Nurses’ Workplace Conditions Impacting Their Mental Health during COVID-19: A Cross-Sectional Survey Study





Abstract
:1. Introduction
1.1. Literature Review
1.2. Theoretical Framework
2. Materials and Methods
2.1. Data Collection and Sample
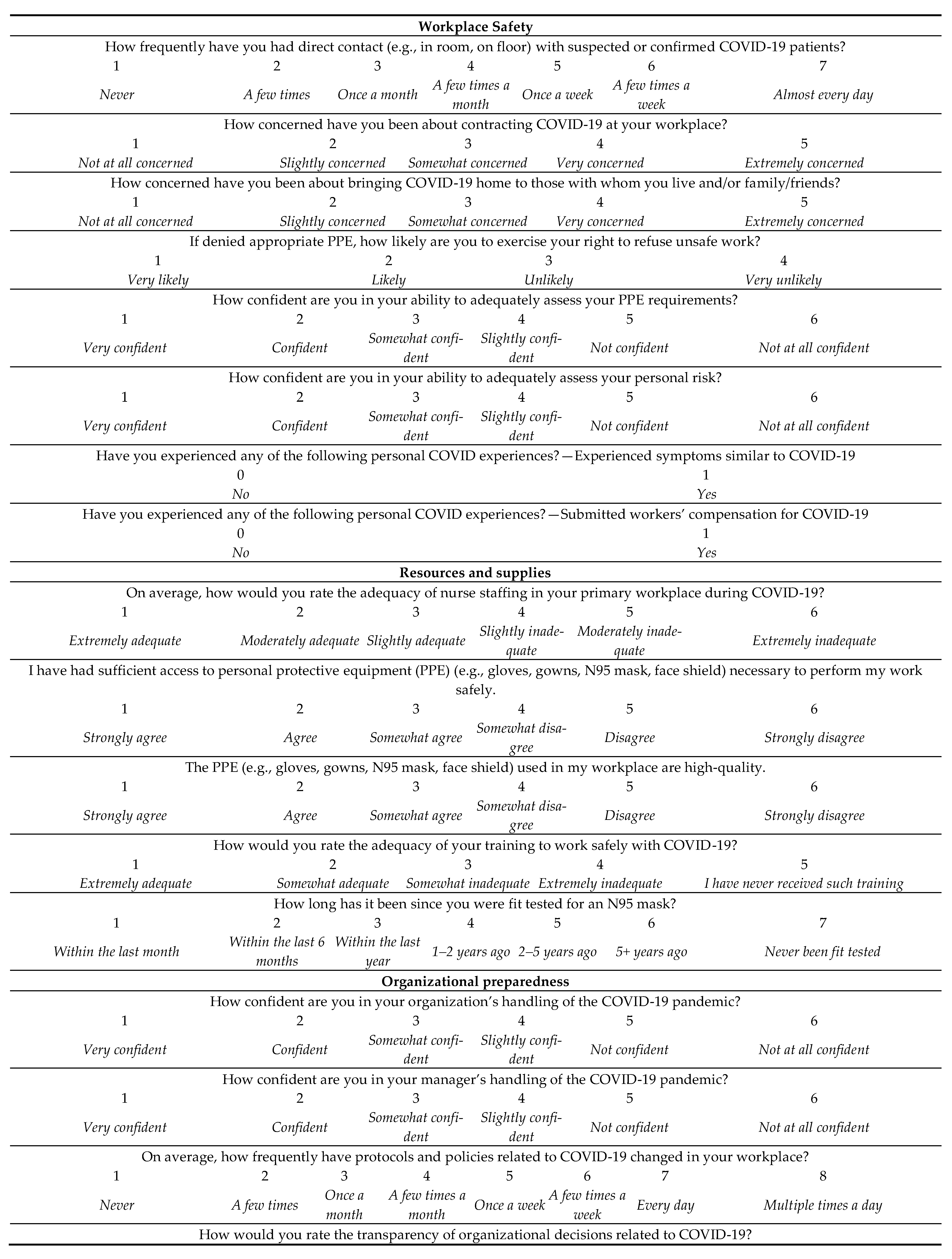
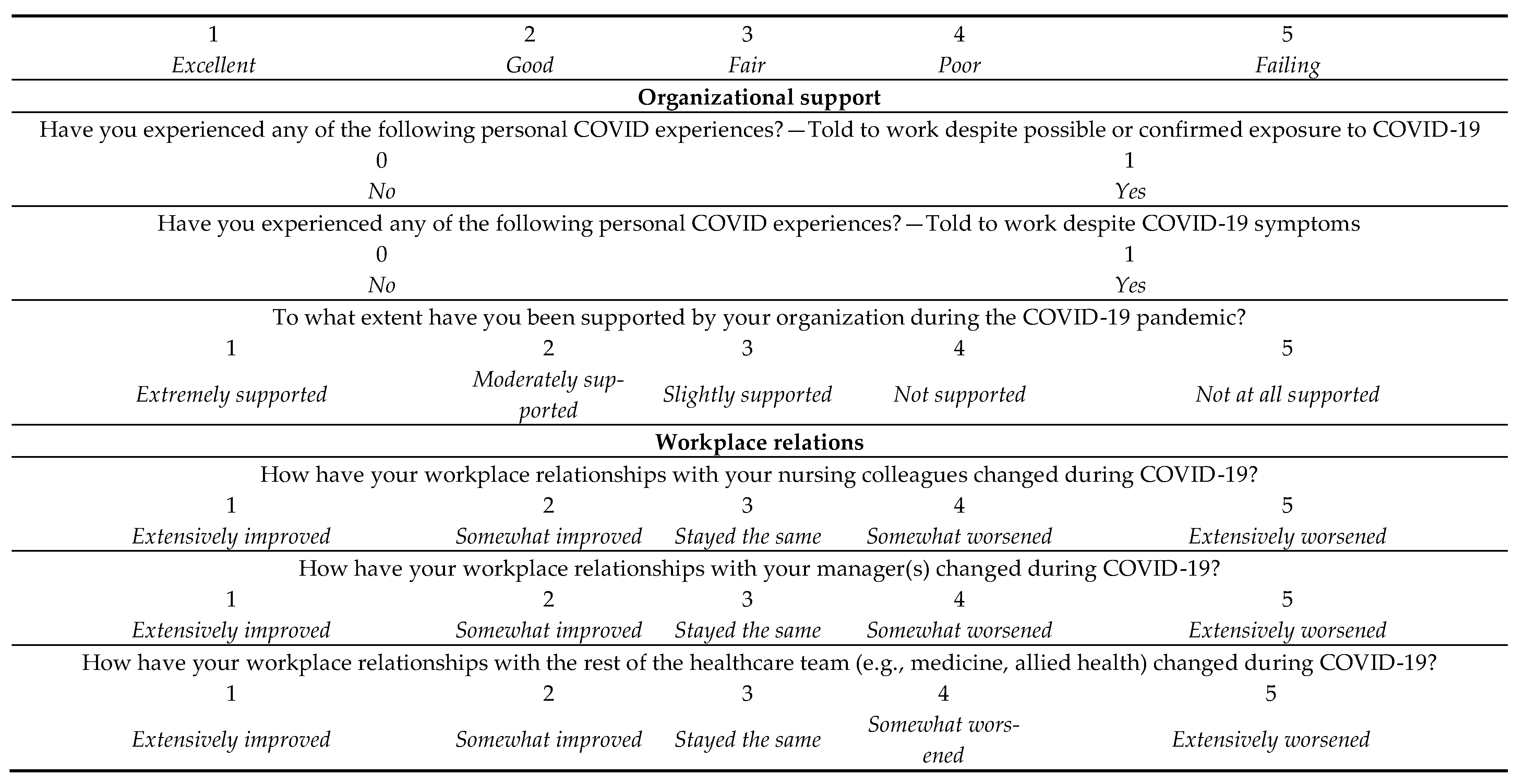
2.2. Measures
2.2.1. Outcome Variables
2.2.2. Key Predictors
2.2.3. Control Variables
2.3. Analysis
3. Results
Regression Analysis Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jackson, D.; Anders, R.; Padula, W.V.; Daly, J.; Davidson, P.M. Vulnerability of nurse and physicians with COVID-19: Monitoring and surveillance needed. J. Clin. Nurs. 2020. [Google Scholar] [CrossRef]
- Gómez-Ochoa, S.A.; Franco, O.H.; Rojas, L.Z.; Romero Guevara, S.L.; Echeverría, L.E.; Glisic, M.; Muka, T. COVID-19 in Healthcare Workers: A Systematic Review and Meta-Analysis of Prevalence, Risk Factors, Clinical Characteristics, and Outcomes. Am. J. Epidemiol. 2020. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Shaukat, N.; Ali, D.M.; Razzak, J. Physical and mental health impacts of COVID-19 on healthcare workers: A scoping review. Int. J. Emerg. Med. 2020, 13, 40. [Google Scholar] [CrossRef] [PubMed]
- Murphy, G.T.; Birch, S.; MacKenzie, A.; Alder, R.; Lethbridge, L.; Little, L. Eliminating the Shortage of Registered Nurses in Canada: An Exercise in Applied Needs-based Planning. Health Policy 2012, 105, 192–202. [Google Scholar] [CrossRef]
- World Health Organization Nursing and Midwifery: Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/nursing-and-midwifery. (accessed on 1 November 2020).
