‘One Health’ Actors in Multifaceted Health Systems: An Operational Case for India



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.1.1. General Setting
2.1.2. Specific Setting
2.2. Study Design
2.3. Study Concepts
2.4. Study Sample and Sampling
2.5. Study Data Variables and Data Collection
2.5.1. Phase-I (Qualitative Data Collection)
2.5.2. Phase-II (Quantitative Data Collection)
2.6. Study Analysis
2.6.1. Phase-I (Qualitative Analysis)
2.6.2. Phase-II (Quantitative Analysis)
2.7. Ethics Approval and Consent to Participate
3. Results
3.1. One Health Actors of the Complex Health System
3.2. Interest–Influence Matrix (IIM)
3.3. Issues and Challenges for Intersectoral Collaboration
3.3.1. Perceived Need for ISC
“…Our teamwork is not by need; it’s by demand. During the outbreak, the Collector (prime administrative authority of a district) sensitizes all the actors based on the demand for action. And our collaborative effort was very good during the last outbreak”(Human health actor)
“We need stringent collaboration for the diseases which are not reported currently in the system… and all actors need to understand their respective contribution towards the collaborative work…”(Animal health actor)
“We get information on the outbreak alert from state or center and they tell us what to do and how to proceed.”(Human health actor)
“City administration is different and also the city has limited strength for Animal Husbandry, so we wish to collaborate with district officials…”(Animal health actor)
“We (in Human health) have our own system in place and we do have animal husbandry cell at the corporation level. We at AMC meet them (in Animal Health) regularly; however, if we need help like a laboratory or additive human resources, then only we approach the district animal husbandry department.”(Human health actor)
3.3.2. Challenges for Collaboration
“Within the human health sector, the administrative system is different for the city (urban) and rural…so difficult to collaborate sometime; we directly communicate with the state government regarding any epidemic, outbreak situation…”(Human health actor)
