Comparison of Perceived and Observed Hand Hygiene Compliance in Healthcare Workers in MERS-CoV Endemic Regions


Abstract
:1. Introduction
1.1. Middle East Respiratory Syndrome (MERS)
1.2. Transmission of Virus in Hospitals
2. Materials and Methods
2.1. Setting
2.1.1. Public Hospital
2.1.2. Security Forces Hospital
2.1.3. Private Clinic
2.2. Participant Recruitment
2.3. Data Collection
2.3.1. Observation Checklist
2.3.2. Self-Report Questionnaire
2.4. Data Analysis
2.4.1. Person Correlation
2.4.2. t-test
3. Results
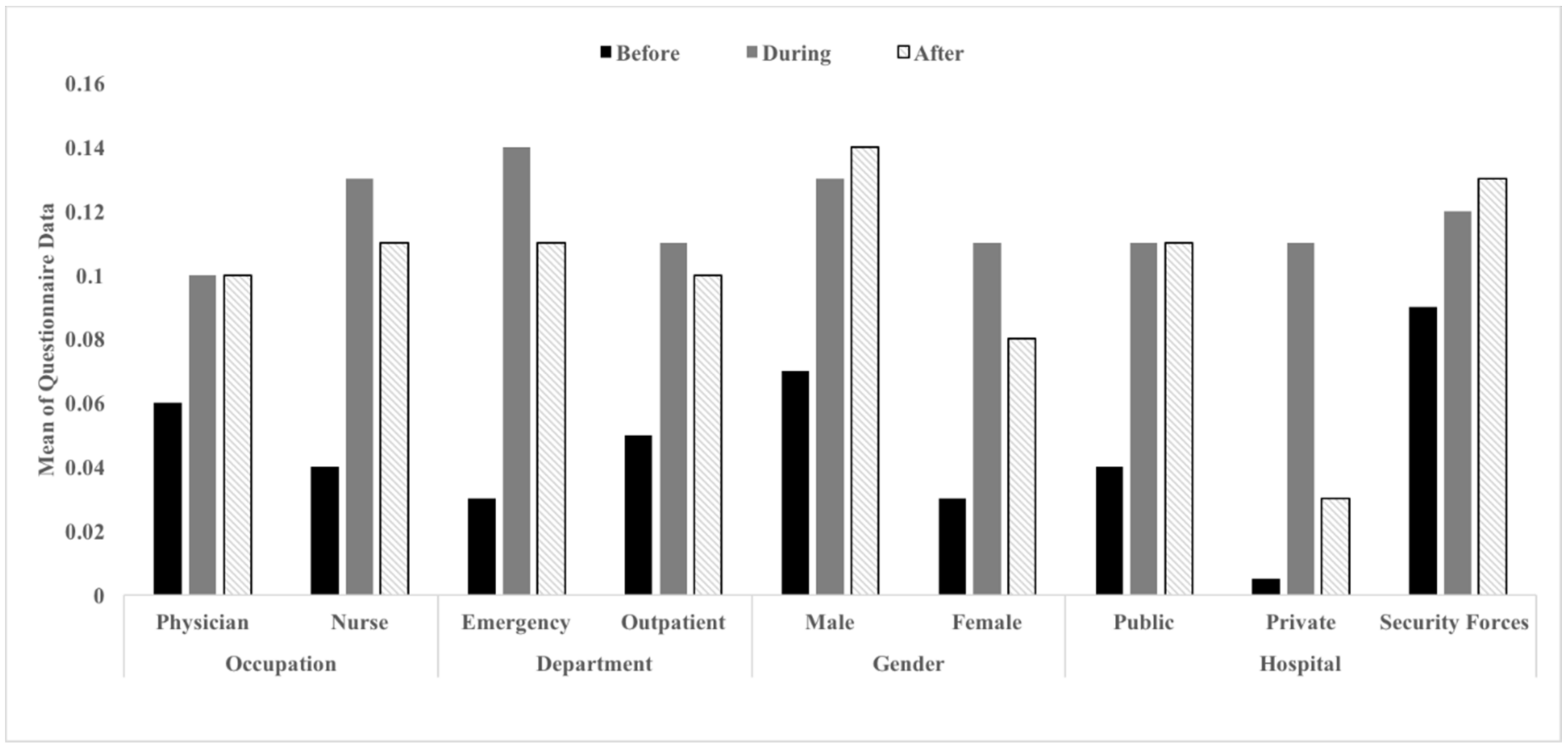
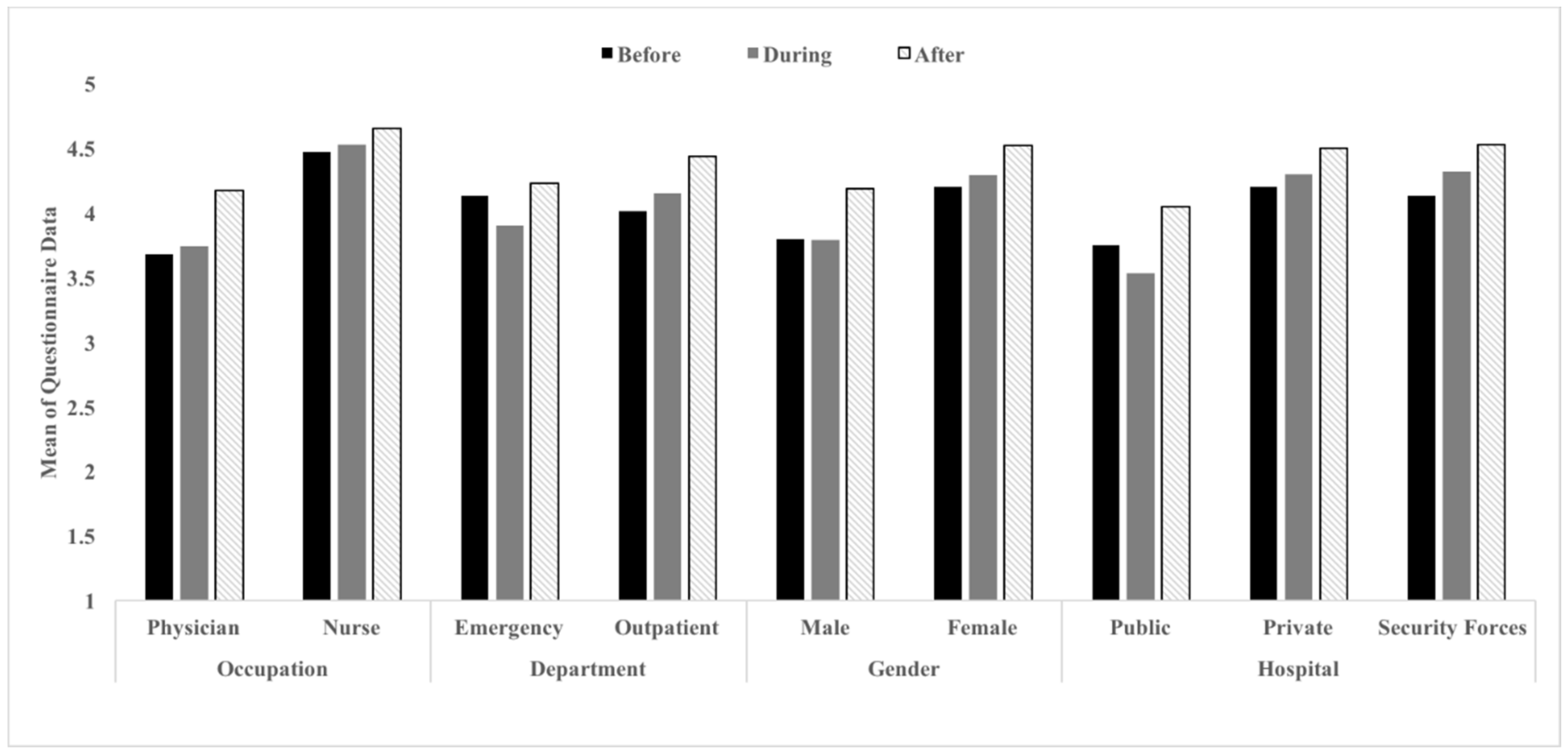
3.1. Descriptive Statistics
3.2. Person Correlation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kharma, M.Y.; Alalwani, M.S.; Amer, M.F.; Tarakji, B.; Aws, G. Assessment of the awareness level of dental students toward Middle East Respiratory Syndrome-coronavirus. J. Int. Soc. Prev. Community Dent. 2015, 5, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Pavli, A.; Tsiodras, S.; Maltezou, H.C. Middle East respiratory syndrome coronavirus (MERS-CoV: Prevention in travelers. Travel Med. Infect. Dis. 2014, 12, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Badawi, A.; Ryoo, S.G. Prevalence of comorbidities in the Middle East respiratory syndrome coronavirus (MERS-CoV): a systematic review and meta-analysis. Int. J. Infect. Dis. 2016, 49, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Mohd, H.A.; Al-Tawfiq, J.A.; Memish, Z.A. Middle East Respiratory Syndrome Coronavirus (MERS-CoV) origin and animal reservoir. Virol. J. 2016, 13, 87. [Google Scholar] [CrossRef] [PubMed]
