
A Local Survey of COVID-19: Vaccine Potential Acceptance Rate among Personnel in a Level 1 Trauma Center without Severe COVID-19 Cases


Abstract
:1. Introduction
1.1. Importance of HCWs
1.1.1. General Knowledge and Attitudes of HCW towards Vaccination
1.1.2. The Vaccine Hesitancy (VH) among Healthcare Workers
1.2. Vaccine
1.3. Vaccination Acceptance
1.4. The Vaccine in Germany
2. Methods
2.1. Study Design
2.2. 5C Model
2.3. Statistics
3. Results
3.1. Sociodemographic Characteristics
3.2. Survey on Vaccination Readiness
3.3. Effects of COVID-19 Demands on Vaccination Intention with Work Stress
3.4. Validity of the 5C Model in COVID-19 Vaccine Intention
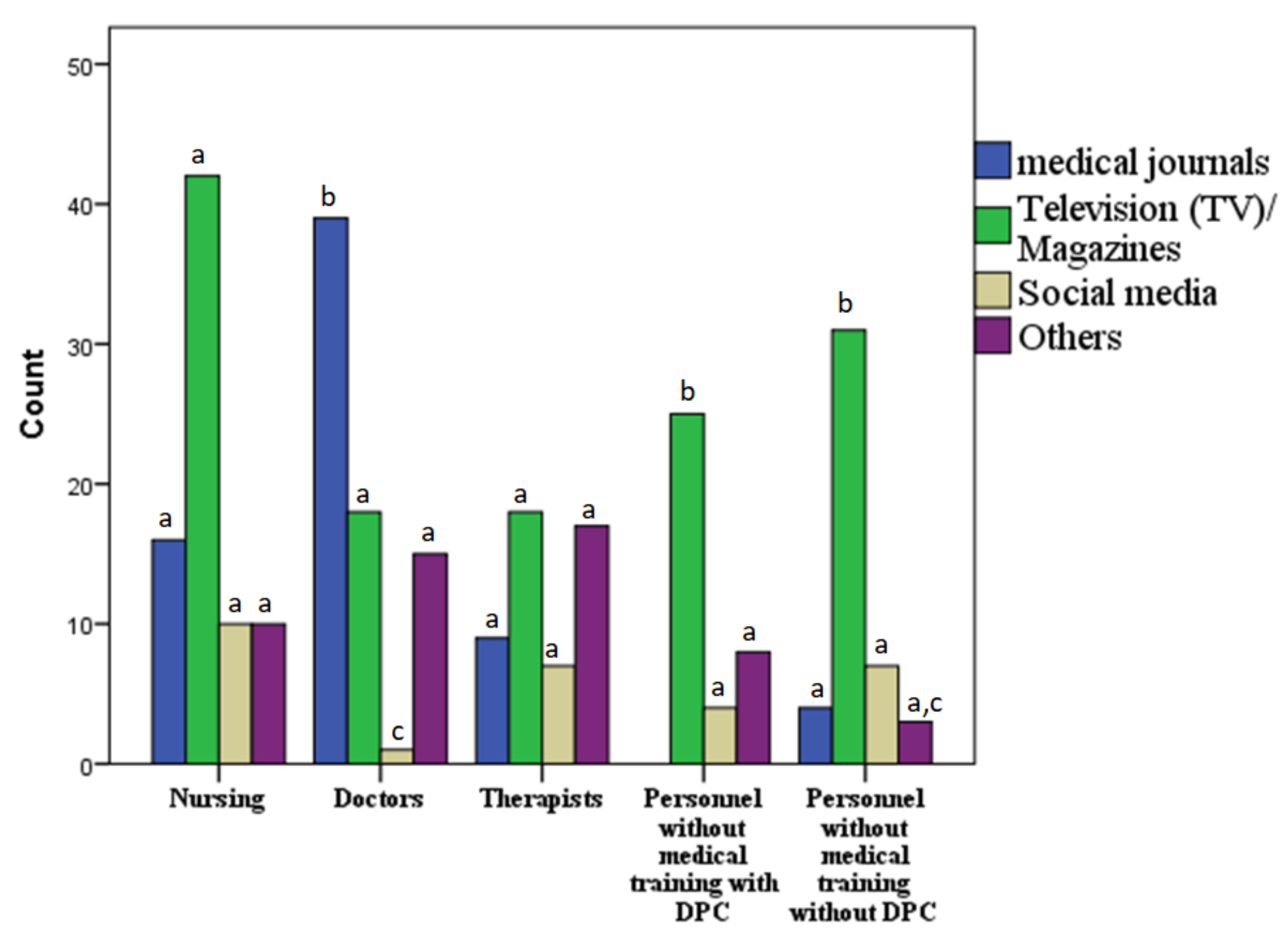
3.5. Source of Information of the COVID-19 Pandemic
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| HCWs | Healthcare workers |
| DPC | Direct patient contact |
| TV | Television |
| KMO | Kaiser–Meyer–Olkin |
References
- Dashraath, P.; Wong, J.L.J.; Lim, M.X.K.; Lim, L.M.; Li, S.; Biswas, A.; Choolani, M.; Mattar, C.; Su, L.L. Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. Am. J. Obstet. Gynecol. 2020, 222, 521–531. [Google Scholar] [CrossRef]
- Baker, M.G.; Kvalsvig, A.; Verrall, A.J. New Zealand’s COVID-19 elimination strategy. Med. J. Aust. 2020, 213, 198–200. [Google Scholar] [CrossRef]