“Animal Husbandry should be the lead for prevention of zoonotic diseases with some support from the human health sectors and transparency is essential for collaboration”(Animal health actor)
“We are in short of human resource, there is a huge shortage of veterinarians and livestock inspectors, with this situation how to collaborate with other sectors…; I am afraid it would increase the burden on our department”(Animal health actor)
“All staffs need to undergo training on the need of collaborations for zoonoses disease management, prevention, control through a common platform at the city level including the private actors”(Human health actor)
“Circular training is essential for the front line health workers, who never studied what zoonoses are! If we train and sensitize our multipurpose healthcare workers, then they could also work on zoonoses prevention, as they have a good reach to every house of the community”(Human health actor)
“Whatever and however we collaborate, if people will not (be) aware enough then prevention of any zoonoses will be difficult, sometimes we provide awareness without the help of a medical doctor…and media may play a vital role in sensitization”(Animal health actor)
3.3.3. Continuing Neglect of Private Actors in Collaborations
“Non-governmental organizations are great helping hands in livestock care, so we should strengthen their effort by providing further training and educating them on various preventive activities.”(Animal health actor)
“We (NGOs) do not get any support (neither financial nor technical) from Govt., so why we will collaborate with them?”(NGO actor)
“Govt. never ask us (private providers) to collaborate for anything, I am trained abroad and I can contribute in many things, but Govt. never provided a scope to work with them….”(Animal health actor)