- World Health Organization Mental Health: Strengthening Our Response. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response (accessed on 30 May 2020).
- Twigg, E.; Humphris, G.; Jones, C.; Bramwell, R.; Griffiths, R.D. Use of a Screening Questionnaire for Post-traumatic Stress Disorder (PTSD) on a Sample of UK ICU Patients. Acta Anaesthesiol. Scand. 2008, 52, 202–208. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Leiter, M.P.; Maslach, C. Latent Burnout Profiles: A New Approach to Understanding the Burnout Experience. Burn. Res. 2016, 3, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Havaei, F.; Astivia, O.L.O.; MacPhee, M. The impact of workplace violence on medical-surgical nurses’ health outcome: A moderated mediation model of work environment conditions and burnout using secondary data. Int. J. Nurs. Stud. 2020, 109, 103666. [Google Scholar] [CrossRef]
- MacPhee, M.; Dahinten, V.; Havaei, F. The Impact of Heavy Perceived Nurse Workloads on Patient and Nurse Outcomes. Admin. Sci. 2017, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Shields, M.; Wilkins, K. Findings from the 2005 National Survey of the Work and Health of Nurses: Statistics Canada; Statistics Canada: Ottawa, ON, Canada, 2006; ISBN 0-662-44485-X.
- Kvas, A.; Seljak, J. Unreported workplace violence in nursing. Int. Nurs. Rev. 2014, 61, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Havaei, F.; MacPhee, M.; McLeod, C.B.; Ma, A.; Gear, A.; Sorensen, C. A Provincial Study of Nurses’ Psychological Health and Safety in British Columbia, Canada: Final Report. UBC cIRcle 2020. [Google Scholar] [CrossRef]
- Shi, L.; Lu, Z.-A.; Que, J.-Y.; Huang, X.-L.; Liu, L.; Ran, M.-S.; Gong, Y.-M.; Yuan, K.; Yan, W.; Sun, Y.-K.; et al. Prevalence of and Risk Factors Associated with Mental Health Symptoms Among the General Population in China During the Coronavirus Disease 2019 Pandemic. JAMA Netw. Open 2020, 3, e2014053. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Clarke, S.P.; Sloane, D.M.; Sochalski, J.A.; Busse, R.; Clarke, H.; Giovannetti, P.; Hunt, J.; Rafferty, A.M.; Shamian, J. Nurses’ reports on hospital care in five countries. Health Aff. 2001, 20, 43–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Havaei, F.; Dahinten, V.S.; MacPhee, M. Effect of Nursing Care Delivery Models on Registered Nurse Outcomes. SAGE Open Nurs. 2019, 5. [Google Scholar] [CrossRef] [Green Version]
- Leiter, M.P.; Laschinger, H.K.S. Relationships of work and practice environment to professional burnout: Testing a causal model. Nurs. Res. 2006, 55, 137–146. [Google Scholar] [CrossRef]
- Lake, E.T.; Sanders, J.; Duan, R.; Riman, K.A.; Schoenauer, K.M.; Chen, Y. A Meta-Analysis of the Associations Between the Nurse Work Environment in Hospitals and 4 Sets of Outcomes. Med. Care 2019, 57, 353–361. [Google Scholar] [CrossRef]
