Comparison of the Effects of Hand Reflexology versus Acupressure on Anxiety and Vital Signs in Female Patients with Coronary Artery Diseases

 and
and 
Abstract
:1. Introduction
2. Methods
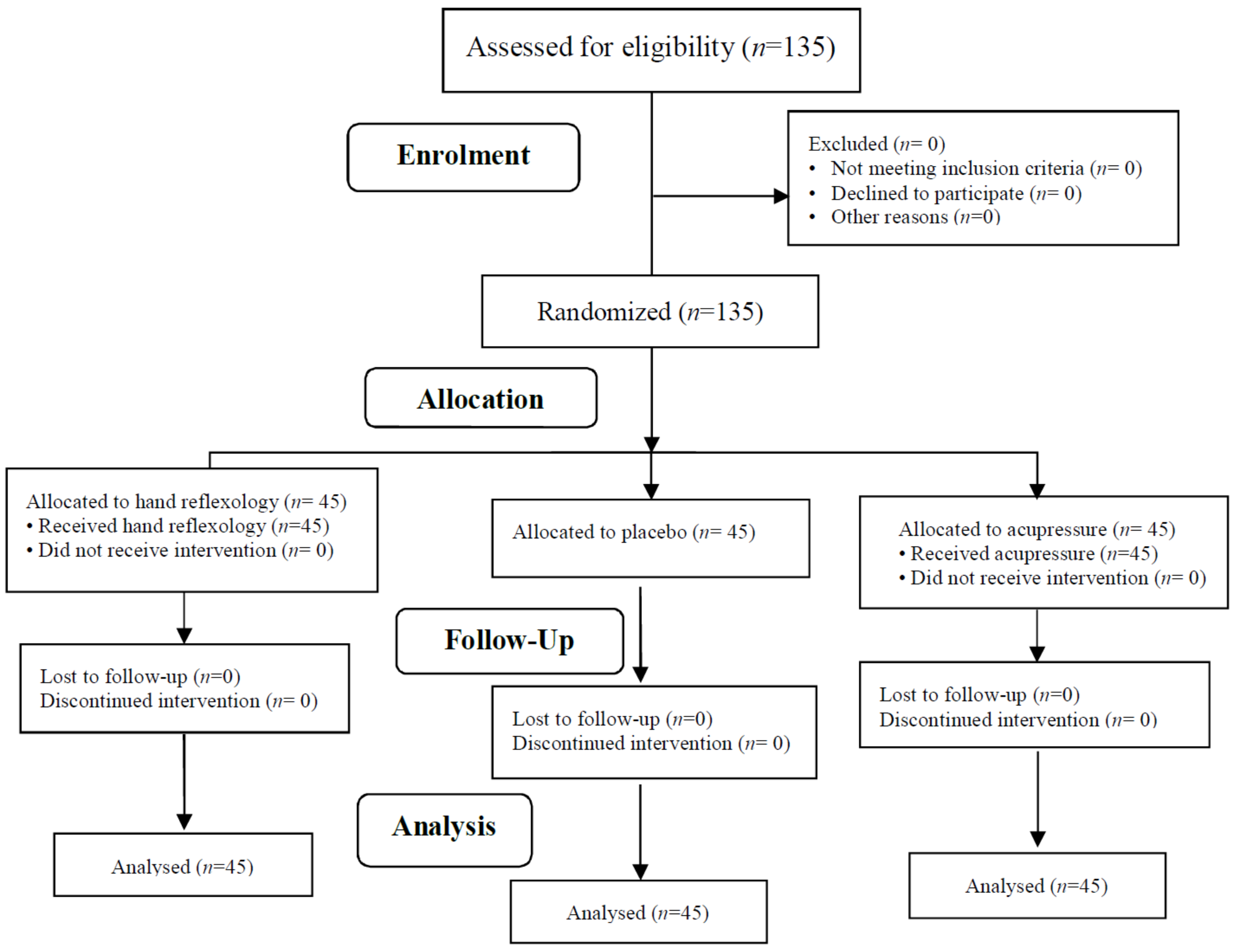
2.1. Design and Sample
2.2. Ethical Considerations
2.3. Eligibility Criteria
2.4. Setting and Participants
2.5. Sample Size
2.6. Random Allocation
2.7. Measurements
2.8. Interventions
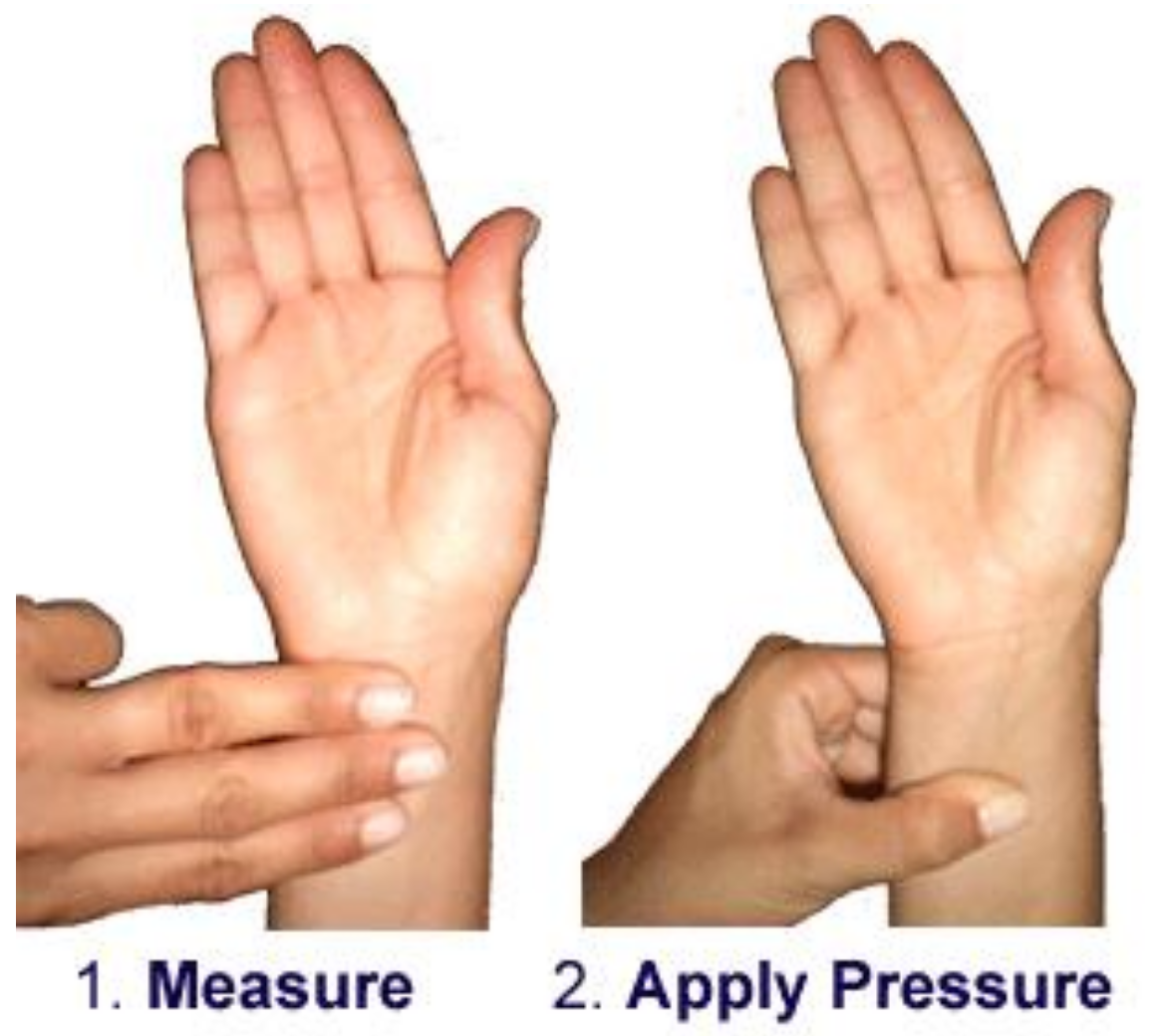
2.9. Acupressure Group
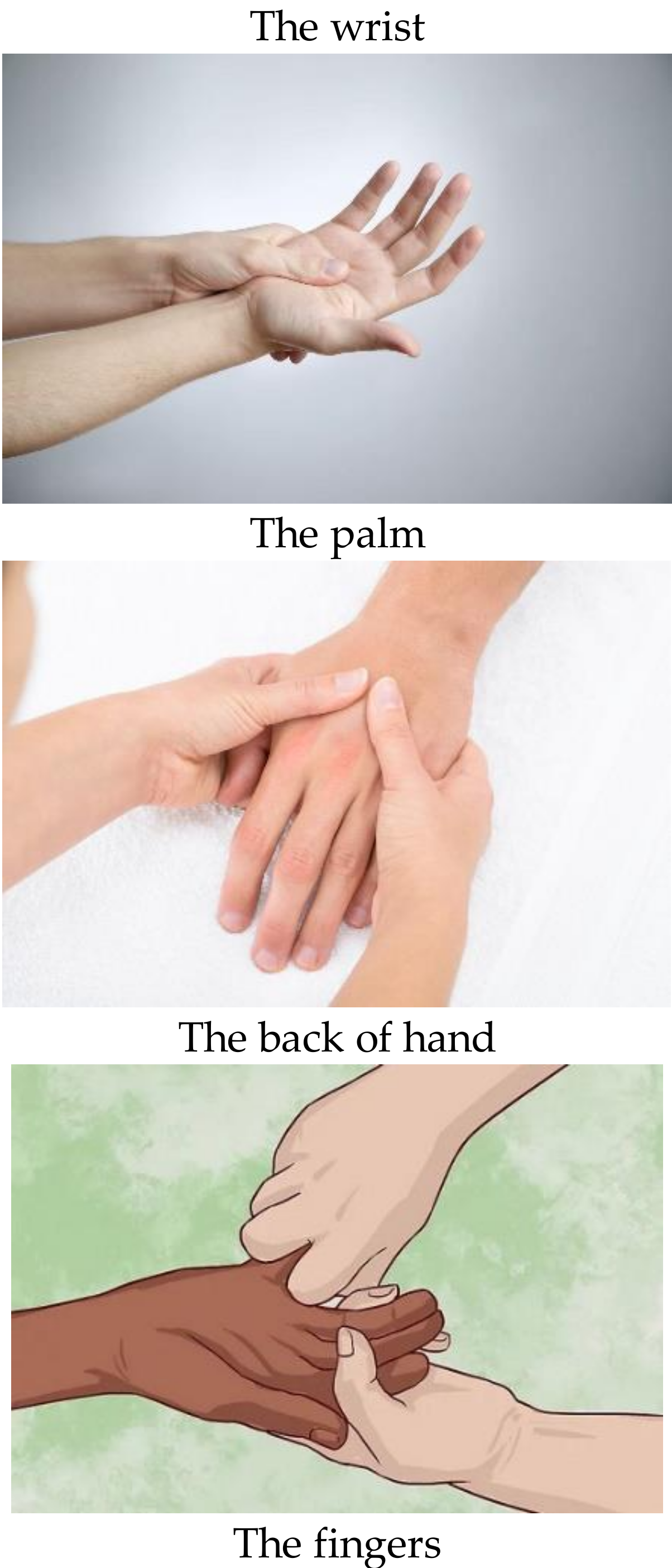
2.10. Hand Reflexology Group
2.11. Placebo Group
2.12. Data Collection and Analysis
2.13. Ethical Approval and Consent to Participate
3. Results
3.1. Demographic Characteristics
3.2. Vital Signs
3.3. Anxiety Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Okrainec, K.; Banerjee, D.K.; Eisenberg, M.J. Coronary artery disease in developing world. Am. Heart J. 2004, 148, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Gomar, F.; Perez-Quilis, C.; Leischik, R.; Lucia, A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann. Transl. Med. 2016, 4, 256. [Google Scholar] [CrossRef] [PubMed]
- Mohseni, J.; Kazemi, T.; Maleki, M.H.; Beydokhti, H. A systematic review on the prevalence of acute myocardial infarction in Iran. Heart Views 2017, 18, 125–132. [Google Scholar] [PubMed]
- Barquera, S.; Pedroza-Tobías, A.; Medina, C.; Hernández-Barrera, L.; Bibbins-Domingo, K.; Lozano, R.; Moran, A.E. Global overview of the epidemiology of atherosclerotic cardiovascular disease. Arch. Med. Res. 2015, 46, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Eng, H.S.; Yean, L.C.; Das, S.; Letchmi, S.; Yee, K.S.; Bakar, R.A.; Choy, C.Y. Anxiety and depression in patients with coronary heart disease: A study in a tertiary hospital. Iran. J. Med. Sci. 2011, 36, 201–206. [Google Scholar] [PubMed]
- Rahimiyan, B.; Jahanshahi, M.; Hajiyan, K.; Nikfar, J.; Nasiri, M. Stressors associated with hospitalization in the stressful cardiac care unit. Crit. Care Nurs. J. 2011, 4, e7098. [Google Scholar]
- Larsen, K.K.; Christensen, B.; Nielsen, T.J.; Vestergaard, M. Post-myocardial infarction anxiety or depressive symptoms and risk of new cardiovascular events or death: A population-based longitudinal study. Psychosom. Med. 2014, 76, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Farach, F.J.; Pruitt, L.D.; Jun, J.J.; Jerud, A.B.; Zoellner, L.A.; Roy-Byrne, P.P. Pharmacological treatment of anxiety disorders: Current treatments and future directions. J. Anxiety Disord. 2012, 26, 833–843. [Google Scholar] [CrossRef] [PubMed]
