
Disparities across Diverse Populations in the Health and Treatment of Patients with Osteoarthritis

Abstract
:1. Introduction
2. Prevalence of Arthritis/Osteoarthritis among Racial, Ethnic, and Regional Subpopulations in the United States
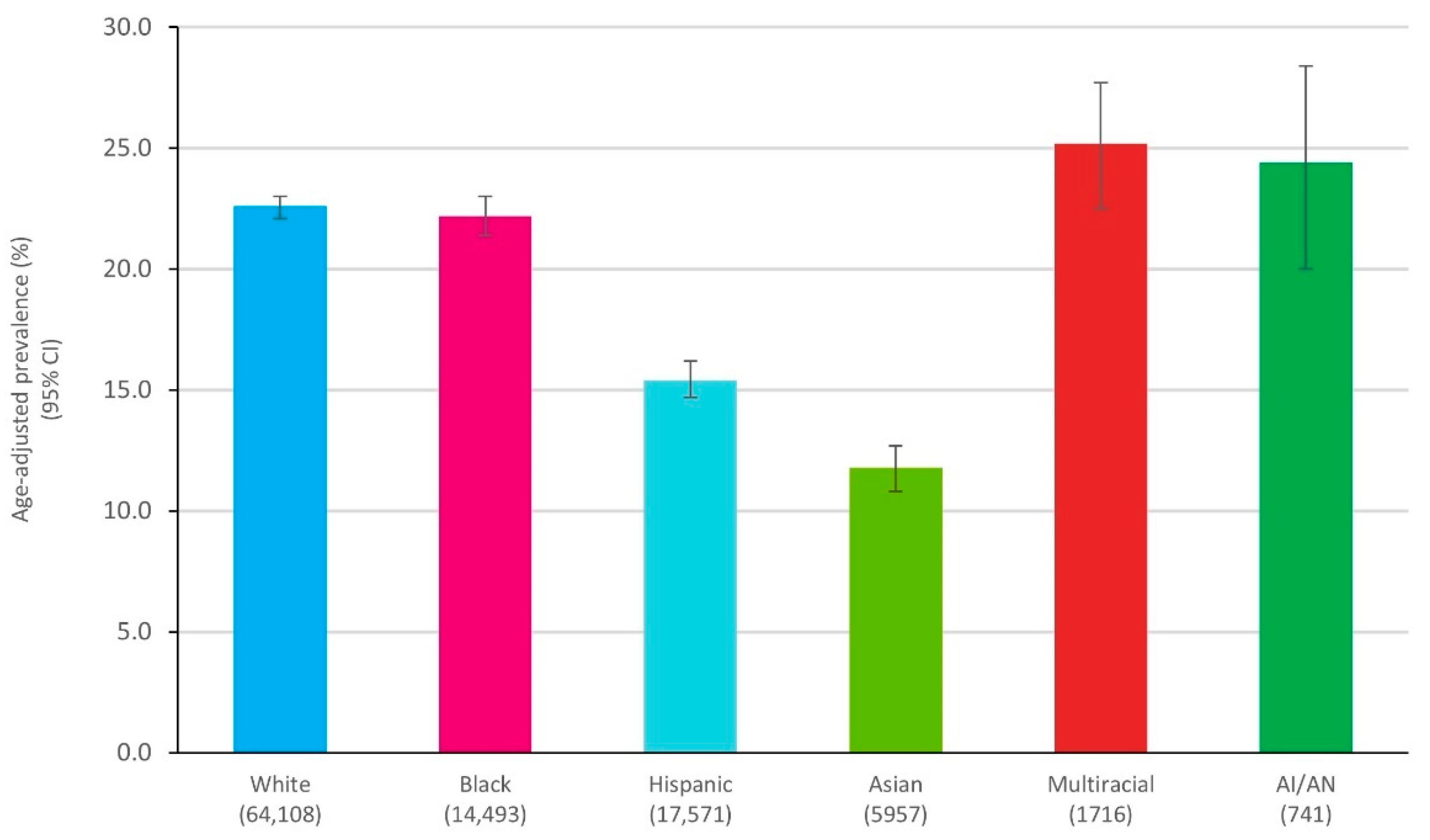
2.1. Prevalence of Arthritis by Race/Ethnicity

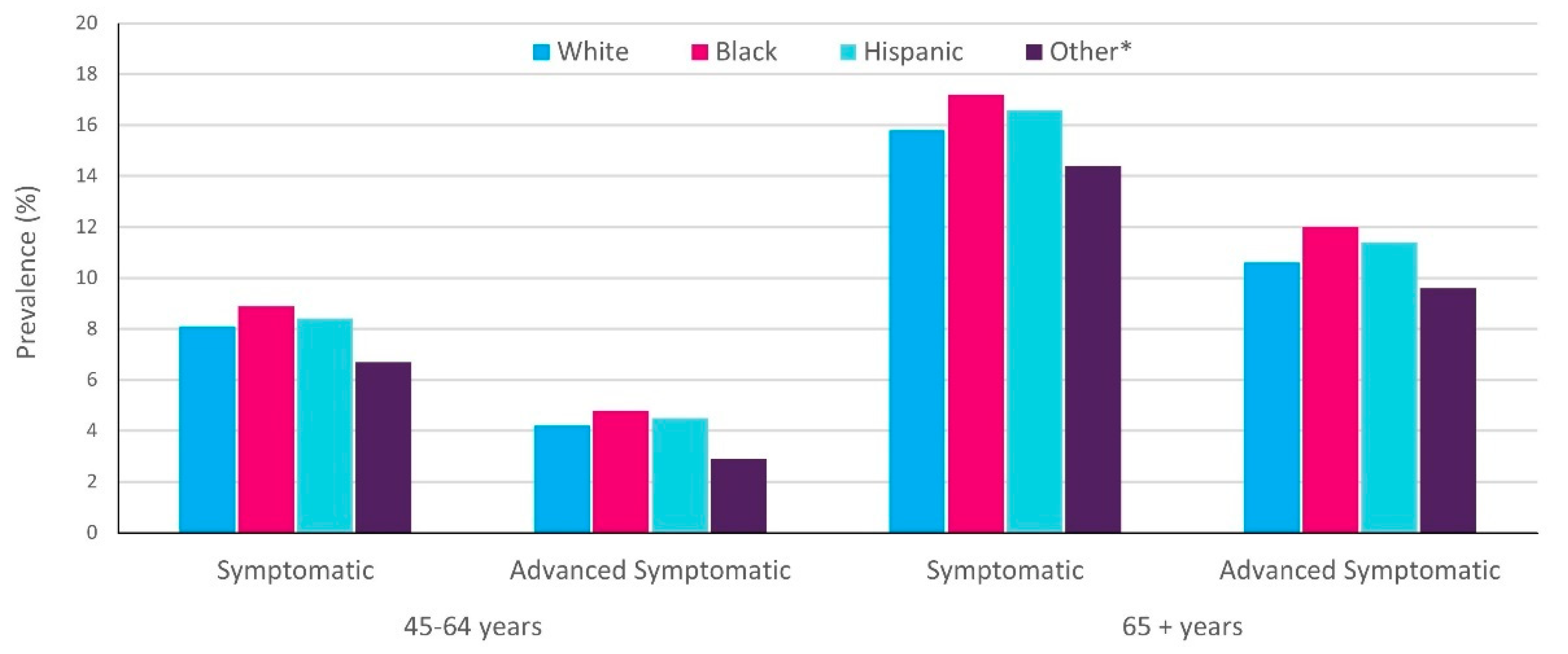
2.2. Prevalence of Knee OA by Race/Ethnicity and Age

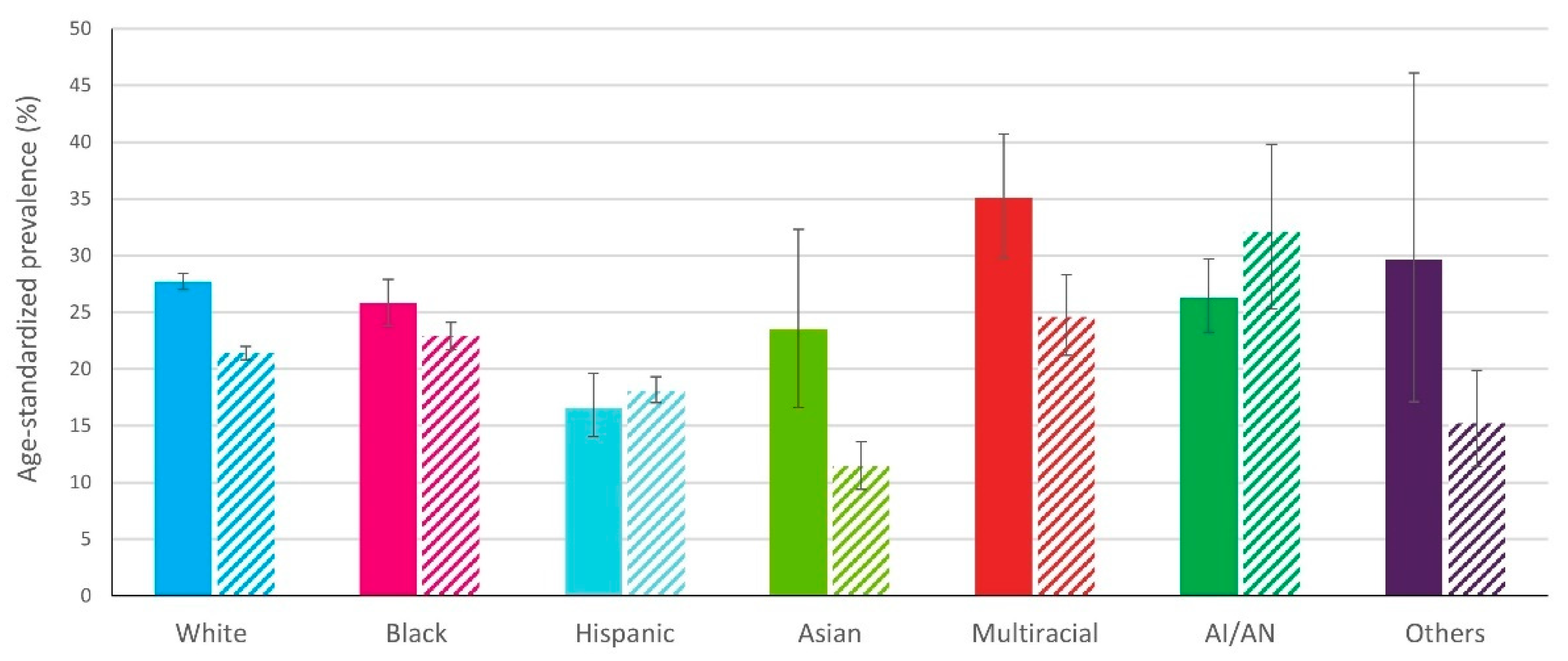
2.3. Prevalence of Arthritis in Rural Versus Urban Communities

3. Disparities in Healthcare Utilization among Patients with Arthritis/Osteoarthritis
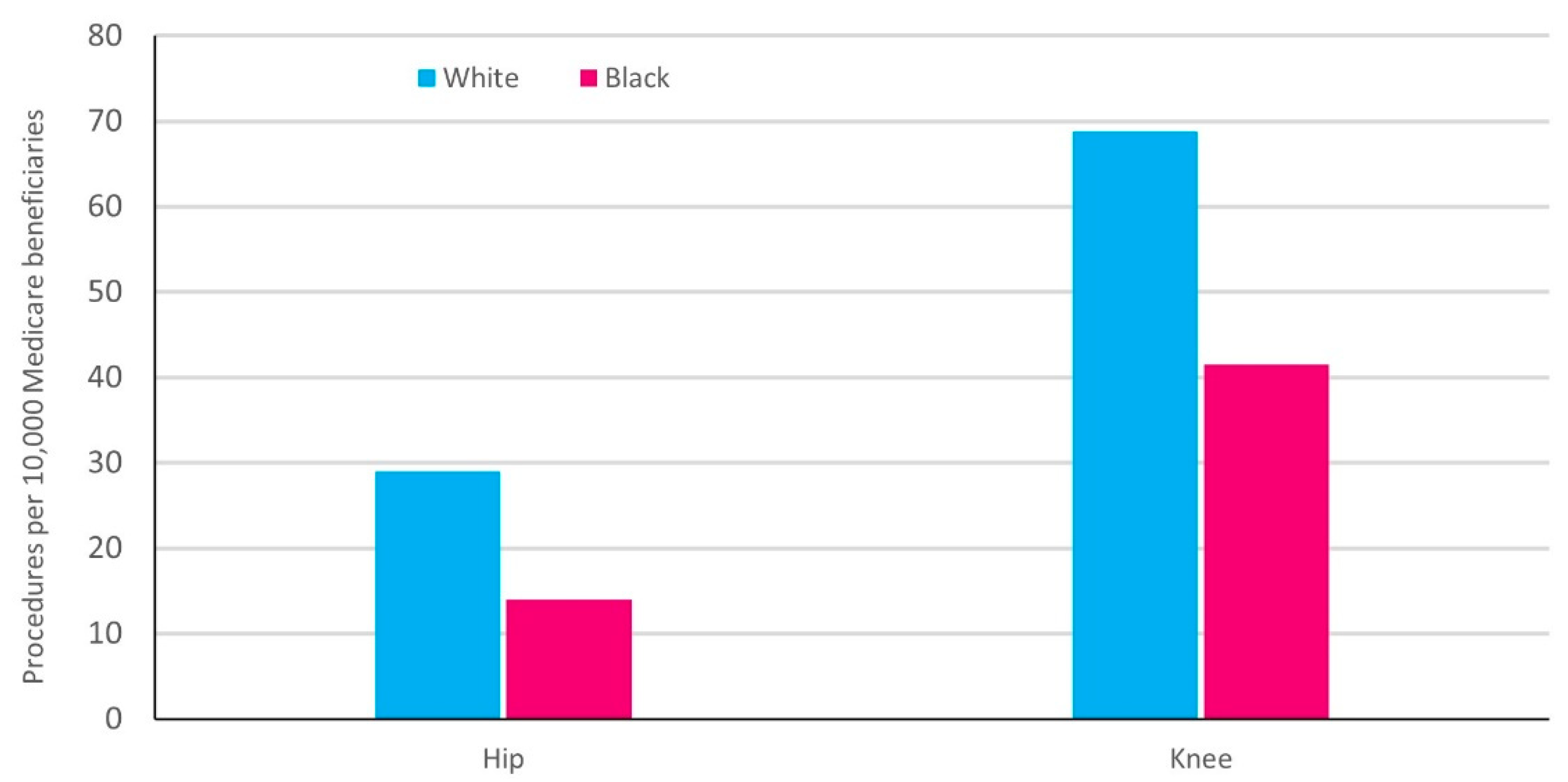
3.1. Treatment Utilization: Total Joint Arthroplasty (TJA)

3.2. Patient Factors That May Influence Racial Disparity in TJA Utilization
3.3. Healthcare Provider Factors That May Influence Racial Disparity in TJA Utilization
3.4. Healthcare System Factors That May Influence Racial Disparity in TJA Utilization
3.5. Utilization of Other Treatments Apart from Surgery and Treatment Recommendations
4. Disparities in Treatment Outcomes for Patients with Arthritis/Osteoarthritis
4.1. Disparities in Treatment Outcomes: Total Knee/Hip Arthroplasty
4.2. The Influence of Poverty on Racial Disparity in Treatment Outcomes

4.3. The Economic Impact of Racial Disparity in Treatment Utilization and Clinical Outcomes
5. Summary and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Lawrence, R.C.; Felson, D.T.; Helmick, C.G.; Arnold, L.M.; Choi, H.; Deyo, R.A.; Gabriel, S.; Hirsch, R.; Hochberg, M.C.; Hunder, G.G.; et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 2008, 58, 26–35. [Google Scholar] [CrossRef] [Green Version]