- Havaei, F.; MacPhee, M. Effect of Workplace Violence and Psychological Stress Responses on Medical-Surgical Nurses’ Medication Intake. Can. J. Nurs. Res. 2020. [Google Scholar] [CrossRef]
- Laschinger, H.K.S.; Leiter, M.P. The impact of nursing work environments on patient safety outcomes: The mediating role of burnout/engagement. J. Nurs. Adm. 2006, 36, 259–267. [Google Scholar] [CrossRef]
- Laschinger, H.K.S. Effect of empowerment on professional practice environments, work satisfaction, and patient care quality: Further testing the Nursing Worklife Model. J. Nurs. Care Qual. 2008, 23, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, K.H. Will COVID-19 generate global preparedness? Lancet 2020, 395, 1013–1014. [Google Scholar] [CrossRef]
- Villa, S.; Lombardi, A.; Mangioni, D.; Bozzi, G.; Bandera, A.; Gori, A.; Raviglione, M.C. The COVID-19 pandemic preparedness or lack thereof: From China to Italy. Glob. Health Med. 2020, 2, 73–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maslach, C.; Jackson, S.; Leiter, M. Burnout Inventory Manual; Consulting Psychologists Press: Palo Alto, CA, USA, 1996. [Google Scholar]
- Oudyk, J.; Smith, P. Preliminary Results for the Pandemic Healthcare Workers’ Survey; Occupational Health Clinics for Ontario Workers: Hamilton, ON, Canada, 2020. [Google Scholar]
- Zhao, S.; Xie, F.; Wang, J.; Shi, Y.; Zhang, S.; Han, X.; Sun, Z.; Shi, L.; Li, Z.; Mu, H.; et al. Prevalence of Workplace Violence Against Chinese Nurses and Its Association with Mental Health: A Cross-sectional Survey. Arch. Psychiatr. Nurs. 2018, 32, 242–247. [Google Scholar] [CrossRef]
- Zhang, S.-E.; Liu, W.; Wang, J.; Shi, Y.; Xie, F.; Cang, S.; Sun, T.; Fan, L. Impact of workplace violence and compassionate behaviour in hospitals on stress, sleep quality and subjective health status among Chinese nurses: A cross-sectional survey. BMJ Open 2018, 8, e019373. [Google Scholar] [CrossRef] [Green Version]
- Lanctôt, N.; Guay, S. The aftermath of workplace violence among healthcare workers: A systematic literature review of the consequences. Aggress. Violent Behav. 2014, 19, 492–501. [Google Scholar] [CrossRef]
- Zheng, R.; Zhou, Y.; Fu, Y.; Xiang, Q.; Cheng, F.; Chen, H.; Xu, H.; Fu, L.; Wu, X.; Feng, M.; et al. Prevalence and associated factors of depression and anxiety among nurses during the outbreak of COVID-19 in China: A cross-sectional study. Int. J. Nurs. Stud. 2020, 114, 103809. [Google Scholar] [CrossRef]
- Hu, D.; Kong, Y.; Li, W.; Han, Q.; Zhang, X.; Zhu, L.X.; Wan, S.W.; Liu, Z.; Shen, Q.; Yang, J.; et al. Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large-scale cross-sectional study. Lancet 2020, 24, 100424. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P. Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Mind Garden A Message from the Maslach Burnout Inventory Authors. Available online: https://www.mindgarden.com/blog/post/44-a-message-from-the-maslach-burnout-inventory-authors (accessed on 27 June 2020).