- Statistics - Statistics. Available online: https://www.moh.gov.sa/en/CCC/PressReleases/Pages/default.aspx (accessed on 12 June 2018).
- Chowell, G.; Abdirizak, F.; Lee, S.; Jung, E.; Nishiura, H.; Viboud, C. Transmission characteristics of MERS and SARS in the healthcare setting: A comparative study. BMC Med. 2015, 13, 210. [Google Scholar] [CrossRef] [PubMed]
- Sampathkumar, P. Middle East respiratory syndrome: What clinicians need to know. Mayo Clin. Proc. 2014, 89, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Infection control standard precautions in health care. 2006. Available online: http://www.who.int/csr/resources/publications/4EPR_AM2.pdf (accessed on 5 October 2018).
- Al-Tawfiq, J.A.; Memish, Z.A. Middle East respiratory syndrome coronavirus: Transmission and phylogenetic evolution. Trends Microbiol. 2014, 22, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Sax, H.; Uçkay, I.; Richet, H.; Allegranzi, B.; Pittet, D. Determinants of Good Adherence to Hand Hygiene Among Healthcare Workers Who Have Extensive Exposure to Hand Hygiene Campaigns. Infect. Control Hosp. Epidemiol. 2007, 28, 1267–274. [Google Scholar] [CrossRef] [PubMed]
- Darawad, M.W.; Al-Hussami, M.; Almhairat, I.I.; Al-Sutari, M. Investigating Jordanian nurses’ handwashing beliefs, attitudes, and compliance. Am. J. Infect. Control. 2012, 40, 643–647. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, W.E.; Reynolds, T.M.; Sessler, C.N.; Edmond, M.B.; Wenzel, R.P. Handwashing compliance by health care workers: The impact of introducing an accessible, alcohol-based hand antiseptic. Arch. Intern Med. 2000, 160, 1017–1021. [Google Scholar] [CrossRef] [PubMed]
- Duggan, J.M.; Hensley, S.; Khuder, S.; Papadimos, T.J.; Jacobs, L. Inverse Correlation Between Level of Professional Education and Rate of Handwashing Compliance in a Teaching Hospital. Infect. Control Hosp. Epidemiol. 2008, 29, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Caglar, S.; Yıldız, S.; Savaser, S. Observation results of handwashing by health-care workers in a neonatal intensive care unit. Int. J. Nurs. Pract. 2010, 16, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Creedon, S.A. Healthcare workers’ hand decontamination practices: Compliance with recommended guidelines. J. Adv. Nurs. 2005, 51, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Allen, I.E.; Seaman, C.A. Likert Scales and Data Analyses. Qual. Prog. 2007, 40, 64–65. [Google Scholar]
- Siegel, J.D.; Rhinehart, E.; Jackson, M.; Chiarello, L.; Health Care Infection Control Practices Advisory Committee. 2007 Guideline for isolation precautions: Preventing transmission of infectious agents in healthcare settings. 2007, 35, S65–S164. [Google Scholar] [CrossRef] [PubMed]
- Programme, I.C. Clean hands are safer hands. World Health, 2006. Available online: http://www.who.int/gpsc/5may/background/5moments/en/ (accessed on 5 October 2018).