- Barbour, K.E.; Helmick, C.G.; Boring, M.; Brady, T.J. Vital Signs: Prevalence of Doctor-diagnosed arthritis and arthritis-attributable activity limitation–United States, 2013–2015. Morb. Mortal. Wkly. Rep. 2017, 66, 246–253. Available online: https://www.cdc.gov/mmwr (accessed on 12 October 2021). [CrossRef]
- Dieppe, P.A.; Lohmander, L.S. Pathogenesis and management of pain in osteoarthritis. Lancet 2005, 365, 965–973. [Google Scholar] [CrossRef]
- Badley, E.M.; Wagstaff, S.; Wood, P. Measures of functional ability (disability) in arthritis in relation to impairment of range of joint movement. Ann. Rheum. Dis. 1984, 43, 563–569. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Chang, R.W.; Dunlop, D.D. Population impact of arthritis on disability in older adults. Arthritis Rheum. 2006, 55, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Alkan, B.M.; Fidan, F.; Tosun, A.; Ardifoğlu, Ö. Quality of life and self-reported disability in patients with knee osteoarthritis. Mod. Rheumatol. 2014, 24, 166–171. [Google Scholar] [CrossRef]
- Goldenberg, D.L. The interface of pain and mood disturbances in the rheumatic diseases. Semin Arthritis Rheum. 2010, 40, 15–31. [Google Scholar] [CrossRef]
- US: US Bone and Joint Initiative. The Burden of Musculoskeletal Diseases in the United States (BMUS), 4th ed. Available online: http://www.boneandjointburden.org (accessed on 10 October 2021).
- Allen, K.D. Racial and ethnic disparities in osteoarthritis phenotypes. Curr. Opin. Rheumatol. 2010, 22, 528–532. [Google Scholar] [CrossRef]
