
The Role of Vitamin E in Slowing Down Mild Cognitive Impairment: A Narrative Review




Abstract
:1. Introduction
2. Methods
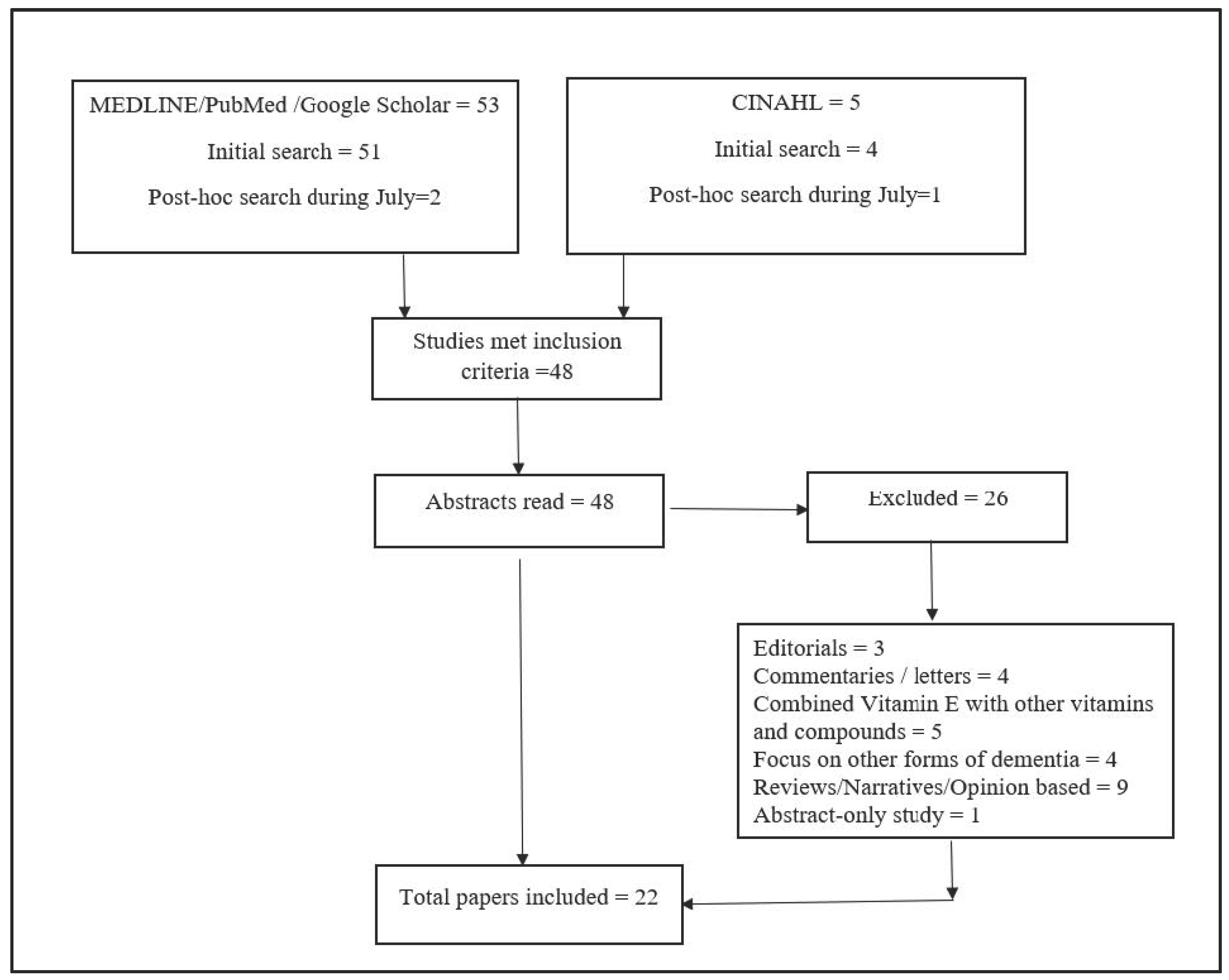
2.1. Search Strategy
2.2. Inclusion Criteria and Data Abstraction
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
| Authors | Year | Study Type | Sample Characteristics | Findings | Intrument Used to Screen Dementia | Conclusions |
|---|---|---|---|---|---|---|
| Wu et al. | 2010 | Experimental study in rats | Rats were fed 500 IU/Kg Vitamin E with their regular diets for four weeks before performing mild fluid percussion injury (FPI). The Vitamin E counter reacted against the effects of fluid percussion injury. | Vitamin E supplementation diet counteracts the molecular substrates underlying synaptic plasticity and cognitive function in the hippocampus. | Not Applicable | Vitamin E dietary supplementation can protect the brain against the effects of mild TBI on synaptic plasticity and cognition. Declines rate of cognitive impairment. |
| Huang et al. | 2010 | Experimental study in mice | The relationship between Vitamin E was observed with protein oxidation in mice. | Protein oxidation and nitration increased in MCI. | Not Applicable | The study suggested that the therapeutic role of vitamin E should be explored in MCI. |
| Alzoubi et al. | 2013 | Experimental, Animal study | The effect of Vitamin E against a high-fat high carbohydrate diet (HFCD) was observed. It is known that HFCD accelerates learning and cognitive impairment. In this study, the HFCD or Vitamin E was administered to animals for 6 weeks. Behavioral activities were conducted to test spatial learning and memory. | Vitamin E prevented memory impairment induced by HFCD and normalized the effect of HFCD on oxidative stress. | Not Applicable | Probably Vitamin E reduces the risk of MCI by reducing probably through normalizing antioxidant mechanisms in the hippocampus. |
| Giraldo et al. | 2014 | In vivo, mice study | The effect of Vitamin E was observed on the inhibition of p38 which prevents Aβ-induced tau phosphorylation that leads to cognitive impairment. | Vitamin E inhibited tau phosphorylation and reduced cognitive impairment. | Not Applicable | Vitamin E has a therapeutic role in protecting the decline of memory impairment. |
| McDougall et al. | 2017 | Animal experimental study | The study examined learning and memory impairment in zebrafish with vitamin E deficient and sufficient.Zebrafish fed with vitamin E for 45 days acquired sufficient vitamin E levels. | Learning ability was observed in association with vitamin E level by excluding the effect of avoidance conditioning and non-associative learning. Zebrafish with low vitamin E were found learning impaired. | Not Applicable | Study proves that vitamin E plays important role in protecting cognitive delay. |
| Nesari et al. | 2019 | Experimental study on rats | The effect of Alpha-tocopherol was evaluated in view of observing its protective effect on long-term memory impairment. | The Alpha-tocopherol reduced the passive avoidance memory performance, increased the level of malondialdehyde (MDE) and reactive oxygen specifies. | Not Applicable | Alpha-tocopherol was found to have a neuroprotective effect on memory impairment. |
