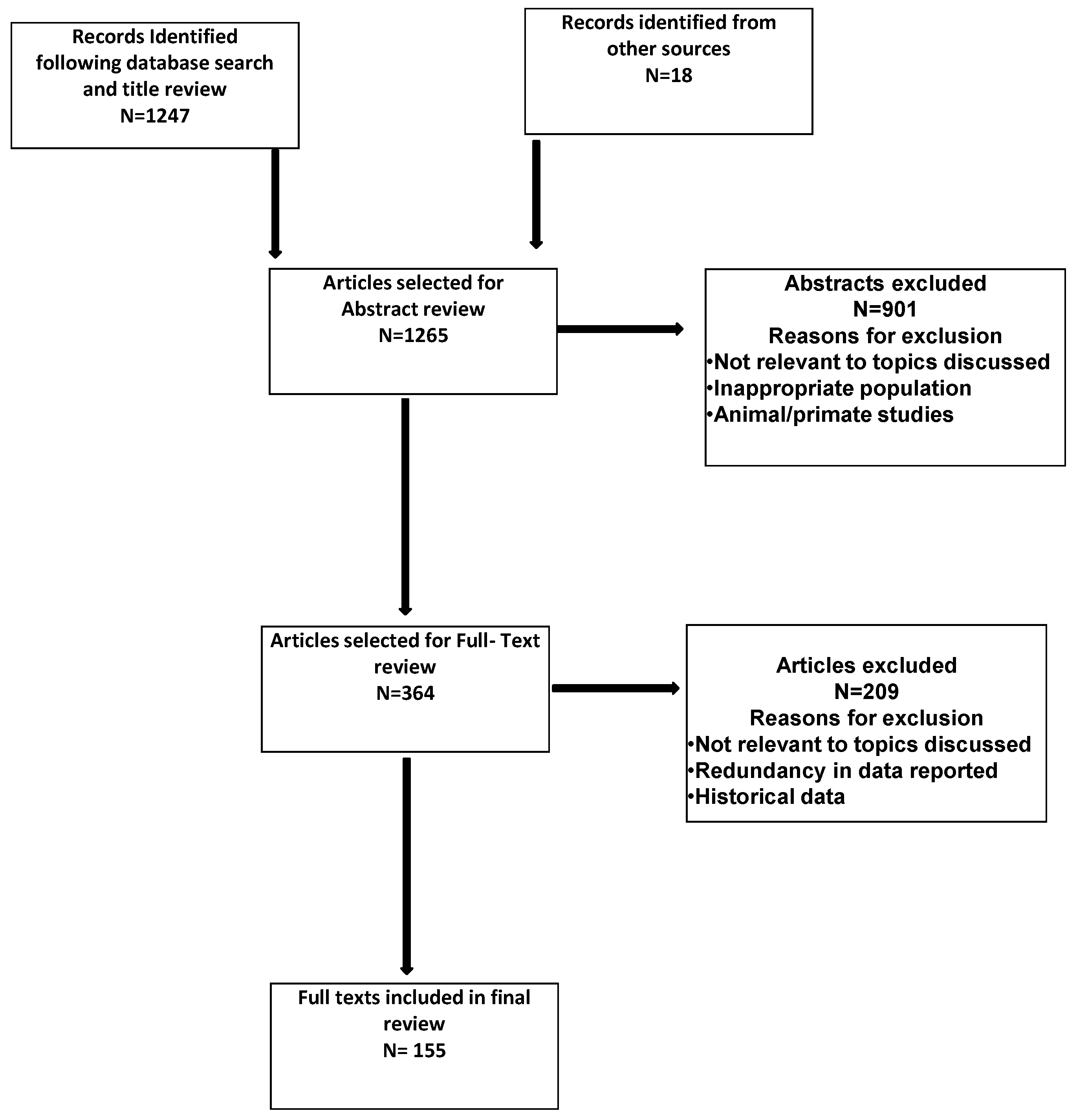
2. Methods
3. Results
4. Summary of Evidence
4.1. Cardiovascular Disease
4.2. Malignancy
4.3. Osteopenia/Osteoporosis
4.4. Cognitive Impairment
4.5. Frailty and Disability
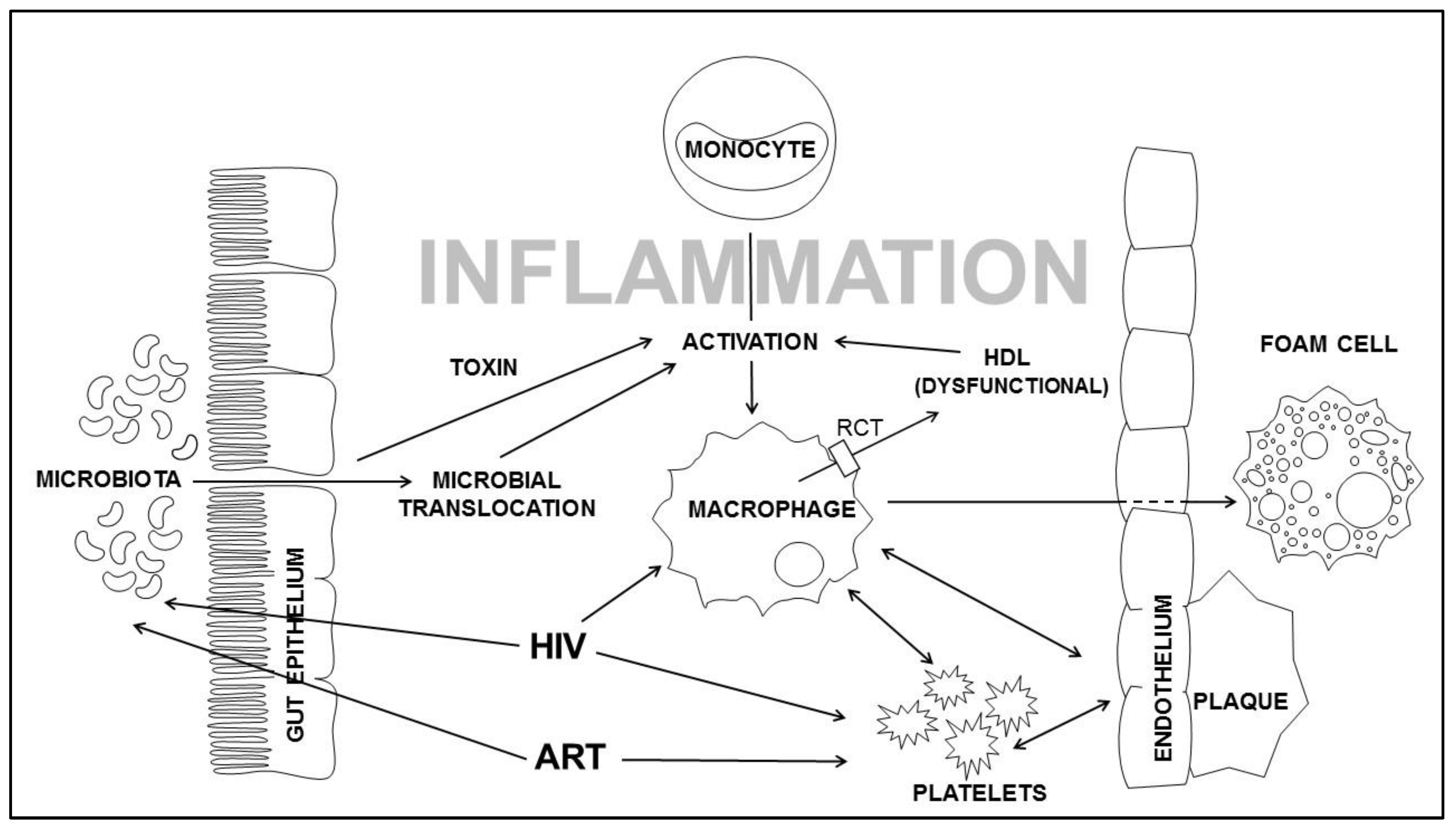
4.6. Chronic Inflammation and Non-AIDS Illnesses
4.7. Implications and Limitations of Current Body of Evidence
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Trickey, A.M.M.; Vehreschild, J.J.; Obel, N.; Gill, M.J.; Crane, H.M.; Boesecke, C.; Patterson, S.; Grabar, S.; Cazanave, C.; Cavassini, M.; et al. Survival of HIV-positive patients starting antiretroviral therapy between 1996 and 2013: A collaborative analysis of cohort studies. Lancet. HIV 2017, 4, e349–e356. [Google Scholar] [CrossRef]
- Deeks, S.G.; Lewin, S.R.; Havlir, D.V. The end of aids: Hiv infection as a chronic disease. Lancet 2013, 382, 1525–1533. [Google Scholar] [CrossRef]
- UNAIDS. HIV and Aging: A Special Supplement to the Unaids Report on the Global Aids Epidemic; Joint UN Programme on HIV/AIDS: Geneva, Switzerland, 2013. [Google Scholar]
- Mahy, M.; Autenrieth, C.S.; Stanecki, K.; Wynd, S. Increasing trends in HIV prevalence among people aged 50 years and older: Evidence from estimates and survey data. AIDS 2014, 28 (Suppl. 4), S453–S459. [Google Scholar] [CrossRef] [PubMed]
- Guaraldi, G.; Orlando, G.; Zona, S.; Menozzi, M.; Carli, F.; Garlassi, E.; Berti, A.; Rossi, E.; Roverato, A.; Palella, F. Premature age-related comorbidities among HIV-infected persons compared with the general population. Clin. Infect. Dis. 2011, 53, 1120–1126. [Google Scholar] [CrossRef] [PubMed]
- Martin-Iguacel, R.; Llibre, J.M.; Friis-Moller, N. Risk of cardiovascular disease in an aging HIV population: Where are we now? Current HIV/AIDS Rep. 2015, 12, 375–387. [Google Scholar] [CrossRef] [PubMed]
- Hanna, D.B.; Ramaswamy, C.; Kaplan, R.C.; Kizer, J.R.; Anastos, K.; Daskalakis, D.; Zimmerman, R.; Braunstein, S.L. Trends in cardiovascular disease mortality among persons with HIV in new york city, 2001–2012. Clin. Infect. Dis. 2016, 63, 1122–1129. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, M.J.; Bahiru, E.; Achenbach, C.; Longenecker, C.T.; Hsue, P.; So-Armah, K.; Freiberg, M.S.; Lloyd-Jones, D.M. Patterns of cardiovascular mortality for HIV-infected adults in the united states: 1999 to 2013. Am. J. Cardiol. 2016, 117, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.J.; Ryom, L.; Weber, R.; Morlat, P.; Pradier, C.; Reiss, P.; Kowalska, J.D.; de Wit, S.; Law, M.; el Sadr, W.; et al. Trends in underlying causes of death in people with HIV from 1999 to 2011 (d:A:D): A multicohort collaboration. Lancet 2014, 384, 241–248. [Google Scholar] [CrossRef]
- Smith, C.; Sabin, C.A.; Lundgren, J.D.; Thiebaut, R.; Weber, R.; Law, M.; Monforte, A.; Kirk, O.; Friis-Moller, N.; Phillips, A.; et al. Factors associated with specific causes of death amongst HIV-positive individuals in the d:A:D study. AIDS 2010, 24, 1537–1548. [Google Scholar] [PubMed]
- Mocroft, A.; Reiss, P.; Gasiorowski, J.; Ledergerber, B.; Kowalska, J.; Chiesi, A.; Gatell, J.; Rakhmanova, A.; Johnson, M.; Kirk, O.; et al. Serious fatal and nonfatal non-AIDS-defining illnesses in europe. J. Acquir. Immune Defic. Syndr. 2010, 55, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Friis-Moller, N.; Weber, R.; Reiss, P.; Thiebaut, R.; Kirk, O.; d’Arminio Monforte, A.; Pradier, C.; Morfeldt, L.; Mateu, S.; Law, M.; et al. Cardiovascular disease risk factors in HIV patients—Association with antiretroviral therapy: Results from the dad study. AIDS 2003, 17, 1179–1193. [Google Scholar] [CrossRef] [PubMed]