- Allen, K.D.; Chen, J.-C.; Callahan, L.F.; Golightly, Y.M.; Helmick, C.G.; Renner, J.B.; Schwartz, T.A.; Jordan, J.M. Racial differences in knee osteoarthritis pain: Potential contribution of occupational and household tasks. J. Rheumatol. 2012, 39, 337–344. [Google Scholar] [CrossRef] [Green Version]
- Glover, T.L.; Goodin, B.R.; Horgas, A.L.; Kindler, L.L.; King, C.D.; Sibille, K.T.; Peloquin, C.A.; Riley, J.L., 3rd; Staud, R.; Bradley, L.A.; et al. Vitamin D, race, and experimental pain sensitivity in older adults with knee osteoarthritis. Arthritis Rheum. 2012, 64, 3926–3935. [Google Scholar] [CrossRef]
- Jordan, J.M.; Helmick, C.G.; Renner, J.B.; Luta, G.; Dragomir, A.D.; Woodard, J.; Fang, F.; Schwartz, T.A.; Abbate, L.M.; Callahan, L.F. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthritis in African Americans and Caucasians: The Johnston County Osteoarthritis Project. J. Rheumatol. 2007, 34, 172–180. [Google Scholar]
- Nelson, A.E.; Renner, J.B.; Schwartz, T.A.; Kraus, V.B.; Helmick, C.G.; Jordan, J.M. Differences in multijoint radiographic osteoarthritis phenotypes among African Americans and Caucasians: The Johnston County Osteoarthritis project. Arthritis Rheum. 2011, 63, 3843–3852. [Google Scholar] [CrossRef]
- NIAMS National Institute of Arthritis Musculoskeletal and Skin Diseases. Department of Health and Human Services. Strategic Plan for Reducing Racial Disparities. Available online: https://www.niams.nih.gov/about-niams/strategic-plan-fiscal-years-2020-2024 (accessed on 12 October 2021).