“Private practitioners are never prioritized to be part of the health system, although we contribute largely to the healthcare and also there is no guideline for involving private actors, thus we lack cooperation!”(Human health actor)
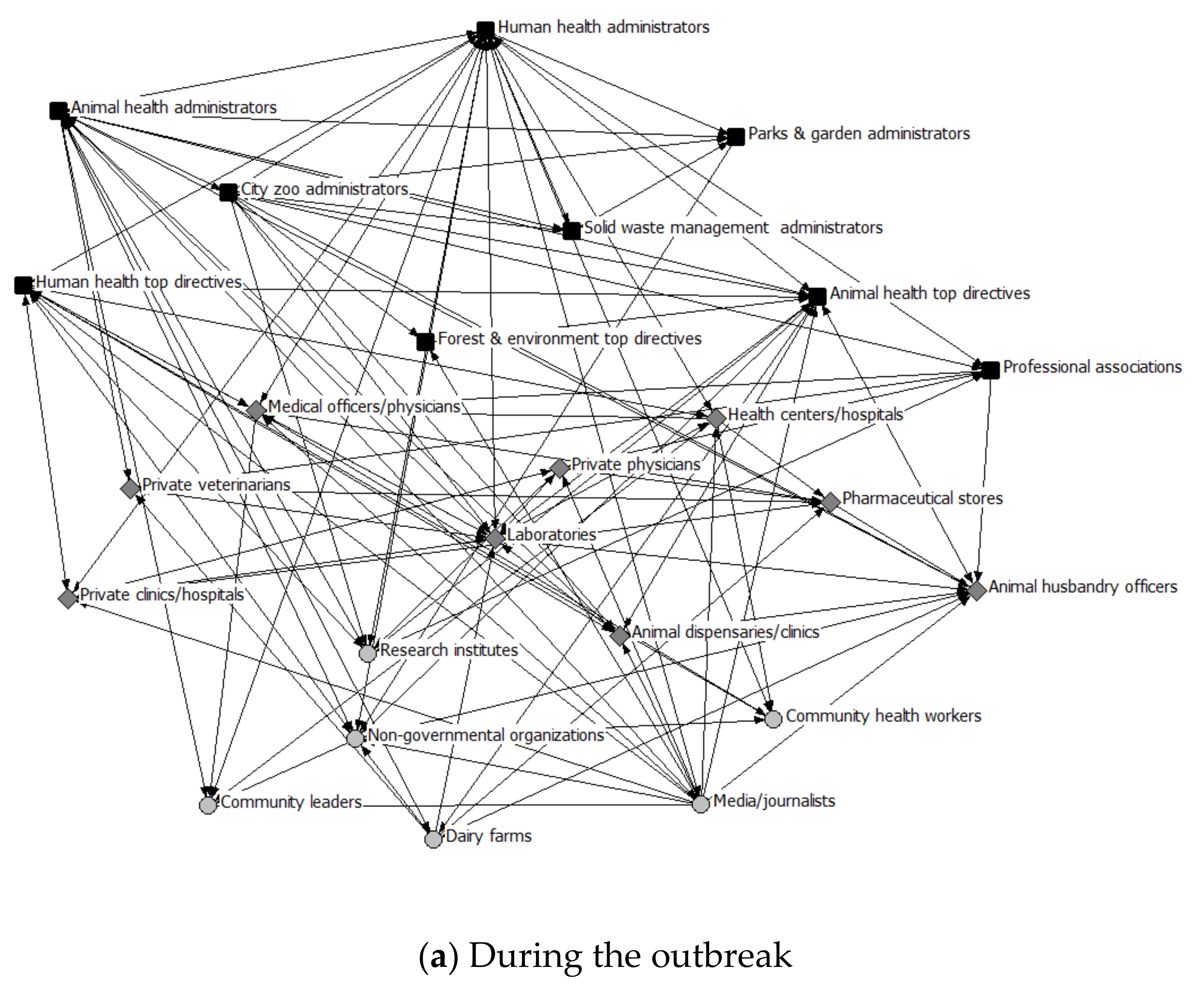
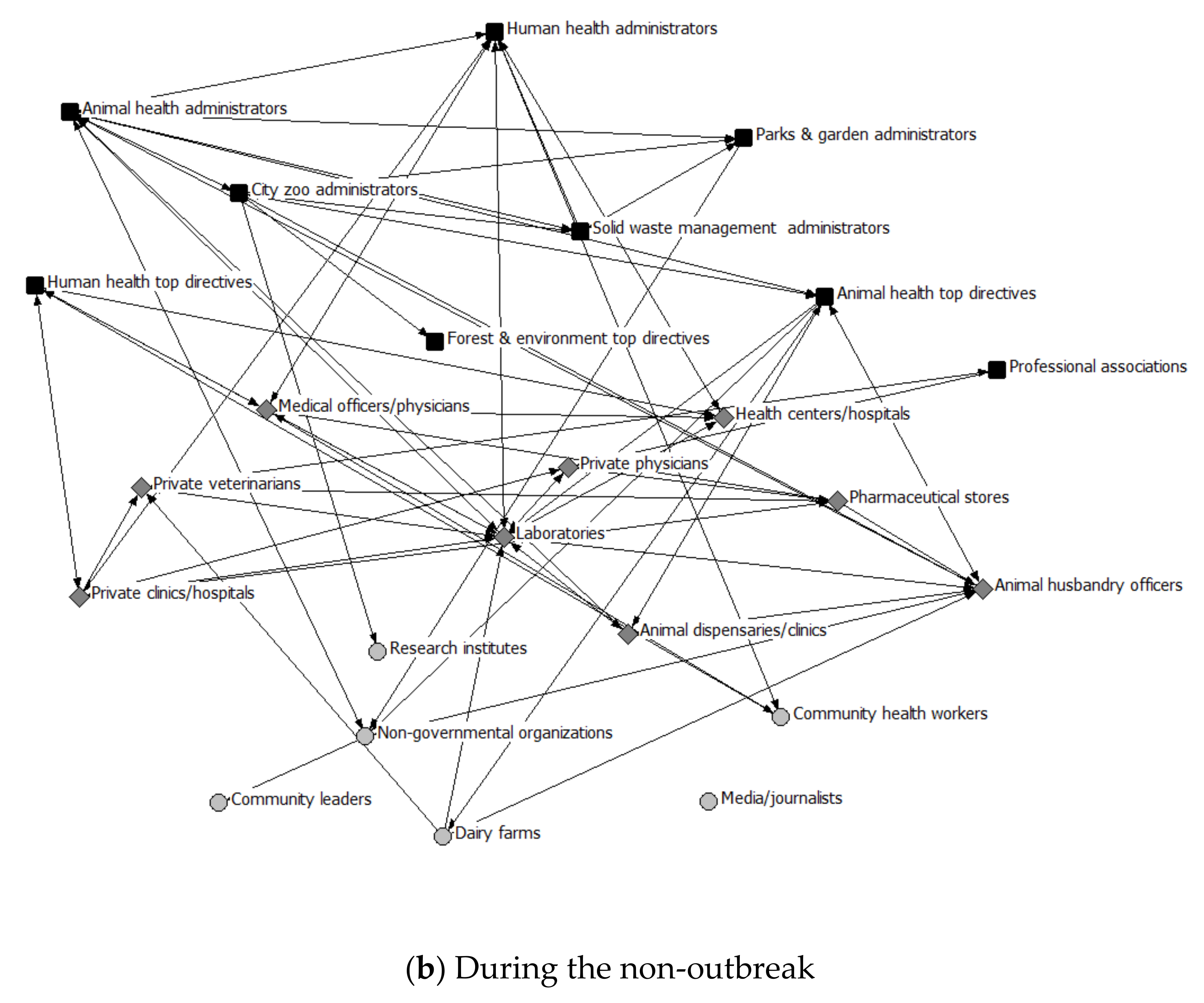
3.4. Interconnectedness of the Actors in the Health System Network
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Availability of Data and Materials
References
- Vesterinen, H.M.; Dutcher, T.V.; Errecaborde, K.M.; Mahero, M.W.; Macy, K.W.; Prasarnphanich, O.-O.; Kassenborg, H.; Yulizar, E.; Fauzi, R.P.; Budayanti, N.S.; et al. Strengthening multi-sectoral collaboration on critical health issues: One health systems mapping and analysis resource toolkit (OH-SMART) for operationalizing One Health. PLoS ONE 2019, 14, e0219197. [Google Scholar] [CrossRef] [PubMed]
- Queenan, K. Roadmap to a One Health agenda 2030. CAB Rev. Perspect Agric. Vet. Sci. Nutr. Nat. Resour. 2017, 12. [Google Scholar] [CrossRef] [Green Version]
- Dhiman, R.; Tiwari, A. Emergence of zoonotic diseases in India: A systematic review. Med Rep. Case Stud. 2018, 3, 3. [Google Scholar] [CrossRef]
- Chatterjee, P.; Kakkar, M.; Chaturvedi, S. Integrating one health in national health policies of developing countries: India’s lost opportunities. Infect. Dis. Poverty 2016, 5, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenzie, J.S.; Dahal, R.; Kakkar, M.; Debnath, N.; Rahman, M.; Dorjee, S.; Naeem, K.; Wijayathilaka, T.; Sharma, B.K.; Maidanwal, N.; et al. One Health research and training and government support for One Health in South Asia. Infect. Ecol. Epidemiol. 2016, 6, 33842. [Google Scholar] [CrossRef]
- Baum, S.E.; Machalaba, C.; Daszak, P.; Salerno, R.H.; Karesh, W.B. Evaluating one health: Are we demonstrating effectiveness? One Health 2017, 3, 5–10. [Google Scholar] [CrossRef]
- Galaz, V.; Leach, M.; Scoones, I.; Christina, S. The Political Economy of One Health Research and Policy. 2015. Available online: https://steps-centre.org/wp-content/uploads/One-Health-wp3.pdf (accessed on 14 June 2020).