- Freiberg, M.S.; Chang, C.C.; Kuller, L.H.; Skanderson, M.; Lowy, E.; Kraemer, K.L.; Butt, A.A.; Bidwell Goetz, M.; Leaf, D.; Oursler, K.A.; et al. HIV infection and the risk of acute myocardial infarction. JAMA Intern. Med. 2013, 173, 614–622. [Google Scholar] [CrossRef] [PubMed]
- Paisible, A.L.; Chang, C.C.; So-Armah, K.A.; Butt, A.A.; Leaf, D.A.; Budoff, M.; Rimland, D.; Bedimo, R.; Goetz, M.B.; Rodriguez-Barradas, M.C.; et al. HIV infection, cardiovascular disease risk factor profile, and risk for acute myocardial infarction. J. Acquir. Immune Defic. Syndr. 2015, 68, 209–216. [Google Scholar] [CrossRef] [PubMed]
- El-Sadr, W.M.; Lundgren, J.; Neaton, J.D.; Gordin, F.; Abrams, D.; Arduino, R.C.; Babiker, A.; Burman, W.; Clumeck, N.; Cohen, C.J.; et al. Cd4+ count-guided interruption of antiretroviral treatment. N. Engl. J. Med. 2006, 355, 2283–2296. [Google Scholar] [PubMed]
- Nordell, A.D.; McKenna, M.; Borges, A.H.; Duprez, D.; Neuhaus, J.; Neaton, J.D. Severity of cardiovascular disease outcomes among patients with HIV is related to markers of inflammation and coagulation. J. Am. Heart Assoc. 2014, 3, e000844. [Google Scholar] [CrossRef] [PubMed]
- Duprez, D.A.; Neuhaus, J.; Kuller, L.H.; Tracy, R.; Belloso, W.; De Wit, S.; Drummond, F.; Lane, H.C.; Ledergerber, B.; Lundgren, J.; et al. Inflammation, coagulation and cardiovascular disease in HIV-infected individuals. PLoS ONE 2012, 7, e44454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subramanian, S.; Tawakol, A.; Burdo, T.H.; Abbara, S.; Wei, J.; Vijayakumar, J.; Corsini, E.; Abdelbaky, A.; Zanni, M.V.; Hoffmann, U.; et al. Arterial inflammation in patients with HIV. JAMA 2012, 308, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Zanni, M.V.; Abbara, S.; Lo, J.; Wai, B.; Hark, D.; Marmarelis, E.; Grinspoon, S.K. Increased coronary atherosclerotic plaque vulnerability by coronary computed tomography angiography in HIV-infected men. AIDS 2013, 27, 1263–1272. [Google Scholar] [CrossRef] [PubMed]
- Durand, M.; Sheehy, O.; Baril, J.G.; Lelorier, J.; Tremblay, C.L. Association between HIV infection, antiretroviral therapy, and risk of acute myocardial infarction: A cohort and nested case-control study using quebec’s public health insurance database. J. Acquir. Immune Defic. Syndr. 2011, 57, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Sabin, C.A.; Worm, S.W.; Weber, R.; Reiss, P.; El-Sadr, W.; Dabis, F.; De Wit, S.; Law, M.; D’Arminio Monforte, A.; Friis-Moller, N.; et al. Use of nucleoside reverse transcriptase inhibitors and risk of myocardial infarction in HIV-infected patients enrolled in the d:A:D study: A multi-cohort collaboration. Lancet 2008, 371, 1417–1426. [Google Scholar] [PubMed]
- Glesby, M.J. Cardiovascular complications of HIV infection. Top. Antivir. Med. 2017, 24, 127–131. [Google Scholar] [PubMed]
- Ding, X.; Andraca-Carrera, E.; Cooper, C.; Miele, P.; Kornegay, C.; Soukup, M.; Marcus, K.A. No association of abacavir use with myocardial infarction: Findings of an fda meta-analysis. J. Acquir. Immune Defic. Syndr. 2012, 61, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Ryom, L.; Boesecke, C.; Gisler, V.; Manzardo, C.; Rockstroh, J.K.; Puoti, M.; Furrer, H.; Miro, J.M.; Gatell, J.M.; Pozniak, A.; et al. Essentials from the 2015 european aids clinical society (EACS) guidelines for the treatment of adult HIV-positive persons. HIV Med. 2016, 17, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Panel on antiretroviral guidelines for adults and adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of health and human services. Available online: http://aidsinfo.Nih.Gov/contentfiles/lvguideline (accessed on 10 January 2018).