- American Academy of Orthopaedic Surgeons. February 2004 Bulletin. AAOS Look at Racial, Ethnic and Gender Disparities in Osthopaedics. Available online: http://www2.aaos.org/bulletin/feb04/fline2.htm (accessed on 12 October 2021).
- Silverwood, V.; Blagojevic-Bucknall, M.; Jinks, C.; Jordan, J.L.; Protheroe, J.; Jordan, K.P. Current evidence on risk factors for knee osteoarthritis in older adults: A systematic review and meta-analysis. Osteoarthr. Cartil. 2015, 23, 507–515. [Google Scholar] [CrossRef] [Green Version]
- Weinstein, A.M.; Rome, B.N.; Reichmann, W.M.; Collins, J.E.; Burbine, S.A.; Thornhill, T.S.; Wright, J.; Katz, J.N.; Losina, E. Estimating the burden of total knee replacement in the United States. J. Bone Joint Surg. Am. 2013, 95, 385–392. [Google Scholar] [CrossRef] [Green Version]
- Daigle, M.E.; Weinstein, A.M.; Katz, J.N.; Losina, E. The cost-effectiveness of total joint arthroplasty: A systematic review of published literature. Best Pract. Res. Clin. Rheumatol. 2012, 26, 649–658. [Google Scholar] [CrossRef] [Green Version]
- Deshpande, B.R.; Katz, J.N.; Solomon, D.H.; Yelin, E.H.; Hunter, D.J.; Messier, S.P.; Suter, L.G.; Losina, E. Number of persons with symptomatic knee osteoarthritis in the US: Impact of race and ethnicity, age, sex, and obesity. Arthritis Care Res. 2016, 68, 1743–1750. [Google Scholar] [CrossRef]
- Meit, M.; Knudson, A.; Gilbert, T.; Yu, A.T.C.; Tanenbaum, E.; Ormson, E.; TenBroeck, S.; Bayne, A.; Popat, S. The 2014 update of the rural-urban chartbook. Bethesda, MD: Rural Health Reform Policy Center. 2014. Available online: https://ruralhealth.und.edu/projects/health-reform-policy-research-center/pdf/2014-rural-urban-chartbook-update.pdf (accessed on 12 October 2021).
