Systematic Approach to the Diagnosis and Treatment of Lyme Carditis and High-Degree Atrioventricular Block


Abstract
:1. Introduction
2. Systematic Approach to the Diagnosis and Management of Lyme Carditis
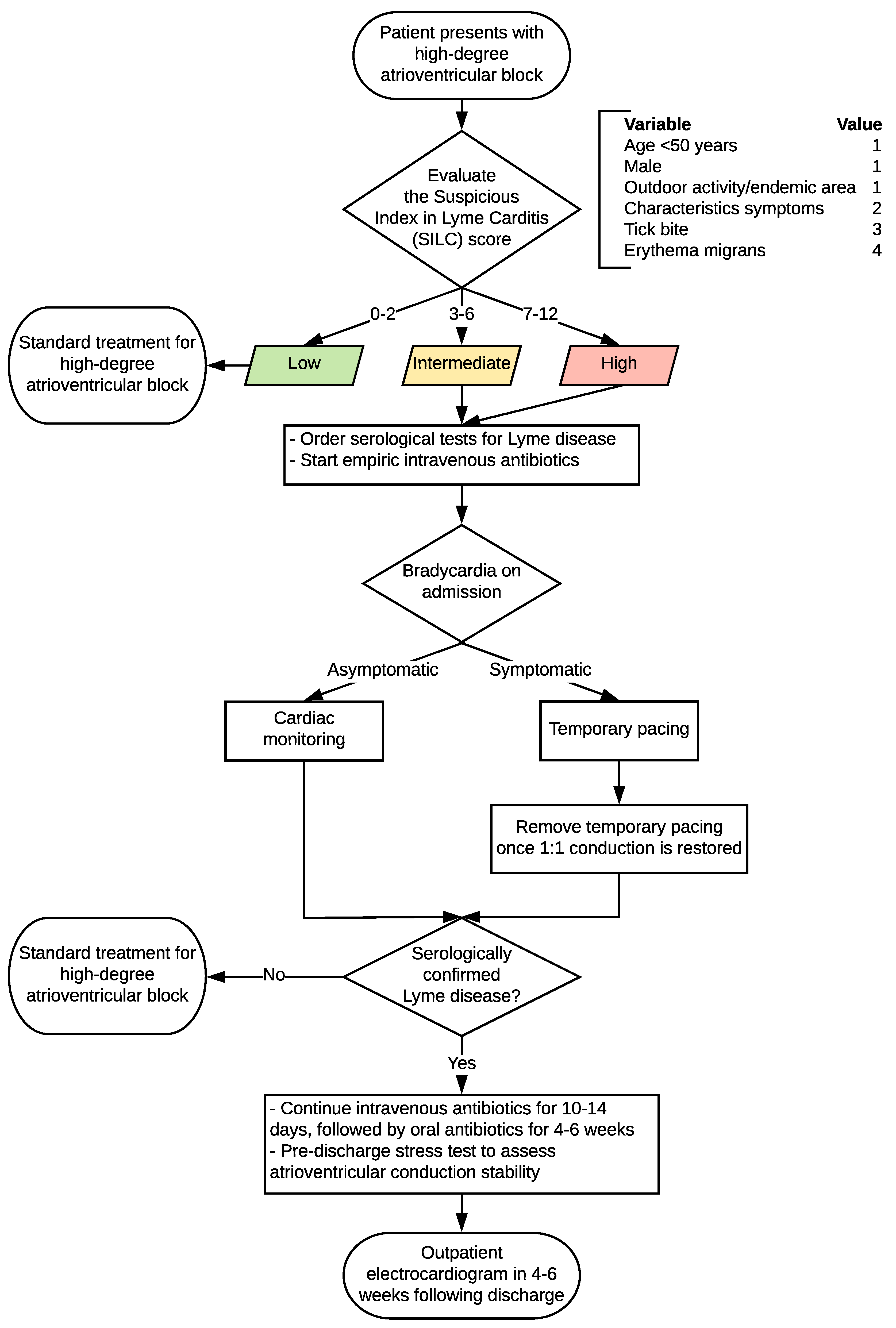
2.1. The Suspicious Index in Lyme Carditis (SILC) Risk Score
2.2. Algorithm for the Diagnosis and Management of Lyme Carditis
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mead, P.S. Epidemiology of Lyme disease. Infect. Dis. Clin. N. Am. 2015, 29, 187–210. [Google Scholar] [CrossRef] [PubMed]
- Bacon, R.M.; Kugeler, K.J.; Mead, P.S.; Centers for Disease Control and Prevention. Surveillance for Lyme disease—United States, 1992–2006. MMWR Surveill Summ. 2008, 57, 1–9. [Google Scholar] [PubMed]
- McAlister, H.F.; Klementowicz, P.T.; Andrews, C.; Fisher, J.D.; Feld, M.; Furman, S. Lyme carditis: An important cause of reversible heart block. Ann. Intern. Med. 1989, 110, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Steere, A.C.; Batsford, W.P.; Weinberg, M.; Alexander, J.; Berger, H.J.; Wolfson, S.; Malawista, S.E. Lyme carditis: Cardiac abnormalities of Lyme disease. Ann. Intern. Med. 1980, 93, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Krause, P.J.; Bockenstedt, L.K. Cardiology patient pages. Lyme disease and the heart. Circulation 2013, 127, e451–e454. [Google Scholar] [CrossRef] [PubMed]
- Nagi, K.S.; Joshi, R.; Thakur, R.K. Cardiac manifestations of Lyme disease: A review. Can. J. Cardiol. 1996, 12, 503–506. [Google Scholar] [PubMed]
- Van der Linde, M.R. Lyme carditis: Clinical characteristics of 105 cases. Scand. J. Infect. Dis. Suppl. 1991, 77, 81–84. [Google Scholar] [PubMed]
- Reznick, J.W.; Braunstein, D.B.; Walsh, R.L.; Smith, C.R.; Wolfson, P.M.; Gierke, L.W.; Gorelkin, L.; Chandler, F.W. Lyme carditis. Electrophysiologic and histopathologic study. Am. J. Med. 1986, 81, 923–927. [Google Scholar] [CrossRef]
- Van der Linde, M.R.; Crijns, H.J.; De Koning, J.; Hoogkamp-Korstanje, J.A.; De Graaf, J.J.; Piers, D.A.; Van der Galien, A.; Lie, K.I. Range of atrioventricular conduction disturbances in Lyme borreliosis: A report of four cases and review of other published reports. Br. Heart J. 1990, 63, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Cadavid, D.; Bai, Y.; Hodzic, E.; Narayan, K.; Barthold, S.W.; Pachner, A.R. Cardiac involvement in non-human primates infected with the lyme disease spirochete borrelia burgdorferi. Lab. Investig. 2004, 84, 1439–1450. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.L.; Barthold, S.W.; Persing, D.H.; Beck, D.S. Carditis in Lyme disease susceptible and resistant strains of laboratory mice infected with borrelia burgdorferi. Am. J. Trop. Med. Hyg 1992, 47, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.K.; Almaddah, N.; Chaudhry, K.; Ganatra, S.; Chaudhry, G.M.; Silver, J. Without further delay: Lyme carditis. Am. J. Med. 2018, 131, 384–386. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Three sudden cardiac deaths associated with Lyme carditis—United States, November 2012–July 2013. MMWR Morb. Mortal. Wkly. Rep. 2013, 62, 993–996. [Google Scholar]
- Forrester, J.D.; Meiman, J.; Mullins, J.; Nelson, R.; Ertel, S.H.; Cartter, M.; Brown, C.M.; Lijewski, V.; Schiffman, E.; Neitzel, D.; et al. Notes from the field: Update on Lyme carditis, groups at high risk, and frequency of associated sudden cardiac death—United States. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 982–983. [Google Scholar] [PubMed]
- Muehlenbachs, A.; Bollweg, B.C.; Schulz, T.J.; Forrester, J.D.; DeLeon Carnes, M.; Molins, C.; Ray, G.S.; Cummings, P.M.; Ritter, J.M.; Blau, D.M.; et al. Cardiac tropism of borrelia burgdorferi: An autopsy study of sudden cardiac death associated with Lyme carditis. Am. J. Pathol. 2016, 186, 1195–1205. [Google Scholar] [CrossRef] [PubMed]
- Fuster, L.S.; Gul, E.E.; Baranchuk, A. Electrocardiographic progression of acute Lyme disease. Am. J. Emerg Med. 2017, 35, 1040.e5–1040.e6. [Google Scholar] [CrossRef] [PubMed]
- Fu Md, J.; Bhatta, L. Lyme carditis: Early occurrence and prolonged recovery. J. Electrocardiol. 2018, 51, 516–518. [Google Scholar] [CrossRef] [PubMed]
- Wan, D.; Baranchuk, A. Lyme carditis and atrioventricular block. CMAJ 2018, 190, E622. [Google Scholar] [CrossRef] [PubMed]
- Wan, D.; Blakely, C.; Branscombe, P.; Suarez-Fuster, L.; Glover, B.; Baranchuk, A. Lyme carditis and high-degree atrioventricular block. Am. J. Cardiol. 2018, 121, 1102–1104. [Google Scholar] [CrossRef] [PubMed]
- Ogden, N.H.; Lindsay, L.R.; Morshed, M.; Sockett, P.N.; Artsob, H. The emergence of Lyme disease in Canada. CMAJ 2009, 180, 1221–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wormser, G.P.; Dattwyler, R.J.; Shapiro, E.D.; Halperin, J.J.; Steere, A.C.; Klempner, M.S.; Krause, P.J.; Bakken, J.S.; Strle, F.; Stanek, G.; et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: Clinical practice guidelines by the infectious diseases society of America. Clin. Infect. Dis. 2006, 43, 1089–1134. [Google Scholar] [CrossRef] [PubMed]
- Besant, G.; Wan, D.; Blakely, C.; Branscombe, P.; Suarez-Fuster, L.; Redfearn, D.; Simpson, C.; Abdollah, H.; Glover, B.; Baranchuk, A. Lyme carditis presenting with high-degree atrioventricular block: A systematic review. J. Electrocardiol. 2018, in press. [Google Scholar]