- Zheng, L.; Wang, X.; Zhou, C.; Liu, Q.; Li, S.; Sun, Q.; Wang, M.; Zhou, Q.; Wang, W. Analysis of the Infection Status of Healthcare Workers in Wuhan During the COVID-19 Outbreak: A Cross-sectional Study. Clin. Infect. Dis. 2020, 71, 2109–2113. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Fang, M.; Chen, Q.; He, B. SARS, MERS and COVID-19 among healthcare workers: A narrative review. J. Infect. Public Health 2020, 13, 843–848. [Google Scholar] [CrossRef]
- La Torre, G.; Scalingi, S.; Garruto, V.; Siclari, M.; Chiarini, M.; Mannocci, A. Knowledge, attitude and behaviours towards recommended vaccinations among healthcare workers. Healthcare 2017, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Mattia, G.; Anna, I.; Alice, B.; Riccardo, M.; Stefania, C.; Alessandra, G. Who Is Willing to Get Vaccinated? A Study into the Psychological, Socio-Demographic, and Cultural Determinants of COVID-19 Vaccination Intentions. Vaccines 2021, 9, 810. [Google Scholar]
- Ling, Y.; Zhong, J.; Luo, J. Safety and effectiveness of SARS-CoV-2 vaccines: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 6486–6495. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Whittington, J.; Yuan, H.-Y.; Miao, H.; Tian, H.; Stenseth, N.C. Evaluating the effectiveness of control measures in multiple regions during the early phase of the COVID-19 pandemic in 2020. Biosaf. Health 2021, 3, 264–275. [Google Scholar] [CrossRef]
- Arce, J.S.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Armand, A.; et al. medRxiv 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.03.11.21253419v1.full.pdf (accessed on 10 September 2021).