- Deliberto, T.J.; Nolte, D.L.; Clay, W. Integrative approaches to disease control: The value of international collaborations. In Proceedings of the Compendium of the OIE Global Conference on Wildlife, Paris, France, 23–25 February 2011; p. 7. [Google Scholar]
- Gongal, G. One Health approach in the South East Asia region: Opportunities and challenges. Curr. Top. Microbiol. Immunol. 2013, 366, 113. [Google Scholar] [CrossRef]
- Dahal, R.; Upadhyay, A.; Ewald, B. One Health in South Asia and its challenges in implementation from stakeholder perspective. Vet. Rec. 2017, 181, 626. [Google Scholar] [CrossRef]
- EClinicalMedicine. Emerging zoonoses: A one health challenge. EClinicalMedicine 2020, 19, 100300. [Google Scholar] [CrossRef]
- FAO-OIE-WHO. Taking a Multisectoral One Health Approach: A Tripartite Guide to Addressing Zoonotic Diseases in Countries. 2019. Available online: http://www.fao.org/3/ca2942en/ca2942en.pdf (accessed on 2 January 2020).
- Sekar, N.; Shah, N.K.; Abbas, S.S.; Kakkar, M. Research options for controlling zoonotic disease in India, 2010–2015. PLoS ONE 2011, 6, e17120. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, P.; Bhaumik, S.; Chauhan, A.S.; Kakkar, M. Protocol for developing a database of zoonotic disease research in India (DoZooRI). BMJ Open 2017, 7, e017825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varma, G.B.S.N.P. India needs “One Health” policy to eradicate zoonotic diseases. Nat. India 2014, 10. [Google Scholar] [CrossRef]
- John, T.J.; Dandona, L.; Sharma, V.P.; Kakkar, M. Continuing challenge of infectious diseases in India. Lancet 2011, 377, 252–269. [Google Scholar] [CrossRef]
- Hyder, A.; Syed, S.; Puvanachandra, P.; Bloom, G.; Sundaram, S.; Mahmood, S.; Iqbal, M.; Hongwen, Z.; Ravichandran, N.; Oladepo, O.; et al. Stakeholder analysis for health research: Case studies from low—And middle-income countries. Public Health 2010, 124, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Kurian, A.; Dandapat, P.; Jacob, S.; Francis, J. Ranking of zoonotic diseases using composite index method: An illustration in Indian context. Indian J. Anim. Sci. 2014, 84, 357–363. [Google Scholar]
- World Organization for Animal Health (OIE). Animal health and biodiversity: Preparing for the future. In Proceedings of the OIE Global Conference on Wildlife, Paris, France, 23–25 February 2011. [Google Scholar]
- Lee, K.; Brumme, Z.L. Operationalizing the One Health approach: The global governance challenges. Health Policy Plan. 2013, 28, 778–785. [Google Scholar] [CrossRef] [Green Version]
- Abimbola, S.; Negin, J.; Jan, S.; Martiniuk, A. Towards people-centred health systems: A multi-level framework for analysing primary health care governance in low-and middle-income countries. Health Policy Plan. 2014, 29, 29–39. [Google Scholar] [CrossRef]
- Abimbola, S.; Negin, J.; Martiniuk, A.L.; Jan, S. Institutional analysis of health system governance. Inst. Anal. Health Syst. Gov. 2017, 32, 1337–1344. [Google Scholar] [CrossRef]
- Horwath, J.; Morrison, T. Collaboration, integration and change in children’s services: Critical issues and key ingredients. Child Abus. Negl. 2007, 31, 55–69. [Google Scholar] [CrossRef]
- Shigayeva, A.; Atun, R.; McKee, M.; Coker, R. Health systems, communicable diseases and integration. Health Policy Plan. 2010, 25, 4–20. [Google Scholar] [CrossRef] [Green Version]
- Axelsson, R.; Axelsson, S.B. Integration and collaboration in public health—A conceptual framework. Int. J. Health Plan. Manag. 2006, 21, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.C.; Sambo, L.G. Health systems research and critical systems thinking: The case for partnership. Syst. Res. Behav. Sci. 2020, 37, 3–22. [Google Scholar] [CrossRef] [Green Version]
- Siddiqi, S.; Masud, T.I.; Nishtar, S.; Peters, D.H.; Sabri, B.; Bile, K.M.; Jama, M.A. Framework for assessing governance of the health system in developing countries: Gateway to good governance. Health Policy 2009, 90, 13–25. [Google Scholar] [CrossRef] [PubMed]
- National Centre for Disease Control (NCDC), Division of Zoonotic Diseases Programmes (DZDP). Directorate General of Health Services, Ministry of Health & Family Welfare, Government of India. 2019. Available online: https://ncdc.gov.in/index1.php?lang=1&level=1&sublinkid=105&lid=56 (accessed on 12 February 2020).