- Shaw, K.M.; Theis, K.A.; Self-Brown, S.; Roblin, D.W.; Barker, L. Chronic disease disparities by county economic status and metropolitan classification, Behavioral Risk Factor Surveillance System, 2013. Prev. Chronic Dis. 2016, 13, E119. [Google Scholar] [CrossRef] [Green Version]
- Barbour, K.E.; Helmick, C.G.; Boring, M.; Zhang, X.; Lu, H.; Holt, J.B. Prevalence of doctor-diagnosed arthritis at state and county levels—United States, 2014. Morb. Mortal. Wkly. Rep. 2016, 65, 489–494. [Google Scholar] [CrossRef] [Green Version]
- Boring, M.A.; Hootman, J.M.; Liu, Y.; Theis, K.A.; Murphy, L.B.; Barbour, K.E.; Helmick, C.G.; Brady, T.J.; Croft, J.B. Prevalence of arthritis and arthritis-attributable activity limitation by urban-rural county classification–United States, 2015. Morb. Mortal. Wkly. Rep. 2017, 66, 527–532. [Google Scholar] [CrossRef] [Green Version]
- HCUP. HCUP Facts and Figures 2009- Section 3: Inpatient Hospital Stays by Procedure. Exhibit 3.1 Most Frequent All-Listed Procedures. Available online: https://www.hcup-us.ahrq.gov/reports/factsandfigures/2009/section3_TOC.jsp (accessed on 12 October 2021).
- Ibrahim, S.A.; Siminoff, L.A.; Burant, C.J.; Kwoh, C.K. Understanding ethnic differences in the utilization of joint replacement for osteoarthritis: The role of patient-level factors. Med. Care 2002, 40, 144–151. [Google Scholar] [CrossRef]
- Ibrahim, S.A.; Stone, R.A.; Han, X.; Cohen, P.; Fine, M.J.; Henderson, W.G.; Khuri, S.F.; Kwoh, C.K. Racial/ethnic differences in surgical outcomes in veterans following knee or hip arthroplasty. Arthritis Rheum. 2005, 52, 3143–3151. [Google Scholar] [CrossRef]
- Skinner, J.; Weinstein, J.N.; Sporer, S.M.; Wennberg, J.E. Racial, ethnic, and geographic disparities in rates of knee arthroplasty among Medicare patients. N. Engl. J. Med. 2003, 349, 1350–1359. [Google Scholar] [CrossRef] [Green Version]
- Jha, A.K.; Fisher, E.S.; Li, Z.; Orav, E.J.; Epstein, A.M. Racial trends in the use of major procedures among the elderly. N. Engl. J. Med. 2005, 353, 683–691. [Google Scholar] [CrossRef]
- Singh, J.A.; Lu, X.; Rosenthal, G.E.; Ibrahim, S.; Cram, P. Racial disparities in knee and hip total joint arthroplasty: An 18-year analysis of national Medicare data. Ann. Rheum. Dis. 2014, 73, 2107–2115. [Google Scholar] [CrossRef]
- MacFarlane, L.A.; Kim, E.; Cook, N.R.; Lee, I.-M.; Iversen, M.D.; Katz, J.N.; Costenbader, K.H. Racial variation in total knee replacement in a diverse nationwide clinical trial. J. Clin. Rheumatol. 2018, 24, 1–5. [Google Scholar] [CrossRef]
- Zhang, W.; Lyman, S.; Boutin-Foster, C.; Parks, M.L.; Pan, T.-J.; Lan, A.; Ma, Y. Racial and ethnic disparities in utilization rate, hospital volume, and perioperative outcomes after total knee arthroplasty. J. Bone Joint Surg. Am. 2016, 98, 1243–1252. [Google Scholar] [CrossRef]
- Cavanaugh, A.M.; Rauh, M.J.; Thompson, C.A.; Alcaraz, J.; Mihalko, W.M.; Bird, C.E.; Eaton, C.B.; Rosal, M.C.; Li, W.; Shadyab, A.H.; et al. Racial and ethnic disparities in utilization of total knee arthroplasty among older women. Osteoarthr. Cartil. 2019, 27, 1746–1754. [Google Scholar] [CrossRef]
- Anderson, G.L.; Manson, J.; Wallace, R.; Lund, B.; Hall, D.; Davis, S.; Shumaker, S.; Wang, C.-Y.; Stein, E.; Prentice, R.L. Implementation of the Women’s Health Initiative study design. Ann. Epidemiol 2003, 13, S5–S17. [Google Scholar] [CrossRef]
- Group TWHIS. Design of the Women’s Health Initiative clinical trial and observational study. The Women’s Health Initiative Study Group. Control Clin. Trials 1998, 19, 61–109. [Google Scholar] [CrossRef]
- Ibrahim, S.A.; Kim, H.; McConnell, K.J. The CMS Comprehensive Care Model and racial disparity in joint replacement. JAMA 2016, 316, 1258–1259. [Google Scholar] [CrossRef]
- Ibrahim, S.A. Racial variations in the utilization of knee and hip joint replacement: An introduction and review of the most recent literature. Curr. Orthop. Pract. 2010, 21, 126–131. [Google Scholar] [CrossRef] [Green Version]