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing Covid-19 Vaccines at Pandemic Speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- To, K.; Lai, A.; Lee, K.; Koh, D.; Lee, S. Increasing the coverage of influenza vaccination in healthcare workers: Review of challenges and solutions. J. Hosp. Infect. 2016, 94, 133–142. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Theodoridou, K.; Ledda, C.; Rapisarda, V.; Theodoridou, M. Vaccination of healthcare workers: Is mandatory vaccination needed? Expert Rev. Vaccines 2019, 18, 5–13. [Google Scholar] [CrossRef]
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; Suk, J.; Celentano, L.P.; Kramarz, P.; Larson, H.J. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef] [PubMed]
- Verger, P.; Fressard, L.; Collange, F.; Gautier, A.; Jestin, C.; Launay, O.; Raude, J.; Pulcini, C.; Peretti-Watel, P. Vaccine Hesitancy Among General Practitioners and Its Determinants During Controversies: A National Cross-sectional Survey in France. EBioMedicine 2015, 2, 891–897. [Google Scholar] [CrossRef] [Green Version]
- Sundaram, N.; Duckett, K.; Yung, C.F.; Thoon, K.C.; Sidharta, S.; Venkatachalam, I.; Chow, A.; Yoong, J. “I wouldn’t really believe statistics”–Challenges with influenza vaccine acceptance among healthcare workers in Singapore. Vaccine 2018, 36, 1996–2004. [Google Scholar] [CrossRef] [PubMed]
- Chor, J.S.Y.; Ngai, K.L.; Goggins, W.B.; Wong, M.C.; Wong, S.Y.S.; Lee, N.; Leung, T.-F.; Rainer, T.; Griffiths, S.; Chan, P.K.S. Willingness of Hong Kong healthcare workers to accept pre-pandemic influenza vaccination at different WHO alert levels: Two questionnaire surveys. BMJ 2009, 339, b3391. [Google Scholar] [CrossRef] [Green Version]
- Rachiotis, G.; Mouchtouri, V.A.; Kremastinou, J.; Gourgoulianis, K.; Hadjichristodoulou, C. Low acceptance of vaccination against the 2009 pandemic influenza A(H1N1) among healthcare workers in Greece. Eurosurveillance 2010, 15, 19486. [Google Scholar] [CrossRef] [PubMed]
- Forni, G.; Mantovani, A. COVID-19 vaccines: Where we stand and challenges ahead. Cell Death Differ. 2021, 28, 626–639. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Draft Landscape of COVID-19 Candidate Vaccines; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Akst, J. COVID-19 vaccine frontrunners. Scientist 2020, 7, 1. [Google Scholar]
- Krammer, F. SARS-CoV-2 vaccines in development. Nature 2020, 586, 516–527. [Google Scholar] [CrossRef]
- SteelFisher, G.K.; Blendon, R.J.; Caporello, H. An Uncertain Public—Encouraging Acceptance of Covid-19 Vaccines. N. Engl. J. Med. 2021, 384, 1483–1487. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Global, M.W. How Does the World Feel about Science and Health; GALLUP: London, UK, 2018. [Google Scholar]
- Amit, S.; Beni, S.A.; Biber, A.; Grinberg, A.; Leshem, E.; Regev-Yochay, G. Post-Vaccination COVID-19 among Healthcare Workers, Israel. Emerg. Infect. Dis. 2021, 27, 1220–1222. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Knight, B. COVID: German Regulations on Who Gets Vaccine First 2020. Available online: https://www.dw.com/en/covid-german-regulations-on-who-gets-vaccine-first/a-55987647 (accessed on 10 April 2021).
- Cinelli, M.; Quattrociocchi, W.; Galeazzi, A.; Valensise, C.M.; Brugnoli, E.; Schmidt, A.L.; Zola, P.; Zollo, F.; Scala, A. The COVID-19 social media infodemic. Sci. Rep. 2020, 10, 1–10. [Google Scholar]
- Gallotti, R.; Valle, F.; Castaldo, N.; Sacco, P.; De Domenico, M. Assessing the risks of ‘infodemics’ in response to COVID-19 epidemics. Nat. Hum. Behav. 2020, 4, 1285–1293. [Google Scholar] [CrossRef]