- Aiken, L.H.; Sermeus, W.; den Heede, K.V.; Sloane, D.M.; Busse, R.; McKee, M.; Bruyneel, L.; Rafferty, A.M.; Griffiths, P.; Moreno-Casbas, M.T.; et al. Patient safety, satisfaction, and quality of hospital care: Cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ 2012, 344. [Google Scholar] [CrossRef] [Green Version]
- Aiken, L.H.; Sloane, D.M.; Bruyneel, L.; Van den Heede, K.; Sermeus, W. RN4CAST Consortium Nurses’ reports of working conditions and hospital quality of care in 12 countries in Europe. Int. J. Nurs. Stud. 2013, 50, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Sloane, D.M.; Cimiotti, J.P.; Clarke, S.P.; Flynn, L.; Seago, J.A.; Spetz, J.; Smith, H.L. Implications of the California Nurse Staffing Mandate for Other States. Health Serv. Res. 2010, 45, 904–921. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Park, J.-H.; Bae, S.-H. Nurse staffing and nurse outcomes: A systematic review and meta-analysis. Nurs. Outlook 2018, 66, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.X.; Liu, J.; Afshar Jahanshahi, A.; Nawaser, K.; Yousefi, A.; Li, J.; Sun, S. At the height of the storm: Healthcare staff’s health conditions and job satisfaction and their associated predictors during the epidemic peak of COVID-19. Brain Behav. Immun. 2020, 87, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Arnetz, J.E.; Goetz, C.M.; Sudan, S.; Arble, E.; Janisse, J.; Arnetz, B.B. Personal Protective Equipment and Mental Health Symptoms Among Nurses During the COVID-19 Pandemic. J. Occup. Environ. Med. 2020, 61, 892–897. [Google Scholar] [CrossRef]
- Smith, P.M.; Oudyk, J.; Potter, G.; Mustard, C. The Association between the Perceived Adequacy of Workplace Infection Control Procedures and Personal Protective Equipment with Mental Health Symptoms: A Cross-sectional Survey of Canadian Health-care Workers during the COVID-19 Pandemic. Can. J. Psychiatry 2020. [Google Scholar] [CrossRef]
- Labrague, L.J.; Santos, J.A.A.D. COVID-19 anxiety among front-line nurses: Predictive role of organisational support, personal resilience and social support. J. Nurs. Manag. 2020, 28, 1653–1661. [Google Scholar] [CrossRef]
- Fernandez, R.; Lord, H.; Halcomb, E.; Moxham, L.; Middleton, R.; Alananzeh, I.; Ellwood, L. Implications for COVID-19: A systematic review of nurses’ experiences of working in acute care hospital settings during a respiratory pandemic. Int. J. Nurs. Stud. 2020, 111, 103637. [Google Scholar] [CrossRef]
- Bradley, J.R.; Cartwright, S. Social Support, Job Stress, Health, and Job Satisfaction Among Nurses in the United Kingdom. Int. J. Stress Manag. 2002, 9, 163–182. [Google Scholar] [CrossRef]
- Miner, K.N.; Settles, I.H.; Pratt-Hyatt, J.S.; Brady, C.C. Experiencing incivility in organizations: The buffering effects of emotional and organizational support. J. Appl. Soc. Psychol. 2012, 42, 340–372. [Google Scholar] [CrossRef]
- Brunetto, Y.; Xerri, M.; Shriberg, A.; Farr-Wharton, R.; Shacklock, K.; Newman, S.; Dienger, J. The impact of workplace relationships on engagement, well-being, commitment and turnover for nurses in Australia and the USA. J. Adv. Nurs. 2013, 69, 2786–2799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMillan, K.; Perron, A. Change fatigue in nurses: A qualitative study. J. Adv. Nurs. 2020, 76, 2627–2636. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.; Wey, H.; Foland, K. The Relationship Among Change Fatigue, Resilience, and Job Satisfaction of Hospital Staff Nurses. J. Nurs. Sch. 2018, 50, 306–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMillan, K.; Perron, A. Nurses amidst change: The concept of change fatigue offers an alternative perspective on organizational change. Policy Polit. Nurs. Pract. 2013, 14, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Ead, H. Change Fatigue in Health Care Professionals--An Issue of Workload or Human Factors Engineering? J. Perianesth Nurs. 2015, 30, 504–515. [Google Scholar] [CrossRef] [PubMed]
- Parasher, A. COVID-19: Current understanding of its pathophysiology, clinical presentation and treatment. Postgrad. Med. J. 2020. [Google Scholar] [CrossRef]
- Government of Canada COVID-19: Main Modes of Transmission. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/health-professionals/main-modes-transmission.html (accessed on 12 December 2020).
