
Buccal Bone Thickness in Anterior and Posterior Teeth—A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Process
2.3. Eligibility Criteria
- Human randomized clinical trials, nonrandomized clinical trials, cohort studies, case-control studies, and case series (prospective or retrospective);
- Studies reporting BBT in healthy, adult patients as dimension between tooth and outer border of the buccal bone;
- Studies measuring bone thickness by (cone beam) computed tomography.
- Case reports, systematic and narrative reviews, animal studies, human cadaver studies, editorial, and doctoral theses;
- Patients with dental implants;
- Patients with periodontitis, cleft palate, osteoporosis, dysgnathia, skeletal malocclusion, post-augmentation, post-extraction, and impacted teeth;
- Languages other than English, German, French, and Chinese.
2.4. Data Items
2.5. Risk of Bias Assessment
2.6. The Detailed Approach
- 1.
- To provide the mean and the standard deviation that are obtained by pooling all measurement points pertaining to the same aggregated region.
- 2.
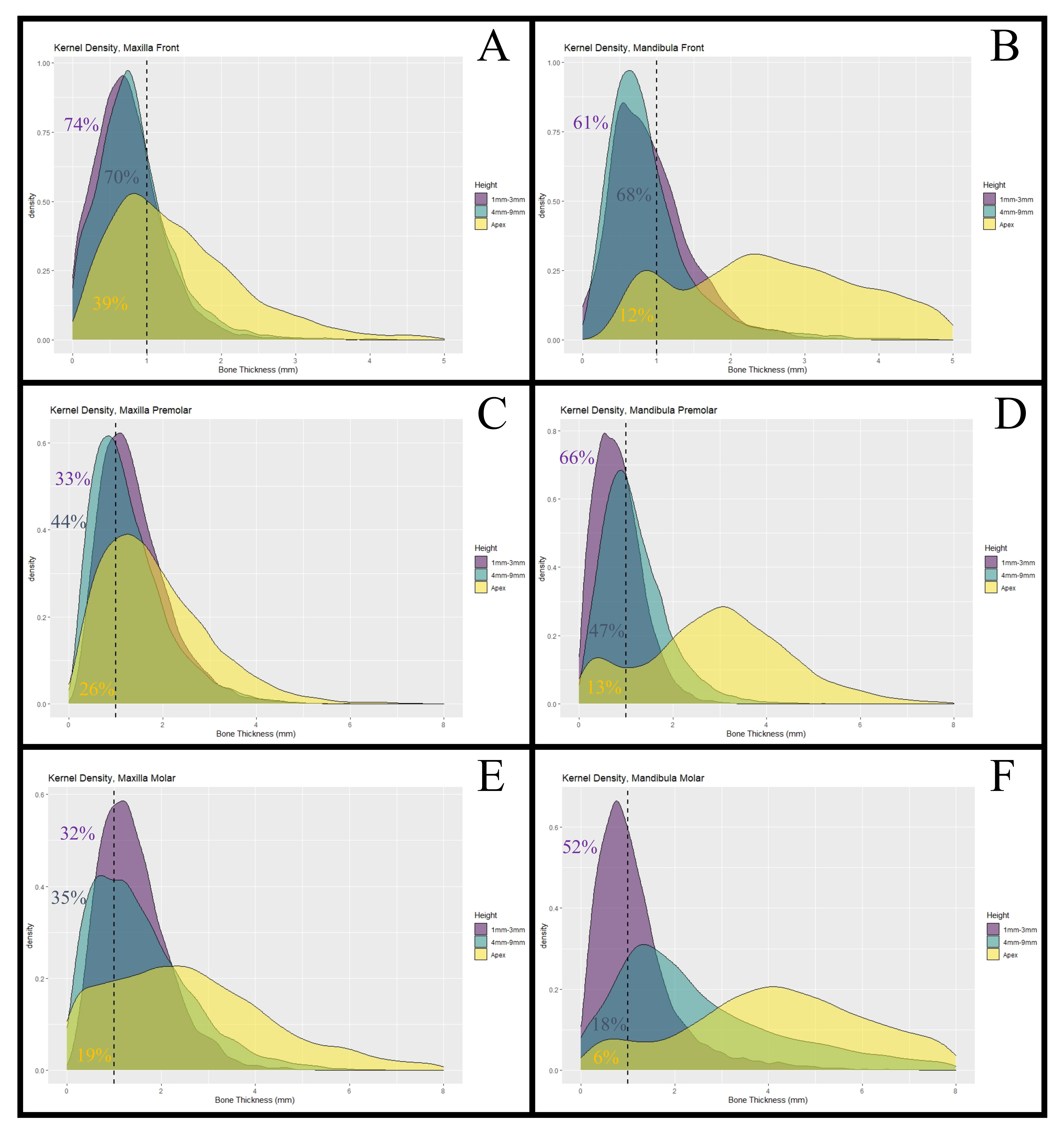
- To approximate the 18 distributions, from which the respective BBTs are assumed to have been generated, and thereby estimate the proportions of BBTs that are smaller than 1 mm.
