Functionality in Middle-Aged and Older Overweight and Obese Individuals with Knee Osteoarthritis





Abstract
:1. Introduction
2. Materials and Methods
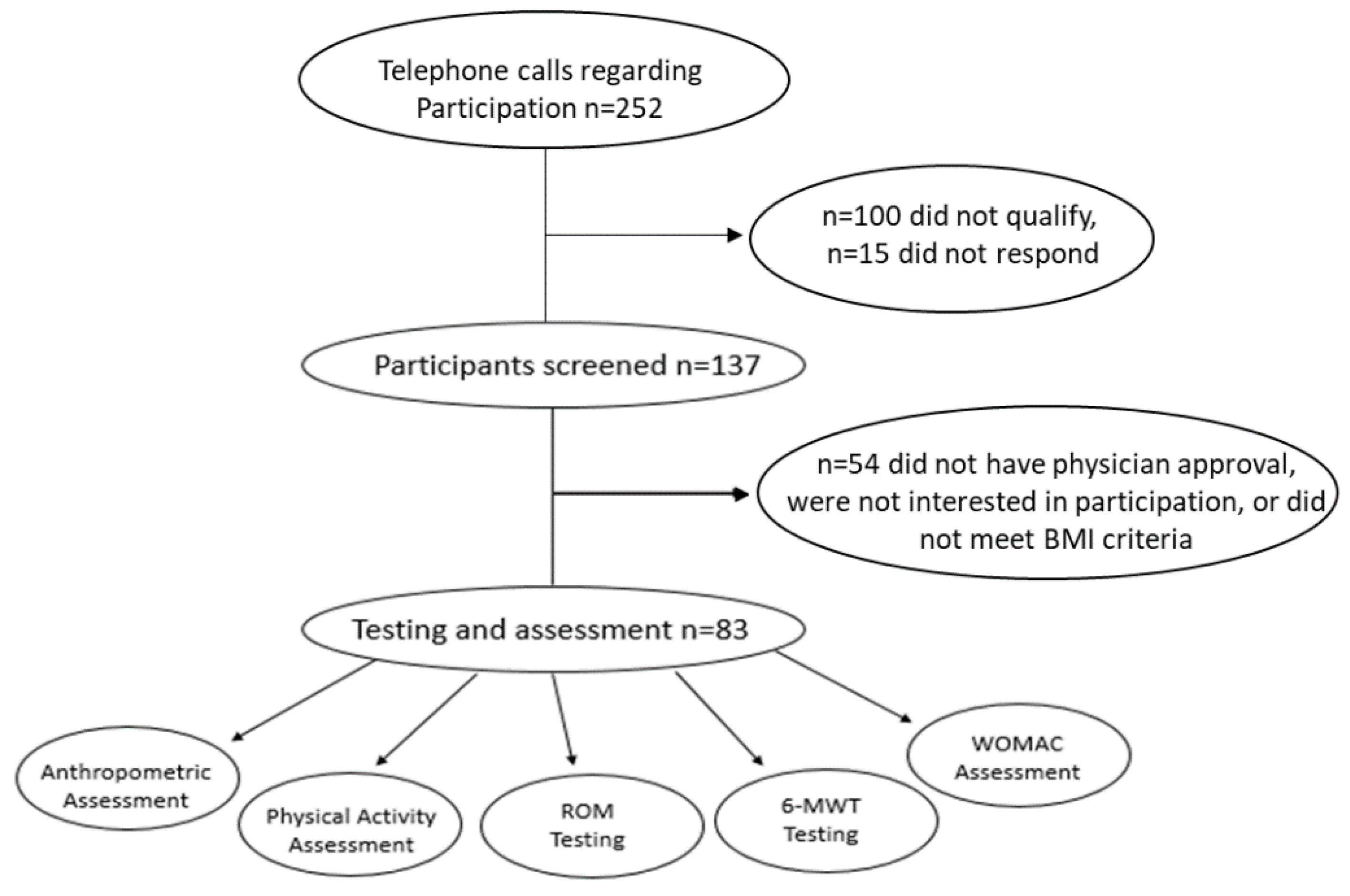
2.1. Participants
2.2. Study Overview
2.3. Assessment of Physical Activity
2.4. Assessment of Range of Motion, Functionality, and Lower Extremity Pain
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
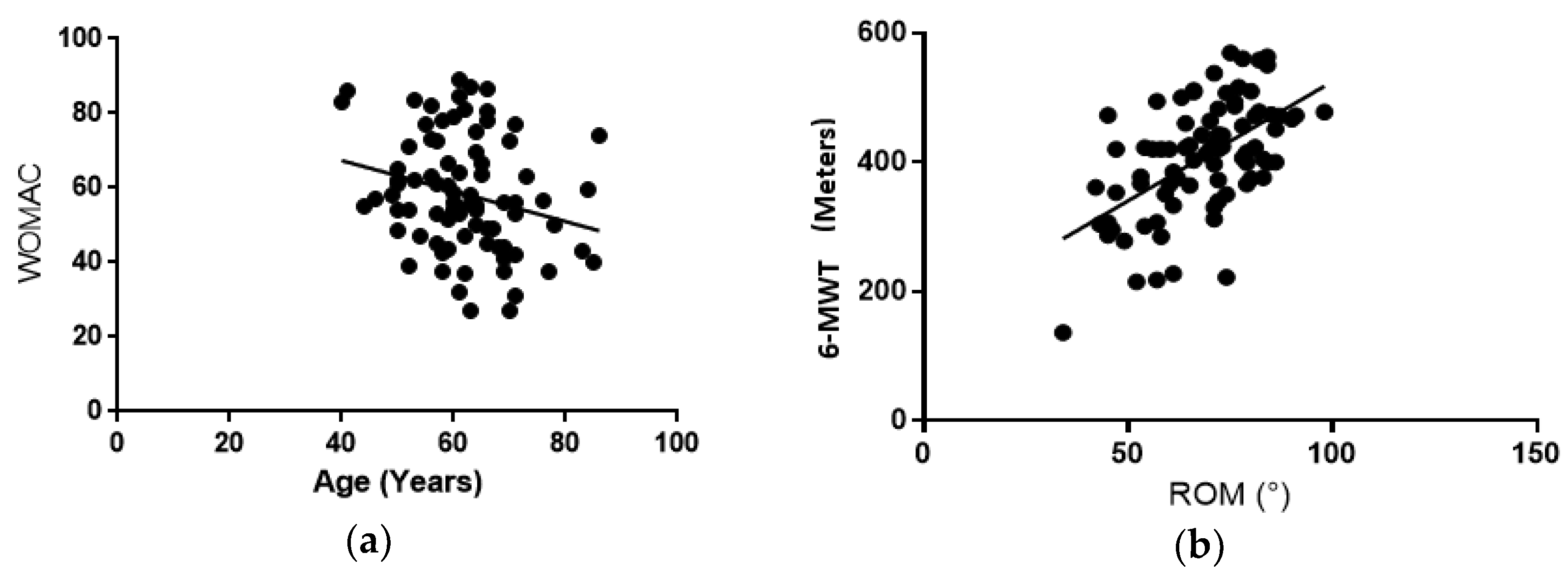
3.2. Age
3.3. Body Mass Index (BMI)
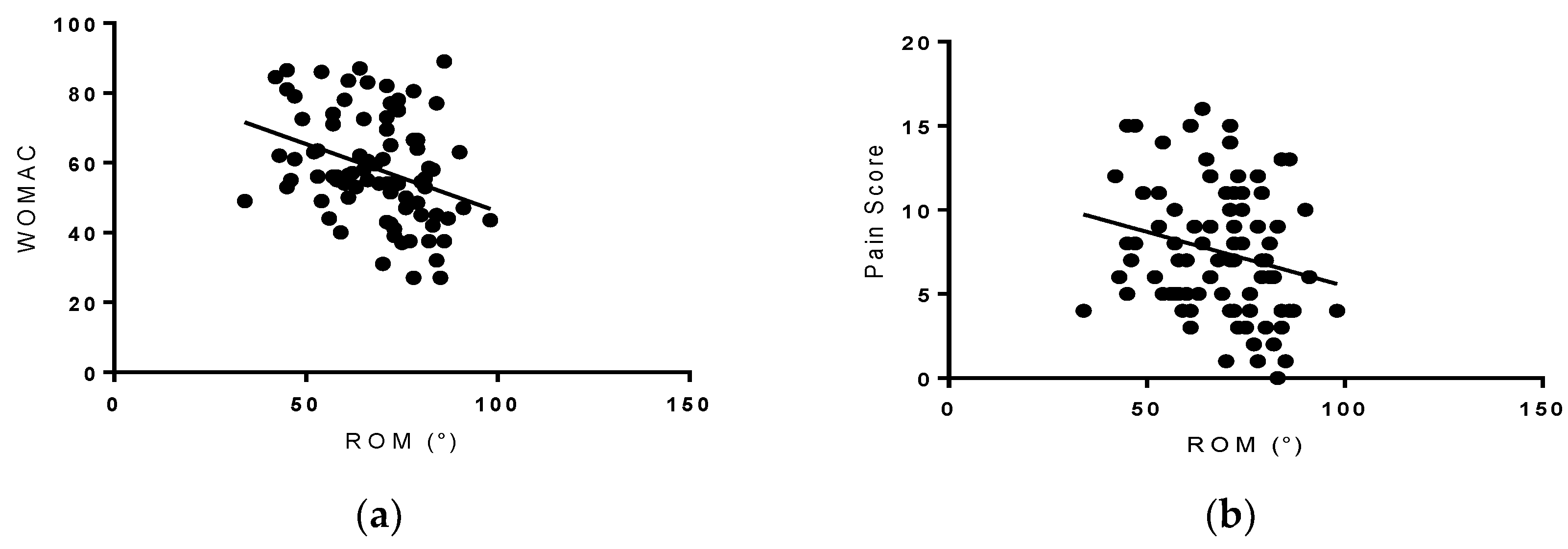
3.4. Range of Motion (ROM)
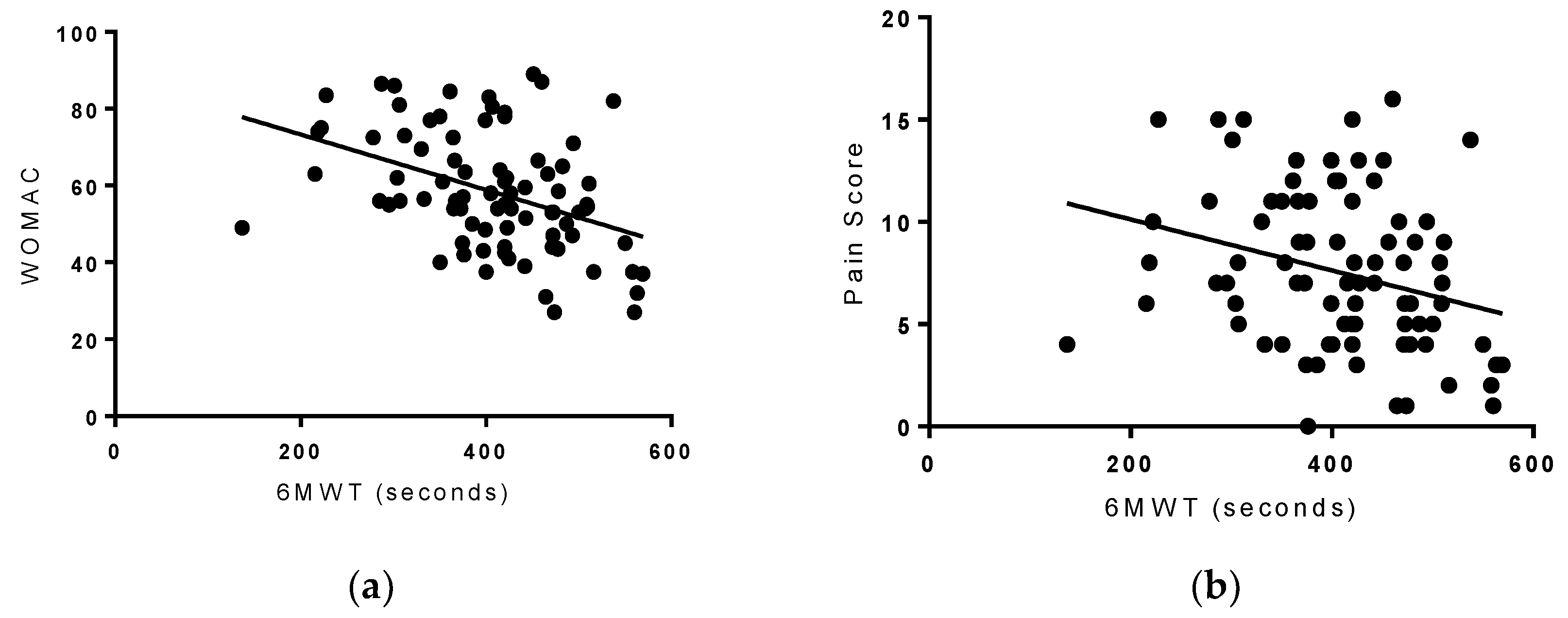
3.5. Six-Minute Walk Test (6-MWT)
3.6. Total Energy Expenditure (TEE)
3.7. Gender
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Xing, D.; Xu, Y.; Liu, Q.; Ke, Y.; Wang, B.; Li, Z.; Lin, J. Osteoarthritis and all-cause mortality in worldwide populations: Grading the evidence from a meta-analysis. Sci. Rep. 2016, 6, 24393. [Google Scholar] [CrossRef] [PubMed]
- Word Health Organization. Priority Medicines for Europe and the World 2013 Update. vol. 6.12 Osteoarthritis-Priority Diseases and Reasons for Inclusion; Word Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Woolf, A.D.; Pfleger, B. Burden of major musculoskeletal conditions. Bull. World Health Organ. 2003, 81, 646–656. [Google Scholar] [PubMed]
- Bhatia, D.; Bejarano, T.; Novo, M. Current interventions in the management of knee osteoarthritis. J. Pharm. Bioallied Sci. 2013, 5, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Yin, J.; Gao, J.; Cheng, T.S.; Pavlos, N.J.; Zhang, C.; Zheng, M.H. Subchondral bone in osteoarthritis: Insight into risk factors and microstructural changes. Arthritis Res. Ther. 2013, 15, 223. [Google Scholar] [CrossRef] [PubMed]
- Henrotin, Y.; Pesesse, L.; Sanchez, C. Subchondral bone and osteoarthritis: Biological and cellular aspects. Osteoporos Int. 2012, 23 (Suppl. 8), S847–S851. [Google Scholar] [CrossRef] [PubMed]