- Chen, Q.; Liang, M.; Li, Y.; Guo, J.; Fei, D.; Wang, L.; He, L.; Sheng, C.; Cai, Y.; Li, X.; et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e15–e16. [Google Scholar] [CrossRef]
- Havaei, F.; MacPhee, M.; Dahinten, V.S. The effect of nursing care delivery models on quality and safety outcomes of care: A cross-sectional survey study of medical-surgical nurses. J. Adv. Nurs. 2019, 75, 2144–2155. [Google Scholar] [CrossRef]
- Lasater, K.B.; Aiken, L.H.; Sloane, D.M.; French, R.; Martin, B.; Reneau, K.; Alexander, M.; McHugh, M.D. Chronic hospital nurse understaffing meets COVID-19: An observational study. BMJ Qual. Saf. 2020. [Google Scholar] [CrossRef]
- Canadian Institute of Health Information. Nursing in Canada, 2019: A Lense on Supply and Workforce; CIHI: Ottawa, ON, Canada, 2019. [Google Scholar]



{kind=link}
{kind=link}
| Mean (SD) | n | % | |
|---|---|---|---|
| Nurse Characteristics | |||
| Role | |||
| Direct care provider | - | 3161 | 86 |
| Nurse leader | - | 393 | 10.7 |
| Educator | - | 122 | 3.3 |
| Total | 3676 | ||
| Designation 1 | |||
| RN | - | 2735 | 74.4 |
| RPN | - | 200 | 5.4 |
| Dually registered (RN/RPN) | - | 15 | 0.4 |
| LPN | - | 714 | 19.4 |
| Total | 3664 | ||
| Years of nursing experience | 12 (7.2) | - | - |
| Workplace Characteristics | Mean (SD) | n | % |
| Sector | |||
| Acute care | - | 2319 | 63.2 |
| Community care | - | 870 | 23.7 |
| Long-term care | - | 483 | 13.2 |
| Total | 3672 | ||
| Geographic area | |||
| Urban | - | 2324 | 63.6 |
| Suburban | - | 727 | 19.9 |
| Rural | - | 605 | 16.5 |
| Total | 3656 |
| Workplace Conditions | n | Mean | SD | Range 1 |
|---|---|---|---|---|
| Key predictors | ||||
| Workplace safety | ||||
| Frequency of direct contact with COVID patients 1 | 3587 | 2.91 | 1.97 | 1–7 |
| Concern for contracting COVID 2 | 3597 | 3.47 | 1.12 | 1–5 |
| Concern for bringing COVID home 2 | 3597 | 3.90 | 1.14 | 1–5 |
| Likelihood of refusing unsafe work if denied appropriate PPE 3 | 3563 | 1.99 | 0.92 | 1–4 |
| Confidence in ability to assess PPE requirements 4 | 3576 | 2.55 | 1.20 | 1–6 |
| Confidence in ability to assess risk 4 | 3574 | 2.48 | 1.07 | 1–6 |
| Experienced COVID-19 symptoms 5 | 3577 | 0.31 | 0.46 | 0–1 |
| Submitted workers’ compensation 5 | 3549 | 0.02 | 0.12 | 0–1 |
| Resources and supplies | ||||
| Nurse staffing adequacy 6 | 3597 | 3.48 | 1.60 | 1–6 |
| PPE adequacy 7 | 3574 | 3.30 | 1.54 | 1–6 |
| PPE quality 7 | 3569 | 3.59 | 1.50 | 1–6 |
| Training 8 | 3526 | 2.33 | 0.99 | 1–5 |
| N95 mask fitting 9 | 3575 | 3.27 | 1.54 | 1–7 |
| Organizational preparedness | ||||
| Confidence in organizational handling of the pandemic 4 | 3527 | 3.49 | 1.34 | 1–6 |
| Confidence in manager’s handling of the pandemic 4 | 3522 | 3.48 | 1.46 | 1–6 |
| Frequency of COVID-19 related policy changes 10 | 3527 | 5.47 | 1.68 | 1–8 |
| Transparency of pandemic-related organizational decisions 11 | 3522 | 3.29 | 1.02 | 1–5 |