- National Animal Disease Control Programme, Department of Animal Husbandry and Dairying. Ministry of Fisheries, Animal Husbandry & Dairying, Government of India. 2019. Available online: http://dahd.nic.in/ (accessed on 12 February 2020).
- Gandhi, S.; Dave, P.; Patel, G.; Khatri, H.; Shah, N.; Mishra, U. An epidemiological investigation of a multisource outbreak of crimean-Congo hemorrhagic fever in Gujarat. J. Commun. Dis. 2011, 43, 161–167. [Google Scholar]
- The Times of India. Swine flu in Ahmedabad: 408 new cases and 10 deaths in September 2018. Times of India, 26 September 2018. Available online: https://timesofindia.indiatimes.com/city/ahmedabad/408-swine-flu-cases-10-deaths-this-september/articleshow/65956967.cms (accessed on 15 January 2020).
- Integrated Disease Surveillance Program (IDSP). Bird flu scare: Foresters order autopsies of birds in Ahmedabad, Gujarat. Times of India, 3 January 2017. Available online: https://timesofindia.indiatimes.com/city/ahmedabad/bird-flu-scare-foresters-order-autopsies-of-birds/articleshow/56300935.cms (accessed on 16 January 2020).
- Achievements of Ahmedabad Municipal Corporation. Available online: https://ahmedabadcity.gov.in/portal/jsp/Static_pages/amc_awards.jsp (accessed on 12 February 2020).
- Gupta, I.; Bhatia, M. The Indian health care system. Institute of Economics Growth and London School of Economics. 2013. Available online: https://www.commonwealthfund.org/international-health-policy-center/countries/india (accessed on 20 March 2020).
- Ahmedabad Municipal Corporation. Ahmedabad City. Available online: https://ahmedabadcity.gov.in/portal/jsp/Static_pages/about_us.jsp (accessed on 2 January 2018).
- Yasobant, S.; Bruchhausen, W.; Saxena, D.; Falkenberg, T. Convergence model for effectual prevention and control of zoonotic diseases: A health system study on “One Health” approach in Ahmedabad, India. Health Res. Policy Syst. 2018, 16, 124. [Google Scholar] [CrossRef]
- Asokan, G.V.; Asokan, V.; Fedorowicz, Z.; Tharyan, P. Use of a systems approach and evidence-based One Health for zoonoses research. J. Evid. Based Med. 2011, 4, 62–65. [Google Scholar] [CrossRef]
- Luke, D.A.; Harris, J.K. Network analysis in public health: History, methods, and applications. Annu. Rev. Public Health 2007, 28, 69–93. [Google Scholar] [CrossRef] [Green Version]
- Young, D.; Borland, R.; Coghill, K. An actor-network theory analysis of policy innovation for smoke-free places: Understanding change in complex systems. Am. J. Public Health 2010, 100, 1208–1217. [Google Scholar] [CrossRef]
- ATLAS.ti, version 8 [Computer Software]; ATLAS.ti Scientific Software Development GmbH: Berlin, Germany, 2017.
- Varvasovszky, Z.; Brugha, R. How to do (or not to do) A stakeholder analysis. Health Policy Plan. 2000, 15, 338–345. [Google Scholar] [CrossRef]
- Bryson, J.M. What to do when Stakeholders matter. Public Manag. Rev. 2004, 6, 21–53. [Google Scholar] [CrossRef]
- Borgatti, S.P.; Everett, M.G.; Freeman, L. Ucinet for Windows: Software for Social Network Analysis (UCINET version 6) [Computer Software]; Analytic Technologies: Lexington, KY, USA, 2002. [Google Scholar]
- R version 3.4.1. [Computer Software]; A language and environment for statistical computing; R Core Team: New Zealand, 2017.