- Bystritsky, A.; Khalsa, S.S.; Cameron, M.E.; Schiffman, J. Current diagnosis and treatment of anxiety disorders. Pharm. Ther. 2013, 38, 30–57. [Google Scholar]
- Bahrami, T.; Rejeh, N.; Heravi-Karimooi, M.; Vaismoradi, M.; Tadrisi, S.D.; Sieloff, C. Effect of aromatherapy massage on anxiety, depression, and physiologic parameters in older patients with the acute coronary syndrome: A randomized clinical trial. Int. J. Nurs. Pract. 2017, 23, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Shirneshan, E. Cost of Illness Study of Anxiety Disorders for the Ambulatory Adult Population of the United States. Ph.D. Thesis, The University of Tennessee, Health Science Center, Tennessee, TN, USA, 2013. [Google Scholar]
- Dempe, C.; Jünger, J.; Hoppe, S.; Katzenberger, M.L.; Möltner, A.; Ladwig, K.H.; Schultz, J.H. Association of anxious and depressive symptoms with medication nonadherence in patients with stable coronary artery disease. J. Psychosom. Res. 2013, 74, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.J.; Frazier, S.K. The efficacy of acupressure for symptom management: A systematic review. J. Pain Symptom. Manag. 2011, 42, 589–603. [Google Scholar] [CrossRef] [PubMed]
- McGovern, K.; Lockhart, A. Nurse’s Handbook of Alternative & Complementary Therapies; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2003. [Google Scholar]
- Dastgir, F. Combination aromatherapy and acupressure for treating nausea and vomiting. Gastroenterology 2016, 1–14. Available online: https://www.sharn.com/images/art/Nomo-Med-Band-Nausea-Reduction-Study.pdf (accessed on 6 February 2019).
- Tsay, S.L.; Wang, J.C.; Lin, K.C.; Chung, U.L. Effects of acupressure therapy for patients having prolonged mechanical ventilation support. J. Adv. Nurs. 2005, 52, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.S.; Wu, S.C.; Lin, J.G.; Lin, L.C. Effectiveness of acupressure in improving dyspnoea in chronic obstructive pulmonary disease. J. Adv. Nurs. 2004, 45, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Valiee, S.; Bassampour, S.S.; Nasrabadi, A.N.; Pouresmaeil, Z.; Mehran, A. Effect of acupressure on preoperative anxiety: A clinical trial. J. Perianesth. Nurs. 2012, 27, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S. Acupressure and anxity in patients before amputation in poorsina hospital—rasht. Iran. J. Med. Sci. 2007, 15, 101–107. [Google Scholar]