- Bendau, A.; Petzold, M.B.; Pyrkosch, L.; Maricic, L.M.; Betzler, F.; Rogoll, J.; Große, J.; Ströhle, A.; Plag, J. Associations between COVID-19 related media consumption and symptoms of anxiety, depression and COVID-19 related fear in the general population in Germany. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 283–291. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [Green Version]
- Khatana, S.A.M.; Groeneveld, P.W. Health Disparities and the Coronavirus Disease 2019 (COVID-19) Pandemic in the USA. J. Gen. Intern. Med. 2020, 35, 2431–2432. [Google Scholar] [CrossRef]
- Pérez-López, F.R.; Tajada, M.; Savirón-Cornudella, R.; Sánchez-Prieto, M.; Chedraui, P.; Terán, E. Coronavirus disease 2019 and gender-related mortality in European countries: A meta-analysis. Maturitas 2020, 141, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Szmyd, B.; Karuga, F.F.; Bartoszek, A.; Staniecka, K.; Siwecka, N.; Bartoszek, A.; Błaszczyk, M.; Radek, M. Attitude and behaviors towards SARS-CoV-2 vaccination among healthcare workers: A cross-sectional study from Poland. Vaccines 2021, 9, 218. [Google Scholar] [CrossRef]
- Sun, Y.; Chen, X.; Cao, M.; Xiang, T.; Zhang, J.; Wang, P.; Dai, H. Will Healthcare Workers Accept a COVID-19 Vaccine When It Becomes Available? A Cross-Sectional Study in China. Front. Public Health 2021, 9, 609. [Google Scholar] [CrossRef]
- Fakonti, G.; Kyprianidou, M.; Toumbis, G.; Giannakou, K. Attitudes and Acceptance of COVID-19 Vaccination Among Nurses and Midwives in Cyprus: A Cross-Sectional Survey. Front. Public Health 2021, 9, 481. [Google Scholar] [CrossRef] [PubMed]
- Oruç, M.A.; Öztürk, O. Attitudes of health care professionals towards COVID-19 vaccine—A sequence from Turkey. Hum. Vaccines Immunother. 2021, 17, 3377–3383. [Google Scholar] [CrossRef]
- Shekhar, R.; Sheikh, A.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 Vaccine Acceptance among Health Care Workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef]
- Nohl, A.; Afflerbach, C.; Lurz, C.; Brune, B.; Ohmann, T.; Weichert, V.; Zeiger, S.; Dudda, M. Acceptance of COVID-19 Vaccination among Front-Line Health Care Workers: A Nationwide Survey of Emergency Medical Services Personnel from Germany. Vaccines 2021, 9, 424. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Al-Mohaithef, M.; Padhi, B.K. Determinants of COVID-19 Vaccine Acceptance in Saudi Arabia: A Web-Based National Survey. J. Multidiscip. Healthc. 2020, 13, 1657. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.-K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Ali, M.Y.; Bhatti, R. COVID-19 (Coronavirus) Pandemic: Information Sources Channels for the Public Health Awareness. Asia Pac. J. Public Health 2020, 32, 168–169. [Google Scholar] [CrossRef]
- Geldsetzer, P. Knowledge and Perceptions of COVID-19 Among the General Public in the United States and the United Kingdom: A Cross-sectional Online Survey. Ann. Intern. Med. 2020, 173, 157–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sari, D.K.; Amelia, R.; Dharmajaya, R.; Sari, L.M.; Fitri, N.K. Positive Correlation Between General Public Knowledge and Attitudes Regarding COVID-19 Outbreak 1 Month After First Cases Reported in Indonesia. J. Community Health 2021, 46, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Bhagavathula, A.S.; AlDhaleei, W.A.; Rahmani, J.; Mahabadi, M.A.; Bandari, D.K. Knowledge and Perceptions of COVID-19 Among Health Care Workers: Cross-Sectional Study. JMIR Public Health Surveill. 2020, 6, e19160. [Google Scholar] [CrossRef] [PubMed]
- Bhagavathula, A.S.; Aldhaleei, W.A.; Rahmani, J.; Mahabadi, M.A.; Bandari, D.K.; Novel Coronavirus (COVID-19) Knowledge and Perceptions: A Survey on Healthcare Workers. MedRxiv 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.03.09.20033381v2 (accessed on 10 August 2021).