- Pelletier, D.; Gervais, S.; Hafeez-ur-Rehman, H.; Sanou, D.; Tumwine, J. Boundary-spanning actors in complex adaptive governance systems: The case of multisectoral nutrition. Int. J. Health Plan. Manag. 2018, 33, e293–e319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bednarek, A.T.; Wyborn, C.; Cvitanovic, C.; Meyer, R.; Colvin, R.M.; Addison, P.F.E.; Close, S.L.; Curran, K.; Farooque, M.; Goldman, E.; et al. Boundary spanning at the science–policy interface: The practitioners’ perspectives. Sustain. Sci. 2018, 13, 1175–1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dotson David, V. Boundary-spanning actors in urban 4-H: An action research case study. J. High. Educ. Outreach Engag. 2014, 18, 104, ISSN:1534. [Google Scholar]
- Burris, S.; Hancock, T.; Lin, V.; Herzog, A. Emerging strategies for healthy urban governance. J. Urban Health 2007, 84, 154–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plochg, T.; Delnoij, D.M.J.; Hogervorst, W.V.G.; van Dijk, P.; Belleman, S.; Klazinga, N.S. Local health systems in 21st century: Who cares?—An exploratory study on health system governance in Amsterdam. Eur. J. Public Health 2006, 16, 559–564. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.; Rasheed Sulaiman, V.; Natchimuthu, K.; Ramkumar, S.; Sasidhar, P.; Gandhi, R. Improvement of veterinary services delivery in India. Rev. Sci. Tech. Off. Int. 2015, 34. [Google Scholar] [CrossRef]
- Rao, K.D.; Bhatnagar, A.; Berman, P. So many, yet few: Human resources for health in India. Hum. Resour. Health 2012, 10, 19. [Google Scholar] [CrossRef] [Green Version]
- Murphy, S.C.; Negron, M.E.; Pieracci, E.G.; Deressa, A.; Bekele, W.; Regassa, F.; Wassie, B.A.; Afera, B.; Hajito, K.W.; Walelign, E.; et al. One Health collaborations for zoonotic disease control in Ethiopia. Revue Scientifique Technique 2019, 38, 51–60. [Google Scholar] [CrossRef]
- British Veterinary Association. One Health: Collaboration on all levels is key, concludes joint meeting. Vet. Rec. 2014, 174, 644. [Google Scholar] [CrossRef]
- Thadani, K.B. Public private partnership in the health sector: Boon or Bane. Procedia Soc. Behav. Sci. 2014, 157, 307–316. [Google Scholar] [CrossRef]
- Das, A. Public-private partnerships for providing healthcare services. Indian J. Med Ethics 2007, 4, 174–175. [Google Scholar] [CrossRef] [PubMed]
- Bhat, R. Issues in health: Public-private partnership. Econ. Polit. Wkly. 2000, 35, 4706–4716. [Google Scholar] [CrossRef]
- Yadav, V.; Kumar, S.; Balasubramaniam, S.; Srivastava, A.; Pallipamula, S.; Memon, P.; Singh, D.; Bhargava, S.; Sunil, G.A.; Sood, B.; et al. Facilitators and barriers to participation of private sector health facilities in government-led schemes for maternity services in India: A qualitative study. BMJ Open 2017, 7, e017092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spencer, J.; McRobie, E.; Dar, O.; Rahman-Shepherd, A.; Hasan, N.; Hanefeld, J.; Khan, M. Is the current surge in political and financial attention to One Health solidifying or splintering the movement? BMJ Glob. Health. 2019, 4, e001102. [Google Scholar] [CrossRef] [PubMed]
- Söderlund, N.; Mendoza-Arana, P.; Goudge, J. The New Public/Private Mix in Health: Exploring the Changing Landscape; Alliance for Health Policy and Systems Research: Geneva, Switzerland, 2003. [Google Scholar]
- Johnston, L.M.; Finegood, D.T. Cross-sector partnerships and public health: Challenges and opportunities for addressing obesity and noncommunicable diseases through engagement with the private sector. Annu. Rev. Public Health 2015, 36, 255–271. [Google Scholar] [CrossRef] [PubMed]
- Kuruvilla, S.; Hinton, R.; Boerma, T.; Bunney, R.; Casamitjana, N.; Cortez, R.; Fracassi, P.; Franz-Vasdeki, J.; Helldén, D.; McManus, J.; et al. Business not as usual: How multisectoral collaboration can promote transformative change for health and sustainable development. BMJ (Online) 2018, 363. [Google Scholar] [CrossRef] [Green Version]
- Willis, C.D.; Greene, J.K.; Abramowicz, A.; Riley, B.L. Strengthening the evidence and action on multi-sectoral partnerships in public health: An action research initiative. Health promotion and chronic disease prevention in Canada. Res. Policy Pract. 2016, 36, 101–111. [Google Scholar] [CrossRef] [Green Version]