- Cisternas, M.G.; Murphy, L.; Sacks, J.J.; Solomon, D.H.; Pasta, D.J.; Helmick, C.G. Alternative Methods for Defining Osteoarthritis and the Impact on Estimating Prevalence in a US Population-Based Survey. Arthritis Care Res. 2016, 68, 574–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bitton, R. The economic burden of osteoarthritis. Am. J. Manag. Care 2009, 15, S230–S235. [Google Scholar] [PubMed]
- Coggon, D.; Reading, I.; Croft, P.; McLaren, M.; Barrett, D.; Cooper, C. Knee osteoarthritis and obesity. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 622–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, L.K.; March, L. Anandacoomarasamy A: Obesity & osteoarthritis. Indian J. Med. Res. 2013, 138, 185–193. [Google Scholar] [PubMed]
- Berry, P.A.; Wluka, A.E.; Davies-Tuck, M.L.; Wang, Y.; Strauss, B.J.; Dixon, J.B.; Proietto, J.; Jones, G.; Cicuttini, F.M. The relationship between body composition and structural changes at the knee. Rheumatology 2010, 49, 2362–2369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sowers, M.R.; Karvonen-Gutierrez, C.A. The evolving role of obesity in knee osteoarthritis. Curr. Opin. Rheumatol. 2010, 22, 533–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arden, N.; Nevitt, M.C. Osteoarthritis: Epidemiology. Best Pract. Res. Clin. Rheumatol. 2006, 20, 3–25. [Google Scholar] [CrossRef] [PubMed]
- Loeser, R.F. Aging processes and the development of osteoarthritis. Curr. Opin. Rheumatol. 2013, 25, 108–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conley, S.; Rosenberg, A.; Crowninshield, R. The female knee: Anatomic variations. J. Am. Acad. Orthop. Surg. 2007, 15 (Suppl. 1), S31–S36. [Google Scholar] [CrossRef] [PubMed]