| Mehrabadi & Sadr | 2020 | Experimental study on rats | The effect of vitamins D3 and E, in a combination of both, was observed on learning and memory. 60 rats received different doses of vitamins. | Memory and learning were measured by the Novel Object Recognition (NOR) test found to improve in the rat group that received vitamin E. | Not Applicable | Vitamin E can improve learning and memory. |
| Iuliano et al. | 2010 | Case-control, experimental research | An enzymatic relationship between oxysterols (24S-hydroxycholesterol and 27 hydroxycholesterol, free radical related oxysterols of oxidative stress and Vitamin E were compared between 37 patients of Alzheimer’s disease, 24 MCI, 29 multi-domains (md-MCI). | People with mild cognitive impairment with oxidative stress found to be lower in Vitamin E. | Mini Mental State Examination, Mental Deterioration Battery (MDB) | Vitamin E might have some role in reducing oxidative stress delay and cognitive delay. |
| Whitehair et al. | 2010 | Experimental research design | The relationship of Apolipoprotein E ɛ4 (APOE ɛ4) allele was observed for 36 months of the period in 516 MCI patients age between 55 to 90 years who were on Vitamin E in 516 MCI participants aged 55–90 years who received placebo. | Vitamin E did not find to be associated with the progression of Apolipoprotein E ɛ4. | Mini Mental State Examination, Alzheimer’s Disease Assessment Scale-Cognitive subscale (ADAS-cog) | A direct connection between Vitamin E and the decline of cognitive function could not be found. However, the active status of APOE ɛ4 was found associated with a fast decline in cognitive function. |
| Mangialasche et al. | 2012 | Clinical study | This study examined the relationship between 8 natural compounds of Vitamin E with cognitive impairment. 166 MCI subjects were compared with cognitively normal people. | Low plasma tocopherols and tocotrienols levels of vitamin E were found with increased odds of MCI in people with ID. | The Folstein Mini-Mental State Examination (MMSE), Clinical dementia rating scale and Hachinski ischemic scale | Vitamin E may have a role against the progression of MCI to AD. |
| Mangialasche et al. | 2013 | Cohort research design | 140 non-cognitively impaired people were observed for 8 years. The baseline serum vitamin E and cognitive impairment were observed. | The risk of cognitive impairment was found lower among those who had a moderate level of tocopherol/cholesterol ratio than those who had the lowest level of tocopherols. | Mini-Mental State Examination (MMSE) | Vitamin E might play an important role in cognitive impairment in humans. Vitamin E’s therapeutic role should be explored. |
| Shahar et al. | 2013 | Cross-sectional. | The relationship between MCI and Vitamin A and E was explored in a total of 333 participants age 60 years and above. | Vitamin E level was found lower in APOEe4 carriers that affect MCI. | The Folstein Mini-Mental State Examination (MMSE) | The role of vitamin E needs to be further explored in relation to MCI. |