- Nguyen, A.; Calmy, A.; Delhumeau, C.; Mercier, I.; Cavassini, M.; Mello, A.F.; Elzi, L.; Rauch, A.; Bernasconi, E.; Schmid, P.; et al. A randomized cross-over study to compare raltegravir and efavirenz (switch-er study). AIDS 2011, 25, 1481–1487. [Google Scholar] [CrossRef] [PubMed]
- Tungsiripat, M.; Kitch, D.; Glesby, M.J.; Gupta, S.K.; Mellors, J.W.; Moran, L.; Jones, L.; Alston-Smith, B.; Rooney, J.F.; Aberg, J.A. A pilot study to determine the impact on dyslipidemia of adding tenofovir to stable background antiretroviral therapy: Actg 5206. AIDS 2010, 24, 1781–1784. [Google Scholar] [CrossRef] [PubMed]
- Worm, S.W.; Sabin, C.; Weber, R.; Reiss, P.; El-Sadr, W.; Dabis, F.; De Wit, S.; Law, M.; Monforte, A.D.A.; Friis-Møller, N.; et al. Risk of myocardial infarction in patients with HIV infection exposed to specific individual antiretroviral drugs from the 3 major drug classes: The data collection on adverse events of anti-HIV drugs (d:A:D) study. J. Infect. Dis. 2010, 201, 318–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DAD Study Group; Friis-Møller, N.; Reiss, P.; Sabin, C.A.; Weber, R.; Monforte, A.D.A.; El-Sadr, W.; Thiébaut, R.; De Wit, S.; Kirk, O.; et al. Class of antiretroviral drugs and the risk of myocardial infarction. N. Engl. J. Med. 2007, 356, 1723–1735. [Google Scholar]
- Brown, T.T.; Li, X.; Cole, S.R.; Kingsley, L.A.; Palella, F.J.; Riddler, S.A.; Chmiel, J.S.; Visscher, B.R.; Margolick, J.B.; Dobs, A.S. Cumulative exposure to nucleoside analogue reverse transcriptase inhibitors is associated with insulin resistance markers in the multicenter aids cohort study. AIDS 2005, 19, 1375–1383. [Google Scholar] [CrossRef] [PubMed]
- Islam, F.M.; Wu, J.; Jansson, J.; Wilson, D.P. Relative risk of cardiovascular disease among people living with HIV: A systematic review and meta-analysis. HIV Med. 2012, 13, 453–468. [Google Scholar] [CrossRef] [PubMed]
- Ryom, J.L.; Lundgren, J.D.; El-Sadr, W.M.; Reiss, P.; Phillips, A.; Kirk, O.; Weber, R.; Sabin, C.; Mocroft, A.; et al. Association between Cardiovascular Disease and Contemporarily Used Protease Inhibitors. In Proceedings of the Retroviruses and Opportunistic Infections, Seattle, WA, USA, 13–16 February 2017. [Google Scholar]
- Zanni, M.V.; Fitch, K.V.; Feldpausch, M.; Han, A.; Lee, H.; Lu, M.T.; Abbara, S.; Ribaudo, H.; Douglas, P.S.; Hoffmann, U.; et al. 2013 american college of cardiology/american heart association and 2004 adult treatment panel iii cholesterol guidelines applied to HIV-infected patients with/without subclinical high-risk coronary plaque. AIDS 2014, 28, 2061–2070. [Google Scholar] [CrossRef] [PubMed]
- Lo, J.; Lu, M.T.; Ihenachor, E.J.; Wei, J.; Looby, S.E.; Fitch, K.V.; Oh, J.; Zimmerman, C.O.; Hwang, J.; Abbara, S.; et al. Effects of statin therapy on coronary artery plaque volume and high-risk plaque morphology in HIV-infected patients with subclinical atherosclerosis: A randomised, double-blind, placebo-controlled trial. Lancet. HIV 2015, 2, e52–e63. [Google Scholar] [CrossRef]
- Aberg, J.A.; Sponseller, C.A.; Ward, D.J.; Kryzhanovski, V.A.; Campbell, S.E.; Thompson, M.A. Pitavastatin versus pravastatin in adults with HIV-1 infection and dyslipidaemia (intrepid): 12 week and 52 week results of a phase 4, multicentre, randomised, double-blind, superiority trial. Lancet. HIV 2017, 4, e284–e294. [Google Scholar] [CrossRef]
- Evaluating the use of pitavastatin to reduce the risk of cardiovascular disease in HIV-infected adults (reprieve). Available online: https://clinicaltrials.gov/ct2/show/NCT02344290 (accessed on 20 January 2018).
- Il-1beta inhibition significantly reduces atherosclerotic inflammation in treated HIV. Available online: http://www.croiconference.org/sessions/il-1%CE%B2-inhibition-significantly-reduces-atherosclerotic-inflammation-treated-hiv (accessed on 20 January 2018).