- Shahid, H.; Singh, J.A. Racial/ethnic disparity in rates and outcomes of total joint arthroplasty. Curr. Rheumatol. Rep. 2016, 18, 20. [Google Scholar] [CrossRef]
- Groeneveld, P.W.; Kwoh, C.K.; Mor, M.K.; Appelt, C.J.; Geng, M.; Gutierrez, J.C.; Wessel, D.S.; Ibrahim, S.A. Racial differences in expectations of joint replacement surgery outcomes. Arthritis Rheum. 2008, 59, 730–737. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, S.A.; Siminoff, L.A.; Burant, C.J.; Kwoh, C.K. Variation in Perceptions of Treatment and Self-Care Practices in Elderly with Osteoarthritis: A Comparison Between African American and White Patients. Arthritis Care Res. 2001, 45, 340–345. [Google Scholar] [CrossRef]
- Kwoh, C.K.; Vina, E.R.; Cloonan, Y.K.; Hannon, M.J.; Boudreau, R.M.; Ibrahim, S.A. Determinants of patient preferences for total knee replacement: African-Americans and whites. Arthritis Res. Ther. 2015, 17, 348. [Google Scholar] [CrossRef] [Green Version]
- Jones, A.C.; Kwoh, C.K.; Groeneveld, P.W.; Mor, M.; Geng, M.; Ibrahim, S.A. Investigating racial differences in coping with chronic osteoarthritis pain. J. Cross Cult. Gerontol. 2008, 23, 339–347. [Google Scholar] [CrossRef]
- Allen, K.D.; Golightly, Y.M.; Callahan, L.F.; Helmick, C.G.; Ibrahim, S.A.; Kwoh, C.K.; Renner, J.B.; Jordan, J.M. Race and sex differences in willingness to undergo total joint replacement: The Johnston County Osteoarthritis Project. Arthritis Care Res. 2014, 66, 1193–1202. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, S.A.; Siminoff, L.A.; Burant, C.J.; Kwoh, C.K. Differences in expectations of outcome mediate African American/white patient differences in “willingness” to consider joint replacement. Arthritis Rheum. 2002, 46, 2429–2435. [Google Scholar] [CrossRef]
- Vina, E.R.; Cloonan, Y.K.; Ibrahim, S.A.; Hannon, M.J.; Boudreau, R.M.; Kwoh, C.K. Race, sex, and total knee replacement consideration: Role of social support. Arthritis Care Res. 2013, 65, 1103–1111. [Google Scholar] [CrossRef]
- Hausmann, L.R.; Mor, M.; Hanusa, B.H.; Zickmund, S.; Cohen, P.Z.; Grant, R.; Kresevic, D.M.; Gordon, H.S.; Ling, B.S.; Kwoh, C.K.; et al. The effect of patient race on total joint replacement recommendations and utilization in the orthopedic setting. J. Gen. Intern. Med. 2010, 25, 982–988. [Google Scholar] [CrossRef] [Green Version]
- Tepper, S.; Hochberg, M.C. Factors associated with hip osteoarthritis: Data from the first National Health and Nutrition Examination Survey (NHANES-I). Am. J. Epidemiol. 1993, 137, 1081–1088. [Google Scholar] [CrossRef]
- Levinson, W.; Hudak, P.L.; Feldman, J.J.; Frankel, R.M.; Kuby, A.; Bereknyei, S.; Braddock, C., III. “It is not what you say”: Racial disparities in communication between orthopedic surgeons and patients. Med. Care 2008, 46, 410–416. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, S.A.; Burant, C.J.; Mercer, M.B.; Siminoff, L.A.; Kwoh, C.K. Older Patients’ Perceptions of Quality of Chronic Knee or Hip Pain: Differences by Ethnicity and Relationship to Clinical Variables. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, M472–M477. [Google Scholar] [CrossRef] [Green Version]
- Hanchate, A.D.; Zhang, Y.; Felson, D.T.; Ash, A.S. Exploring the determinants of racial and ethnic disparities in total knee arthroplasty. Health insurance, income, and assets. Med. Care 2008, 46, 481–488. [Google Scholar] [CrossRef] [Green Version]
- Leacock, C. Getting Started with the Health and Retirement Study. 2006. Version 1. Ann Arbor, MI: Survey Research Center, Institute for Social Research, University of Michigan. Available online: https://hrsonline.isr.umich.edu/ (accessed on 12 October 2021).
- St Clair, P.; Bugliari, D.; Chien, S.; Haider, S.; Hayden, O.; Hurd, M.; Ilchuk, S.; Lopez, G.; Loughran, D.; Panis, C.; et al. RAND HRS Data Documentation; Version, D; Rand Center for the Study of Aging: Los Angeles, CA, USA, 2004; Available online: http://www.rand.org/labor/aging (accessed on 19 October 2021).