2.7. Statistics
2.8. Research Reporting Guidelines
3. Results
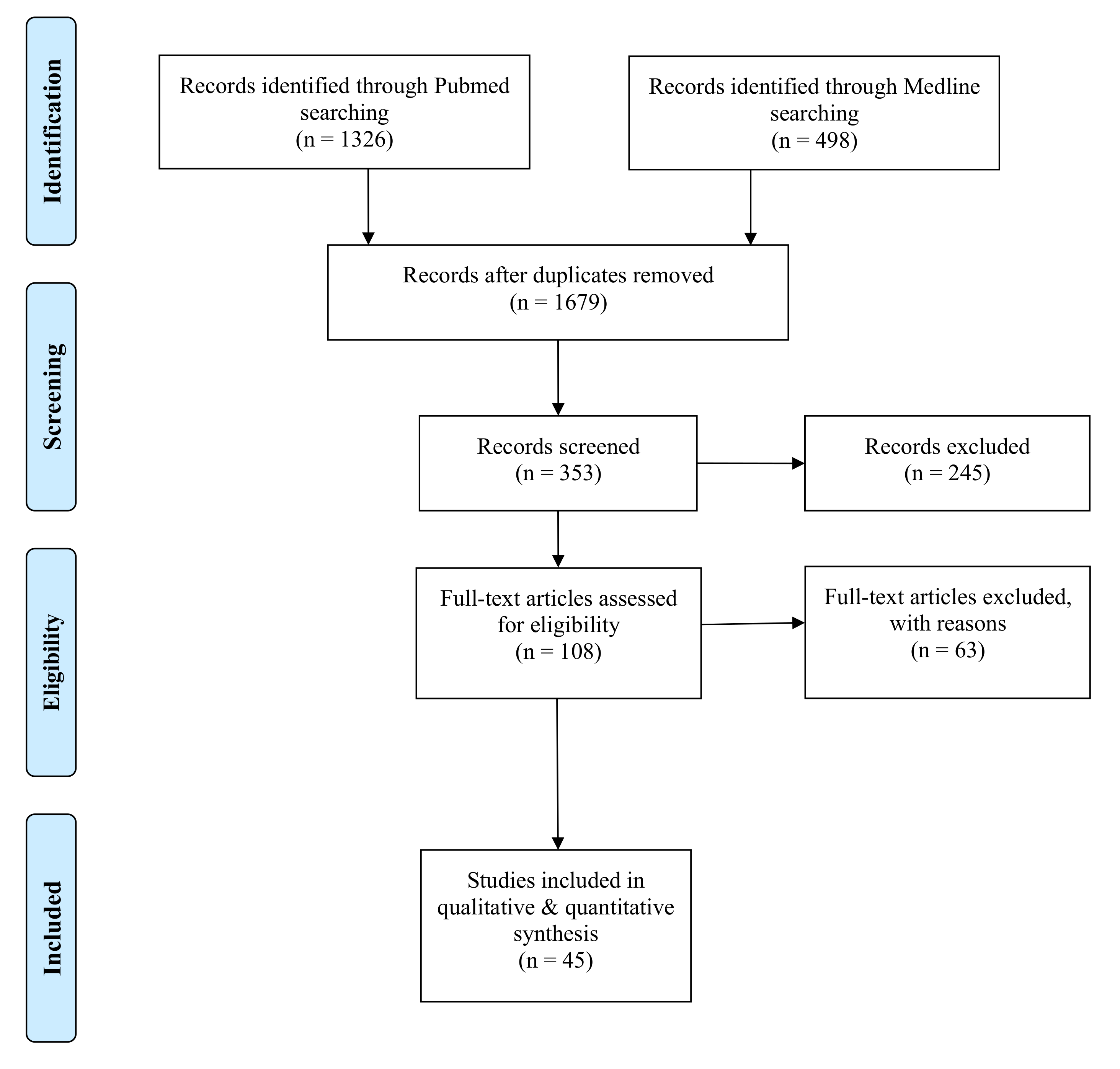
3.1. Selection and Data Collection Process
3.2. Study Selection
3.3. Risk of Bias in Studies
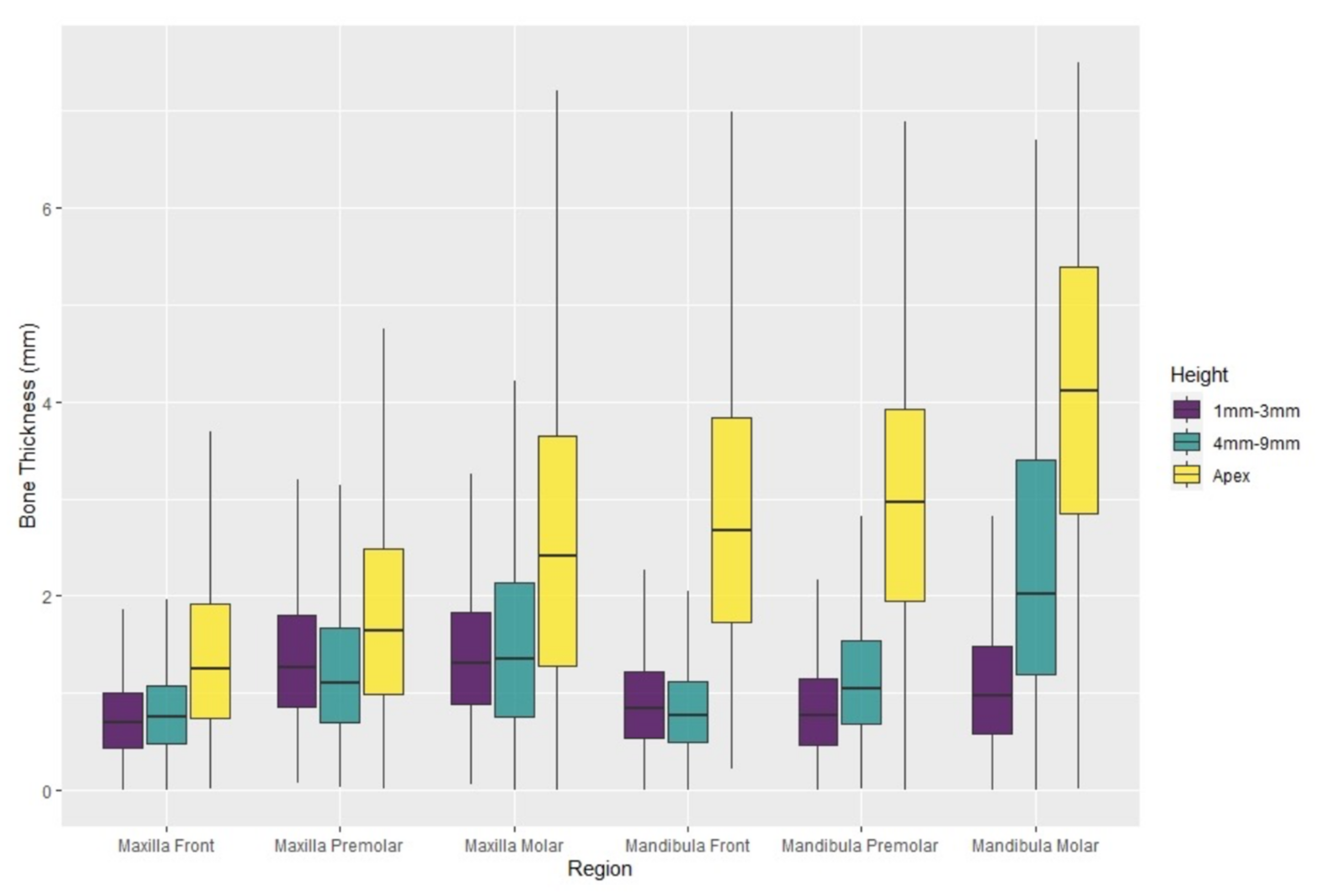
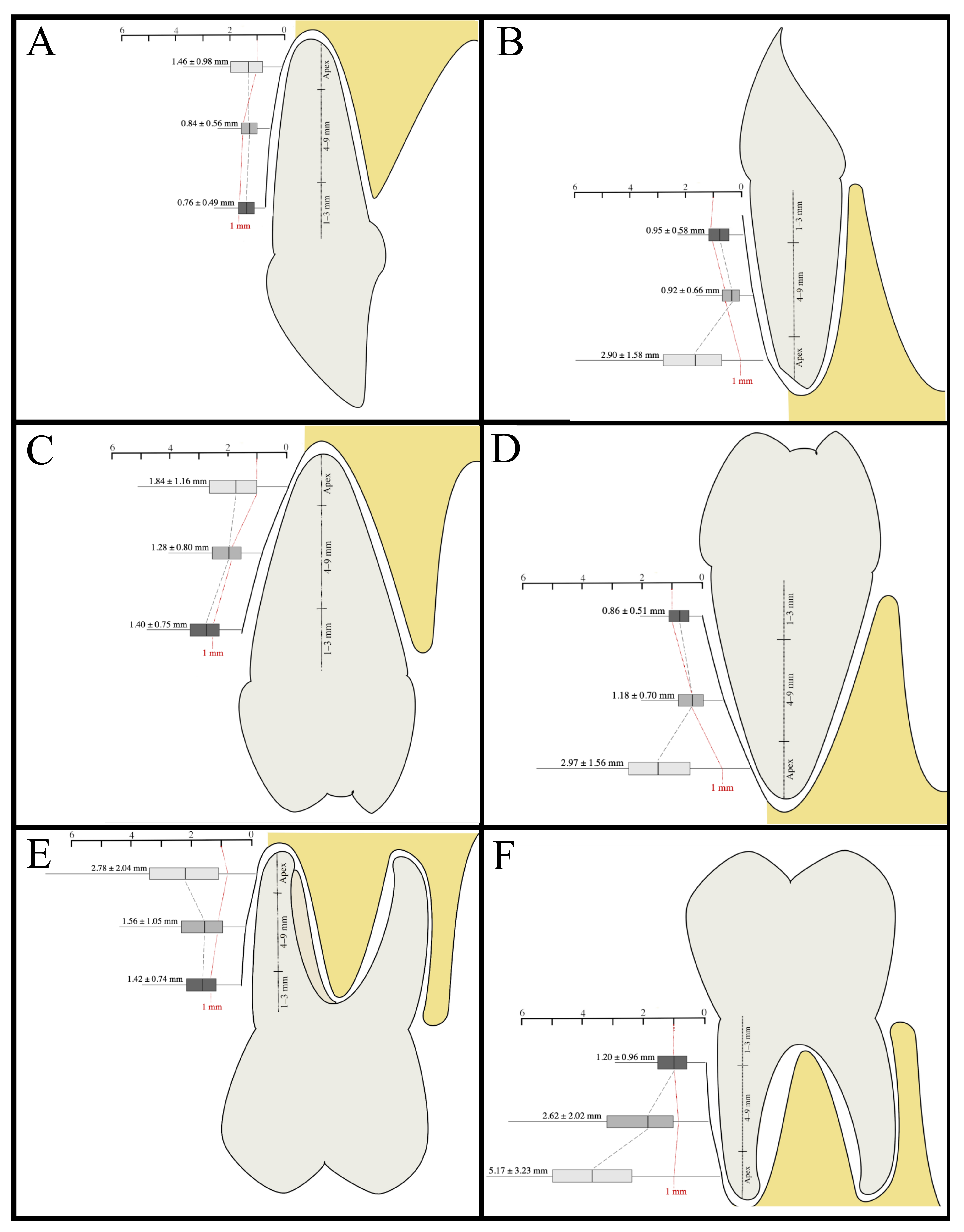
3.4. Buccal Bone Thickness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Simulation Study
References
- Hammerle, C.H.; Chen, S.T.; Wilson, T.G., Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int. J. Oral Maxillofac. Implant. 2004, 19, 26–28. [Google Scholar]
- Chen, S.T.; Buser, D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla—A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 186–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buser, D.; Chappuis, V.; Belser, U.C.; Chen, S. Implant placement post extraction in esthetic single tooth sites: When immediate, when early, when late? Periodontology 2000 2017, 73, 84–102. [Google Scholar] [CrossRef]
- Wismeijer, D.; Chen, S.T. Proceedings of the Sixth ITI Consensus Conference. Clin. Oral Implant. Res. 2018, 29. [Google Scholar] [CrossRef] [PubMed]
- Koh, R.U.; Rudek, I.; Wang, H.L. Immediate implant placement: Positives and negatives. Implant Dent. 2010, 19, 98–108. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Dental implants inserted in fresh extraction sockets versus healed sites: A systematic review and meta-analysis. J. Dent. 2015, 43, 16–41. [Google Scholar] [CrossRef] [PubMed]
- Mello, C.C.; Lemos, C.A.A.; Verri, F.R.; Dos Santos, D.M.; Goiato, M.C.; Pellizzer, E.P. Immediate implant placement into fresh extraction sockets versus delayed implants into healed sockets: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 1162–1177. [Google Scholar] [CrossRef] [Green Version]
- Atieh, M.A.; Duncan, W.J.; Faggion, C.M., Jr. Quality Assessment of Systematic Reviews on Oral Implants Placed Immediately into Fresh Extraction Sockets. Int. J. Oral Maxillofac. Implant. 2016, 31, 338–351. [Google Scholar] [CrossRef]
- Araujo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef]
- Scala, A.; Lang, N.P.; Schweikert, M.T.; de Oliveira, J.A.; Rangel-Garcia, I., Jr.; Botticelli, D. Sequential healing of open extraction sockets. An experimental study in monkeys. Clin. Oral Implant. Res. 2014, 25, 288–295. [Google Scholar] [CrossRef]
- Chappuis, V.; Engel, O.; Reyes, M.; Shahim, K.; Nolte, L.P.; Buser, D. Ridge alterations post-extraction in the esthetic zone: A 3D analysis with CBCT. J. Dent. Res. 2013, 92, 195S–201S. [Google Scholar] [CrossRef] [Green Version]
- Cardaropoli, G.; Araujo, M.; Lindhe, J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. J. Clin. Periodontol. 2003, 30, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.G.; Silva, C.O.; Misawa, M.; Sukekava, F. Alveolar socket healing: What can we learn? Periodontology 2000 2015, 68, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Chappuis, V.; Araujo, M.G.; Buser, D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000 2017, 73, 73–83. [Google Scholar] [CrossRef]
- Vignoletti, F.; Matesanz, P.; Rodrigo, D.; Figuero, E.; Martin, C.; Sanz, M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. Clin. Oral Implant. Res. 2012, 23 (Suppl. 5), 22–38. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, B. Some Useful Moment Results in Sampling Problems. Am. Stat. 2013, 282–296. [Google Scholar] [CrossRef]
- Raber, A.; Kula, K.; Ghoneima, A. Three-dimensional evaluation of labial alveolar bone overlying the maxillary and mandibular incisors in different skeletal classifications of malocclusion. Int. Orthod. 2019, 17, 287–295. [Google Scholar] [CrossRef]
- Yuan, J.; Guo, Q.Q.; Li, Q.; Sui, Y.J.; Jiang, B.Q. Relationships among the periodontal biotype characteristics in the maxillary anterior. Hua Xi Kou Qiang Yi Xue Za Zhi 2020, 38, 398–403. [Google Scholar] [CrossRef]
- Zhang, F.; Lee, S.C.; Lee, J.B.; Lee, K.M. Geometric analysis of alveolar bone around the incisors after anterior retraction following premolar extraction. Angle Orthod. 2020, 90, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Adiguzel, O.; Aktuna Belgin, C.; Falakaloglu, S.; Cangul, S.; Akkus, Z. Maxillary Cortical Bone Thickness in a South-Eastern Anatolian Population: A Cone-Beam Computed Tomography Study. Med. Sci. Monit. 2017, 23, 5812–5817. [Google Scholar] [CrossRef] [Green Version]
