Long-Term Melatonin Therapy for Adolescents and Young Adults with Chronic Sleep Onset Insomnia and Late Melatonin Onset: Evaluation of Sleep Quality, Chronotype, and Lifestyle Factors Compared to Age-Related Randomly Selected Population Cohorts

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
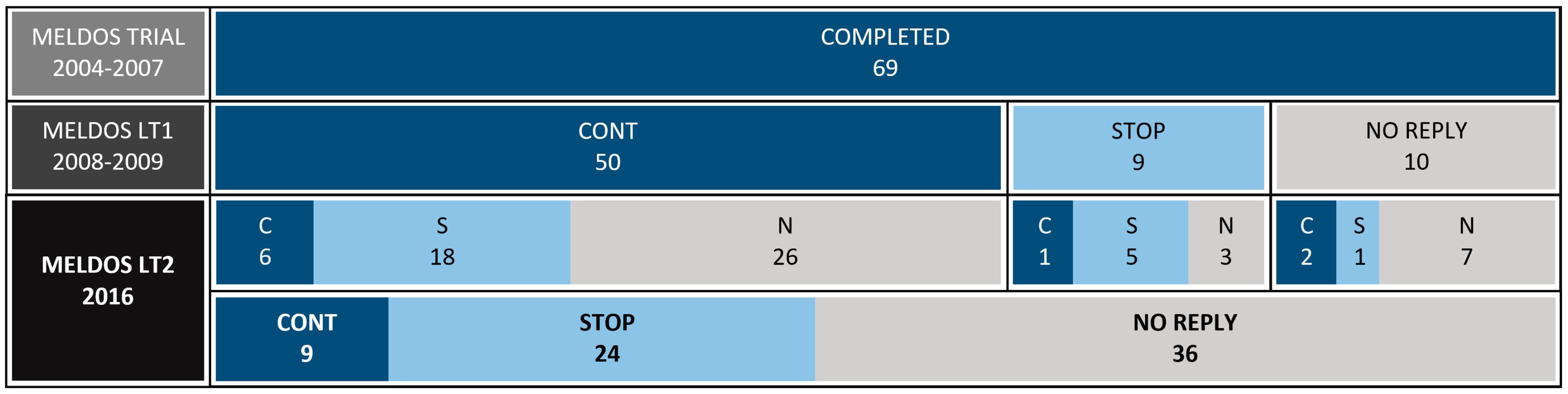
2.1. Study Design
2.2. Participants
2.3. Control Population
2.4. Questionnaire
2.5. Patient Characteristics
2.5.1. Demographics and Melatonin Use
2.5.2. Chronotype
2.5.3. Lifestyle Factors
2.6. Therapy Effectiveness
2.6.1. Sleep Quality
2.6.2. Sleep Timing
2.6.3. Safety
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
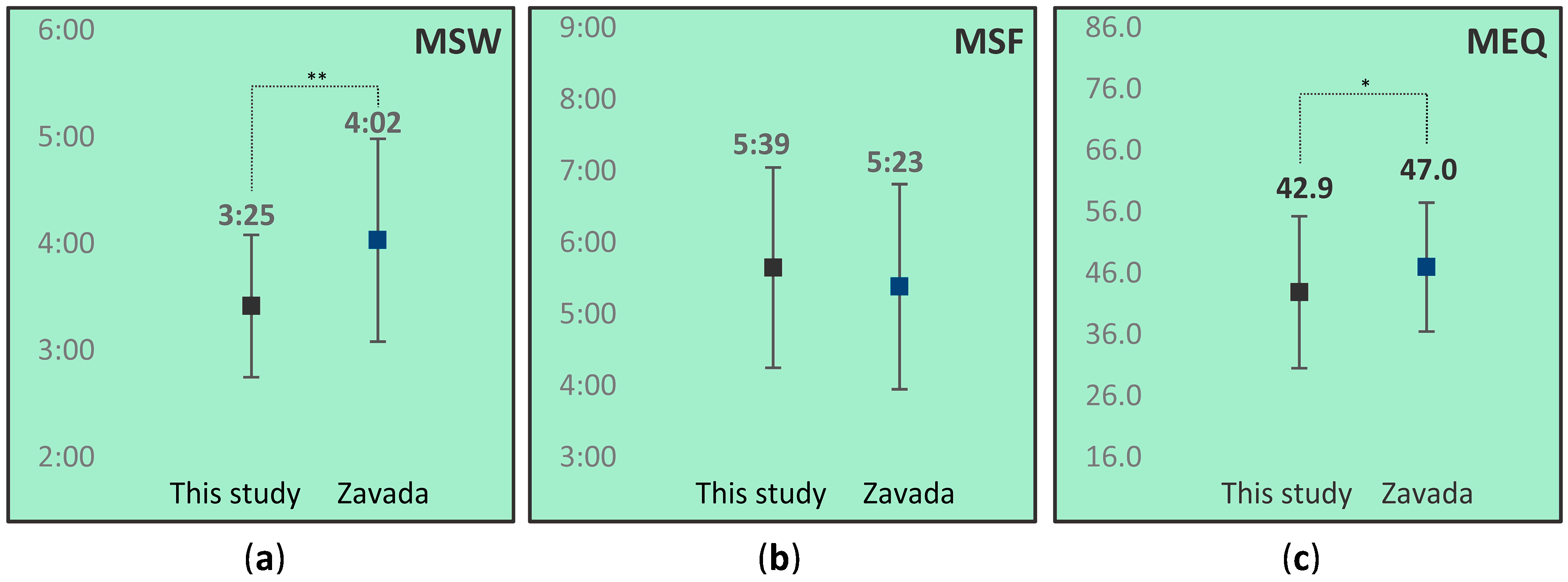
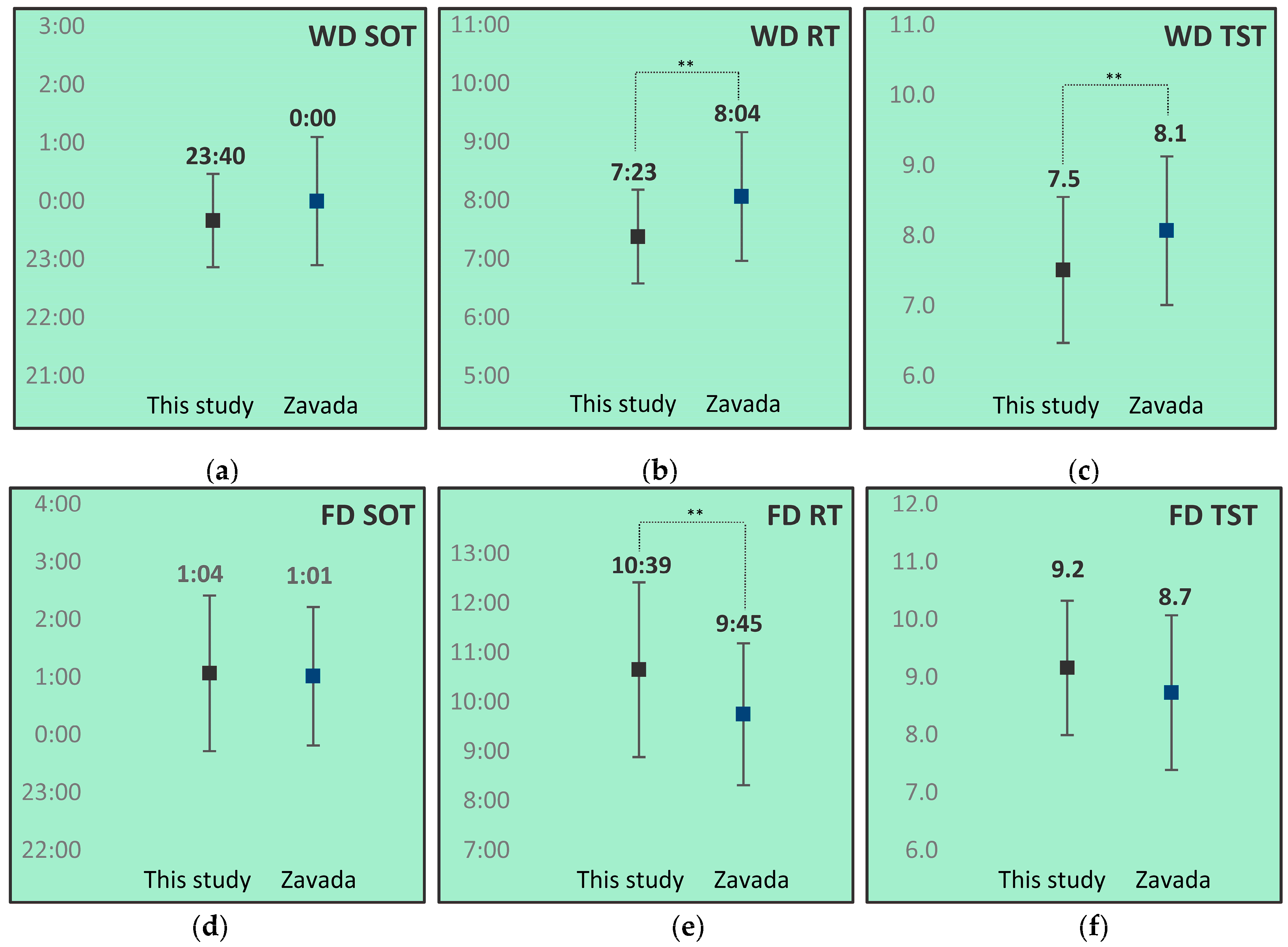
3.2. Chronotype
3.3. Lifestyle Factors
3.4. Therapy Effectiveness
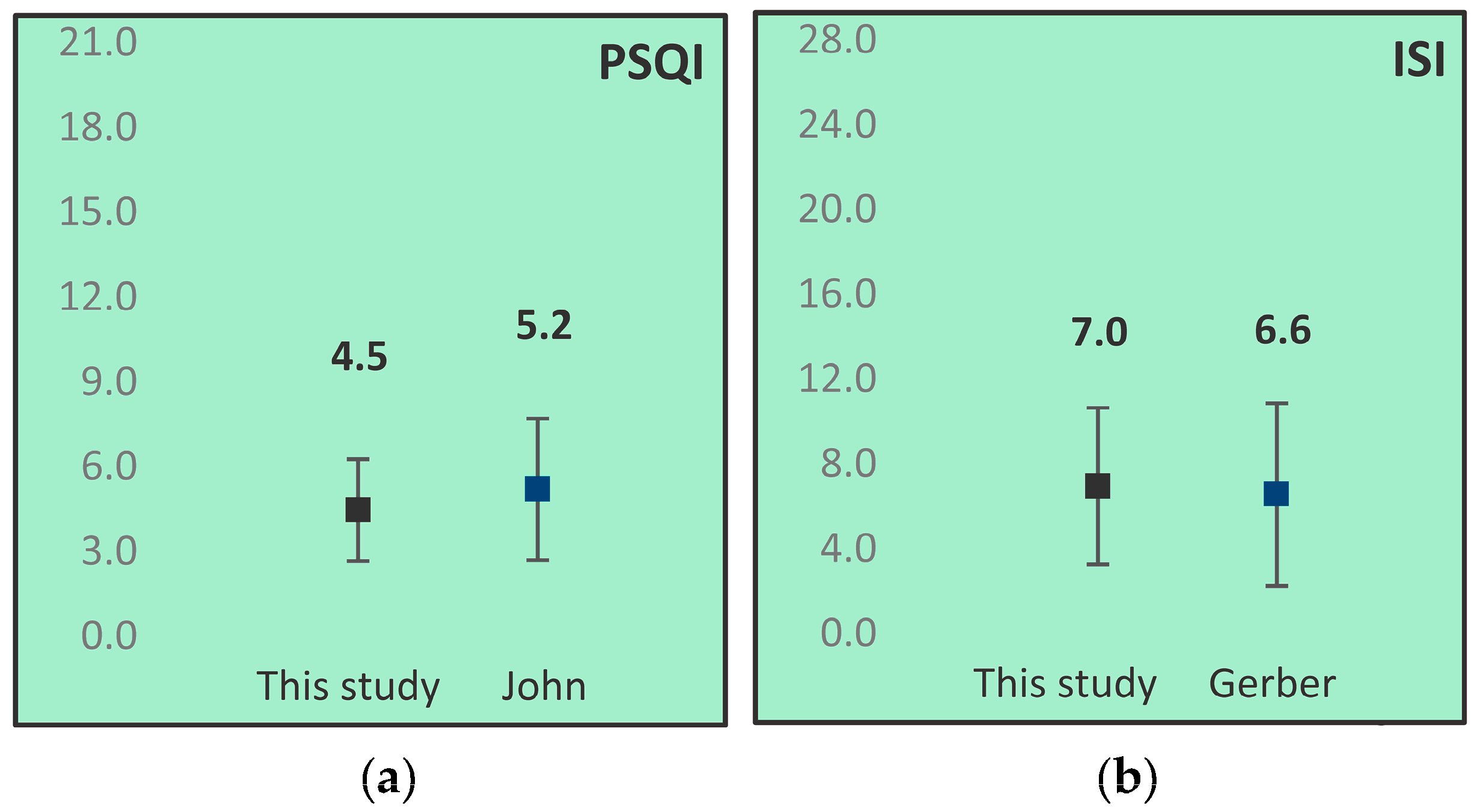
3.4.1. Sleep Quality
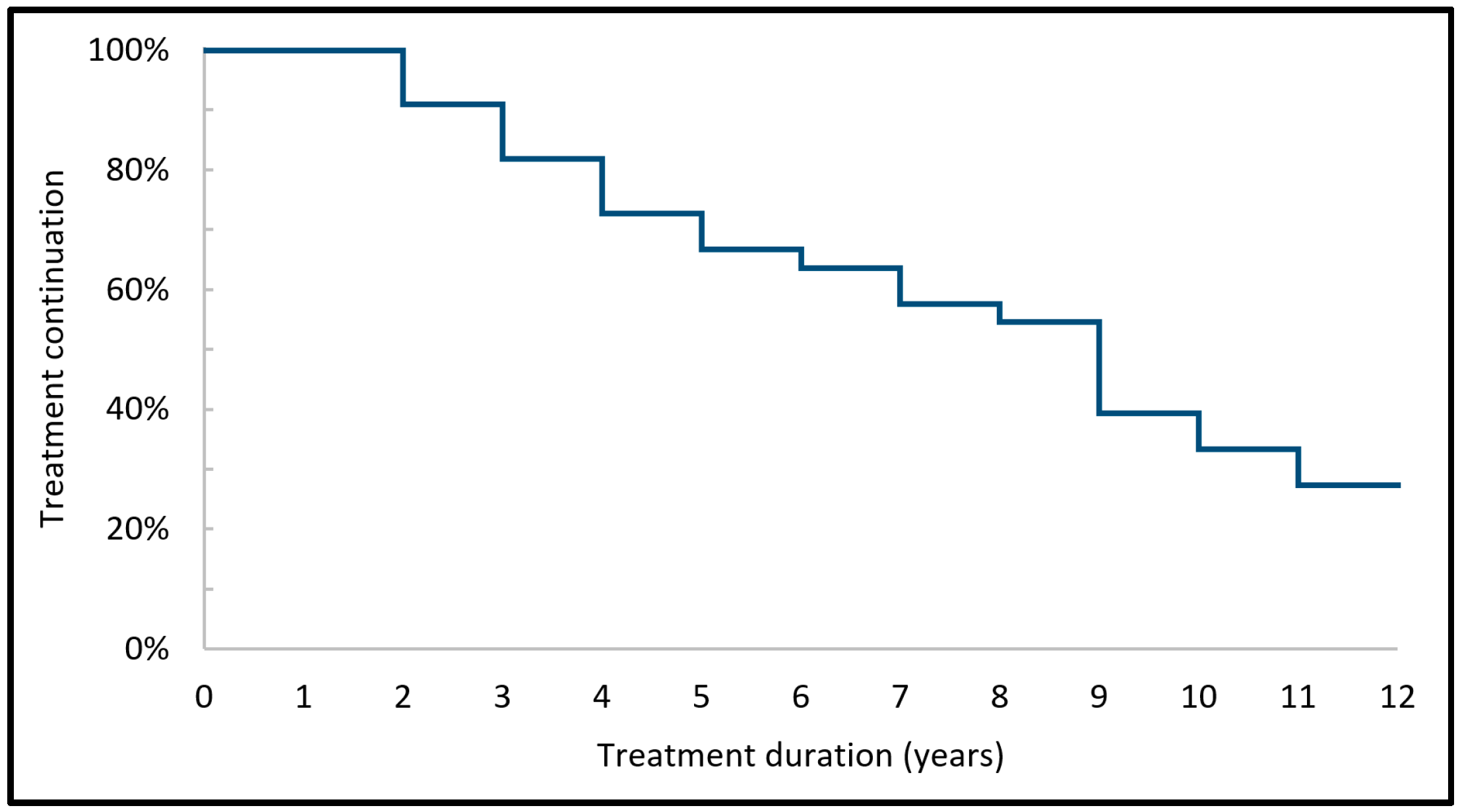
3.4.2. Sleep Timing
3.5. Safety
3.5.1. Adverse Effects
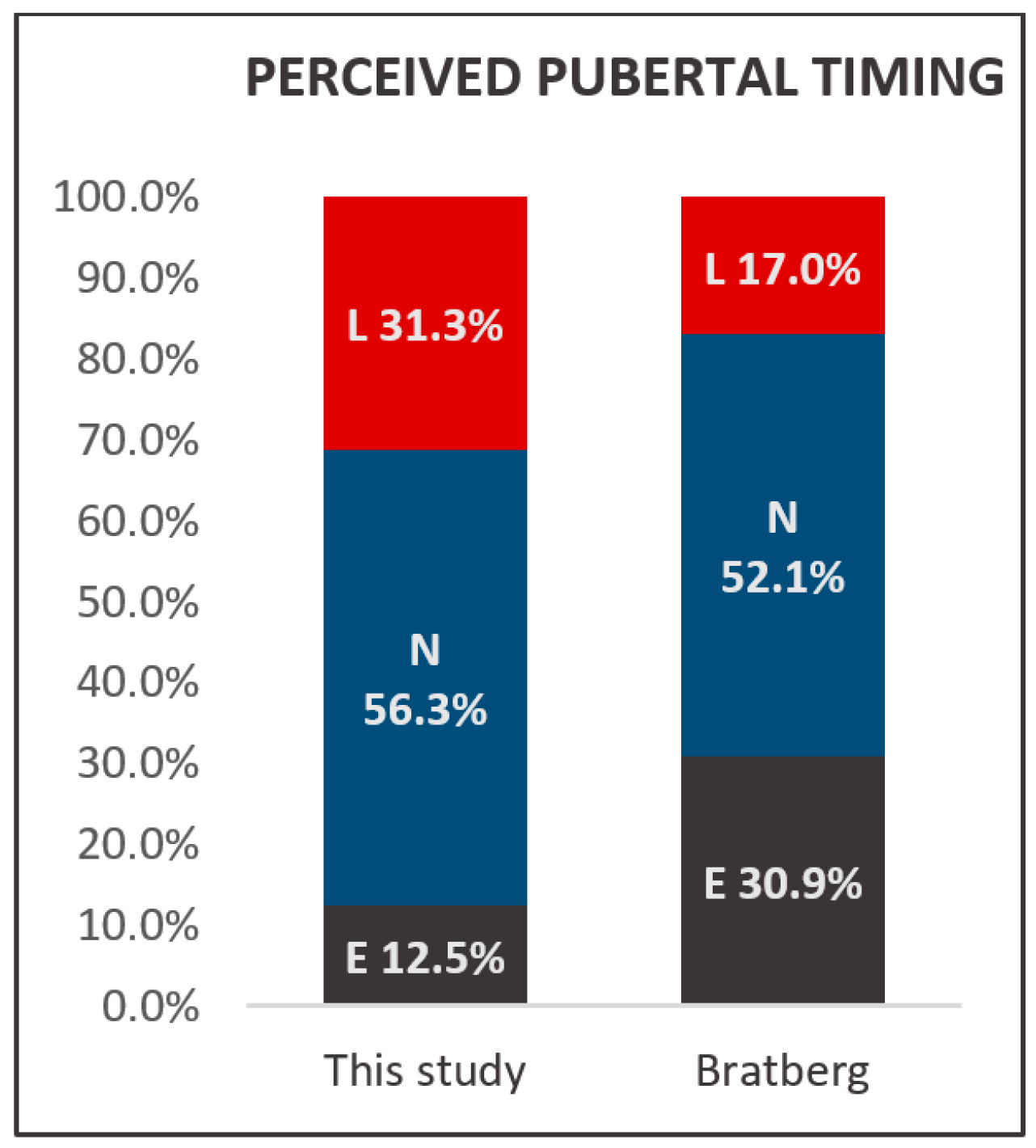
3.5.2. Pubertal Timing
4. Discussion
Strenghts and Limitations