- Srikanth, V.K.; Fryer, J.L.; Zhai, G.; Winzenberg, T.M.; Hosmer, D.; Jones, G. A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthr. Cartil. 2005, 13, 769–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steultjens, M.P.; Dekker, J.; van Baar, M.E.; Oostendorp, R.A.; Bijlsma, J.W. Range of joint motion and disability in patients with osteoarthritis of the knee or hip. Rheumatology 2000, 39, 955–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angst, F.; Aeschlimann, A.; Steiner, W.; Stucki, G. Responsiveness of the WOMAC osteoarthritis index as compared with the SF-36 in patients with osteoarthritis of the legs undergoing a comprehensive rehabilitation intervention. Ann. Rheum. Dis. 2001, 60, 834–840. [Google Scholar] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar]
- Sallis, J.F.; Haskell, W.L.; Wood, P.D.; Fortmann, S.P.; Rogers, T.; Blair, S.N.; Paffenbarger, R.S. Physical activity assessment methodology in the Five-City Project. Am. J. Epidemiol. 1985, 121, 91–106. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar] [PubMed]
- Guyatt, G.H.; Sullivan, M.J.; Thompson, P.J.; Fallen, E.L.; Pugsley, S.O.; Taylor, D.W.; Berman, L.B. The 6-minute walk: A new measure of exercise capacity in patients with chronic heart failure. Can. Med. Assoc. J. 1985, 132, 919–923. [Google Scholar] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Oyeyemi, A.L. Body mass index, pain and function in individuals with knee osteoarthritis. Niger. Med. J. 2013, 54, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Shane Anderson, A.; Loeser, R.F. Why is osteoarthritis an age-related disease? Best Pract. Res. Clin. Rheumatol. 2010, 24, 15–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzcharles, M.A.; Lussier, D.; Shir, Y. Management of chronic arthritis pain in the elderly. Drugs Aging 2010, 27, 471–490. [Google Scholar] [CrossRef] [PubMed]
- Kauppila, A.M.; Kyllonen, E.; Mikkonen, P.; Ohtonen, P.; Laine, V.; Siira, P.; Niinimaki, J.; Arokoski, J.P. Disability in end-stage knee osteoarthritis. Disabil. Rehabil. 2009, 31, 370–380. [Google Scholar] [CrossRef] [PubMed]