- Sathianathan, S.; Van Scoy, L.J.; Sakya, S.M.; Miller, E.; Snyder, B.; Wasserman, E.; Chinchilli, V.M.; Garman, J.; Lennon, R.P. Knowledge, Perceptions, and Preferred Information Sources Related to COVID-19 Among Healthcare Workers: Results of a Cross Sectional Survey. Am. J. Health Promot. 2021, 35, 633–636. [Google Scholar] [CrossRef] [PubMed]
- Sakya, S.M.; Van Scoy, L.J.; Garman, J.C.; Miller, E.L.; Snyder, B.; Wasserman, E.; Chinchilli, V.M.; Lennon, R.P. The impact of COVID-19-related changes in media consumption on public knowledge: Results of a cross-sectional survey of Pennsylvania adults. Curr. Med. Res. Opin. 2021, 37, 911–915. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Items | Respondents (n = 285) n (%) |
|---|---|
| Gender | |
| Female | 196 (68.8) |
| Male | 89 (31.2) |
| Age group in years | |
| 0–19 | 1 (0.4) |
| 20–29 | 46 (16.1) |
| 30–39 | 67 (23.5) |
| 40–49 | 59 (20.7) |
| 50–59 | 83 (29.1) |
| 60–69 | 25 (8.8) |
| Occupation | |
| Nursing | 90 (31.6) |
| Doctors | 64 (22.5) |
| Therapists | 49 (17.2) |
| Personnel without medical training with direct patient contact (e.g., reception workers, staff of patient registration, cleaning staff and post workers) | 31 (10.9) |
| Personnel without medical training without direct patient contact (e.g., IT workers, research and finance department and HR department) | 51 (17.9) |
| Variables | Count | Percentage (%) | STD | p-Value |
|---|---|---|---|---|
| (n) | ||||
| Confidence | ||||
| I am completely confident that vaccines are safe | 285 | 62.1 | 34.1 | 0.001 |
| Vaccinations are effective | 285 | 67.8 | 27.02 | 0.049 |
| Regarding vaccines, I am confident that public authorities decide in the best interest of the community | 284 | 64.6 | 31.9 | 0.211 |
| Complacency | ||||
| Vaccination is unnecessary because vaccine-preventable diseases are not common anymore | 284 | 6.02 | 16.0 | 0.035 |
| My immune system is so strong, it also protects me against diseases | 284 | 15. 09 | 22.06 | 0.002 |
| Vaccine-preventable diseases are not so severe that I should get vaccinated | 284 | 10. 06 | 19.07 | 0.002 |
| Constraints | ||||
| Everyday stress prevents me from getting vaccinated | 284 | 05. 04 | 15.06 | 0.069 |
| For me, it is inconvenient to receive vaccinations | 284 | 11.0 | 22.0 | 0.014 |
| Visiting the doctors’ makes me feel uncomfortable; this keeps me from getting vaccinated | 284 | 5.0 | 15.04 | 0.05 |
| Calculation | ||||
| When I think about getting be vaccinated, I weigh benefits and risks to make the best decision possible | 284 | 84.5 | 24.05 | 0.004 |
| For each and every vaccination, I closely consider whether it is useful for me | 284 | 80.1 | 29.05 | 0.228 |
| It is important for me to fully understand the topic of vaccination, before I get vaccinated | 284 | 86.3 | 20.09 | 0.001 |
| Collective responsibility | ||||
| When everyone is vaccinated, I don’t have to get vaccinated, too | 284 | 69 | 12.07 | 0.001 |
| I get vaccinated because I can also protect people with a weaker immune system | 284 | 78.1 | 33.5 | 0.30 |
| Vaccination is a collective action to prevent the spread of diseases | 284 | 85.1 | 25.09 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nohl, A.; Ben Abdallah, H.; Weichert, V.; Zeiger, S.; Ohmann, T.; Dudda, M. A Local Survey of COVID-19: Vaccine Potential Acceptance Rate among Personnel in a Level 1 Trauma Center without Severe COVID-19 Cases. Healthcare 2021, 9, 1616. https://doi.org/10.3390/healthcare9121616
Nohl A, Ben Abdallah H, Weichert V, Zeiger S, Ohmann T, Dudda M. A Local Survey of COVID-19: Vaccine Potential Acceptance Rate among Personnel in a Level 1 Trauma Center without Severe COVID-19 Cases. Healthcare. 2021; 9(12):1616. https://doi.org/10.3390/healthcare9121616
Chicago/Turabian StyleNohl, André, Heithem Ben Abdallah, Veronika Weichert, Sascha Zeiger, Tobias Ohmann, and Marcel Dudda. 2021. "A Local Survey of COVID-19: Vaccine Potential Acceptance Rate among Personnel in a Level 1 Trauma Center without Severe COVID-19 Cases" Healthcare 9, no. 12: 1616. https://doi.org/10.3390/healthcare9121616
APA StyleNohl, A., Ben Abdallah, H., Weichert, V., Zeiger, S., Ohmann, T., & Dudda, M. (2021). A Local Survey of COVID-19: Vaccine Potential Acceptance Rate among Personnel in a Level 1 Trauma Center without Severe COVID-19 Cases. Healthcare, 9(12), 1616. https://doi.org/10.3390/healthcare9121616