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Bruni, O.; Alonso-Alconada, D.; Besag, F.; Biran, V.; Braam, W.; Cortese, S.; Moavero, R.; Parisi, P.; Smits, M.; Heijden, K.V.D.; et al. Current role of melatonin in pediatric neurology: Clinical recommendations. Eur. J. Paediatr. Neurol. 2015, 19, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Auger, R.R.; Burgess, H.J.; Emens, J.S.; Deriy, L.V.; Thomas, S.M.; Sharkey, K.M. Clinical Practice Guideline for the Treatment of Intrinsic Circadian Rhythm Sleep-Wake Disorders: Advanced Sleep-Wake Phase Disorder (ASWPD), Delayed Sleep-Wake Phase Disorder (DSWPD), Non-24-Hour Sleep-Wake Rhythm Disorder (N24SWD), and Irregular Sleep-Wake Rhythm Disorder (ISWRD). An Update for 2015: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2015, 11, 1199–1236. [Google Scholar] [CrossRef] [PubMed]
- Kennaway, D.J. Paediatric use of melatonin. Eur. J. Paediatr. Neurol. 2015, 19, 489–490. [Google Scholar] [CrossRef] [PubMed]
- Bruni, O.; Alonso-Alconada, D.; Besag, F.; Biran, V.; Braam, W.; Cortese, S.; Moavero, R.; Parisi, P.; Smits, M.; Heijden, K.V.D.; et al. Paediatric use of melatonin (Author reply to D. J. Kennaway). Eur. J. Paediatr. Neurol. 2015, 19, 491–493. [Google Scholar] [CrossRef] [PubMed]
- Carr, R.; Wasdell, M.B.; Hamilton, D.; Weiss, M.D.; Freeman, R.D.; Tai, J.; Rietveld, W.J.; Jan, J.E. Long-term effectiveness outcome of melatonin therapy in children with treatment-resistant circadian rhythm sleep disorders. J. Pineal Res. 2007, 43, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Hoebert, M.; van der Heijden, K.B.; van Geijlswijk, I.M.; Smits, M.G. Long-term follow-up of melatonin treatment in children with ADHD and chronic sleep onset insomnia. J. Pineal Res. 2009, 47, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Van Geijlswijk, I.M.; Mol, R.H.; Egberts, T.C.; Smits, M.G. Evaluation of sleep, puberty and mental health in children with long-term melatonin treatment for chronic idiopathic childhood sleep onset insomnia. Psychopharmacology 2011, 216, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Van Geijlswijk, I.M.; Korzilius, H.P.; Smits, M.G. The use of exogenous melatonin in delayed sleep phase disorder: A meta-analysis. Sleep 2010, 33, 1605–1614. [Google Scholar] [CrossRef] [PubMed]