- Losina, E.; Hyle, E.P.; Borre, E.D.; Linas, B.P.; Sax, P.E.; Weinstein, M.C.; Rusu, C.; Ciaranello, A.L.; Walensky, R.P.; Freedberg, K.A. Projecting 10-yr, 20-yr and lifetime risks of cardiovascular disease in persons living with HIV in the us. Clin. Infect. Dis. 2017. [Google Scholar] [CrossRef] [PubMed]
- Grulich, A.E.; van Leeuwen, M.T.; Falster, M.O.; Vajdic, C.M. Incidence of cancers in people with HIV/aids compared with immunosuppressed transplant recipients: A meta-analysis. Lancet 2007, 370, 59–67. [Google Scholar] [CrossRef]
- Engels, E.A.; Brock, M.V.; Chen, J.; Hooker, C.M.; Gillison, M.; Moore, R.D. Elevated incidence of lung cancer among HIV-infected individuals. J. Clin. Oncol. 2006, 24, 1383–1388. [Google Scholar] [CrossRef] [PubMed]
- Antiretroviral Therapy Cohort Collaboration. Causes of death in HIV-1-infected patients treated with antiretroviral therapy, 1996–2006: Collaborative analysis of 13 HIV cohort studies. Clin. Infect. Dis. 2010, 50, 1387–1396. [Google Scholar]
- Lewden, C.; May, T.; Rosenthal, E.; Burty, C.; Bonnet, F.; Costagliola, D.; Jougla, E.; Semaille, C.; Morlat, P.; Salmon, D.; et al. Changes in causes of death among adults infected by HIV between 2000 and 2005: The "mortalite 2000 and 2005" surveys (anrs en19 and mortavic). J. Acquir. Immune Defic. Syndr. 2008, 48, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Brock, M.V.; Hooker, C.M.; Engels, E.A.; Moore, R.D.; Gillison, M.L.; Alberg, A.J.; Keruly, J.C.; Yang, S.C.; Heitmiller, R.F.; Baylin, S.B.; et al. Delayed diagnosis and elevated mortality in an urban population with HIV and lung cancer: Implications for patient care. J. Acquir. Immune Defic. Syndr. 2006, 43, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Glaser, S.L.; Clarke, C.A.; Gulley, M.L.; Craig, F.E.; DiGiuseppe, J.A.; Dorfman, R.F.; Mann, R.B.; Ambinder, R.F. Population-based patterns of human immunodeficiency virus-related hodgkin lymphoma in the greater san francisco bay area, 1988–1998. Cancer 2003, 98, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Engels, E.A.; Pfeiffer, R.M.; Goedert, J.J.; Virgo, P.; McNeel, T.S.; Scoppa, S.M.; Biggar, R.J. Trends in cancer risk among people with aids in the united states 1980–2002. AIDS 2006, 20, 1645–1654. [Google Scholar] [CrossRef] [PubMed]
- Burgi, A.; Brodine, S.; Wegner, S.; Milazzo, M.; Wallace, M.R.; Spooner, K.; Blazes, D.L.; Agan, B.K.; Armstrong, A.; Fraser, S.; et al. Incidence and risk factors for the occurrence of non-aids-defining cancers among human immunodeficiency virus-infected individuals. Cancer 2005, 104, 1505–1511. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.M.; Polesel, J.; Rickenbach, M.; Dal Maso, L.; Keiser, O.; Kofler, A.; Rapiti, E.; Levi, F.; Jundt, G.; Fisch, T.; et al. Cancer risk in the swiss HIV cohort study: Associations with immunodeficiency, smoking, and highly active antiretroviral therapy. J. National Cancer Institute 2005, 97, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Piketty, C.; Selinger-Leneman, H.; Bouvier, A.M.; Belot, A.; Mary-Krause, M.; Duvivier, C.; Bonmarchand, M.; Abramowitz, L.; Costagliola, D.; Grabar, S. Incidence of HIV-related anal cancer remains increased despite long-term combined antiretroviral treatment: Results from the french hospital database on HIV. J. Clin. Oncol. 2012, 30, 4360–4366. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.; Leyden, W.A.; Xu, L.; Horberg, M.A.; Klein, D.; Towner, W.J.; Quesenberry, C.P., Jr.; Abrams, D.I.; Silverberg, M.J. Exposure to antiretroviral therapy and risk of cancer in HIV-infected persons. AIDS 2012, 26, 2223–2231. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Robinson, D.; Stebbing, J.; Shamash, J.; Nelson, M.; Gazzard, B.; Mandelia, S.; Møller, H.; Bower, M. Highly active antiretroviral therapy and the incidence of non–aids-defining cancers in people with HIV infection. J. Clin. Oncol. 2009, 27, 884–890. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, P.G.; Aboulafia, D.M.; Zloza, A. Malignancies in HIV/aids: From epidemiology to therapeutic challenges. AIDS 2014, 28, 453–465. [Google Scholar] [CrossRef] [PubMed]
- Cutrell, J.; Bedimo, R. Non-aids-defining cancers among HIV-infected patients. Curr. HIV/AIDS Rep. 2013, 10, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Borges, A.H.; Silverberg, M.J.; Wentworth, D.; Grulich, A.E.; Fatkenheuer, G.; Mitsuyasu, R.; Tambussi, G.; Sabin, C.A.; Neaton, J.D.; Lundgren, J.D. Predicting risk of cancer during HIV infection: The role of inflammatory and coagulation biomarkers. AIDS 2013, 27, 1433–1441. [Google Scholar] [CrossRef] [PubMed]
- Vendrame, E.; Hussain, S.K.; Breen, E.C.; Magpantay, L.I.; Widney, D.P.; Jacobson, L.P.; Variakojis, D.; Knowlton, E.R.; Bream, J.H.; Ambinder, R.F.; et al. Serum levels of cytokines and biomarkers for inflammation and immune activation, and HIV-associated non-hodgkin b-cell lymphoma risk. Cancer Epidemiol. Biomark. Prev. 2014, 23, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Bedimo, R.J.; McGinnis, K.A.; Dunlap, M.; Rodriguez-Barradas, M.C.; Justice, A.C. Incidence of non-aids-defining malignancies in HIV-infected versus noninfected patients in the haart era: Impact of immunosuppression. J. Acquir. Immune Defic. Syndr. 2009, 52, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Shiels, M.S.; Cole, S.R.; Kirk, G.D.; Poole, C. A meta-analysis of the incidence of non-aids cancers in HIV-infected individuals. J. Acquir. Immune Defic. Syndr. 2009, 52, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Hanson, D.L.; Sullivan, P.S.; Novak, R.M.; Moorman, A.C.; Tong, T.C.; Holmberg, S.D.; Brooks, J.T. Incidence of types of cancer among HIV-infected persons compared with the general population in the united states, 1992–2003. Ann. Intern. Med. 2008, 148, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Schacker, T.W.; Nguyen, P.L.; Martinez, E.; Reilly, C.; Gatell, J.M.; Horban, A.; Bakowska, E.; Berzins, B.; van Leeuwen, R.; Wolinsky, S.; et al. Persistent abnormalities in lymphoid tissues of human immunodeficiency virus–infected patients successfully treated with highly active antiretroviral therapy. J. Infect. Dis. 2002, 186, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Fausto, A.; Bongiovanni, M.; Cicconi, P.; Menicagli, L.; Ligabo, E.V.; Melzi, S.; Bini, T.; Sardanelli, F.; Cornalba, G.; Monforte, A. Potential predictive factors of osteoporosis in HIV-positive subjects. Bone 2006, 38, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Grund, B.; Peng, G.; Gibert, C.L.; Hoy, J.F.; Isaksson, R.L.; Shlay, J.C.; Martinez, E.; Reiss, P.; Visnegarwala, F.; Carr, A.D. Continuous antiretroviral therapy decreases bone mineral density. AIDS 2009, 23, 1519–1529. [Google Scholar] [CrossRef] [PubMed]
- Knobel, H.; Guelar, A.; Vallecillo, G.; Nogues, X.; Diez, A. Osteopenia in HIV-infected patients: Is it the disease or is it the treatment? AIDS 2001, 15, 807–808. [Google Scholar] [CrossRef] [PubMed]
- Arnsten, J.H.; Freeman, R.; Howard, A.A.; Floris-Moore, M.; Lo, Y.; Klein, R.S. Decreased bone mineral density and increased fracture risk in aging men with or at risk for HIV infection. AIDS 2007, 21, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Triant, V.A.; Brown, T.T.; Lee, H.; Grinspoon, S.K. Fracture prevalence among human immunodeficiency virus (HIV)-infected versus non-HIV-infected patients in a large u.S. Healthcare system. J. Clin. Endocrinol. Metab. 2008, 93, 3499–3504. [Google Scholar] [CrossRef] [PubMed]
- Prieto-Alhambra, D.; Guerri-Fernandez, R.; De Vries, F.; Lalmohamed, A.; Bazelier, M.; Starup-Linde, J.; Diez-Perez, A.; Cooper, C.; Vestergaard, P. Hiv infection and its association with an excess risk of clinical fractures: A nationwide case-control study. J. Acquir. Immune Defic. Syndr. 2014, 66, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Shiau, S.; Broun, E.C.; Arpadi, S.M.; Yin, M.T. Incident fractures in HIV-infected individuals: A systematic review and meta-analysis. AIDS 2013, 27, 1949–1957. [Google Scholar] [CrossRef] [PubMed]