| Dysken et al. | 2014 | Double-blind, placebo-controlled, parallel-group, randomized clinical trial | The effect of vitamin E on the progression of cognitive impairment was examined. 613 patients were recruited. They received either 2000 IU/d of alpha-tocopherol (n = 152), 20 mg/d of memantine (n = 155), the combination (n = 154), or placebo (n = 152). | Activities of Daily Living (ADCS-ADL) Inventory score declined in the group that was given vitamin E. | Activities of Daily Living (ADCS-ADL) Inventory score, Mini-Mental State Examination (MMSE) | Vitamin E can slow down the progression of cognitive impairment. |
| Zanotta, Puricelli & Bonoldi | 2014 | Prospective cohort | The effect of vitamin E in improving cognition in people diagnosed with MCI was assessed. 104 people about 70 years old were included in the research. | Vitamin E as a supplementary dietary found to be counteractive to cognitive impairment. | Alzheimer’s Disease Assessment Scale-Cognitive subscale (ADAS-cog) | Vitamin E may have a role in lowering the risk of MCI. |
| Naeini et al. | 2014 | Double-blind randomized, placebo-controlled trial | 256 elderly, ages between 65 to 75 were received 300 mg vitamin E with 400 mg of vitamin C or placebo for 1 year | Vitamin E reduced the malondialdehyde level and raised total antioxidant capacity and glutathione. | Mini-Mental State Examination (MMSE) | Vitamin E supplementation did not appear to be enhancing cognitive performance |
| Li et al. | 2015 | Prospective cohort | This study examined the effect of vitamin E and C together and both vitamins independently on cognitive functions in the elderly population. 276 elderly people received Vitamin E and C together and E independently. | Radioimmunoassay (RIA) results, MMSE, and HDS assessments indicated improvement in cognitive functions with vitamin E and also when vitamin E was given in combination with Vitamin C. | Mini-mental state examination and Hasegawa Dementia Scale | Vitamin E can improve cognitive functions in the elderly population. |
| De Beaumont et al. | 2016 | Experimental research | The relationship of apolipoprotein E4 (APOE-ɛ4) gene and butyryl cholinesterase (BCHE) was assessed on the effect of cognitive impairment. | The study did not mention vitamin E; however, it was designed on the premise of that lower levels of vitamin E increases apolipoprotein E4 (APOE-ɛ4) and butyryl cholinesterase (BCHE) activity that increases declines memory. | histopathological confirmation of AD according to NINCDS-ADRDA criteria | Vitamin E may have a role in lowering the rate of memory impairment. |
| Basambombo et al. | 2017 | Cohort research design | The effect of Vitamin E and also Vitamin C was observed in a cohort of 5269 individuals aged 65 years and above in the Canadian Study of Health and Aging (1991–2002). | The baseline memory and learning ability were compared on the same standardized tests. Vitamin E and C together and independently were found to be associated with a lower risk of memory decline. | Modified Mini-Mental State (3MS) Examination. | Vitamin E plays a role in reducing the risk of memory decline in individuals. |