- Van Geijlswijk, I.M.; van der Heijden, K.B.; Egberts, A.C.; Korzilius, H.P.; Smits, M.G. Dose finding of melatonin for chronic idiopathic childhood sleep onset insomnia: An RCT. Psychopharmacology 2010, 212, 379–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horne, J.A.; Ostberg, O. A self assessment questionnaire to determine Morningness Eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar] [PubMed]
- Hofstra, W.A.; Gordijn, M.C.M.; Van Hemert-Van Der Poel, J.C.; Van Der Palen, J.; De Weerd, A.W. Chronotypes and subjective sleep parameters in epilepsy patients: A large questionnaire study. Chronobiol. Int. 2010, 27, 1271–1286. [Google Scholar] [CrossRef] [PubMed]
- Di Milia, L.; Adan, A.; Natale, V.; Randler, C. Reviewing the psychometric properties of contemporary circadian typology measures. Chronobiol. Int. 2013, 30, 1261–1271. [Google Scholar] [CrossRef] [PubMed]
- Kerkhof, G. A Dutch questionnaire for the selection of morning and evening types (in Dutch). Ned. Tijdschr. Psychol. 1984, 39, 281–294. [Google Scholar]
- Roenneberg, T.; Wirz-Justice, A.; Merrow, M. Life between Clocks: Daily Temporal Patterns of Human Chronotypes. J. Biol. Rhythm. 2003, 18, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Kuehnle, T.; Juda, M.; Kantermann, T.; Allebrandt, K.; Gordijn, M.; Merrow, M. Epidemiology of the human circadian clock. Sleep Med. Rev. 2007, 11, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Zavada, A.; Gordijn, M.C.; Beersma, D.G.; Daan, S.; Roenneberg, T. Comparison of the Munich Chronotype Questionnaire with the Horne-Ostberg’s Morningness-Eveningness Score. Chronobiol. Int. 2005, 22, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Kantermann, T.; Sung, H.; Burgess, H.J. Comparing the Morningness-Eveningness Questionnaire and Munich ChronoType Questionnaire to the Dim Light Melatonin Onset. J. Biol. Rhythm. 2015, 30, 449–453. [Google Scholar] [CrossRef] [PubMed]
- LMU, M. Munich Chronotype Questionnaire. Available online: https://www.bioinfo.mpg.de/mctq/core_work_life/core/introduction.jsp?language=dut (accessed on 24 March 2016).