- Guerri-Fernandez, R.; Vestergaard, P.; Carbonell, C.; Knobel, H.; Aviles, F.F.; Castro, A.S.; Nogues, X.; Prieto-Alhambra, D.; Diez-Perez, A. Hiv infection is strongly associated with hip fracture risk, independently of age, gender, and comorbidities: A population-based cohort study. J. Bone Miner. Res. 2013, 28, 1259–1263. [Google Scholar] [CrossRef] [PubMed]
- Cotter, A.G.; Sabin, C.A.; Simelane, S.; Macken, A.; Kavanagh, E.; Brady, J.J.; McCarthy, G.; Compston, J.; Mallon, P.W. Relative contribution of HIV infection, demographics and body mass index to bone mineral density. AIDS 2014, 28, 2051–2060. [Google Scholar] [CrossRef] [PubMed]
- Duvivier, C.; Kolta, S.; Assoumou, L.; Ghosn, J.; Rozenberg, S.; Murphy, R.L.; Katlama, C.; Costagliola, D. Greater decrease in bone mineral density with protease inhibitor regimens compared with nonnucleoside reverse transcriptase inhibitor regimens in HIV-1 infected naive patients. AIDS 2009, 23, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.T.; Qaqish, R.B. Antiretroviral therapy and the prevalence of osteopenia and osteoporosis: A meta-analytic review. AIDS 2006, 20, 2165–2174. [Google Scholar] [CrossRef] [PubMed]
- Compston, J. Hiv infection and osteoporosis. BoneKEy Rep. 2015, 4, 636. [Google Scholar] [CrossRef] [PubMed]
- Stellbrink, H.J.; Orkin, C.; Arribas, J.R.; Compston, J.; Gerstoft, J.; Van Wijngaerden, E.; Lazzarin, A.; Rizzardini, G.; Sprenger, H.G.; Lambert, J.; et al. Comparison of changes in bone density and turnover with abacavir-lamivudine versus tenofovir-emtricitabine in HIV-infected adults: 48-week results from the assert study. Clin. Infect. Dis. 2010, 51, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Nolan, D.; Upton, R.; McKinnon, E.; John, M.; James, I.; Adler, B.; Roff, G.; Vasikaran, S.; Mallal, S. Stable or increasing bone mineral density in HIV-infected patients treated with nelfinavir or indinavir. AIDS 2001, 15, 1275–1280. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Rivera, J.; Garcia, R.; Lozano, F.; Macias, J.; Garcia-Garcia, J.A.; Mira, J.A.; Corzo, J.E.; Gomez-Mateos, J.; Rueda, A.; Sanchez-Burson, J.; et al. Relationship between low bone mineral density and highly active antiretroviral therapy including protease inhibitors in HIV-infected patients. HIV Clin. Trials 2003, 4, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Bolland, M.J.; Grey, A.B.; Horne, A.M.; Briggs, S.E.; Thomas, M.G.; Ellis-Pegler, R.B.; Woodhouse, A.F.; Gamble, G.D.; Reid, I.R. Bone mineral density is not reduced in HIV-infected caucasian men treated with highly active antiretroviral therapy. Clin. Endocrinol. 2006, 65, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Dolan, S.E.; Kanter, J.R.; Grinspoon, S. Longitudinal analysis of bone density in human immunodeficiency virus-infected women. J. Clin. Endocrinol. Metab. 2006, 91, 2938–2945. [Google Scholar] [CrossRef] [PubMed]
- Bolland, M.J.; Wang, T.K.; Grey, A.; Gamble, G.D.; Reid, I.R. Stable bone density in haart-treated individuals with HIV: A meta-analysis. J. Clin. Endocrinol. Metab. 2011, 96, 2721–2731. [Google Scholar] [CrossRef] [PubMed]
- Bloch, M.; Tong, W.W.Y.; Hoy, J.; Baker, D.; Lee, F.J.; Richardson, R.; Carr, A.; TROP (Switch from Tenofovir to Raltegravir for Low Bone Density) study team. Switch from tenofovir to raltegravir increases low bone mineral density and decreases markers of bone turnover over 48 weeks. HIV Med. 2014, 15, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Cotter, A.G.; Vrouenraets, S.M.E.; Brady, J.J.; Wit, F.W.; Fux, C.A.; Furrer, H.; Brinkman, K.; Sabin, C.A.; Reiss, P.; Mallon, P.W.G.; et al. Impact of switching from zidovudine to tenofovir disoproxil fumarate on bone mineral density and markers of bone metabolism in virologically suppressed HIV-1 infected patients; a substudy of the prepare study. J. Clin. Endocrinol. Metab. 2013, 98, 1659–1666. [Google Scholar] [CrossRef] [PubMed]
- Negredo, E.; Diez-Perez, A.; Bonjoch, A.; Domingo, P.; Perez-Alvarez, N.; Gutierrez, M.; Mateo, G.; Puig, J.; Echeverria, P.; Escrig, R.; et al. Switching from tenofovir to abacavir in HIV-1-infected patients with low bone mineral density: Changes in bone turnover markers and circulating sclerostin levels. J. Antimicrob. Chemother. 2015, 70, 2104–2107. [Google Scholar] [CrossRef] [PubMed]
- Negredo, E.; Domingo, P.; Pérez-Álvarez, N.; Gutiérrez, M.; Mateo, G.; Puig, J.; Escrig, R.; Echeverría, P.; Bonjoch, A.; Clotet, B. Improvement in bone mineral density after switching from tenofovir to abacavir in HIV-1-infected patients with low bone mineral density: Two-centre randomized pilot study (osteotdf study). J. Antimicrob. Chemother. 2014, 69, 3368–3371. [Google Scholar] [CrossRef] [PubMed]
- Haskelberg, H.; Mallon, P.W.G.; Hoy, J.; Amin, J.; Moore, C.; Phanuphak, P.; Ferret, S.; Belloso, W.H.; Boyd, M.A.; Cooper, D.A.; et al. Bone mineral density over 96 weeks in adults failing first-line therapy randomized to raltegravir/lopinavir/ritonavir compared with standard second-line therapy. JAIDS 2014, 67, 161–168. [Google Scholar] [CrossRef] [PubMed]
- McComsey, G.A.; Kitch, D.; Daar, E.S.; Tierney, C.; Jahed, N.C.; Tebas, P.; Myers, L.; Melbourne, K.; Ha, B.; Sax, P.E. Bone mineral density and fractures in antiretroviral-naive persons randomized to receive abacavir-lamivudine or tenofovir disoproxil fumarate-emtricitabine along with efavirenz or atazanavir-ritonavir: Aids clinical trials group a5224s, a substudy of actg a5202. J. Infect. Dis. 2011, 203, 1791–1801. [Google Scholar] [PubMed]
- Haskelberg, H.; Hoy, J.F.; Amin, J.; Ebeling, P.R.; Emery, S.; Carr, A.; STEAL Study Group. Changes in bone turnover and bone loss in HIV-infected patients changing treatment to tenofovir-emtricitabine or abacavir-lamivudine. PLoS ONE 2012, 7, e38377. [Google Scholar] [CrossRef] [PubMed]
- Assoumou, L.; Katlama, C.; Viard, J.P.; Bentata, M.; Simon, A.; Roux, C.; Kolta, S.; Costagliola, D.; Rozenberg, S. Changes in bone mineral density over a 2-year period in HIV-1-infected men under combined antiretroviral therapy with osteopenia. AIDS 2013, 27, 2425–2430. [Google Scholar] [CrossRef] [PubMed]
- Arribas, J.R.; Thompson, M.; Sax, P.E.; Haas, B.; McDonald, C.; Wohl, D.A.; DeJesus, E.; Clarke, A.E.; Guo, S.; Wang, H.; et al. Brief report: Randomized, double-blind comparison of tenofovir alafenamide (taf) vs tenofovir disoproxil fumarate (tdf), each coformulated with elvitegravir, cobicistat, and emtricitabine (e/c/f) for initial HIV-1 treatment: Week 144 results. J. Acquir. Immune Defic. Syndr. 2017, 75, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Cotter, A.G.; Mallon, P.W. Hiv infection and bone disease: Implications for an aging population. Sex. Health 2011, 8, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.; Rieder, M.J. Interventions for the treatment of decreased bone mineral density associated with HIV infection. Cochrane Database Syst. Rev. 2007, Cd005645. [Google Scholar] [CrossRef] [PubMed]
- Cotter, A.G.; Mallon, P.W. Therapeutic options for low bone mineral density in HIV-infected subjects. Curr. HIV/AIDS Rep. 2012, 9, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Ofotokun, I.; Titanji, K.; Lahiri, C.D.; Vunnava, A.; Foster, A.; Sanford, S.E.; Sheth, A.N.; Lennox, J.L.; Knezevic, A.; Ward, L.; et al. A single-dose zoledronic acid infusion prevents antiretroviral therapy-induced bone loss in treatment-naive HIV-infected patients: A phase iib trial. Clin. Infect. Dis. 2016, 63, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Mallon, P. Alendronate for prevention of antiretroviral therapy-associated bone loss (apart). Available online: https://clinicaltrials.gov/ct2/show/NCT02322099 (accessed on 7 March 2017).