- Al-Jandan, B.A.; Al-Sulaiman, A.A.; Marei, H.F.; Syed, F.A.; Almana, M. Thickness of buccal bone in the mandible and its clinical significance in mono-cortical screws placement. A CBCT analysis. Int. J. Oral Maxillofac. Surg. 2013, 42, 77–81. [Google Scholar] [CrossRef]
- Al-Masri, M.M.; Ajaj, M.A.; Hajeer, M.Y.; Al-Eed, M.S. Evaluation of Bone Thickness and Density in the Lower Incisors’ Region in Adults with Different Types of Skeletal Malocclusion using Cone-beam Computed Tomography. J. Contemp. Dent. Pract. 2015, 16, 630–637. [Google Scholar] [CrossRef]
- AlTarawneh, S.; AlHadidi, A.; Hamdan, A.A.; Shaqman, M.; Habib, E. Assessment of Bone Dimensions in the Anterior Maxilla: A Cone Beam Computed Tomography Study. J. Prosthodont. 2018, 27, 321–328. [Google Scholar] [CrossRef]
- Amid, R.; Mirakhori, M.; Safi, Y.; Kadkhodazadeh, M.; Namdari, M. Assessment of gingival biotype and facial hard/soft tissue dimensions in the maxillary anterior teeth region using cone beam computed tomography. Arch. Oral Biol. 2017, 79, 1–6. [Google Scholar] [CrossRef]
- Behnia, H.; Motamedian, S.R.; Kiani, M.T.; Morad, G.; Khojasteh, A. Accuracy and reliability of cone beam computed tomographic measurements of the bone labial and palatal to the maxillary anterior teeth. Int. J. Oral Maxillofac. Implant. 2015, 30, 1249–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botelho, S.V.; Perussolo, J.; Misawa, M.Y.; Zadeh, H.H.; Araujo, M.G. The Basal Bone and Alveolar Process in the Maxillary Anterior Region in Humans: A Cone Beam Computed Tomographic Study. Int. J. Periodontics Restor. Dent. 2020, 40, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Darby, I. The relationship between facial bone wall defects and dimensional alterations of the ridge following flapless tooth extraction in the anterior maxilla. Clin. Oral Implant. Res. 2017, 28, 931–937. [Google Scholar] [CrossRef]
- D’Silva, E.; Fraser, D.; Wang, B.; Barmak, A.B.; Caton, J.; Tsigarida, A. The association between gingival recession and buccal bone at maxillary anterior teeth. J. Periodontol. 2020, 91, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Demircan, S.; Demircan, E. Dental Cone Beam Computed Tomography Analyses of the Anterior Maxillary Bone Thickness for Immediate Implant Placement. Implant Dent. 2015, 24, 664–668. [Google Scholar] [CrossRef]
- El Nahass, H.; N Naiem, S. Analysis of the dimensions of the labial bone wall in the anterior maxilla: A cone-beam computed tomography study. Clin. Oral Implant. Res. 2015, 26, e57–e61. [Google Scholar] [CrossRef]
- Eraydin, F.; Germec-Cakan, D.; Tozlu, M.; Ozdemir, F.I. Three-dimensional evaluation of alveolar bone thickness of mandibular anterior teeth in different dentofacial types. Niger. J. Clin. Pract. 2018, 21, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Farahamnd, A.; Sarlati, F.; Eslami, S.; Ghassemian, M.; Youssefi, N.; Jafarzadeh Esfahani, B. Evaluation of Impacting Factors on Facial Bone Thickness in the Anterior Maxillary Region. J. Craniofac. Surg. 2017, 28, 700–705. [Google Scholar] [CrossRef]
- Foosiri, P.; Mahatumarat, K.; Panmekiate, S. Relationship between mandibular symphysis dimensions and mandibular anterior alveolar bone thickness as assessed with cone-beam computed tomography. Dental Press J. Orthod. 2018, 23, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Gakonyo, J.; Mohamedali, A.J.; Mungure, E.K. Cone Beam Computed Tomography Assessment of the Buccal Bone Thickness in Anterior Maxillary Teeth: Relevance to Immediate Implant Placement. Int. J. Oral Maxillofac. Implant. 2018, 33, 880–887. [Google Scholar] [CrossRef]
- Ganji, K.K.; Alswilem, R.O.; Abouonq, A.O.; Alruwaili, A.A.; Alam, M.K. Noninvasive evaluation of the correlation between thickness of the buccal bone and attached gingiva of maxillary premolars. J. Esthet. Restor. Dent. 2019, 31, 240–245. [Google Scholar] [CrossRef]
- Gluckman, H.; Pontes, C.C.; Du Toit, J. Radial plane tooth position and bone wall dimensions in the anterior maxilla: A CBCT classification for immediate implant placement. J. Prosthet. Dent. 2018, 120, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Januario, A.L.; Duarte, W.R.; Barriviera, M.; Mesti, J.C.; Araujo, M.G.; Lindhe, J. Dimension of the facial bone wall in the anterior maxilla: A cone-beam computed tomography study. Clin. Oral Implant. Res. 2011, 22, 1168–1171. [Google Scholar] [CrossRef]