| Liu et al. | 2018 | Randomized controlled study | A randomized controlled study in 7781 individuals of European descent. | No association was observed between dietary supplementation of vitamin E with cognitive impairment. | Not available, since this study utilized biomarkers | The study suggests no association between vitamin E supplementation and MCI in the general population. |
| Edmonds et al. | 2018 | Experimental research design | The effect of donepezil and Vitamin E was compared for 756 MCI participants. | The donepezil treatment group had a lower rate of progression from MCI to AD than the Vitamin E group. | The Wechsler Memory Scale–Revised Logical Memory II subtest, Mini-mental state examination. | Vitamin E may not have an effect on lowering the rate of MCI towards AD. |
| Kim et al. | 2018 | Cross-sectional | The effect of serum vitamin A, C, and E was evaluated for the risk of cognitive impairment in 230 participants aged 60 to 79 years. | Association between vitamin A and C serum was not observed while a negative relationship between vitamin E, beta-gamma tocopherol was observed with a lower risk of cognitive impairment. | Korean version of the Mini-Mental State Examination | Serum beta-gamma tocopherol levels tended to be inversely associated with the risk of cognitive impairment. |
| Casati et al. | 2019 | Experimental research design | The relationship between Vitamin E forms and leukocyte telomere length (LTL) in AD was explored for the purpose of knowing its effect on MCI. Vitamin E forms (α-, β-, γ- and δ-tocopherol, α-, β-, γ- and δ-tocotrienol), the ratio of α-tocopherylquinone/α-tocopherol and 5-nitro-γ-tocopherol/γ-tocopherol (markers of oxidative/nitrosative damage) and LTL were measured in 53 AD subjects and 40 cognitively healthy controls (CTs). | People suffering from AD found to have lower concentrations of α-, β-, γ- and δ-tocopherol, α- and δ-tocotrienol, total tocopherols, total tocotrienols, and total vitamin E compared to CTs. | Not available, since this study utilized telomere length as an indicator | The study suggests that Vitamin E deficiency may be playing a role in AD pathology in progressing MCI to AD. |
References
- World Health Organization (WHO). WHO Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 20 November 2020).
- Alzheimer Association. Mild Cognitive Impairment. 2020. Available online: https://www.alz.org/alzheimers-dementia/what-is-dementia/related_conditions/mild-cognitive-impairment (accessed on 21 September 2020).
- Roberts, R.O.; Knopman, D.S.; Mielke, M.M.; Cha, R.H.; Pankratz, V.S.; Christianson, T.J.; Geda, Y.E.; Boeve, B.F.; Ivnik, R.J.; Tangalos, E.G.; et al. Higher risk of progression to dementia in mild cognitive impairment cases who revert to normal. Neurology 2014, 82, 317–325. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Neurology. Update, Mild Cognitive Impairment. Available online: https://www.aan.com/ (accessed on 19 May 2020).