- Navia, B.A.; Jordan, B.D.; Price, R.W. The aids dementia complex: I. Clinical features. Ann. Neurol. 1986, 19, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Snider, W.D.; Simpson, D.M.; Nielsen, S.; Gold, J.W.; Metroka, C.E.; Posner, J.B. Neurological complications of acquired immune deficiency syndrome: Analysis of 50 patients. Ann. Neurol. 1983, 14, 403–418. [Google Scholar] [CrossRef] [PubMed]
- Heaton, R.K.; Franklin, D.R.; Ellis, R.J.; McCutchan, J.A.; Letendre, S.L.; Leblanc, S.; Corkran, S.H.; Duarte, N.A.; Clifford, D.B.; Woods, S.P.; et al. Hiv-associated neurocognitive disorders before and during the era of combination antiretroviral therapy: Differences in rates, nature, and predictors. J. Neurovirol. 2011, 17, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Clifford, K.M.; Samboju, V.; Cobigo, Y.; Milanini, B.; Marx, G.A.; Hellmuth, J.M.; Rosen, H.J.; Kramer, J.H.; Allen, I.E.; Valcour, V.G. Progressive brain atrophy despite persistent viral suppression in HIV over age 60. J. Acquir. Immune Defic. Syndr. 2017, 76, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Saylor, D.; Dickens, A.M.; Sacktor, N.; Haughey, N.; Slusher, B.; Pletnikov, M.; Mankowski, J.L.; Brown, A.; Volsky, D.J.; McArthur, J.C. Hiv-associated neurocognitive disorder—Pathogenesis and prospects for treatment. Nat. Rev. Neurol. 2016, 12, 234–248. [Google Scholar] [CrossRef] [PubMed]
- Valcour, V.; Shikuma, C.; Shiramizu, B.; Watters, M.; Poff, P.; Selnes, O.; Holck, P.; Grove, J.; Sacktor, N. Higher frequency of dementia in older HIV-1 individuals: The hawaii aging with HIV-1 cohort. Neurology 2004, 63, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Joska, J.A.; Westgarth-Taylor, J.; Myer, L.; Hoare, J.; Thomas, K.G.; Combrinck, M.; Paul, R.H.; Stein, D.J.; Flisher, A.J. Characterization of HIV-associated neurocognitive disorders among individuals starting antiretroviral therapy in south africa. AIDS Behav. 2011, 15, 1197–1203. [Google Scholar] [CrossRef] [PubMed]
- Simioni, S.; Cavassini, M.; Annoni, J.-M.; Rimbault Abraham, A.; Bourquin, I.; Schiffer, V.; Calmy, A.; Chave, J.-P.; Giacobini, E.; Hirschel, B.; et al. Cognitive dysfunction in HIV patients despite long-standing suppression of viremia. AIDS 2010, 10, 1243–1250. [Google Scholar] [CrossRef] [PubMed]
- Gisslen, M.; Price, R.W.; Nilsson, S. The definition of HIV-associated neurocognitive disorders: Are we overestimating the real prevalence? BMC Infect. Dis. 2011, 11, 356. [Google Scholar] [CrossRef] [PubMed]
- Underwood, J.; De Francesco, D.; Post, F.A.; Vera, J.H.; Williams, I.; Boffito, M.; Mallon, P.W.; Anderson, J.; Sachikonye, M.; Sabin, C.; et al. Associations between cognitive impairment and patient-reported measures of physical/mental functioning in older people living with HIV. HIV Med. 2017, 18, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Grant, I.; Franklin, D.R., Jr.; Deutsch, R.; Woods, S.P.; Vaida, F.; Ellis, R.J.; Letendre, S.L.; Marcotte, T.D.; Atkinson, J.H.; Collier, A.C.; et al. Asymptomatic HIV-associated neurocognitive impairment increases risk for symptomatic decline. Neurology 2014, 82, 2055–2062. [Google Scholar] [CrossRef] [PubMed]
- Robertson, K.R.; Smurzynski, M.; Parsons, T.D.; Wu, K.; Bosch, R.J.; Wu, J.; McArthur, J.C.; Collier, A.C.; Evans, S.R.; Ellis, R.J. The prevalence and incidence of neurocognitive impairment in the haart era. AIDS 2007, 21, 1915–1921. [Google Scholar] [CrossRef] [PubMed]
- Eden, A.; Price, R.W.; Spudich, S.; Fuchs, D.; Hagberg, L.; Gisslen, M. Immune activation of the central nervous system is still present after >4 years of effective highly active antiretroviral therapy. J. Infect. Dis. 2007, 196, 1779–1783. [Google Scholar] [CrossRef] [PubMed]
- Anthony, I.C.; Ramage, S.N.; Carnie, F.W.; Simmonds, P.; Bell, J.E. Influence of haart on HIV-related cns disease and neuroinflammation. J. Neuropathol. Exp. Neurol. 2005, 64, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Vaida, F.; Wong, J.; Sanders, C.A.; Kao, Y.T.; Croteau, D.; Clifford, D.B.; Collier, A.C.; Gelman, B.B.; Marra, C.M.; et al. Long-term efavirenz use is associated with worse neurocognitive functioning in HIV-infected patients. J. Neurovirol. 2016, 22, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Robertson, K.; Liner, J.; Meeker, R.B. Antiretroviral neurotoxicity. J. Neurovirol. 2012, 18, 388–399. [Google Scholar] [CrossRef] [PubMed]
- Ancuta, P.; Kamat, A.; Kunstman, K.J.; Kim, E.Y.; Autissier, P.; Wurcel, A.; Zaman, T.; Stone, D.; Mefford, M.; Morgello, S.; et al. Microbial translocation is associated with increased monocyte activation and dementia in aids patients. PLoS ONE 2008, 3, e2516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaul, M.; Garden, G.A.; Lipton, S.A. Pathways to neuronal injury and apoptosis in HIV-associated dementia. Nature 2001, 410, 988–994. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.; Westmoreland, S.; Greco, J.; Ratai, E.; Lentz, M.; Kim, W.-K.; Fuller, R.A.; Kim, J.P.; Autissier, P.; Sehgal, P.K.; et al. Magnetic resonance spectroscopy reveals that activated monocytes contribute to neuronal injury in siv neuroaids. J. Clin. Investig. 2005, 115, 2534–2545. [Google Scholar] [CrossRef] [PubMed]
- Ellis, R.J.; Badiee, J.; Vaida, F.; Letendre, S.; Heaton, R.K.; Clifford, D.; Collier, A.C.; Gelman, B.; McArthur, J.; Morgello, S.; et al. Cd4 nadir is a predictor of HIV neurocognitive impairment in the era of combination antiretroviral therapy. AIDS 2011, 25, 1747–1751. [Google Scholar] [CrossRef] [PubMed]
- Molsberry, S.A.; Lecci, F.; Kingsley, L.; Junker, B.; Reynolds, S.; Goodkin, K.; Levine, A.J.; Martin, E.; Miller, E.N.; Munro, C.A.; et al. Mixed membership trajectory models of cognitive impairment in the multicenter aids cohort study. AIDS 2015, 29, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Brothers, T.D.; Kirkland, S.; Guaraldi, G.; Falutz, J.; Theou, O.; Johnston, B.L.; Rockwood, K. Frailty in people aging with human immunodeficiency virus (HIV) infection. J. Infect. Dis. 2014, 210, 1170–1179. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Rothman, M.D.; Leo-Summers, L.; Gill, T.M. Prognostic significance of potential frailty criteria. J. Am. Geriatr. Soc. 2008, 56, 2211–2216. [Google Scholar] [CrossRef] [PubMed]