- USAID-SPIRNG. Operationalizing Multi-Sectoral Coordination and Collaboration for Improved Nutrition: Recommendations from an in-Depth Assessment of Three Countries’ Experiences; Feed the Future: Washington, DC, USA, 2016. [Google Scholar]
- Degeling, C.; Johnson, J.; Kerridge, I.; Wilson, A.; Ward, M.; Stewart, C.; Gilbert, G. Implementing a One Health approach to emerging infectious disease: Reflections on the socio-political, ethical and legal dimensions. BMC Public Health 2015, 15, 1307. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine, US Committee. Guidance for Establishing Standards of Care for Use in Disaster Situations; Altevogt, B.M., Stroud, C., Hanson, S.L., Hanfling, D., Gostin, L.O., Eds.; National Academies Press: Washington, DC, USA, 2009; ISBN 978-0-309-14430-8. [Google Scholar]
- Menon, V.C. India—National disaster and epidemic preparedness. Int. J. Infect. Dis. 2016, 45, 12. [Google Scholar] [CrossRef] [Green Version]
- Mazet, J.A.K.; Uhart, M.M.; Keyyu, J.D. Stakeholders in One Health. Revue Scientifique Technique 2014, 33, 443–452. [Google Scholar] [CrossRef] [Green Version]
- Plianbangchang, S. International leadership for the control of disease outbreaks relating to “One Health”. J. Health Res. 2018, 32, 106–111. [Google Scholar] [CrossRef] [Green Version]
- Stephen, C.; Stemshorn, B. Leadership, governance and partnerships are essential One Health competencies. One Health 2016, 2, 161–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hueston, W.D.; van Klink, E.G.M.; Rwego, I.B. One Health Leadership and Policy. In Beyond One Health; John Wiley & Sons: Hoboken, NJ, USA, 2018; pp. 267–278. [Google Scholar]
- Eussen, B.G.M.; Schaveling, J.; Dragt, M.J.; Blomme, R.J. Stimulating collaboration between human and veterinary health care professionals. BMC Vet. Res. 2017, 13, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Giusti, M.; Barbato, D.; Lia, L.; Colamesta, V.; Lombardi, A.M.; Cacchio, D.; Villari, P.; La Torre, G. Collaboration between human and veterinary medicine as a tool to solve public health problems. Lancet Planet. Health 2019, 3, e64–e65. [Google Scholar] [CrossRef] [Green Version]
- Speare, R.; Mendez, D.; Judd, J.; Reid, S.; Tzipori, S.; Massey, P.D. Willingness to consult a veterinarian on physician’s advice for zoonotic diseases: A formal role for veterinarians in medicine? PLoS ONE 2015, 10, e0131406. [Google Scholar] [CrossRef] [Green Version]
- Shanko, K.; Kemal, J.; Kenea, D. A Review on confronting zoonoses: The role of veterinarian and physician. J. Vet. Sci. Technol. 2014, 6, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Matthiessen, P.W.; Sansone, R.A.; Meier, B.P.; Gaither, G.A.; Shrader, J. Zoonotic diseases and at-risk patients: A survey of veterinarians and physicians. AIDS 2003, 17, 1404–1406. [Google Scholar] [CrossRef] [PubMed]
- Hill, W.A.; Petty, G.C.; Erwin, P.C.; Souza, M.J. A survey of Tennessee veterinarian and physician attitudes, knowledge, and practices regarding zoonoses prevention among animal owners with HIV infection or AIDS. J. Am. Vet. Med. Assoc. 2012, 240, 1432–1440. [Google Scholar] [CrossRef]
- Courtenay, M.; Sweeney, J.; Zielinska, P.; Brown Blake, S.; La Ragione, R. One Health: An opportunity for an interprofessional approach to healthcare. J. Interprof. Care 2015, 29, 641–642. [Google Scholar] [CrossRef]
- Berrian, A.M.; Smith, M.H.; van Rooyen, J.; Martínez-López, B.; Plank, M.N.; Smith, W.A.; Conrad, P.A. A community-based One Health education program for disease risk mitigation at the human-animal interface. One Health 2018, 5, 9–20. [Google Scholar] [CrossRef]
- Conrad, P.A.; Meek, L.A.; Dumit, J. Operationalizing a One Health approach to global health challenges. Comp. Immunol. Microbiol. Infect. Dis. 2013, 36, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Kriegner, S.; Ottersen, T.; Røttingen, J.A.; Gopinathan, U. Promoting intersectoral collaboration through the evaluations of public health interventions: Insights from key informants in 6 European countries. Int. J Health Policy Manag. 2020, 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bennett, S.; Glandon, D.; Rasanathan, K. Governing multisectoral action for health in low-income and middle-income countries: Unpacking the problem and rising to the challenge. BMJ Global Health 2018, 3, e000880. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Health System Level | One Health Actors | Status in the Interest–Influence Matrix (IIM) |