- Sosa, A.L.; Albanese, E.; Stephan, B.; Dewey, M.; Acosta, D.; Ferri, C.; Guerra, M.; Huang, Y.; Jacob, K.S.; Jiménez-Velázquez, I.Z.; et al. Prevalence, distribution, and impact of mild cognitive impairment in Latin America, China, and India: A 10/66 population-based study. PLoS Med. 2012, 9, e1001170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, S.K.; Bose, P.; Biswas, A.; Dutt, A.; Banerjee, T.K.; Hazra, A.; Raut, D.K.; Chaudhuri, A.; Roy, T. An epidemiologic study of mild cognitive impairment in Kolkata, India. Neurology 2007, 68, 2019–2026. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, Y.J.; Zhang, M.; Xu, Z.Q.; Gao, C.Y.; Fang, C.Q.; Yan, J.C.; Zhou, H.D. Vascular risk factors promote conversion from mild cognitive impairment to Alzheimer disease. Neurology 2011, 76, 1485–1491. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.K.; Shahar, S.; Chin, A.-V.; Yusoff, N.A.M.; Rajab, N.; Aziz, S.A. Prevalence of gender disparities and predictors affecting the occurrence of mild cognitive impairment (MCI). Arch. Gerontol. Geriatr. 2012, 54, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.W.; Park, J.H.; Kim, M.-H.; Kim, M.D.; Kim, B.-J.; Kim, S.-K.; Kim, J.L.; Moon, S.W.; Bae, J.N.; Woo, J.I.; et al. A nationwide survey on the prevalence of dementia and mild cognitive impairment in South Korea. J. Alzheimer’s Dis. 2011, 23, 281–291. [Google Scholar] [CrossRef] [Green Version]
- Hale, J.M.; Schneider, D.C.; Mehta, N.K.; Myrskylä, M. Cognitive impairment in the U.S.: Lifetime risk, age at onset, and years impaired. SSM—Popul. Healh 2020, 11, 100577. [Google Scholar] [CrossRef]
- Katz, M.J.; Lipton, R.B.; Hall, C.; Zimmerman, M.E.; Sanders, A.E.; Verghese, J.; Dickson, D.W.; Derby, C.A. Age-specific and sex-specific prevalence and incidence of mild cognitive impairment, dementia, and Alzheimer dementia in blacks and whites: A report from the einstein aging study. Alzheimer Dis. Assoc. Disord. 2012, 26, 335–343. [Google Scholar] [CrossRef]
- McDougall, G.J., Jr.; Vaughan, P.W.; Acee, T.W.; Becker, H. Memory performance and mild cognitive impairment in Black and White community elders. Ethn. Dis. 2007, 17, 381–388. [Google Scholar]
- Langa, K.M.; Levine, D.A. The diagnosis and management of mild cognitive impairment: A clinical review. JAMA 2014, 312, 2551–2561. [Google Scholar] [CrossRef]
- Murman, D.L. The impact of age on cognition. Semin. Hear. 2015, 36, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Teng, E.; Tassniyom, K.; Lu, P.H. Reduced quality-of-life ratings in mild cognitive impairment: Analyses of subject and informant responses. Am. J. Geriatr. Psychiatry 2012, 20, 1016–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connors, M.H.; Seeher, K.; Teixeira-Pinto, A.; Woodward, M.; Ames, D.; Brodaty, H. Mild cognitive impairment and caregiver burden: A 3-year-longitudinal study. Am. J. Geriatr. Psychiatry 2019, 27, 1206–1215. [Google Scholar] [CrossRef] [PubMed]
- Eshkoor, S.A.; Mun, C.Y.; Ng, C.K.; Hamid, T.A. Mild cognitive impairment and its management in older people. Clin. Interv. Aging 2015, 10, 687–693. [Google Scholar] [CrossRef] [Green Version]