- Jin, G.C.; Kim, K.D.; Roh, B.D.; Lee, C.Y.; Lee, S.J. Buccal bone plate thickness of the Asian people. J. Endod. 2005, 31, 430–434. [Google Scholar] [CrossRef]
- Kheur, M.G.; Kantharia, N.R.; Kheur, S.M.; Acharya, A.; Le, B.; Sethi, T. Three-Dimensional Evaluation of Alveolar Bone and Soft Tissue Dimensions of Maxillary Central Incisors for Immediate Implant Placement: A Cone-Beam Computed Tomography Assisted Analysis. Implant Dent. 2015, 24, 407–415. [Google Scholar] [CrossRef]
- Khoury, J.; Ghosn, N.; Mokbel, N.; Naaman, N. Buccal Bone Thickness Overlying Maxillary Anterior Teeth: A Clinical and Radiographic Prospective Human Study. Implant Dent. 2016, 25, 525–531. [Google Scholar] [CrossRef]
- Lau, S.L.; Chow, J.; Li, W.; Chow, L.K. Classification of maxillary central incisors-implications for immediate implant in the esthetic zone. J. Oral Maxillofac. Surg. 2011, 69, 142–153. [Google Scholar] [CrossRef]
- Lee, S.; Hwang, S.; Jang, W.; Choi, Y.J.; Chung, C.J.; Kim, K.H. Assessment of lower incisor alveolar bone width using cone-beam computed tomography images in skeletal Class III adults of different vertical patterns. Korean J. Orthod. 2018, 48, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Pan, W.L.; Wang, H.L. Facial Fenestration and Dehiscence Defects Associated With Immediate Implant Placement Without Flap Elevation in Anterior Maxillary Ridge: A Preliminary Cone Beam Computed Tomography Study. Int. J. Oral Maxillofac. Implant. 2018, 33, 1112–1118. [Google Scholar] [CrossRef]
- Lopez-Jarana, P.; Diaz-Castro, C.M.; Falcao, A.; Falcao, C.; Rios-Santos, J.V.; Herrero-Climent, M. Thickness of the buccal bone wall and root angulation in the maxilla and mandible: An approach to cone beam computed tomography. BMC Oral Health 2018, 18, 194. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, H.; Borzabadi-Farahani, A.; Le, B.T. Three-Dimensional Alveolar Bone Anatomy of the Maxillary First Molars: A Cone-Beam Computed Tomography Study With Implications for Immediate Implant Placement. Implant Dent. 2016, 25, 367–372. [Google Scholar] [CrossRef]
- Nahas-Scocate, A.C.; de Siqueira Brandao, A.; Patel, M.P.; Lipiec-Ximenez, M.E.; Chilvarquer, I.; do Valle-Corotti, K.M. Bone tissue amount related to upper incisors inclination. Angle Orthod. 2014, 84, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Nowzari, H.; Molayem, S.; Chiu, C.H.; Rich, S.K. Cone beam computed tomographic measurement of maxillary central incisors to determine prevalence of facial alveolar bone width >/=2 mm. Clin. Implant Dent. Relat. Res. 2012, 14, 595–602. [Google Scholar] [CrossRef]
- Nucera, R.; Lo Giudice, A.; Bellocchio, A.M.; Spinuzza, P.; Caprioglio, A.; Perillo, L.; Matarese, G.; Cordasco, G. Bone and cortical bone thickness of mandibular buccal shelf for mini-screw insertion in adults. Angle Orthod. 2017, 87, 745–751. [Google Scholar] [CrossRef] [Green Version]
- Park, J.B.; Lee, J.E.; Kim, K.; Yoo, J.T.; Kim, Y.; Kook, Y.A.; Ko, Y. The thickness of alveolar bone at the mandibular canine and premolar teeth in normal occlusion. J. Craniofac. Surg. 2014, 25, 1115–1119. [Google Scholar] [CrossRef]
- Pascual, A.; Barallat, L.; Santos, A.; Levi, P., Jr.; Vicario, M.; Nart, J.; Medina, K.; Romanos, G.E. Comparison of Periodontal Biotypes Between Maxillary and Mandibular Anterior Teeth: A Clinical and Radiographic Study. Int. J. Periodontics Restor. Dent. 2017, 37, 533–539. [Google Scholar] [CrossRef]
- Porto, O.C.L.; Silva, B.S.F.; Silva, J.A.; Estrela, C.R.A.; Alencar, A.H.G.; Bueno, M.D.R.; Estrela, C. CBCT assessment of bone thickness in maxillary and mandibular teeth: An anatomic study. J. Appl. Oral Sci. 2020, 28, e20190148. [Google Scholar] [CrossRef] [Green Version]
- Ramanauskaite, A.; Becker, K.; Kassira, H.C.; Becker, J.; Sader, R.; Schwarz, F. The dimensions of the facial alveolar bone at tooth sites with local pathologies: A retrospective cone-beam CT analysis. Clin. Oral Investig. 2020, 24, 1551–1560. [Google Scholar] [CrossRef]
- Rojo-Sanchis, J.; Vina-Almunia, J.; Penarrocha-Oltra, D.; Penarrocha-Diago, M. Facial Alveolar Bone Width at the First and Second Maxillary Premolars in Healthy Patients: A Cone Beam Computed Tomography Study. J. Oral Implantol. 2017, 43, 261–265. [Google Scholar] [CrossRef]