- Hmwe, N.T.; Subramanian, P.; Tan, L.P.; Chong, W.K. The effects of acupressure on depression, anxiety and stress in patients with hemodialysis: A randomized controlled trial. Int. J. Nurs. Stud. 2015, 52, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.; Mirzaei, M.; Rezasoltani, P. The effect of acupressure on anxiety nursing, midwifery and operating room students. J. Guilan Univ. Med. Sci. 2009, 18, 82–89. [Google Scholar]
- Adib-Hajbaghery, M.; Etri, M.; Hosseainian, M.; Mousavi, M.-S. Pressure to the P6 acupoint and post-appendectomy pain, nausea, and vomiting: A randomized clinical trial. J. Caring Sci. 2013, 2, 115–122. [Google Scholar] [PubMed]
- Isoyama, D.; Cordts, E.B.; de Souza van Niewegen, A.M.; de Almeida Pereira de Carvalho, W.; Matsumura, S.T.; Barbosa, C.P. Effect of acupuncture on symptoms of anxiety in women undergoing in vitro fertilisation: A prospective randomised controlled study. Acupunct. Med. 2012, 30, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Torabi, M.; Salavati, M.; Ghahri Sarabi, A.; Pourismail, Z.; Akbarian Baghban, A. Effect of foot reflexology massage and Benson relaxation techniques on anxiety and physiological indexes of patients undergoing coronary heart angiography. Sci. J. Hamadan Nurs. Midwifery Fac. 2012, 20, 63–71. [Google Scholar]
- Xavier, R. Facts on reflexology (foot massage). Nurs. J. India 2007, 98, 11–12. [Google Scholar] [PubMed]
- Schoolmeesters, L.J. The Effect of Reflexology on Joint Pain. Ph.D. Thesis, School of Nursing, Case Western Reserve University, Ohio, OH, USA, 2005. [Google Scholar]
- Ghafari, F.; Pourghaznein, T.; Shamsalinia, A. Effect of sole reflex on pregnant women’s constipation severity. Iran. J. Obstet. IJOGI 2008, 10, 27–38. [Google Scholar]
- Mobini-Bidgoli, M.; Taghadosi, M.; Gilasi, H.; Farokhian, A. The effect of hand reflexology on anxiety in patients undergoing coronary angiography: A single-blind randomized controlled trial. Complement. Ther. Clin. Pract. 2017, 27, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Heidari, F.; Rejeh, N.; Heravi-Karimooi, M.; Tadrisi, S.D.; Vaismoradi, M. Effect of short-term hand reflexology on anxiety in patients before coronary. Eur. J. Integr. Med. 2017, 16, 1–7. [Google Scholar] [CrossRef]