- Vega, J.; Newhouse, P.A. Mild cognitive impairment: Diagnosis, longitudinal course, and emerging treatments. Curr. Psychiatry Rep. 2014, 16, 490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farina, N.; Llewellyn, D.; Isaac, M.G.E.K.N.; Tabet, N. Vitamin E for Alzheimer’s dementia and mild cognitive impairment. Cochrane Database Syst. Rev. 2017, 4, CD002854. [Google Scholar] [CrossRef]
- Wu, A.; Ying, Z.; Gomez-Pinilla, F. Vitamin E protects against oxidative damage and learning disability after mild traumatic brain injury in rats. Neurorehabilit. Neural Repair 2009, 24, 290–298. [Google Scholar] [CrossRef] [Green Version]
- Huang, Q.; Aluise, C.D.; Joshi, G.; Sultana, R.; Clair, D.K.S.; Markesbery, W.R.; Butterfield, D.A. Potential in vivo amelioration by N-acetyl-L-cysteine of oxidative stress in brain in human double mutant APP/PS-1 knock-in mice: Toward therapeutic modulation of mild cognitive impairment. J. Neurosci. Res. 2010, 88, 2618–2629. [Google Scholar] [CrossRef]
- Alzoubi, K.H.; Khabour, O.F.; Salah, H.A.; Hasan, Z. Vitamin E prevents high-fat high-carbohydrates diet-induced memory impairment: The role of oxidative stress. Physiol. Behav. 2013, 119, 72–78. [Google Scholar] [CrossRef]
- Giraldo, E.; Lloret, A.; Fuchsberger, T.; Vina, J. Aβ and tau toxicities in Alzheimer’s are linked via oxidative stress-induced p38 activation: Protective role of vitamin E. Redox Biol. 2014, 2, 873–877. [Google Scholar] [CrossRef] [Green Version]
- Nesari, A.; Mansouri, M.T.; Khodayar, M.J.; Rezaei, M. Preadministration of high-dose alpha-tocopherol improved memory impairment and mitochondrial dysfunction induced by proteasome inhibition in rat hippocampus. Nutr. Neurosci. 2021, 24, 119–129. [Google Scholar] [CrossRef]
- Mehrabadi, S.; Sadr, S.S. Administration of Vitamin D3 and E supplements reduces neuronal loss and oxidative stress in a model of rats with Alzheimer’s disease. Neurol. Res. 2020, 42, 862–868. [Google Scholar] [CrossRef]
- Iuliano, L.; Monticolo, R.; Straface, G.; Spoletini, I.; Gianni, W.; Caltagirone, C.; Bossu, P.; Spalletta, G. Vitamin E and enzymatic/oxidative stress-driven oxysterols in amnestic mild cognitive impairment subtypes and Alzheimer’s disease. J. Alzheimer’s Dis. 2010, 21, 1383–1392. [Google Scholar] [CrossRef]
- Whitehair, D.C.; Sherzai, A.; Emond, J.; Raman, R.; Aisen, P.S.; Petersen, R.C.; Fleisher, A.S. Alzheimer’s disease cooperative study influence of apolipoprotein E ɛ4 on rates of cognitive and functional decline in mild cognitive impairment. Alzheimer’s Dement. 2010, 6, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangialasche, F.; Xu, W.; Kivipelto, M.; Costanzi, E.; Ercolani, S.; Pigliautile, M.; Cecchetti, R.; Baglioni, M.; Simmons, A.; Soininen, H.; et al. Tocopherols and tocotrienols plasma levels are associated with cognitive impairment. Neurobiol. Aging 2012, 33, 2282–2290. [Google Scholar] [CrossRef] [PubMed]
- Mangialasche, F.; Solomon, A.; Kåreholt, I.; Hooshmand, B.; Cecchetti, R.; Fratiglioni, L.; Soininen, H.; Laatikainen, T.; Mecocci, P.; Kivipelto, M. Serum levels of vitamin E forms and risk of cognitive impairment in a Finnish cohort of older adults. Exp. Gerontol. 2013, 48, 1428–1435. [Google Scholar] [CrossRef] [PubMed]
- Shahar, S.; Lee, L.K.; Rajab, N.; Lim, C.L.; Harun, N.A.; Noh, M.F.N.M.; Mian-Then, S.; Jamal, R. Association between vitamin A, vitamin E and apolipoprotein E status with mild cognitive impairment among elderly people in low-cost residential areas. Nutr. Neurosci. 2013, 16, 6–12. [Google Scholar] [CrossRef]