- Boyce, J.M.; Pittet, D.; Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America. MMWR Recomm. Rep. 2002, 51, 1–45. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.; Samore, M.; Nafziger, R.; DiRosario, K.; Roghmann, M.; Carmeli, Y. A survey on handwashing practices and opinions of healthcare workers. J. Hosp. Infect. 2000, 45, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Antoniak, J. Handwashing compliance. Can. Nurse 2004, 100, 21–25. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Hospital | Observation | Questionnaire | ||||
|---|---|---|---|---|---|---|
| Physicians | Nurses | Total | Physicians | Nurses | Total | |
| Public | 20 | 14 | 34 | 12 | 3 | 15 |
| Private | 8 | 9 | 17 | 5 | 5 | 10 |
| Security Forces | 16 | 16 | 32 | 12 | 16 | 28 |
| Total | 44 | 39 | 83 | 29 | 24 | 53 |
| Physicians and Nurses | |||||||
|---|---|---|---|---|---|---|---|
| Hand Hygiene | Physicians Descriptive Statistics | Nurses Descriptive Statistics | |||||
| M | SD | M | SD | df | t | p | |
| Before | 0.06 | 0.14 | 0.04 | 0.12 | 81 | 0.69 | 0.49 |
| During | 0.10 | 0.11 | 0.14 | 0.13 | 81 | −1.32 | 0.19 |
| After | 0.10 | 0.16 | 0.11 | 0.15 | 81 | −0.17 | 0.87 |
| Total | 0.27 | 0.27 | 0.29 | 0.26 | 81 | −0.37 | 0.72 |
| Physicians and Nurses | |||||||
|---|---|---|---|---|---|---|---|
| Hand Hygiene | Physicians Descriptive Statistics | Nurses Descriptive Statistics | |||||
| M | SD | M | SD | df | t | p | |
| Before | 3.68 | 1.13 | 4.47 | 0.63 | 51 | −3.04 | 0.004 |
| During | 3.74 | 0.94 | 4.53 | 0.48 | 51 | −3.72 | 0.000 |
| After | 4.17 | 1.01 | 4.65 | 0.54 | 51 | −2.10 | 0.041 |
| Total | 10.19 | 4.57 | 13.65 | 1.51 | 51 | −3.56 | 0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshammari, M.; Reynolds, K.A.; Verhougstraete, M.; O’Rourke, M.K. Comparison of Perceived and Observed Hand Hygiene Compliance in Healthcare Workers in MERS-CoV Endemic Regions. Healthcare 2018, 6, 122. https://doi.org/10.3390/healthcare6040122
Alshammari M, Reynolds KA, Verhougstraete M, O’Rourke MK. Comparison of Perceived and Observed Hand Hygiene Compliance in Healthcare Workers in MERS-CoV Endemic Regions. Healthcare. 2018; 6(4):122. https://doi.org/10.3390/healthcare6040122
Chicago/Turabian StyleAlshammari, Modhi, Kelly A. Reynolds, Marc Verhougstraete, and Mary Kay O’Rourke. 2018. "Comparison of Perceived and Observed Hand Hygiene Compliance in Healthcare Workers in MERS-CoV Endemic Regions" Healthcare 6, no. 4: 122. https://doi.org/10.3390/healthcare6040122
APA StyleAlshammari, M., Reynolds, K. A., Verhougstraete, M., & O’Rourke, M. K. (2018). Comparison of Perceived and Observed Hand Hygiene Compliance in Healthcare Workers in MERS-CoV Endemic Regions. Healthcare, 6(4), 122. https://doi.org/10.3390/healthcare6040122