- Sutbeyaz, S.T.; Sezer, N.; Koseoglu, B.F.; Ibrahimoglu, F.; Tekin, D. Influence of knee osteoarthritis on exercise capacity and quality of life in obese adults. Obesity 2007, 15, 2071–2076. [Google Scholar] [CrossRef] [PubMed]
- Glass, N.; Segal, N.A.; Sluka, K.A.; Torner, J.C.; Nevitt, M.C.; Felson, D.T.; Bradley, L.A.; Neogi, T.; Lewis, C.E.; Frey-Law, L.A. Examining sex differences in knee pain: The multicenter osteoarthritis study. Osteoarthr. Cartil. 2014, 22, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Alves, J.C.; Bassitt, D.P. Quality of life and functional capacity of elderly women with knee osteoarthritis. Einstein 2013, 11, 209–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Jordan, J.M. Epidemiology of osteoarthritis. Clin. Geriatr. Med. 2010, 26, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Nejati, P.; Farzinmehr, A.; Moradi-Lakeh, M. The effect of exercise therapy on knee osteoarthritis: A randomized clinical trial. Med. J. Islam. Repub. Iran 2015, 29, 186. [Google Scholar] [PubMed]
- Tanaka, R.; Ozawa, J.; Kito, N.; Moriyama, H. Effects of exercise therapy on walking ability in individuals with knee osteoarthritis: A systematic review and meta-analysis of randomised controlled trials. Clin. Rehabil. 2016, 30, 36–52. [Google Scholar] [CrossRef] [PubMed]
- Reijman, M.; Pols, H.A.; Bergink, A.P.; Hazes, J.M.; Belo, J.N.; Lievense, A.M.; Bierma-Zeinstra, S.M. Body mass index associated with onset and progression of osteoarthritis of the knee but not of the hip: The Rotterdam Study. Ann. Rheum. Dis. 2007, 66, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Hart, D.J.; Doyle, D.V.; Spector, T.D. Incidence and risk factors for radiographic knee osteoarthritis in middle-aged women: The Chingford Study. Arthritis Rheum. 