- Dysken, M.W.; Sano, M.; Asthana, S.; Vertrees, J.E.; Pallaki, M.; Llorente, M.; Love, S.; Schellenberg, G.D.; McCarten, J.R.; Malphurs, J.; et al. Effect of vitamin E and memantine on functional decline in Alzheimer disease: The TEAM-AD VA cooperative randomized trial. JAMA 2014, 311, 33–44. [Google Scholar] [CrossRef]
- Zanotta, D.; Puricelli, S.; Bonoldi, G. Cognitive effects of a dietary supplement made from extract of Bacopa monnieri, astaxanthin, phosphatidylserine, and vitamin E in subjects with mild cognitive impairment: A noncomparative, exploratory clinical study. Neuropsychiatr. Dis. Treat. 2014, 10, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Naeini, A.M.A.; Elmadfa, I.; Djazayery, A.; Barekatain, M.; Ghazvini, M.R.A.; Djalali, M.; Feizi, A. The effect of antioxidant vitamins E and C on cognitive performance of the elderly with mild cognitive impairment in Isfahan, Iran: A double-blind, randomized, placebo-controlled trial. Eur. J. Nutr. 2013, 53, 1255–1262. [Google Scholar] [CrossRef]
- De Beaumont, L.; Pelleieux, S.; Lamarre-Theroux, L.; Dea, D.; Poirier, J. Butyrylcholinesterase K and apolipoprotein E-ɛ4 reduce the age of onset of Alzheimer’s disease, accelerate cognitive decline, and modulate donepezil response in mild cognitively impaired subjects. J. Alzheimer’s Dis. 2016, 54, 913–922. [Google Scholar] [CrossRef] [PubMed]
- Basambombo, L.L.; Carmichael, P.-H.; Côté, S.; Laurin, D. Use of vitamin E and C supplements for the prevention of cognitive decline. Ann. Pharmacother. 2016, 51, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Zhao, Y.; Jin, S.; Hu, Y.; Wang, T.; Tian, R.; Han, Z.; Xu, D.; Jiang, Q. Circulating vitamin E levels and Alzheimer’s disease: A mendelian randomization study. Neurobiol. Aging 2018, 72, 189-e1. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liu, S.; Man, Y.; Li, N.; Zhou, Y.U. Effects of vitamins E and C combined with β-carotene on cognitive function in the elderly. Exp. Ther. Med. 2015, 9, 1489–1493. [Google Scholar] [CrossRef] [Green Version]
- Edmonds, E.C.; Ard, M.C.; Edland, S.D.; Galasko, D.R.; Salmon, D.P.; Bondi, M.W. Unmasking the benefits of donepezil via psychometrically precise identification of mild cognitive impairment: A secondary analysis of the ADCS vitamin E and donepezil in MCI study. Alzheimer’s Dement. 2018, 4, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Casati, M.; Boccardi, V.; Ferri, E.; Bertagnoli, L.; Bastiani, P.; Ciccone, S.; Mansi, M.; Scamosci, M.; Rossi, P.D.; Mecocci, P.; et al. Vitamin E and Alzheimer’s disease: The mediating role of cellular aging. Aging Clin. Exp. Res. 2019, 32, 459–464. [Google Scholar] [CrossRef]
- Kim, S.H.; Park, Y.M.; Choi, B.Y.; Kim, M.K.; Roh, S.; Kim, K.; Yang, Y.J. Associations of serum levels of vitamins A, C, and E with the risk of cognitive impairment among elderly Koreans. Nutr. Res. Pract. 2018, 12, 160–165. [Google Scholar] [CrossRef] [Green Version]
- McDougall, M.; Choi, J.; Magnusson, K.; Truong, L.; Tanguay, R.; Traber, M.G. Chronic vitamin E deficiency impairs cognitive function in adult zebrafish via dysregulation of brain lipids and energy metabolism. Free Radic. Biol. Med. 2017, 112, 308–317. [Google Scholar] [CrossRef]