| Organizational support | ||||
| Told to work despite exposure 5 | 3571 | 0.24 | 0.43 | 0–1 |
| Told to work despite symptoms 5 | 3556 | 0.31 | 0.23 | 0–1 |
| Organizational support 12 | 3523 | 2.64 | 1.03 | 1–5 |
| Workplace relations | ||||
| Relationships with nursing colleagues 13 | 3524 | 3.05 | 0.79 | 1–5 |
| Relationships with manager 13 | 3526 | 3.25 | 0.80 | 1–5 |
| Relationships with the rest of allied health 13 | 3523 | 3.11 | 0.70 | 1–5 |
| Outcome Variables | Frequency | Percent | Mean | SD | Range |
|---|---|---|---|---|---|
| Post-traumatic stress disorder (PTSD) (PTSS-14) | |||||
| Under cutoff (14–44) | 1944 | 52.9 | |||
| Met cutoff, PTSD (45–98) | 1732 | 47.1 | |||
| Total | 3369 | 46.68 | 19.37 | 14–98 | |
| Anxiety (GAD-7) | |||||
| Under cutoff (0–9) | 2114 | 62.4 | |||
| Met cutoff, anxiety (10–21) | 1273 | 37.6 | |||
| Total | 3387 | 8.53 | 5.80 | 0–21 | |
| Depression (PHQ-9) | |||||
| Under cutoff (0–9) | 1972 | 58.6 | |||
| Met cutoff, major depression (10–27) | 1391 | 41.4 | |||
| Total | 3363 | 8.99 | 6.23 | 0–27 | |
| Emotional Exhaustion (EE) (MBI-HSS) | |||||
| Low EE (0–16) | 602 | 18.4 | |||
| Moderate EE (17–26) | 692 | 21.2 | |||
| High EE (27–54) | 1975 | 60.4 | |||
| Total | 3269 | 30.05 | 13.23 | 0–54 |
| PTSD (PTSS-14) | Anxiety (GAD-7) | Depression (PHQ-9) | Emotional Exhaustion (MBI-HSS) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | B | 95% CI | p | B | 95% CI | p | B | 95% CI | p | B | 95% CI | p |
| (Constant) | −9.50 | −14.35–−4.65 | 0.00 | −6.46 | −7.94–−4.98 | 0.00 | −5.43 | −7.06–−3.79 | 0.00 | −1.92 | −5.27–1.43 | 0.26 |
| CONTROL VARIABLES | ||||||||||||
| Role (Direct care provider) | −1.23 | −2.96–0.49 | 0.16 | −0.61 | −1.14–−0.09 | 0.02 | −0.55 | −1.13–0.03 | 0.06 | −3.29 | −4.48–−2.10 | 0.00 |
| Sector (Acute care) | 1.04 | −0.26–2.34 | 0.12 | −0.04 | −0.44–0.36 | 0.84 | −0.19 | −0.63–0.25 | 0.39 | 0.42 | −0.48–1.32 | 0.36 |
| Geographic area (Urban/suburban) | 0.94 | −0.62–2.49 | 0.24 | −0.07 | −0.54–0.41 | 0.79 | 0.00 | −0.53–0.52 | 0.99 | −0.20 | −1.27–0.87 | 0.71 |
| Designation (RN/RPN) | 0.55 | −0.96–2.07 | 0.47 | 0.52 | 0.06–0.98 | 0.03 | 0.04 | −0.47–0.55 | 0.87 | 1.47 | 0.42–2.52 | 0.01 |
| Experience (Years of experience) | −0.08 | −0.17–0.00 | 0.06 | −0.06 | −0.09–−0.04 | 0.00 | −0.04 | −0.06–−0.01 | 0.01 | −0.09 | −0.15–−0.03 | 0.00 |
| KEY PREDICTORS | ||||||||||||
| Workplace safety | ||||||||||||
| Frequency of direct contact | 0.62 | 0.30–0.94 | 0.00 | 0.09 | 0.00–0.19 | 0.06 | 0.10 | −0.01–0.21 | 0.07 | 0.38 | 0.16–0.60 | 0.00 |
| Concern for contracting COVID | 1.27 | 0.48–2.06 | 0.00 | 0.37 | 0.13–0.61 | 0.00 | 0.16 | −0.11–0.42 | 0.24 | 0.47 | −0.07–1.01 | 0.09 |
| Concern for bringing COVID home | 1.17 | 0.40–1.95 | 0.00 | 0.44 | 0.21–0.68 | 0.00 | 0.30 | 0.04–0.56 | 0.02 | 0.29 | −0.24–0.82 | 0.29 |