1999, 42, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Tang, X.; Wang, S.; Zhan, S.; Niu, J.; Tao, K.; Zhang, Y.; Lin, J. The Prevalence of Symptomatic Knee Osteoarthritis in China: Results From the China Health and Retirement Longitudinal Study. Arthritis Rheumatol. 2016, 68, 648–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunlop, D.D.; Song, J.; Semanik, P.A.; Chang, R.W.; Sharma, L.; Bathon, J.M.; Eaton, C.B.; Hochberg, M.C.; Jackson, R.D.; Kwoh, C.K.; et al. Objective physical activity measurement in the osteoarthritis initiative: Are guidelines being met? Arthritis Rheum. 2011, 63, 3372–3382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, R.; Astrup, A.; Bliddal, H. Weight loss: The treatment of choice for knee osteoarthritis? A randomized trial. Osteoarthr. Cartil. 2005, 13, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Christensen, R.; Bartels, E.M.; Astrup, A.; Bliddal, H. Effect of weight reduction in obese patients diagnosed with knee osteoarthritis: A systematic review and meta-analysis. Ann. Rheum. Dis. 2007, 66, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Connor Gorber, S.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Lagerros, Y.T.; Mucci, L.A.; Bellocco, R.; Nyrén, O.; Bälter, O.; Bälter, K.A. Validity and reliability of self-reported total energy expenditure using a novel instrument. Eur. J. Epidemiol. 2006, 21, 227–236. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 83) | Female (n = 66) | Male (n = 17) | Range | |
|---|---|---|---|---|
| Age (years) | 62.0 (9.0) | 61.2 (8.6) | 64.8 (8.8) | 52.8–71.2 |
| Weight (kg) | 90.0 (19.5) | 88.6 (20.0) | 99.4 (15.7) | 70.5–109.5 |
| Height (cm) | 167.0 (8.4) | 164.6 (7.1) | 176.5 (6.5) | 158.6–175.4 |
| BMI (kg/m2) | 32. (6.2) | 32.6 (6.6) | 31.9 (4.9) | 26.3–38.7 |
| ROM (°) | 68.2 (13.4) | 64.1 (13.9) | 68.4 (11.7) | 54.8–81.6 |