- Pace, A.; Savarese, A.; Picardo, M.; Maresca, V.; Pacetti, U.; Del Monte, G.; Biroccio, A.; Leonetti, C.; Jandolo, B.; Cognetti, F.; et al. Neuroprotective effect of vitamin E supplementation in patients teated with cisplatin chemotherapy. J. Clin. Oncol. 2003, 21, 927–931. [Google Scholar] [CrossRef]
- Gugliandolo, A.; Bramanti, P.; Mazzon, E. Role of vitamin E in the treatment of Alzheimer’s disease: Evidence from animal models. Int. J. Mol. Sci. 2017, 18, 2504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Torre, M.E.; Villano, I.; Monda, M.; Messina, A.; Cibelli, G.; Valenzano, A.; Pisanelli, D.; Panaro, M.A.; Tartaglia, N.; Ambrosi, A.; et al. Role of vitamin E and the orexin system in neuroprotection. Brain Sci. 2021, 11, 1098. [Google Scholar] [CrossRef] [PubMed]
- Kaneai, N.; Arai, M.; Takatsu, H.; Fukui, K.; Urano, S. Vitamin E inhibits oxidative stress-induced denaturation of nerve terminal proteins involved in neurotransmission. J. Alzheimer’s Dis. 2012, 28, 183–189. [Google Scholar] [CrossRef] [PubMed]
- La Fata, G.; Weber, P.; Mohajeri, M.H. Effects of vitamin E on cognitive performance during ageing and in Alzheimer’s disease. Nutrients 2014, 6, 5453–5472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lloret, A.; Badía, M.-C.; Mora, N.J.; Pallardó, F.V.; Alonso, M.-D.; Viña, J. Vitamin E paradox in Alzheimer’s disease: It does not prevent loss of cognition and may even be detrimental. J. Alzheimer’s Dis. 2009, 17, 143–149. [Google Scholar] [CrossRef]

| Main Term | Related Terms Used |
|---|---|
| Vitamin E | Tocopherol * OR D1 alpha tocopherol OR Preventive therapy OR tocotrienols OR Aquasol E OR Antioxidant |
| AND | |
| Mild cognitive impairment | Dementia OR Alzheimer’s disease OR Cognitive decline OR Amentia OR Mental disorder OR Paranoid Dementia OR Senile Paranoid |
| Categories | Delay or a Lower Rate of Cognitive Decline or Neuroprotective Effect | Improved Learning and Memory Functions | May Be Effective | Suggest Further Exploration | No Effect | |
|---|---|---|---|---|---|---|
| Animals | Rats (n = 3) | 3 | ||||
| Mice (n = 2) | 1 | 1 | ||||
| Other animals (n = 2) | 2 | |||||
| Human | Cross-sectional (n = 1) | 1 | ||||
| Case-control (n = 1) | 1 | |||||
| Cohort (prospective) (n = 3) | 2 | 1 | ||||
| Experimental (n = 4) | 2 | 2 | ||||
| Clinical (n = 2) | 2 | 1 | ||||
| Double-blind, randomized, placebo-controlled (n = 4) | 1 | 1 | 2 | |||
| Total (n = 22) | 15 | 2 | 1 | 1 | 4 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lakhan, R.; Sharma, M.; Batra, K.; Beatty, F.B. The Role of Vitamin E in Slowing Down Mild Cognitive Impairment: A Narrative Review. Healthcare 2021, 9, 1573. https://doi.org/10.3390/healthcare9111573
Lakhan R, Sharma M, Batra K, Beatty FB. The Role of Vitamin E in Slowing Down Mild Cognitive Impairment: A Narrative Review. Healthcare. 2021; 9(11):1573. https://doi.org/10.3390/healthcare9111573
Chicago/Turabian StyleLakhan, Ram, Manoj Sharma, Kavita Batra, and Frazier B. Beatty. 2021. "The Role of Vitamin E in Slowing Down Mild Cognitive Impairment: A Narrative Review" Healthcare 9, no. 11: 1573. https://doi.org/10.3390/healthcare9111573
APA StyleLakhan, R., Sharma, M., Batra, K., & Beatty, F. B. (2021). The Role of Vitamin E in Slowing Down Mild Cognitive Impairment: A Narrative Review. Healthcare, 9(11), 1573. https://doi.org/10.3390/healthcare9111573