| Refusing unsafe work if denied appropriate PPE | 1.56 | 0.91–2.21 | 0.00 | 0.44 | 0.25–0.64 | 0.00 | 0.50 | 0.29–0.72 | 0.00 | 0.37 | −0.08–0.82 | 0.11 |
| Experienced COVID-19 symptoms | 4.12 | 2.87–5.37 | 0.00 | 1.24 | 0.86–1.63 | 0.00 | 1.53 | 1.11–1.95 | 0.00 | 1.81 | 0.94–2.67 | 0.00 |
| Resources and supplies | ||||||||||||
| Nurse staffing adequacy | 1.03 | 0.62–1.44 | 0.00 | 0.32 | 0.20–0.44 | 0.00 | 0.32 | 0.19–0.46 | 0.00 | 1.41 | 1.13–1.69 | 0.00 |
| PPE access adequacy | 0.77 | 0.31–1.23 | 0.00 | 0.08 | −0.06–0.22 | 0.27 | 0.16 | 0.00–0.31 | 0.05 | 0.25 | −0.07–0.57 | 0.12 |
| Organizational preparedness | ||||||||||||
| Confidence in organizational handling of the pandemic | 0.63 | 0.03–1.29 | 0.06 | 0.17 | −0.03–0.37 | 0.09 | 0.11 | −0.12–0.33 | 0.35 | 0.77 | 0.32–1.23 | 0.00 |
| Frequency of COVID-19 related policy changes | 1.30 | 0.94–1.66 | 0.00 | 0.43 | 0.32–0.54 | 0.00 | 0.46 | 0.34–0.59 | 0.00 | 0.90 | 0.65–1.15 | 0.00 |
| Transparency of pandemic-related organizational decisions | 0.67 | −0.14–1.49 | 0.10 | 0.11 | −0.13–0.36 | 0.37 | 0.18 | −0.09–0.45 | 0.20 | 0.68 | 0.12–1.24 | 0.02 |
| Organizational support | ||||||||||||
| Organizational support | 1.97 | 1.13–2.80 | 0.00 | 0.60 | 0.35–0.86 | 0.00 | 0.71 | 0.43–0.99 | 0.00 | 1.48 | 0.90–2.06 | 0.00 |
| Workplace relations | ||||||||||||
| Relationships with nursing colleagues | 2.12 | 1.28–2.96 | 0.00 | 0.73 | 0.47–0.99 | 0.00 | 0.74 | 0.46–1.03 | 0.00 | 1.03 | 0.45–1.61 | 0.00 |
| Relationships with manager | 1.34 | 0.44–2.23 | 0.00 | 0.35 | 0.08–0.62 | 0.01 | 0.15 | −0.15–0.45 | 0.33 | 0.87 | 0.25–1.49 | 0.01 |
| Relationships with the rest of allied health | 2.44 | 1.49–3.39 | 0.00 | 0.56 | 0.27–0.85 | 0.00 | 0.71 | 0.39–1.03 | 0.00 | 1.31 | 0.66–1.97 | 0.00 |
| Final model F-statistic, explained variance (Adjusted R2), model p | 59.98 (19, 3229) | 25.7% | 0.00 | 51.40 (19, 3245) | 22.7% | 0.00 | 40.92 (19, 3223) | 19.0% | 0.00 | 58.51 (19, 3136) | 25.7% | 0.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Havaei, F.; Ma, A.; Staempfli, S.; MacPhee, M. Nurses’ Workplace Conditions Impacting Their Mental Health during COVID-19: A Cross-Sectional Survey Study. Healthcare 2021, 9, 84. https://doi.org/10.3390/healthcare9010084
Havaei F, Ma A, Staempfli S, MacPhee M. Nurses’ Workplace Conditions Impacting Their Mental Health during COVID-19: A Cross-Sectional Survey Study. Healthcare. 2021; 9(1):84. https://doi.org/10.3390/healthcare9010084
Chicago/Turabian StyleHavaei, Farinaz, Andy Ma, Sabina Staempfli, and Maura MacPhee. 2021. "Nurses’ Workplace Conditions Impacting Their Mental Health during COVID-19: A Cross-Sectional Survey Study" Healthcare 9, no. 1: 84. https://doi.org/10.3390/healthcare9010084
APA StyleHavaei, F., Ma, A., Staempfli, S., & MacPhee, M. (2021). Nurses’ Workplace Conditions Impacting Their Mental Health during COVID-19: A Cross-Sectional Survey Study. Healthcare, 9(1), 84. https://doi.org/10.3390/healthcare9010084