- Schwartz, B.S.; Goldstein, M.D. Lyme disease in outdoor workers: Risk factors, preventive measures, and tick removal methods. Am. J. Epidemiol. 1990, 131, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Applegren, N.D.; Kraus, C.K. Lyme disease: Emergency department considerations. J. Emerg. Med. 2017, 52, 815–824. [Google Scholar] [CrossRef] [PubMed]
- Russell, H.; Sampson, J.S.; Schmid, G.P.; Wilkinson, H.W.; Plikaytis, B. Enzyme-linked immunosorbent assay and indirect immunofluorescence assay for Lyme disease. J. Infect. Dis. 1984, 149, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Engstrom, S.M.; Shoop, E.; Johnson, R.C. Immunoblot interpretation criteria for serodiagnosis of early Lyme disease. J. Clin. Microbiol. 1995, 33, 419–427. [Google Scholar] [PubMed]
- Dressler, F.; Whalen, J.A.; Reinhardt, B.N.; Steere, A.C. Western blotting in the serodiagnosis of Lyme disease. J. Infect. Dis. 1993, 167, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Steere, A.C.; McHugh, G.; Damle, N.; Sikand, V.K. Prospective study of serologic tests for lyme disease. Clin. Infect. Dis. 2008, 47, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Steere, A.C. Lyme disease. N. Engl. J. Med. 2001, 345, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Pinto, D.S. Cardiac manifestations of Lyme disease. Med. Clin. N. Am. 2002, 86, 285–296. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Value |
|---|---|
| Age < 50 years | 1 |
| Male | 1 |
| Outdoor activity/endemic area | 1 |
| Constitutional symptoms 1 | 2 |
| Tick bite | 3 |
| Erythema migrans | 4 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeung, C.; Baranchuk, A. Systematic Approach to the Diagnosis and Treatment of Lyme Carditis and High-Degree Atrioventricular Block. Healthcare 2018, 6, 119. https://doi.org/10.3390/healthcare6040119
Yeung C, Baranchuk A. Systematic Approach to the Diagnosis and Treatment of Lyme Carditis and High-Degree Atrioventricular Block. Healthcare. 2018; 6(4):119. https://doi.org/10.3390/healthcare6040119
Chicago/Turabian StyleYeung, Cynthia, and Adrian Baranchuk. 2018. "Systematic Approach to the Diagnosis and Treatment of Lyme Carditis and High-Degree Atrioventricular Block" Healthcare 6, no. 4: 119. https://doi.org/10.3390/healthcare6040119
APA StyleYeung, C., & Baranchuk, A. (2018). Systematic Approach to the Diagnosis and Treatment of Lyme Carditis and High-Degree Atrioventricular Block. Healthcare, 6(4), 119. https://doi.org/10.3390/healthcare6040119