- SooHoo, N.F.; Lieberman, J.R.; Ko, C.Y.; Zingmond, D.S. Factors predicting complication rates following total knee replacement. J. Bone Joint Surg. Am. 2006, 88, 480–485. [Google Scholar]
- SooHoo, N.F.; Zingmond, D.S.; Lieberman, J.R.; Ko, C.Y. Primary total knee arthroplasty in California 1991 to 2001: Does hospital volume affect outcomes? J. Arthroplast. 2006, 21, 199–205. [Google Scholar] [CrossRef]
- SooHoo, N.F.; Zingmond, D.S.; Ko, C.Y. Disparities in the utilization of high-volume hospitals for total knee replacement. J. Natl. Med. Assoc. 2008, 100, 559–564. [Google Scholar] [CrossRef]
- Lapane, K.L.; Liu, S.-H.; Dube, C.E.; Driban, J.B.; McAlindon, T.E.; Eaton, C.B. Factors associated with the use of hyaluronic acid and corticosteroid injections among patients with radiographically confirmed knee osteoarthritis: A retrospective data analysis. Clin. Ther. 2017, 39, 347–358. [Google Scholar] [CrossRef]
- Yang, S.; Jawahar, R.; McAlindon, T.E.; Eaton, C.B.; Lapane, K.L. Racial differences in symptom management approaches among persons with radiographic knee osteoarthritis. BMC Complement. Altern. Med. 2012, 12, 86. [Google Scholar] [CrossRef] [Green Version]
- Hichberg, M.C.; Altman, R.D.; April, K.T.; Benkhalti, M.; Guyatt, G.; McGowan, J.; Towheed, T.; Welch, V.; Wells, G.; Tugwell, P.; et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2012, 64, 465–474. [Google Scholar] [CrossRef] [Green Version]
- Nelson, A.E.; Allen, K.D.; Golightly, Y.; Goode, A.P.; Jordan, J.M. A systematic review of recommendations and guidelines for the management of osteoarthritis: The chronic osteoarthritis management initiative of the U.S. bone and joint initiative. Semin. Arthritis Rheum. 2014, 43, 701–712. [Google Scholar] [CrossRef]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef]
- Zhang, W.; Moskowitz, R.; Nuki, G.; Abramson, S.; Altman, R.; Arden, N.; Bierma-Zeinstra, S.; Brandt, K.; Croft, P.; Doherty, M.; et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthr. Cartil. 2008, 16, 137–162. [Google Scholar] [CrossRef] [Green Version]
- Iversen, M.D.; Schwartz, T.A.; von Heideken, J.; Callahan, L.; Golightly, Y.; Goode, A.; Hill, C.; Huffman, K.; Pathak, A.; Cooke, J.; et al. Sociodemographic and clinical correlates of physical therapy utilization in adults with symptomatic knee osteoarthritis. Phys. Ther. 2018, 98, 670–678. [Google Scholar] [CrossRef]
- Austin, S.; Saag, K.G.; Pisu, M. Healthcare Providers’ Recommendations for Physical Activity among US Arthritis Population: A Cross-Sectional Analysis by Race/Ethnicity. Arthritis 2018, 2018, 2807035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, A.H.; MacDonald, J.H.; Joshi, M.S.; King, P.J. Differences in Perioperative Outcomes and Complications between African American and White Patients after Total Joint Arthroplasty. J. Arthroplast. 2019, 34, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Elsharydah, A.; Embabi, A.S.; Minhajuddin, A.; Joshi, G.P. Racial Disparity in the Perioperative Care for Patients Undergoing Total Knee and Hip Arthroplasty: A Retrospective Propensity-Matched Cohort Study. J. Racial Ethn. Health Disparities 2018, 5, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Cram, P.; Hawker, G.; Matelski, J.; Ravi, B.; Pugely, A.; Gandhi, R.; Jackson, T. Disparities in Knee and Hip Arthroplasty Outcomes: An Observational Analysis of the ACS-NSQIP Clinical Registry. J. Racial Ethn. Health Disparities 2018, 5, 151–161. [Google Scholar] [CrossRef]
- Goodman, S.M.; Parks, M.; McHugh, K.; Fields, K.; Smethurst, R.; Figgie, M.P.; Bass, A.R. Disparities in Outcomes for African Americans and Whites Undergoing Total Knee Arthroplasty: A Systematic Literature Review. J. Rheumatol. 2016, 43, 765–770. [Google Scholar] [CrossRef]
- Singh, V.; Realyvasquez, J.; Kugelman, D.N.; Aggarwal, V.K.; Long, W.J.; Schwarzkopf, R. Does racial background influence outcomes following total joint arthroplasty? J. Clin. Orthop. Trauma 2021, 19, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Roche, M.; Law, T.Y.; Sultan, A.; Umpierrez, E.; Khlopas, A.; Rosas, S.; Kurowicki, J.; Wang, K.; Mont, M.A. Racial Disparities in Revision Total Knee Arthroplasty: Analysis of 125,901 Patients in National US Private Payer Database. J. Racial Ethn. Health Disparities 2019, 6, 101–109. [Google Scholar] [CrossRef]
- Kerman, H.M.; Smith, S.R.; Smith, K.C.; Collins, J.E.; Suter, L.G.; Katz, J.N.; Losina, E. Disparities in total knee replacement: Population losses in quality-adjusted life years due to differential offer, acceptance, and complication rates for Black Americans. Arthritis Care Res. 2018, 70, 1326–1334. [Google Scholar] [CrossRef] [PubMed]
- Goodman, S.M.; Mehta, B.; Zhang, M.; Szymonifka, J.; Nguyen, J.T.; Lee, L.; Figgie, M.P.; Parks, M.L.; Dey, S.A.; Crego, D.; et al. Disparities in Total Hip Arthroplasty Outcomes: Census Tract Data Show Interactions Between Race and Community Deprivation. J. Am. Acad. Orthop. Surg. 2018, 26, e457–e464. [Google Scholar] [CrossRef] [PubMed]
- Karmarkar, T.D.; Maurer, A.; Parks, M.L.; Mason, T.; Bejinez-Eastman, A.; Harrington, M.; Morgan, R.; O’Connor, M.I.; Wood, J.E.; Gaskin, D.J. A Fresh Perspective on a Familiar Problem: Examining Disparities in Knee Osteoarthritis Using a Markov Model. Med. Care 2017, 55, 993–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherf, J. AAOS Now. A Snapshot of U.S. Orthopaedic Surgeons: Results from the 2018 OPUS Survey. 2019. Available online: https://www.aaos.org/aaosnow/2019/sep/youraaos/youraaos01/ (accessed on 12 October 2021).