- Kühnle, T. Quantitative Analysis of Human Chronotypes; Ludwig Maximilian University München: München, Germany, 2006. [Google Scholar]
- Terman, J.S.; Terman, M.; Lo, E.S.; Cooper, T.B. Circadian time of morning light administration and therapeutic response in winter depression. Arch. Gen. Psychiatry 2001, 58, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Kuehnle, T.; Pramstaller, P.P.; Ricken, J.; Havel, M.; Guth, A.; Merrow, M. A marker for the end of adolescence. Curr. Biol. 2004, 14, R1038–R1039. [Google Scholar] [CrossRef] [PubMed]
- Wingen, M. Health Survey Questionnaire. 2014. Available online: https://www.cbs.nl/nl-nl/onze-diensten/methoden/onderzoeksomschrijvingen/aanvullende%20onderzoeksbeschrijvingen/vragenlijsten-gezondheidsenquete-vanaf-2014 (accessed on 1 March 2018).
- Netherlands Nutrition Centre Factsheet Caffeine. Available online: http://www.voedingscentrum.nl/Assets/Uploads/voedingscentrum/Documents/Professionals/Pers/Factsheets/English/factsheet%20Cafeine%20engelse%20versie%20vormgeving%20def%20LR.pdf (accessed on 26 July 2016).
- Buysse, D.J.; Reynolds III, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Morin, C. Insomnia: Psychological Assessment and Management; Guilford: New York, NY, USA, 1993. [Google Scholar]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Petersen, A.C.; Crockett, L.; Richards, M.; Boxer, A. A self-report measure of pubertal status: Reliability, validity, and initial norms. J. Youth Adolesc. 1988, 17, 117–133. [Google Scholar] [CrossRef] [PubMed]
- Van der Heijden, K.B.; Hamburger, H. Dutch Society for Sleep-Wake Research National Sleep Survey 2016: Sleep and Studying. 2016. Available online: www.nswo.nl/userfiles/files/Persbericht NSWO 2016.pdf (accessed on 1 March 2018).
- Van Laar, M.W.; Van Ooyen-Houben, M.M.J.; Cruts, A.A.N.; Meijer, R.F.; Croes, E.A.; Ketelaars, A.P.M.; Van der Pol, P.M. Trimbos Institute, Netherlands Institute of Mental Health and Addiction National Drug Monitor: Annual Update 2015. 2016. Available online: https://assets.trimbos.nl/docs/24dd30ba-464f-4dcd-a740-20ac058d310b.pdf (accessed on 1 March 2018).
- European Food Safety Authority (EFSA) Scientific Opinion on the Safety of Caffeine. 2015. Available online: http://onlinelibrary.wiley.com/doi/10.2903/j.efsa.2015.4102/epdf (accessed on 1 March 2018).