- Sendyk, M.; de Paiva, J.B.; Abrao, J.; Rino Neto, J. Correlation between buccolingual tooth inclination and alveolar bone thickness in subjects with Class III dentofacial deformities. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 66–79. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, R.; Liu, X.; Chen, S.; Li, Z.; Chen, Z.; Pow, E.H.N.; Chen, Z.; Huang, B. Correlation of anterior overbite with root position and buccal bone thickness of maxillary anterior teeth: A CBCT study. Surg. Radiol. Anat. 2019, 41, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Temple, K.E.; Schoolfield, J.; Noujeim, M.E.; Huynh-Ba, G.; Lasho, D.J.; Mealey, B.L. A cone beam computed tomography (CBCT) study of buccal plate thickness of the maxillary and mandibular posterior dentition. Clin. Oral Implant. Res. 2016, 27, 1072–1078. [Google Scholar] [CrossRef] [PubMed]
- Uner, D.D.; Izol, B.S.; Gorus, Z. Correlation between buccal and alveolar bone widths at the central incisors according to cone-beam-computed tomography. Niger. J. Clin. Pract. 2019, 22, 79–84. [Google Scholar] [CrossRef]
- Wang, H.M.; Shen, J.W.; Yu, M.F.; Chen, X.Y.; Jiang, Q.H.; He, F.M. Analysis of facial bone wall dimensions and sagittal root position in the maxillary esthetic zone: A retrospective study using cone beam computed tomography. Int. J. Oral Maxillofac. Implant. 2014, 29, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Yoshimine, S.; Nishihara, K.; Nozoe, E.; Yoshimine, M.; Nakamura, N. Topographic analysis of maxillary premolars and molars and maxillary sinus using cone beam computed tomography. Implant Dent. 2012, 21, 528–535. [Google Scholar] [CrossRef]
- Younes, F.; Eghbali, A.; Raes, M.; De Bruyckere, T.; Cosyn, J.; De Bruyn, H. Relationship between buccal bone and gingival thickness revisited using non-invasive registration methods. Clin. Oral Implant. Res. 2016, 27, 523–528. [Google Scholar] [CrossRef]
- Yuan, J.; Wen, Y.; Huang, H.Y.; Xu, X.; Jiang, B.Q. Relationship among gingival thickness, underlying alveolar bone thickness, and sagittal root position in the maxillary anterior. Hua Xi Kou Qiang Yi Xue Za Zhi 2018, 36, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Zahedi, S.; Mostafavi, M.; Lotfirikan, N. Anatomic Study of Mandibular Posterior Teeth Using Cone-beam Computed Tomography for Endodontic Surgery. J. Endod. 2018, 44, 738–743. [Google Scholar] [CrossRef]
- Zekry, A.; Wang, R.; Chau, A.C.; Lang, N.P. Facial alveolar bone wall width—A cone-beam computed tomography study in Asians. Clin. Oral Implant. Res. 2014, 25, 194–206. [Google Scholar] [CrossRef]
- Zhang, W.; Skrypczak, A.; Weltman, R. Anterior maxilla alveolar ridge dimension and morphology measurement by cone beam computerized tomography (CBCT) for immediate implant treatment planning. BMC Oral Health 2015, 15, 65. [Google Scholar] [CrossRef] [Green Version]
- Frost, N.A.; Mealey, B.L.; Jones, A.A.; Huynh-Ba, G. Periodontal Biotype: Gingival Thickness as It Relates to Probe Visibility and Buccal Plate Thickness. J. Periodontol. 2015, 86, 1141–1149. [Google Scholar] [CrossRef]
- Temple, K.E.; Schoolfield, J.; Noujeim, M.E.; Huynh-Ba, G.; Lasho, D.J.; Mealey, B.L. Thickness of the Buccal Plate in Posterior Teeth: A Prospective Cone Beam Computed Tomography Study. Int. J. Periodontics Restor. Dent. 2017, 37, 801–807. [Google Scholar] [CrossRef] [Green Version]
- Agostinelli, C.; Agostinelli, A.; Berardini, M.; Trisi, P. Radiological Evaluation of the Dimensions of Lower Molar Alveoli. Implant Dent. 2018, 27, 271–275. [Google Scholar] [CrossRef]
- Hu, X.; Huang, X.; Gu, Y. Assessment of buccal and lingual alveolar bone thickness and buccolingual inclination of maxillary posterior teeth in patients with severe skeletal Class III malocclusion with mandibular asymmetry. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 503–515. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, M.; Boscolo, S.M.A.; Haiter-Neto, F.; Santos, E.C.D.; Lambrichts, I.; Pauwels, R.; Jacobs, R. Influence of basis images and skull position on evaluation of cortical bone thickness in cone beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, 707–713. [Google Scholar] [CrossRef]
- Fuhrmann, R.; Wehrbein, H.; Dietrich, P. Dreidimensionale computertomographische Darstellung des bezahnten Alveolarkamms. Ein radiologisch-histologischer Vergleich. Fortschr. Kieferorthop. 1993, 54, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Vergara, J.A.; Caffesse, R.G. Preservation of esthetics with implant dentistry: A clinical report. Clin. Implant Dent. Relat. Res. 2002, 4, 200–211. [Google Scholar] [CrossRef]