- Harrington, M.A.; Rankin, E.A.; Ladd, A.L.; Mason, B.S. The Orthopaedic Workforce Is not as Diverse as the Population It Serves: Where Are the Minorities and the Women? AOA Critical Issues Symposium. J. Bone Joint Surg. Am. 2019, 101, e31. [Google Scholar] [CrossRef]
- Ghomrawi, H.M.K.; Funk, R.J.; Parks, M.L.; Owen-Smith, J.; Hollingsworth, J.M. Physician referral patterns and racial disparities in total hip replacement: A network analysis approach. PLoS ONE 2018, 13, e0193014. [Google Scholar] [CrossRef]
- Williams, D.R.; Cooper, L.A. Reducing Racial Inequities in Health: Using What We Already Know to Take Action. Int. J. Environ. Res. Public Health 2019, 16, 606. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Racial and Ethnic Approaches to Community Health (REACH) Program. Available online: https://www.cdc.gov/nccdphp/dnpao/state-local-programs/reach/index.htm (accessed on 12 October 2021).
- Centers for Disease Control and Prevention. Division of Nutrition, Physical Activity, and Obesity. REACH Program Impact. Available online: https://www.cdc.gov/nccdphp/dnpao/state-local-programs/reach/program_impact/index.htm (accessed on 12 October 2021).
- US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. “Healthy People 2030”; Social Determinants of Health Literature Summaries; Access to Health Services. Available online: https://health.gov/healthypeople/objectives-and-data/social-determinants-health/literature-summaries/access-health-services (accessed on 12 October 2021).
- Rottas, M.; Thadeio, P.; Simons, R.; Houck, R.; Gruben, D.; Keller, D.; Scholfield, D.; Soma, K.; Corrigan, B.; Schettino, A.; et al. Demographic diversity of participants in Pfizer sponsored clinical trials in the United States. Contemp. Clin. Trials 2021, 106, 106421. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Expectations | • Black patients have lower levels of expectation for surgical outcomes |
| Social Network | • Black patients are more likely to ask friends or family for advice for severe OA pain |
| Knowledge | • When considering TJA, Black patients are influenced by personal and community knowledge of the procedure |
| Cultural beliefs | • Black patients are more likely to consider prayer as helpful to self-treat knee or hip pain |
| Willingness/preference | • Black patients are less willing to consider or undergo TJA |
| Communication | • Black patients are less satisfied with communication with their orthopedic surgeon |
| Referral bias | • Black patients are less likely to receive a recommendation for TKA, but the effect is no longer significant after adjusting for patient preference for TKA |
| Description of pain | • Black and White patients may use different descriptions for the quality of their knee or hip OA pain, which may lead to differential assessment by healthcare providers of the need for TJA |
| Access | •Insurance coverage and financial limitations explain some of the racial or ethnic variations in total knee arthroplasty (TKA) rates • Black, Hispanic and Asian/Pacific-Islander patients are significantly more likely than White patients to receive TKA at low volume facilities |
| Geographic | •Regional variations may contribute in part to ethnic and racial disparities of TJA utilization - For example, in certain geographic regions, the TKA rate among Black women was significantly lower than that of White women, whereas rates were approximately equal in other regions |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faison, W.E.; Harrell, P.G.; Semel, D. Disparities across Diverse Populations in the Health and Treatment of Patients with Osteoarthritis. Healthcare 2021, 9, 1421. https://doi.org/10.3390/healthcare9111421
Faison WE, Harrell PG, Semel D. Disparities across Diverse Populations in the Health and Treatment of Patients with Osteoarthritis. Healthcare. 2021; 9(11):1421. https://doi.org/10.3390/healthcare9111421
Chicago/Turabian StyleFaison, Warachal E., P. Grace Harrell, and David Semel. 2021. "Disparities across Diverse Populations in the Health and Treatment of Patients with Osteoarthritis" Healthcare 9, no. 11: 1421. https://doi.org/10.3390/healthcare9111421
APA StyleFaison, W. E., Harrell, P. G., & Semel, D. (2021). Disparities across Diverse Populations in the Health and Treatment of Patients with Osteoarthritis. Healthcare, 9(11), 1421. https://doi.org/10.3390/healthcare9111421