| 6-MWT (meters) | 407.6 (88.1) | 404.1 (87.6) | 421.3 (91.3) | 319.5–495.7 |
| WOMAC | 53.4 (15.4) | 60.1 (14.9) | 51.8 (15.7) | 38.0–68.7 |
| Moderate (hours) | 2.8 (2.8) | 2.7 (2.7) | 2.8 (3.0) | 0.0–5.6 |
| Hard (hours) | 0.5 (1.0) | 0.5 (1.1) | 0.7 (0.8) | 0.0–1.5 |
| Very Hard (hours) | 0.04 (0.14) | 0.05 (0.15) | 0.02 (0.06) | 0.0–0.18 |
| TEE (kcals) | 3809 (1120) | 3707 (1105) | 4201 (1120) | 2688–4929 |
| Female (n = 66) | Male (n = 17) | p-Value | <65 years (n = 55) | ≥65 years (n = 28) | p-Value | |
|---|---|---|---|---|---|---|
| BMI (kg/m2) | 32.9 (6.7) | 31.2 (4.8) | p > 0.05 | 43.0 (6.7) | 29.6 (4.0) t | p = 0.002 |
| ROM (°) | 64.8 (12.8) | 78.1 (9.8) | p > 0.05 | 69.8 (12.6) | 65.0(14.6) | p > 0.05 |
| WOMAC | 60.1 (14.9) * | 51.8 (15.7) | p = 0.046 * | 54.4 (15.8) | 60.4(14.9) t | p > 0.05 |
| 6-MWT | 388.0 (85.8) | 465.4 (65.3) | p > 0.05 | 424. 5(84.2) | 374.0(87.6) t | p = 0.013 t |
| Variables | Age (years) | Height (cm) | Weight (kg) | BMI (kg/m2) | ROM (°) | 6-MWT (m) | MOD (h) | HARD (h) | VHARD (h) | TEE (kcal) | WOMAC | PAIN |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 1 | −0.007 | −0.299 a | −0.349 a | 0.006 | −0.124 | 0.002 | −0.071 | −0.145 | −0.2 | −0.247 a | −0.378 |
| Height (cm) | −0.007 | 1 | 0.45 | −0.004 | 0.067 | 0.006 | −0.193 | 0.131 | −0.076 | 0.22 | −0.184 | −0.113 |
| Weight (kg) | −0.299 a | 0.45 | 1 | 0.888 | −0.045 | −0.136 | −0.125 | 0.045 | −0.148 | 0.476 f,g | 0.145 | 0.149 |
| BMI (kg/m2) | −0.349 a | −0.004 | 0.888 | 1 | −0.072 | −0.151 | −0.04 | −0.009 | −0.135 | 0.430 b | 0.268 b | 0.237 |
| ROM (°) | 0.006 | 0.067 | −0.045 | −0.072 | 1 | 0.561 c | 0.063 | 0.139 | 0.2 | 0.159 | −0.338 d | −0.222 d |
| 6-MWT | −0.124 | 0.006 | −0.136 | −0.151 | 0.561 c | 1 | 0.108 | 0.096 | 0.238 e | 0.061 | −0.413 e | −0.283 |
| MOD (h) | 0.002 | −0.193 | −0.125 | −0.04 | 0.063 | 0.108 | 1 | 0.236 | 0.055 | 0.567 g | 0.03 | 0.09 |