- Romero-Delmastro, A.; Kadioglu, O.; Currier, G.F.; Cook, T. Digital tooth-based superimposition method for assessment of alveolar bone levels on cone-beam computed tomography images. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 255–263. [Google Scholar] [CrossRef]
- Chevalier, E.; Philip-Alliez, C.; Le Gall, M. Alveolar bone thickness in A point area : How to avoid periodontal failures in front of upper incisors. L’Orthodontie Française 2016, 87, 39–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.Y.; DeBaz, C.; Bhandal, G.; Alli, F.; Buencamino Francisco, M.C.; Thacker, H.L.; Palomo, J.M.; Palomo, L. Buccal Bone Thickness in the Esthetic Zone of Postmenopausal Women: A CBCT Analysis. Implant Dent. 2016, 25, 478–484. [Google Scholar] [CrossRef]
- Ohiomoba, H.; Sonis, A.; Yansane, A.; Friedland, B. Quantitative evaluation of maxillary alveolar cortical bone thickness and density using computed tomography imaging. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 82–91. [Google Scholar] [CrossRef]
- Tiantian, Y.; Bishuang, P.; Jin, L.; Yulan, X.; Gang, W.; Jing, L. Influence of positional relationship between the long axis of the mandibular anterior teeth and the alveolar bone on the treatment design of dental implants. Hua Xi Kou Qiang Yi Xue Za Zhi 2017, 35, 603–606. [Google Scholar] [CrossRef]
- Morais, J.F.; Melsen, B.; de Freitas, K.M.S.; Castello Branco, N.; Garib, D.G.; Cattaneo, P.M. Evaluation of maxillary buccal alveolar bone before and after orthodontic alignment without extractions: A cone beam computed tomographic study. Angle Orthod. 2018, 88, 748–756. [Google Scholar] [CrossRef] [Green Version]
- Dantas, L.L.; Ferreira, P.P.; Oliveira, L.; Neves, F.S.; Campos, P.; Scarfe, W.C.; Crusoe-Rebello, I. Cone beam computed tomography devices in the evaluation of buccal bone in anterior teeth. Aust. Dent. J. 2019, 64, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Green, P.T.; Mol, A.; Moretti, A.J.; Tyndall, D.A.; Kohltfarber, H.B. Comparing the diagnostic efficacy of intraoral radiography and cone beam computed tomography volume registration in the detection of mandibular alveolar bone defects. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 128, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Kortam, S.; Deguchi, T.; Geuy, P.; Johnston, W.M.; Fields, H.W.; Palomo, J.M.; Kim, D.G. Associations of pretreatment parameters with changes during orthodontic treatment. Orthod. Craniofac. Res. 2019, 22 (Suppl. 1), 120–126. [Google Scholar] [CrossRef] [PubMed]
- Mao, H.; Yang, A.; Pan, Y.; Li, H.; Lei, L. Displacement in root apex and changes in incisor inclination affect alveolar bone remodeling in adult bimaxillary protrusion patients: A retrospective study. Head Face Med. 2020, 16, 29. [Google Scholar] [CrossRef]
- Mao, M.; Xu, L.; Jing, W.; Xu, X.; Hou, J.; Li, X.; Wang, X. Analysis of the position and related factors of the alveolar crest on thelabial side of the anterior teeth in patients with skeletal Class Ⅲmalocclusion. Beijing Da Xue Xue Bao Yi Xue Ban 2020, 18. [Google Scholar] [CrossRef]
- Redua, R.B.; Carvalho, F.A.R.; Artese, F.R.G. Measurement of the bone height of mandibular incisors and canines on computed tomography-Limitations according to bone thickness. Orthod. Craniofac. Res. 2020, 23, 59–65. [Google Scholar] [CrossRef]
- Sheng, Y.; Guo, H.M.; Bai, Y.X.; Li, S. Dehiscence and fenestration in anterior teeth : Comparison before and after orthodontic treatment. J. Orofac. Orthop. 2020, 81, 1–9. [Google Scholar] [CrossRef]
- Arora, H.; Ivanovski, S. Correlation between pre-operative buccal bone thickness and soft tissue changes around immediately placed and restored implants in the maxillary anterior region: A 2-year prospective study. Clin. Oral Implant. Res. 2017, 28, 1188–1194. [Google Scholar] [CrossRef]
- Pramstraller, M.; Farina, R.; Franceschetti, G.; Pramstraller, C.; Trombelli, L. Ridge dimensions of the edentulous posterior maxilla: A retrospective analysis of a cohort of 127 patients using computerized tomography data. Clin. Oral Implant. Res. 2011, 22, 54–61. [Google Scholar] [CrossRef]