- Fossum, I.N.; Nordnes, L.T.; Storemark, S.S.; Bjorvatn, B.; Pallesen, S. The association between use of electronic media in bed before going to sleep and insomnia symptoms, daytime sleepiness, morningness, and chronotype. Behav. Sleep Med. 2014, 12, 343–357. [Google Scholar] [CrossRef] [PubMed]
- John, K.M.; Van den Berg, J.F. Chronotype, sleep quality and depressive symptoms: A cross-sectional study among Dutch students. Annu. Proc. NSWO 2014, 25, 64–67. [Google Scholar]
- Gerber, M.; Lang, C.; Lemola, S.; Colledge, F.; Kalak, N.; Holsboer-Trachsler, E.; Puhse, U.; Brand, S. Validation of the German version of the insomnia severity index in adolescents, young adults and adult workers: Results from three cross-sectional studies. BMC Psychiatry 2016, 16, 174. [Google Scholar] [CrossRef] [PubMed]
- Bratberg, G.H.; Nilsen, T.I.; Holmen, T.L.; Vatten, L.J. Perceived pubertal timing, pubertal status and the prevalence of alcohol drinking and cigarette smoking in early and late adolescence: A population based study of 8950 Norwegian boys and girls. Acta Paediatr. 2007, 96, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.S.; Gaudreault, M.M.; Perron, M.; Laberge, L. Chronotype, Light Exposure, Sleep, and Daytime Functioning in High School Students Attending Morning or Afternoon School Shifts: An Actigraphic Study. J. Biol. Rhythm. 2016, 31, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Braam, W.; van Geijlswijk, I.; Keijzer, H.; Smits, M.G.; Didden, R.; Curfs, L.M. Loss of response to melatonin treatment is associated with slow melatonin metabolism. J. Intellect. Disabil. Res. 2010, 54, 547–555. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.P.; Wang, J.; Holiday, D.B.; Warren, J.Y.; Paradoa, M.; Balkhi, A.M.; Fernandez-Baca, J.; McCrae, C.S. Sleep disturbances associated with cigarette smoking. Psychol. Health Med. 2014, 19, 410–419. [Google Scholar] [CrossRef] [PubMed]
- Cohrs, S.; Rodenbeck, A.; Riemann, D.; Szagun, B.; Jaehne, A.; Brinkmeyer, J.; Grunder, G.; Wienker, T.; Diaz-Lacava, A.; Mobascher, A.; et al. Impaired sleep quality and sleep duration in smokers-results from the German Multicenter Study on Nicotine Dependence. Addict. Biol. 2014, 19, 486–496. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.J.; Salo, P.; Lange, T.; Jennum, P.; Virtanen, M.; Pentti, J.; Kivimaki, M.; Vahtera, J.; Rod, N.H. Onset of impaired sleep as a predictor of change in health-related behaviours; analysing observational data as a series of non-randomized pseudo-trials. Int. J. Epidemiol. 2015, 44, 1027–1037. [Google Scholar] [CrossRef] [PubMed]
- Wittmann, M.; Dinich, J.; Merrow, M.; Roenneberg, T. Social jetlag: Misalignment of biological and social time. Chronobiol. Int. 2006, 23, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Owens, J.; Au, R.; Carskadon, M.; Millman, R.; Wolfson, A.; Braverman, P.K.; Adelman, W.P.; Breuner, C.C.; Levine, D.A.; Marcell, A.V.; et al. Insufficient sleep in adolescents and young adults: An update on causes and consequences. Pediatrics 2014, 134, e921–e932. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.J.; Clay, K.C.; Bramoweth, A.D.; Sethi, K.; Roane, B.M. Circadian phase preference in college students: Relationships with psychological functioning and academics. Chronobiol. Int. 2011, 28, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Ozguner, F.; Koyu, A.; Cesur, G. Active smoking causes oxidative stress and decreases blood melatonin levels. Toxicol. Ind. Health 2005, 21, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Ursing, C.; Wikner, J.; Brismar, K.; Rojdmark, S. Caffeine raises the serum melatonin level in healthy subjects: An indication of melatonin metabolism by cytochrome P450(CYP)1A2. J. Endocrinol. Investig. 2003, 26, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Ogilvie, B.W.; Torres, R.; Dressman, M.A.; Kramer, W.G.; Baroldi, P. Clinical assessment of drug-drug interactions of tasimelteon, a novel dual melatonin receptor agonist. J. Clin. Pharmacol. 2015, 55, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Hartter, S.; Nordmark, A.; Rose, D.M.; Bertilsson, L.; Tybring, G.; Laine, K. Effects of caffeine intake on the pharmacokinetics of melatonin, a probe drug for CYP1A2 activity. Br. J. Clin. Pharmacol. 2003, 56, 679–682. [Google Scholar] [CrossRef] [PubMed]
- Ursing, C.; von Bahr, C.; Brismar, K.; Rojdmark, S. Influence of cigarette smoking on melatonin levels in man. Eur. J. Clin. Pharmacol. 2005, 61, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Lemola, S.; Perkinson-Gloor, N.; Brand, S.; Dewald-Kaufmann, J.F.; Grob, A. Adolescents’ electronic media use at night, sleep disturbance, and depressive symptoms in the smartphone age. J. Youth Adolesc. 2015, 44, 405–418. [Google Scholar] [CrossRef] [PubMed]
- Falbe, J.; Davison, K.K.; Franckle, R.L.; Ganter, C.; Gortmaker, S.L.; Smith, L.; Land, T.; Taveras, E.M. Sleep duration, restfulness, and screens in the sleep environment. Pediatrics 2015, 135, e367–e375. [Google Scholar] [CrossRef] [PubMed]