| HARD (h) | −0.071 | 0.131 | 0.045 | −0.009 | 0.139 | 0.096 | 0.236 | 1 | 0.148 | 0.544 g | 0.058 | 0.114 |
| VHARD (h) | −0.145 | −0.076 | −0.148 | −0.135 | 0.2 | 0.238 e | 0.055 | 0.148 | 1 | 0.078 | −0.109 | −0.014 |
| TEE (kcal) | −0.2 | 0.22 | 0.476 f,g | 0.430 b | 0.159 | 0.061 | 0.567 g | 0.544 g | 0.078 | 1 | 0.096 | 0.174 |
| WOMAC | −0.247 a | −0.184 | 0.145 | 0.268 b | −0.338 d | −0.413 e | 0.03 | 0.058 | −0.109 | 0.096 | 1 | 0.845 |
| PAIN | −0.378 | −0.113 | 0.149 | 0.237 | −0.222 de | −0.283 | 0.09 | 0.114 | −0.014 | 0.174 | 0.845 | 1 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akhavan, N.S.; Ormsbee, L.; Johnson, S.A.; George, K.S.; Foley, E.M.; Elam, M.L.; Ezzat-Zadeh, Z.; Panton, L.B.; Arjmandi, B.H. Functionality in Middle-Aged and Older Overweight and Obese Individuals with Knee Osteoarthritis. Healthcare 2018, 6, 74. https://doi.org/10.3390/healthcare6030074
Akhavan NS, Ormsbee L, Johnson SA, George KS, Foley EM, Elam ML, Ezzat-Zadeh Z, Panton LB, Arjmandi BH. Functionality in Middle-Aged and Older Overweight and Obese Individuals with Knee Osteoarthritis. Healthcare. 2018; 6(3):74. https://doi.org/10.3390/healthcare6030074
Chicago/Turabian StyleAkhavan, Neda S., Lauren Ormsbee, Sarah A. Johnson, Kelli S. George, Elizabeth M. Foley, Marcus L. Elam, Zahra Ezzat-Zadeh, Lynn B. Panton, and Bahram H. Arjmandi. 2018. "Functionality in Middle-Aged and Older Overweight and Obese Individuals with Knee Osteoarthritis" Healthcare 6, no. 3: 74. https://doi.org/10.3390/healthcare6030074
APA StyleAkhavan, N. S., Ormsbee, L., Johnson, S. A., George, K. S., Foley, E. M., Elam, M. L., Ezzat-Zadeh, Z., Panton, L. B., & Arjmandi, B. H. (2018). Functionality in Middle-Aged and Older Overweight and Obese Individuals with Knee Osteoarthritis. Healthcare, 6(3), 74. https://doi.org/10.3390/healthcare6030074