- Gunnarsdottir, T.J.; Jonsdottir, H. Does the experimental design capture the effects of complementary therapy? A study using reflexology for patients undergoing coronary artery bypass graft surgery. J. Clin. Nurs. 2007, 16, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Bagheri-Nesami, M.; Zargar, N.; Gholipour-Baradari, A.; Khalilian, A. The effects of foot reflexology massage on pain and fatigue of patients after coronary artery bypass graft. J. Maz. Univ. Med. Sci. 2012, 22, 52–62. [Google Scholar]
- Mahmoudirad, G.; Ghaedi Mosolo, M.; Bahrami, H. Effect of foot reflexology on anxiety of patients undergoing coronary angiography. J. Crit. Care 2014, 6, 235–242. [Google Scholar]
- Stephenson, N.L.; Swanson, M.; Dalton, J.; Keefe, F.J.; Engelke, M. Partner-delivered reflexology: Effects on cancer pain and anxiety. Oncol. Nurs. Forum 2007, 34, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Abdelaziz, S.H.H.; Mohammed, H.E. Effect of foot massage on postoperative pain and vital signs in breast cancer patient. J. Nurs. Educ. Pract. 2014, 4, 115–124. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushan, R.E. Manual for State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Quek, K.F.; Low, W.Y.; Razack, A.H.; Loh, C.S. Reliability and validity of the spielberger state-trait anxiety inventory (STAI) among urological patients: A Malaysian study. Med. J. Malays. 2004, 59, 258–267. [Google Scholar]
- Mahram, B. Standardization of Spielberger’s State Anxiety Inventory in Mashhad, Iran. Master’s Thesis, Assessment and Measurement in Psychology, Psychology Faculty, Alame Tabatabai University, Dehkadeh-ye-Olympic, Iran, 1994. [Google Scholar]
- Tiedeman, M.E. Anxiety responses of 5- to 11-year-old children during and after hospitalization. J. Pediatr. Health Care 1997, 12, 110–119. [Google Scholar] [CrossRef]
- Byers, D.C. Better Health with Foot Reflexology: The Ingham Method of Reflexology, Recording for the Blind & Dyslexic; Ingham: St. Petersburg, Russia, 2004. [Google Scholar]
- Han Suk, M.; Lee, K. The effect of back massage on degree of pain, state anxiety and quality of sleep of postoperative patients with gastrectomy. Asian Oncol. Nurs. 2011, 16, 1–8. [Google Scholar]