- Wood, B.; Rea, M.S.; Plitnick, B.; Figueiro, M.G. Light level and duration of exposure determine the impact of self-luminous tablets on melatonin suppression. Appl. Ergon. 2013, 44, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Dubas, J.S.; Graber, J.A.; Petersen, A.C. A Longitudinal Investigation of Adolescents’ Changing Perceptions of Pubertal Timing. Dev. Psychol. 1991, 27, 580–586. [Google Scholar] [CrossRef]
- Cance, J.D.; Ennett, S.T.; Morgan-Lopez, A.A.; Foshee, V.A. The Stability of Perceived Pubertal Timing Across Adolescence. J. Youth Adolesc. 2012, 41, 764–775. [Google Scholar] [CrossRef] [PubMed]
- Vitale, J.A.; Roveda, E.; Montaruli, A.; Galasso, L.; Weydahl, A.; Caumo, A.; Carandente, F. Chronotype influences activity circadian rhythm and sleep: Differences in sleep quality between weekdays and weekend. Chronobiol. Int. 2015, 32, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Iglowstein, I.; Jenni, O.G.; Molinari, L.; Largo, R.H. Sleep duration from infancy to adolescence: Reference values and generational trends. Pediatrics 2003, 111, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Hayley, A.C.; Skogen, J.C.; Overland, S.; Wold, B.; Williams, L.J.; Kennedy, G.A.; Sivertsen, B. Trajectories and stability of self-reported short sleep duration from adolescence to adulthood. J. Sleep Res. 2015, 24, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M.; Carskadon, M.A.; Guilleminault, C.; Vitiello, M.V. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: Developing normative sleep values across the human lifespan. Sleep 2004, 27, 1255–1273. [Google Scholar] [CrossRef] [PubMed]
- Stovner, L.J.; Andree, C. Prevalence of headache in Europe: A review for the Eurolight project. J. Headache Pain 2010, 11, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Anonymous. European Medicines Agency (EMA) Circadin: EPAR—Product Information. 2009. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000695/WC500026811.pdf (accessed on 1 March 2018).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| This Study | CONT | STOP | ||
|---|---|---|---|---|
| N | 33 | 9 | 24 | |
| Males | 14 (42.4%) | 2 (22.2%) | 12 (50.0%) | |
| Age (years) | Mean | 19.6 | 20.3 | 19.4 |
| Range | 16.7 to 23.2 | 17.6 to 21.9 | 16.7 to 23.2 | |
| SD | 1.9 | 1.5 | 2.0 | |
| TD (years) | Mean | 7.1 | 10.8 | 5.7 |
| Range | 1.0 to 11.9 | 9.6 to 11.9 | 1.0 to 10.9 | |
| SD | 3.5 | 0.8 | 3.2 | |
| Dose (mg) | Mean | n/a | 2.9 | n/a |
| Range | n/a | 0.5 to 5.0 | n/a | |
| SD | n/a | 1.6 | n/a | |
| TOA (hh:mm) | Mean | n/a | 21:46 | n/a |
| Range | n/a | 19:00 to 23:00 | n/a | |
| SD | n/a | 1:06 | n/a | |
| BMI (kg/m2) | Mean | 21.2 | 23.1 | 20.5 |
| Range | 17.0 to 29.8 | 19.0 to 29.8 | 17.0 to 26.6 | |
| SD | 2.7 | 3.3 | 2.1 | |
| Education level | High | 21 (63.6%) | 7 (77.8%) | 14 (58.3%) |
| Low | 12 (36.4%) | 2 (22.2%) | 10 (41.7%) | |
| Relationship | Yes | 11 (33.3%) | 1 (11.1%) | 10 (41.2%) |
| No | 22 (66.7%) | 8 (88.9%) | 14 (58.8%) | |
| Offspring | Yes | 1 (3.0%) | 0 (0.0%) | 1 (4.2%) |
| No | 32 (97.0%) | 9 (100.0%) | 23 (95.8%) | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zwart, T.C.; Smits, M.G.; Egberts, T.C.G.; Rademaker, C.M.A.; Van Geijlswijk, I.M. Long-Term Melatonin Therapy for Adolescents and Young Adults with Chronic Sleep Onset Insomnia and Late Melatonin Onset: Evaluation of Sleep Quality, Chronotype, and Lifestyle Factors Compared to Age-Related Randomly Selected Population Cohorts. Healthcare 2018, 6, 23. https://doi.org/10.3390/healthcare6010023
Zwart TC, Smits MG, Egberts TCG, Rademaker CMA, Van Geijlswijk IM. Long-Term Melatonin Therapy for Adolescents and Young Adults with Chronic Sleep Onset Insomnia and Late Melatonin Onset: Evaluation of Sleep Quality, Chronotype, and Lifestyle Factors Compared to Age-Related Randomly Selected Population Cohorts. Healthcare. 2018; 6(1):23. https://doi.org/10.3390/healthcare6010023
Chicago/Turabian StyleZwart, Tom C., Marcel G. Smits, Toine C.G. Egberts, Carin M.A. Rademaker, and Ingeborg M. Van Geijlswijk. 2018. "Long-Term Melatonin Therapy for Adolescents and Young Adults with Chronic Sleep Onset Insomnia and Late Melatonin Onset: Evaluation of Sleep Quality, Chronotype, and Lifestyle Factors Compared to Age-Related Randomly Selected Population Cohorts" Healthcare 6, no. 1: 23. https://doi.org/10.3390/healthcare6010023
APA StyleZwart, T. C., Smits, M. G., Egberts, T. C. G., Rademaker, C. M. A., & Van Geijlswijk, I. M. (2018). Long-Term Melatonin Therapy for Adolescents and Young Adults with Chronic Sleep Onset Insomnia and Late Melatonin Onset: Evaluation of Sleep Quality, Chronotype, and Lifestyle Factors Compared to Age-Related Randomly Selected Population Cohorts. Healthcare, 6(1), 23. https://doi.org/10.3390/healthcare6010023