|---|---|---|
| Administrative level $ | Human health administrators # Animal health administrators § Parks & Gardens administrators Solid waste management administrators Professional associations City zoo administrators | Player Subject Crowd Crowd Context setter Crowd |
| Provider level | Health centers/hospitals Medical officers/physicians Private clinics/hospitals Private physicians & infectious disease specialists Nurses/Mid-Wives Pharmaceutical stores Laboratories Animal dispensaries/clinics Government veterinarians Private veterinarians Livestock inspectors/Animal workers | Player Subject Subject Crowd Crowd Crowd Crowd Player Subject Subject Crowd |
| Community level | Community health workers Non-governmental organizations Community leaders Research institutes Media/journalists Households and community Dairy farms Police | Subject Crowd Crowd Crowd Crowd Crowd Crowd Crowd |
| Network Measures | Sub-Groups | During Outbreak | During Non-Outbreak | ||||
|---|---|---|---|---|---|---|---|
| Admin | Provider | Community | Admin | Provider | Community | ||
| Average degree | Overall | 2.652 | 1.406 | ||||
| Admin | 5.833 | 3.001 | 1.500 | 2.667 | 1.417 | 0.417 | |
| Provider | 3.2222 | 0.556 | 3.111 | 0.222 | |||
| Community | 1.800 | 0.600 | |||||
| Network density | Overall | 0.328 | 0.163 | ||||
| Admin | 0.530 | 0.333 | 0.136 | 0.242 | 0.157 | 0.038 | |
| Provider | 0.403 | 0.069 | 0.389 | 0.028 | |||
| Community | 0.450 | 0.150 | |||||
| Degree of centralization | Overall | 0.424 | 0.257 | ||||
| Admin | 0.564 | 0.556 | 0.382 | 0.473 | 0.205 | 0.173 | |
| Provider | 0.625 | 0.232 | 0.607 | 0.125 | |||
| Community | 0.183 | 0.167 | |||||
| Variables | N = 66 (%) | |||||
|---|---|---|---|---|---|---|
| Type of provider | ||||||
| Human health | 49 (74.2) | |||||
| Animal health | 17 (25.8) | |||||
| Gender | ||||||
| Male | 43 (65.2) | |||||
| Female | 23 (34.8) | |||||
| Education | ||||||
| Bachelor degree (MBBS/BVMS) | 55 (83.7) | |||||
| Specialist (MD/MVM) | 11 (16.6) | |||||
| Total years of professional experience (years) | 12 ± 8 | |||||
| Work setting | ||||||
| Government | 49 (74.2) | |||||
| Private/Non-governmental | 17 (25.8) | |||||
| Ever involved in inter-sectoral collaborative activities | ||||||
| Outbreak management | 18 (27.3) | |||||
| Advocacy/Administrative | 11 (16.7) | |||||
| Reasons for lack of collaboration | ||||||
| No policy/guidelines/opportunity | 16 (24.2) | |||||
| Lack of knowledge | 12 (18.2) | |||||
| Not at all required | 38 (57.6) | |||||
| Potential actor who can bridge the human and animal health system | ||||||
| At the administrative level | 19 (28.8) | |||||
| At the provider level | 28 (42.4) | |||||
| At the community level | 42 (63.6) | |||||
| Ever received any training on zoonoses | 39 (59.1) | |||||
| Ever attended health campaigns related to zoonoses | 43 (65.2) | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yasobant, S.; Bruchhausen, W.; Saxena, D.; Falkenberg, T. ‘One Health’ Actors in Multifaceted Health Systems: An Operational Case for India. Healthcare 2020, 8, 387. https://doi.org/10.3390/healthcare8040387
Yasobant S, Bruchhausen W, Saxena D, Falkenberg T. ‘One Health’ Actors in Multifaceted Health Systems: An Operational Case for India. Healthcare. 2020; 8(4):387. https://doi.org/10.3390/healthcare8040387
Chicago/Turabian StyleYasobant, Sandul, Walter Bruchhausen, Deepak Saxena, and Timo Falkenberg. 2020. "‘One Health’ Actors in Multifaceted Health Systems: An Operational Case for India" Healthcare 8, no. 4: 387. https://doi.org/10.3390/healthcare8040387
APA StyleYasobant, S., Bruchhausen, W., Saxena, D., & Falkenberg, T. (2020). ‘One Health’ Actors in Multifaceted Health Systems: An Operational Case for India. Healthcare, 8(4), 387. https://doi.org/10.3390/healthcare8040387