- Rajai, N.; Choopani, N.; Pishgouyi, S.A.H.; Sharififar, S. The effect of acupressure on anxiety of patients candidate for coronary angiography. Mil. Med. Res. 2015, 2, 6–13. [Google Scholar] [CrossRef]
- Weeks, B.P.; Nilsson, U. Music interventions in patients during coronary angiographic procedures: A randomized controlled study of the effect on patients’ anxiety and well-being. Eur. J. Cardiovasc. Nurs. 2011, 10, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Mayo, E. The Human Problems of an Industrial Civilization; Routledge: London, UK, 2003. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Data (Mean ± SD) | Hand Reflexology (n = 45) | Acupressure (n = 45) | Placebo (n = 45) | p-Value |
|---|---|---|---|---|
| Age (years) | 50.16 ± 6.87 | 50.29 ± 6.47 | 48.87 ± 6.72 | * F(2,132) = 0.61, p = 0.54 |
| Duration of stay in the CCU (days) | 2.57 ± 1.05 | 3.04 ± 1.08 | 2.73 ± 1.05 | ** H(2) = 5.01, DF = 2, p = 0.08 |
| Education level | n (%) | n (%) | n (%) | |
| Illiterate | 16 (35.6%) | 10 (22.2%) | 11 (24.5%) | *** X2(6) = 4.03, p = 0.67 |
| Primary school | 15 (33.3%) | 16 (35.6%) | 18 (40.0%) | |
| Pre-high school | 9 (20.0%) | 9 (20.0%) | 10 (22.2%) | |
| High school | 5 (11.1%) | 10 (22.2%) | 6 (13.3%) | |
| Marital status | ||||
| Married | 38 (84.4%) | 37 (82.2%) | 39 (86.7%) | *** X2(2) = 0.33, p = 0.84 |
| Widow | 7 (15.6%) | 8 (17.8%) | 6 (13.3%) | |
| Adequacy of income | ||||
| Yes | 9 (20.0%) | 15 (33.3%) | 15 (33.3%) | *** X2(4) = 4.75, p = 0.31 |
| Somewhat | 30 (66.7%) | 21 (46.7%) | 25 (55.6%) | |
| No | 6 (13.3%) | 9 (20.0%) | 5 (11.1%) | |
| Residence place | ||||
| City | 37 (82.2%) | 34 (75.6%) | 34 (75.6%) | *** X2(2) = 0.77, p = 0.68 |
| Village | 8 (17.8%) | 11 (24.4%) | 11 (24.4%) | |
| Smoking | ||||
| Yes | 8 (17.8%) | 6 (13.3%) | 4 (8.9%) | *** X2(2) = 1.53, p = 0.46 |
| No | 37 (82.2%) | 39 (86.7%) | 41 (91.1%) | |
| History of hospital stay | ||||
| Yes | 33 (73.3%) | 32 (71.1%) | 33 (73.3%) | *** X2(2) = 0.07, p = 0.96 |
| No | 12 (26.7%) | 13 (28.9%) | 12 (26.7%) | |
| History of drug use | ||||
| Yes | 34 (75.6%) | 31 (68.9%) | 33 (73.3%) | *** X2(2) = 0.52, p = 0.77 |
| No | 11 (24.4%) | 14 (31.1%) | 12 (26.7%) |
| Group (Mean ± SD) | Baseline | Immediately after the Intervention | Half an Hour after the Intervention | ** p-Value |
|---|---|---|---|---|
| Hand reflexology (45) Heart rate | 83.49 ± 10.77 | 83.51 ± 9.98 | 82.87 ± 11.04 | Pillai’s Trace = 0.03, F(2,43) = 0.81, p = 0.44 Greenhouse. Geisser, F(2,88)= 0.50, p = 0.60 |