- Onen, N.F.; Overton, E.T. A review of premature frailty in HIV-infected persons; another manifestation of HIV-related accelerated aging. Curr. Aging sci. 2011, 4, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Desquilbet, L.; Jacobson, L.P.; Fried, L.P.; Phair, J.P.; Jamieson, B.D.; Holloway, M.; Margolick, J.B. Hiv-1 infection is associated with an earlier occurrence of a phenotype related to frailty. J. Gerontol. 2007, 62, 1279–1286. [Google Scholar] [CrossRef]
- Althoff, K.N.; Jacobson, L.P.; Cranston, R.D.; Detels, R.; Phair, J.P.; Li, X.; Margolick, J.B. Age, comorbidities, and aids predict a frailty phenotype in men who have sex with men. J. Gerontol. 2014, 69, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Desquilbet, L.; Jacobson, L.P.; Fried, L.P.; Phair, J.P.; Jamieson, B.D.; Holloway, M.; Margolick, J.B. A frailty-related phenotype before haart initiation as an independent risk factor for aids or death after haart among HIV-infected men. J. Gerontol. 2011, 66, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Onen, N.F.; Agbebi, A.; Shacham, E.; Stamm, K.E.; Onen, A.R.; Overton, E.T. Frailty among HIV-infected persons in an urban outpatient care setting. J. Infect. 2009, 59, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Ianas, V.; Berg, E.; Mohler, M.J.; Wendel, C.; Klotz, S.A. Antiretroviral therapy protects against frailty in HIV-1 infection. J. Int. Assoc. Provid. AIDS Care 2013, 12, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Pathai, S.; Gilbert, C.; Weiss, H.A.; Cook, C.; Wood, R.; Bekker, L.G.; Lawn, S.D. Frailty in HIV-infected adults in south africa. J. Acquir. Immune Defic. Syndr. 2013, 62, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Terzian, A.S.; Holman, S.; Nathwani, N.; Robison, E.; Weber, K.; Young, M.; Greenblatt, R.M.; Gange, S.J. Factors associated with preclinical disability and frailty among HIV-infected and HIV-uninfected women in the era of cart. J. Women’s Health 2009, 18, 1965–1974. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.E.; Iudicello, J.E.; Weber, E.; Duarte, N.A.; Riggs, P.K.; Delano-Wood, L.; Ellis, R.; Grant, I.; Woods, S.P. Synergistic effects of HIV infection and older age on daily functioning. J. Acquir. Immune Defic. Syndr. 2012, 61, 341–348. [Google Scholar] [CrossRef] [PubMed]
- John, M.D.; Greene, M.; Hessol, N.A.; Zepf, R.; Parrott, A.H.; Foreman, C.; Bourgeois, J.; Gandhi, M.; Hare, C.B. Geriatric assessments and association with vacs index among HIV-infected older adults in san francisco. J. Acquir. Immune Defic. Syndr. 2016, 72, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Avila-Funes, J.A.; Belaunzaran-Zamudio, P.F.; Tamez-Rivera, O.; Crabtree-Ramirez, B.; Navarrete-Reyes, A.P.; Cuellar-Rodriguez, J.; Sierra-Madero, J.; Amieva, H. Correlates of prevalent disability among HIV-infected elderly patients. AIDS Res. Hum. Retroviruses 2016, 32, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Heaton, R.K.; Marcotte, T.D.; Mindt, M.R.; Sadek, J.; Moore, D.J.; Bentley, H.; McCutchan, J.A.; Reicks, C.; Grant, I. The impact of HIV-associated neuropsychological impairment on everyday functioning. JINS 2004, 10, 317–331. [Google Scholar] [CrossRef] [PubMed]
- Heaton, R.K.; Velin, R.A.; McCutchan, J.A.; Gulevich, S.J.; Atkinson, J.H.; Wallace, M.R.; Godfrey, H.P.; Kirson, D.A.; Grant, I. Neuropsychological impairment in human immunodeficiency virus-infection: Implications for employment. Hnrc group. Hiv neurobehavioral research center. Psychosom. Med. 1994, 56, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Erlandson, K.M.; Allshouse, A.A.; Jankowski, C.M.; Duong, S.; MaWhinney, S.; Kohrt, W.M.; Campbell, T.B. Risk factors for falls in HIV-infected persons. J. Acquir. Immune Defic. Syndr. 2012, 61, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Petoumenos, K.; Worm, S.; Reiss, P.; de Wit, S.; d’Arminio Monforte, A.; Sabin, C.; Friis-Moller, N.; Weber, R.; Mercie, P.; Pradier, C.; et al. Rates of cardiovascular disease following smoking cessation in patients with HIV infection: Results from the d:A:D study(*). HIV Med. 2011, 12, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Kuller, L.H.; Tracy, R.; Belloso, W.; De Wit, S.; Drummond, F.; Lane, H.C.; Ledergerber, B.; Lundgren, J.; Neuhaus, J.; Nixon, D.; et al. Inflammatory and coagulation biomarkers and mortality in patients with HIV infection. PLoS Med. 2008, 5, e203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahrami, H.; Budoff, M.; Haberlen, S.A.; Rezaeian, P.; Ketlogetswe, K.; Tracy, R.; Palella, F.; Witt, M.D.; McConnell, M.V.; Kingsley, L.; et al. Inflammatory markers associated with subclinical coronary artery disease: The multicenter aids cohort study. J. Am. Heart Assoc. 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Greenwald, J.H.; Richterman, A.G.; Rupert, A.; Dutcher, L.; Badralmaa, Y.; Natarajan, V.; Rehm, C.; Hadigan, C.; Sereti, I. Traditional risk factors and d-dimer predict incident cardiovascular disease events in chronic HIV infection. AIDS 2010, 24, 1509–1517. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Villar, S.; Sainz, T.; Lee, S.A.; Hunt, P.W.; Sinclair, E.; Shacklett, B.L.; Ferre, A.L.; Hayes, T.L.; Somsouk, M.; Hsue, P.Y.; et al. Hiv-infected individuals with low cd4/cd8 ratio despite effective antiretroviral therapy exhibit altered t cell subsets, heightened cd8+ t cell activation, and increased risk of non-aids morbidity and mortality. PLoS Pathog. 2014, 10, e1004078. [Google Scholar] [CrossRef] [PubMed]
- So-Armah, K.A.; Tate, J.P.; Chang, C.H.; Butt, A.A.; Gerschenson, M.; Gibert, C.L.; Leaf, D.; Rimland, D.; Rodriguez-Barradas, M.C.; Budoff, M.J.; et al. Do biomarkers of inflammation, monocyte activation, and altered coagulation explain excess mortality between HIV infected and uninfected people? J. Acquir. Immune Defic. Syndr. 2016, 72, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, T.B.; Ertner, G.; Petersen, J.; Moller, H.J.; Moestrup, S.K.; Eugen-Olsen, J.; Kronborg, G.; Benfield, T. Plasma soluble cd163 level independently predicts all-cause mortality in HIV-1-infected individuals. J. Infect. Dis. 2016, 214, 1198–1204. [Google Scholar] [CrossRef] [PubMed]