- Lim, J.E.; Lim, W.H.; Chun, Y.S. Quantitative evaluation of cortical bone thickness and root proximity at maxillary interradicular sites for orthodontic mini-implant placement. Clin. Anat. 2008, 21, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Ono, A.; Motoyoshi, M.; Shimizu, N. Cortical bone thickness in the buccal posterior region for orthodontic mini-implants. Int. J. Oral Maxillofac. Surg. 2008, 37, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Gracco, A.; Lombardo, L.; Mancuso, G.; Gravina, V.; Siciliani, G. Upper incisor position and bony support in untreated patients as seen on CBCT. Angle Orthod. 2009, 79, 692–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Cho, H.J. Three-dimensional evaluation of interradicular spaces and cortical bone thickness for the placement and initial stability of microimplants in adults. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 314.e1–314.e12, discussion 314–315. [Google Scholar] [CrossRef]
- Cremonini, C.C.; Dumas, M.; Pannuti, C.M.; Neto, J.B.; Cavalcanti, M.G.; Lima, L.A. Assessment of linear measurements of bone for implant sites in the presence of metallic artefacts using cone beam computed tomography and multislice computed tomography. Int. J. Oral Maxillofac. Surg. 2011, 40, 845–850. [Google Scholar] [CrossRef]
- Han, M.; Wang, R.Y.; Liu, H.; Zhu, X.J.; Wei, F.L.; Lv, T.; Wang, N.N.; Hu, L.H.; Li, G.J.; Liu, D.X.; et al. Association between mandibular posterior alveolar morphology and growth pattern in a Chinese population with normal occlusion. J. Zhejiang Univ. Sci. B 2013, 14, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Gu, X.M.; Liu, H.C.; Wang, Z.W.; Xun, C.L. Measurement of cortical bone thickness in adults by cone-beam computerized tomography for orthodontic miniscrews placement. J. Huazhong Univ. Sci. Technol. Med. Sci. 2013, 33, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Holmes, P.B.; Wolf, B.J.; Zhou, J. A CBCT atlas of buccal cortical bone thickness in interradicular spaces. Angle Orthod. 2015, 85, 911–919. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.H.; Kim, B.S.; Kim, Y. Proximity of Posterior Teeth to the Maxillary Sinus and Buccal Bone Thickness: A Biometric Assessment Using Cone-beam Computed Tomography. J. Endod. 2015, 41, 1839–1846. [Google Scholar] [CrossRef]
- Garlock, D.T.; Buschang, P.H.; Araujo, E.A.; Behrents, R.G.; Kim, K.B. Evaluation of marginal alveolar bone in the anterior mandible with pretreatment and posttreatment computed tomography in nonextraction patients. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Sadek, M.M.; Sabet, N.E.; Hassan, I.T. Three-dimensional mapping of cortical bone thickness in subjects with different vertical facial dimensions. Prog. Orthod. 2016, 17, 32. [Google Scholar] [CrossRef] [Green Version]
- Kula, T.J., 3rd; Ghoneima, A.; Eckert, G.; Parks, E.T.; Utreja, A.; Kula, K. Two-dimensional vs. 3-dimensional comparison of alveolar bone over maxillary incisors with A-point as a reference. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 836-847.e2. [Google Scholar] [CrossRef]
- Hwang, S.; Jeong, S.; Choi, Y.J.; Chung, C.J.; Lee, H.S.; Kim, K.H. Three-dimensional evaluation of dentofacial transverse widths of adults with various vertical facial patterns. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 692–700. [Google Scholar] [CrossRef]
- Kim, Y.; Roh, B.D.; Shin, Y.; Kim, B.S.; Choi, Y.L.; Ha, A. Morphological Characteristics and Classification of Mandibular First Molars Having 2 Distal Roots or Canals: 3-Dimensional Biometric Analysis Using Cone-beam Computed Tomography in a Korean Population. J. Endod. 2018, 44, 46–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, A.G.; Wang, M.; Gonzalez, S.; Covell, D.A., Jr.; Katancik, J.; Sehgal, H.S. An In Vivo and Cone Beam Computed Tomography Investigation of the Accuracy in Measuring Alveolar Bone Height and Detecting Dehiscence and Fenestration Defects. Int. J. Oral Maxillofac. Implant. 2018, 33, 1296–1304. [Google Scholar] [CrossRef]
- Srebrzynska-Witek, A.; Koszowski, R.; Rozylo-Kalinowska, I. Relationship between anterior mandibular bone thickness and the angulation of incisors and canines-a CBCT study. Clin. Oral Investig. 2018, 22, 1567–1578. [Google Scholar] [CrossRef]
- Buziashvili, D.; Tower, J.I.; Sangal, N.R.; Shah, A.M.; Paskhover, B. Long-term Patterns of Age-Related Facial Bone Loss in Black Individuals. JAMA Facial Plast. Surg. 2019, 21, 292–297. [Google Scholar] [CrossRef]