| Acupressure (45) Heart rate | 78.69 ± 13.80 | 77.16 ± 14.05 | 77.42 ± 13.36 | Pillai’s Trace = 0.065, F(2,43) = 1.50, p = 0.23 Greenhouse. Geisser, F(2,88) = 2.30, p = 0.10 |
| Placebo (45) Heart rate | 83.42 ± 15.516 | 82.93 ± 14.35 | 82.51 ± 14.79 | Pillai’s Trace = 0.02, F(2,43) = 0.06, p = 0.53 Greenhouse. Geisser, F(2,88) = 0.57, p = 0.56 |
| * p-value | F(2,132) = 1.86, 0.15 | F(2,132) = 3.31, p =0.03 | F(2,132) = 2.41, p =0.09 | Pillai’s Trace = 0.02, F(2,131) = 1.64, p = 0.19 Greenhouse. Geisser, F(2,264) = 2.25, p = 0.10 |
| Hand reflexology (45) Respiratory rate | 19.40 ± 1.94 | 18.89 ± 2.10 | 18.78 ± 1.46 | Pillai’s Trace = 0.26, F(2,43) = 7.57, p = 0.002 Sphericity Assumed, F(2,88) = 7.50, p = 0.001 |
| Acupressure (45) Respiratory rate | 19.07 ± 1.42 | 18.91 ± 1.10 | 19.04 ± 1.18 | Pillai’s Trace = 0.01, F(2,43) = 0.35, p = 0.70 Sphericity Assumed, F(2,88) = 0.7, p = 0.69 |
| Control (45) Respiratory rate | 19.40 ± 1.83 | 19.29 ± 2.09 | 19.22 ± 1.59 | Pillai’s Trace = 0.02, F(2,43) = 0.58, p = 0.56 Sphericity Assumed, F(2,88) = 0.57, p = 0.56 |
| * p-value | F(2,132) = 0.54, p = 0.58 | F(2,132) = 0.68, p = 0.50 | F(2,132) = 1.11, p =0.33 | Pillai’s Trace = 0.24, F(2,131) = 1.64, p = 0.19 Greenhouse. Geisser, F(2,264) = 2.5, p = 0.12, |
| Hand reflexology (45) Mean arterial pressure | 97.93 ± 19.09 | 100.02 ± 16.42 | 97.27 ± 17.45 | Pillai’s Trace = 0.07, F(2,43) = 1.68, p = 0.19 Sphericity Assumed, F(2,88) = 1.46, p = 0.23 |
| Acupressure (45) Mean arterial pressure | 100.09 ± 18.12 | 102.89 ± 16.66 | 100.31 ± 16.39 | Pillai’s Trace = 0.12, F(2,43) = 3.02, p = 0.06 Greenhouse. Geisser, F(2,88) = 2.46, p = 0.09 |
| Control (45) Mean arterial pressure | 97.47(19.91) | 98.78(20.67) | 97.82(21.31) | Pillai’s Trace = 0.02, F(2,43) = 0.61, p = 0.54 Greenhouse. Geisser, F(2,88) = 0.48, p = 0.59 |
| * p-value | F(2,132) = 0.24, p = 0.78 | F(2,132) = 0.61, p = 0.54 | F(2,132) = 0.34, p = 0.70 | Pillai’s Trace = 0.06, F(2,131) = 1.74, p = 0.10 Greenhouse. Geisser, F(2,264) = 3.89, p = 0.06 |
| Group (Mean ± SD) | Baseline | Immediately after the Intervention | Half an Hour after the Intervention | ** p-Value |
|---|---|---|---|---|