- Kelesidis, T.; Tran, T.T.; Stein, J.H.; Brown, T.T.; Moser, C.; Ribaudo, H.J.; Dube, M.P.; Murphy, R.; Yang, O.O.; Currier, J.S.; et al. Changes in inflammation and immune activation with atazanavir-, raltegravir-, darunavir-based initial antiviral therapy: Actg 5260s. Clin. Infect. Dis. 2015, 61, 651–660. [Google Scholar] [CrossRef] [PubMed]
- O’Halloran, J.A.; Dunne, E.; Gurwith, M.; Lambert, J.S.; Sheehan, G.J.; Feeney, E.R.; Pozniak, A.; Reiss, P.; Kenny, D.; Mallon, P. The effect of initiation of antiretroviral therapy on monocyte, endothelial and platelet function in HIV-1 infection. HIV Med. 2015, 16, 608–619. [Google Scholar] [CrossRef] [PubMed]
- Sereti, I.; Krebs, S.J.; Phanuphak, N.; Fletcher, J.L.; Slike, B.; Pinyakorn, S.; O’Connell, R.J.; Rupert, A.; Chomont, N.; Valcour, V.; et al. Persistent, albeit reduced, chronic inflammation in persons starting antiretroviral therapy in acute HIV infection. Clin. Infect. Dis. 2017, 64, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Zungsontiporn, N.; Tello, R.R.; Zhang, G.; Mitchell, B.I.; Budoff, M.; Kallianpur, K.J.; Nakamoto, B.K.; Keating, S.M.; Norris, P.J.; Ndhlovu, L.C.; et al. Non-classical monocytes and monocyte chemoattractant protein-1 (mcp-1) correlate with coronary artery calcium progression in chronically HIV-1 infected adults on stable antiretroviral therapy. PLoS ONE 2016, 11, e0149143. [Google Scholar] [CrossRef] [PubMed]
- McKibben, R.A.; Margolick, J.B.; Grinspoon, S.; Li, X.; Palella, F.J., Jr.; Kingsley, L.A.; Witt, M.D.; George, R.T.; Jacobson, L.P.; Budoff, M.; et al. Elevated levels of monocyte activation markers are associated with subclinical atherosclerosis in men with and those without HIV infection. J. Infect. Dis. 2015, 211, 1219–1228. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.V.; Hullsiek, K.H.; Singh, A.; Wilson, E.; Henry, K.; Lichtenstein, K.; Onen, N.; Kojic, E.; Patel, P.; Brooks, J.T.; et al. Immunologic predictors of coronary artery calcium progression in a contemporary HIV cohort. AIDS 2014, 28, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Aron-Wisnewsky, J.; Clement, K. The gut microbiome, diet, and links to cardiometabolic and chronic disorders. Nature reviews. Nephrology 2016, 12, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Koeth, R.A.; Wang, Z.; Levison, B.S.; Buffa, J.A.; Org, E.; Sheehy, B.T.; Britt, E.B.; Fu, X.; Wu, Y.; Li, L.; et al. Intestinal microbiota metabolism of l-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat. Med. 2013, 19, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Handley, S.A.; Desai, C.; Zhao, G.; Droit, L.; Monaco, C.L.; Schroeder, A.C.; Nkolola, J.P.; Norman, M.E.; Miller, A.D.; Wang, D.; et al. Siv infection-mediated changes in gastrointestinal bacterial microbiome and virome are associated with immunodeficiency and prevented by vaccination. Cell. Host Microbe 2016, 19, 323–335. [Google Scholar] [CrossRef] [PubMed]
- Handley, S.A.; Thackray, L.B.; Zhao, G.; Presti, R.; Miller, A.D.; Droit, L.; Abbink, P.; Maxfield, L.F.; Kambal, A.; Duan, E.; et al. Pathogenic simian immunodeficiency virus infection is associated with expansion of the enteric virome. Cell 2012, 151, 253–266. [Google Scholar] [CrossRef] [PubMed]
- Monaco, C.L.; Gootenberg, D.B.; Zhao, G.; Handley, S.A.; Ghebremichael, M.S.; Lim, E.S.; Lankowski, A.; Baldridge, M.T.; Wilen, C.B.; Flagg, M.; et al. Altered virome and bacterial microbiome in human immunodeficiency virus-associated acquired immunodeficiency syndrome. Cell. Host Microbe 2016, 19, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Dillon, S.M.; Kibbie, J.; Lee, E.J.; Guo, K.; Santiago, M.L.; Austin, G.L.; Gianella, S.; Landay, A.L.; Donovan, A.M.; Frank, D.N.; et al. Low abundance of colonic butyrate-producing bacteria in HIV infection is associated with microbial translocation and immune activation. AIDS 2017, 31, 511–521. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, E.A.; Keshavarzian, A.; Losurdo, J.; Swanson, G.; Siewe, B.; Forsyth, C.; French, A.; Demarais, P.; Sun, Y.; Koenig, L.; et al. A compositional look at the human gastrointestinal microbiome and immune activation parameters in HIV infected subjects. PLoS Pathog. 2014, 10, e1003829. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, P.W.; Jeffery, I.B. Gut microbiota and aging. Science 2015, 350, 1214–1215. [Google Scholar] [CrossRef] [PubMed]
- Saraswati, S.; Sitaraman, R. Aging and the human gut microbiota-from correlation to causality. Front. Microbiol. 2014, 5, 764. [Google Scholar]
- Hsue, P.; Currier, J. Effect of Reducing Inflammation with Low Dose Methotrexate on Inflammatory Markers and Endothelial Function in Treated and Suppressed HIV Infection (nct01949116). Available online: https://clinicaltrials.gov/ct2/show/record/NCT01949116 (accessed on 20 January 2018).
- Hsue, P. Effect of il-1β inhibition on inflammation and cardiovascular risk (nct02272946). Available online: https://clinicaltrials.gov/ct2/show/record/NCT02272946 (accessed on 20 January 2018).
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.; Xu, L.; Abrams, D.I.; Towner, W.J.; Horberg, M.A.; Leyden, W.A.; Silverberg, M.J. Hmg-coa reductase inhibitors (statins) use and risk of non-hodgkin lymphoma in HIV-positive persons. AIDS 2011, 25, 1771–1777. [Google Scholar] [CrossRef] [PubMed]
- Overton, E.T.; Kitch, D.; Benson, C.A.; Hunt, P.W.; Stein, J.H.; Smurzynski, M.; Ribaudo, H.J.; Tebas, P. Effect of statin therapy in reducing the risk of serious non-aids-defining events and nonaccidental death. Clin. Infect. Dis. 2013, 56, 1471–1479. [Google Scholar] [CrossRef] [PubMed]


© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McGettrick, P.; Barco, E.A.; Mallon, P.W.G. Ageing with HIV. Healthcare 2018, 6, 17. https://doi.org/10.3390/healthcare6010017
McGettrick P, Barco EA, Mallon PWG. Ageing with HIV. Healthcare. 2018; 6(1):17. https://doi.org/10.3390/healthcare6010017
Chicago/Turabian StyleMcGettrick, Padraig, Elena Alvarez Barco, and Patrick W. G. Mallon. 2018. "Ageing with HIV" Healthcare 6, no. 1: 17. https://doi.org/10.3390/healthcare6010017
APA StyleMcGettrick, P., Barco, E. A., & Mallon, P. W. G. (2018). Ageing with HIV. Healthcare, 6(1), 17. https://doi.org/10.3390/healthcare6010017