| Hand reflexology (45) State-Anxiety | 49.33 ± 11.30 Moderate to high anxiety | 35.00 ± 9.03 Moderate to low anxiety | 35.29 ± 8.96 Moderate to low anxiety | Pillai’s Trace = 0.86, F(2, 43) = 141.17, p = 0.001 Greenhouse. Geisser, F(2,88) = 258.49, p = 0.001 |
| Acupressure (45) State-Anxiety | 44.42 ± 9.22 Moderate to high anxiety | 32.93 ± 11.66 Moderate to low anxiety | 33.18 ± 11.81 Moderate to low anxiety | Pillai’s Trace = 0.60, F(2, 43) = 32.52, p = 0.001 Greenhouse. Geisser, F(2,88) = 61.13, p = 0.001 |
| Control (45) State-Anxiety | 48.22 ± 10.08 Moderate to high anxiety | 43.91 ± 11.79 Moderate to high anxiety | 43.84 ± 11.77 Moderate to high anxiety | Pillai’s Trace =0.21, F(2,43) =5.93, p = 0.005 Greenhouse. Geisser, F(2,88) = 11.64, p = 0.001 |
| * p-value | F(2,132) = 2.84, p = 0.06 | F(2,132) = 12.87, p = 0.001 POWER = 0.99, η2 = 0.163, Cohen = 0.88, large. effect | F(2,132) = 12.007, p = 0.001 POWER = 0.99, η2 = 0.154, Cohen = 0.85, large. effect | Pillai’s Trace =0.60, F(2,131) = 101.91, p = 0.001 Greenhouse. Geisser, F(2,264) = 198.10, p = 0.001, POWER = 1, η2 = 0.60, Cohen = 2.44, large. effect |
| Hand reflexology (45) Trait-Anxiety | 48.36 ± 7.88 Moderate to high anxiety | 37.89 ± 7.24 Moderate to low anxiety | 37.93 ± 7.19 Moderate to low anxiety | Pillai’s Trace = 0.85, F(2,43) = 128.76, p = 0.001 Sphericity Assumed, F(2,88) = 262.11, p = 0.001 |
| Acupressure (45) Trait-Anxiety | 50.60 ± 9.38 Moderate to high anxiety | 36.93 ± 11.82 Moderate to low anxiety | 36.47 ± 11.70 Moderate to low anxiety | Pillai’s Trace = 0.67, F(2,43) = 44.28, p = 0.001 Sphericity Assumed, F(2,88)= 81.93, p = 0.001 |
| Control (45) Trait-Anxiety | 49.11 ± 9.34 Moderate to high-anxiety | 45.49 ± 11.55 Moderate to high anxiety | 45.58 ± 11.57 Moderate to high anxiety | Pillai’s Trace = 0.20, F(2,43) = 5.40, p = 0.008 Sphericity Assumed, F(2,88) = 9.24, p = 0.001 |
| * p-value | F(2,132) = 0.74, p = 0.47 | F(2,132) = 9.11, p = 0.001 POWER = 0.97, η2 = 0.121, Cohen = 0.74, medium. effect | F(2,132) = 10.01, p =0.001 POWER = 0.98, η2 = 0.132, Cohen = 0.77, medium. effect | Pillai’s Trace =0.59, F(2,131) = 97.68, p = 0.001 Greenhouse. Geisser, F(2,264) = 187.36, p = 0.001, POWER = 1, η2 = 0.58, Cohen = 2.35, large. effect |
| Hand reflexology (45)Total Anxiety | 97.69 ± 17.37 Moderate to high anxiety | 72.89 ± 15.17 Moderate to low anxiety | 73.22 ± 15.13 Moderate to low anxiety | Pillai’s Trace = 0.90, F(2,43) = 195.99, p = 0.001 Sphericity Assumed, F(2,88) = 380.72, p = 0.001 |
| Acupressure (45)Total Anxiety | 95.02 ± 15.79 Moderate to high anxiety | 69.87 ± 21.60 Moderate to low anxiety | 69.64 ± 21.41 Moderate to low anxiety | Pillai’s Trace = 0.67, F(2,43) = 45.38, p = 0.001 Greenhouse. Geisser, F(2,88) = 84.69, p = 0.001 |
| Control (45)Total Anxiety | 97.33 ± 16.45 Moderate to high anxiety | 89.40 ± 21.26 Moderate to high anxiety | 89.42 ± 21.27 Moderate to high anxiety | Pillai’s Trace = 0.20, F(2,43) = 5.63, p = 0.007 Greenhouse. Geisser, F(2,88) = 11.15, p = 0.001 |
| * p-value | F(2,132) = 0.34, p = 0.70 | F(2,132) =12.98, p = 0.001 POWER = 0.97, η2 = 0.164, Cohen = 0.88, large. effect | F(2,132) = 13.14, p = 0.001 POWER = 0.99, η2 = 0.166, Cohen = 0.89, large. effect | Pillai’s Trace = 0.63, F(2,131) = 113.80, p = 0.001 Greenhouse. Geisser, F(2,264) = 226.53, p = 0.001, POWER = 1, η2 = 0.63, Cohen = 2.60, large. effect |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahmani Vasokolaei, Z.; Rejeh, N.; Heravi-Karimooi, M.; Tadrisi, S.D.; Saatchi, K.; Poshtchaman, Z.; Sieloff, C.; Vaismoradi, M. Comparison of the Effects of Hand Reflexology versus Acupressure on Anxiety and Vital Signs in Female Patients with Coronary Artery Diseases. Healthcare 2019, 7, 26. https://doi.org/10.3390/healthcare7010026
Rahmani Vasokolaei Z, Rejeh N, Heravi-Karimooi M, Tadrisi SD, Saatchi K, Poshtchaman Z, Sieloff C, Vaismoradi M. Comparison of the Effects of Hand Reflexology versus Acupressure on Anxiety and Vital Signs in Female Patients with Coronary Artery Diseases. Healthcare. 2019; 7(1):26. https://doi.org/10.3390/healthcare7010026
Chicago/Turabian StyleRahmani Vasokolaei, Zohre, Nahid Rejeh, Majideh Heravi-Karimooi, Seyed Davood Tadrisi, Kiarash Saatchi, Zahra Poshtchaman, Christina Sieloff, and Mojtaba Vaismoradi. 2019. "Comparison of the Effects of Hand Reflexology versus Acupressure on Anxiety and Vital Signs in Female Patients with Coronary Artery Diseases" Healthcare 7, no. 1: 26. https://doi.org/10.3390/healthcare7010026
APA StyleRahmani Vasokolaei, Z., Rejeh, N., Heravi-Karimooi, M., Tadrisi, S. D., Saatchi, K., Poshtchaman, Z., Sieloff, C., & Vaismoradi, M. (2019). Comparison of the Effects of Hand Reflexology versus Acupressure on Anxiety and Vital Signs in Female Patients with Coronary Artery Diseases. Healthcare, 7(1), 26. https://doi.org/10.3390/healthcare7010026