- Calvani, L.; Calvani, L.; Hirayama, H.; Pissiotis, A.; Michalakis, K. Association Between Increased Concavity of Maxillary Labial Alveolar Bone and Decreased Labial Cortical Bone Thickness: A Cone Beam Computed Tomography Aided Retrospective Cohort Study. J. Prosthodont. 2019, 28, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S.; Alfarsi, M.A. 3-D mapping of cortical bone thickness in subjects with different face form and arch form: A CBCT analysis. Niger. J. Clin. Pract. 2019, 22, 616–625. [Google Scholar] [CrossRef]
- Coskun, I.; Kaya, B. Relationship between alveolar bone thickness, tooth root morphology, and sagittal skeletal pattern : A cone beam computed tomography study. J. Orofac. Orthop. 2019, 80, 144–158. [Google Scholar] [CrossRef]
- Costa, E.D.; Peyneau, P.D.; Ambrosano, G.M.B.; Oliveira, M.L. Influence of cone beam CT volume orientation on alveolar bone measurements in patients with different facial profiles. Dentomaxillofac. Radiol. 2019, 48, 20180330. [Google Scholar] [CrossRef] [PubMed]
- Do, T.A.; Shen, Y.W.; Fuh, L.J.; Huang, H.L. Clinical assessment of the palatal alveolar bone thickness and its correlation with the buccolingual angulation of maxillary incisors for immediate implant placement. Clin. Implant Dent. Relat. Res. 2019, 21, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Wu, X.; Tan, J.; Li, X. Safe regions of miniscrew implantation for distalization of mandibular dentition with CBCT. Prog. Orthod. 2019, 20, 45. [Google Scholar] [CrossRef]
- Zhou, Y.; Si, M.; Liu, Y.; Wu, M. Likelihood of needing facial bone augmentation in the anterior maxilla of Chinese Asians: A cone beam computed tomography virtual implant study. Clin. Implant Dent. Relat. Res. 2019, 21, 503–509. [Google Scholar] [CrossRef]
- Barbosa, D.A.; Kurita, L.M.; Pimenta, A.V.; Teixeira, R.C.; Silva, P.G.; Ribeiro, T.R.; Melo, D.P.; Costa, F.W. Mandibular incisive canal-related prevalence, morphometric parameters, and implant placement implications: A multicenter study of 847 CBCT scans. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e337–e345. [Google Scholar] [CrossRef]
- Goshtasbi, N.; Hazzard, J.; Mehrkhodavandi, N.; Al-Qawasmi, R. The heritability of alveolar bone thickness in siblings seeking orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 803–808. [Google Scholar] [CrossRef]
- Klinge, A.; Ahmad, M.; Eldh, P.; Ulvan, R.; Andersson, L.; Becktor, J.P. Craniofacial Height in Relation to Cross-Sectional Morphology of the Anterior Maxilla: An Anatomical Consideration in Implant Therapy. Int. J. Oral Maxillofac. Implant. 2020, 35, 386–394. [Google Scholar] [CrossRef]
- Okuzawa-Iwasaki, M.; Ishida, Y.; Ikeda, Y.; Imamura, T.; Oishi, S.; Kita, S.; Matsumura, T.; Sakaguchi-Kuma, T.; Ono, T. Alveolar bone morphology in patients with a unilateral palatally displaced maxillary lateral incisor: A cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 28–34. [Google Scholar] [CrossRef]
- Ghassemian, M.; Nowzari, H.; Lajolo, C.; Verdugo, F.; Pirronti, T.; D’Addona, A. The thickness of facial alveolar bone overlying healthy maxillary anterior teeth. J. Periodontol. 2012, 83, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Bonta, H.; Carranza, N.; Gualtieri, A.F.; Rojas, M.A. Morphological characteristics of the facial bone wall related to the tooth position in the alveolar crest in the maxillary anterior. Acta Odontol. Latinoam. 2017, 30, 49–56. [Google Scholar] [PubMed]
- Hu, X.; Lei, L.; Cui, M.; Huang, Z.; Zhang, X. Anatomical analysis of periapical bone of maxillary posterior teeth: A cone beam computed tomography study. J. Int. Med. Res. 2019, 47, 4701–4710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz-Arad, D.; Chaushu, G. The ways and wherefores of immediate placement of implants into fresh extraction sites: A literature review. J. Periodontol. 1997, 68, 915–923. [Google Scholar] [CrossRef]
- Cooper, L.F.; Raes, F.; Reside, G.J.; Garriga, J.S.; Tarrida, L.G.; Wiltfang, J.; Kern, M.; de Bruyn, H. Comparison of radiographic and clinical outcomes following immediate provisionalization of single-tooth dental implants placed in healed alveolar ridges and extraction sockets. Int. J. Oral Maxillofac. Implant. 2010, 25, 1222–1232. [Google Scholar]
- Aizcorbe-Vicente, J.; Penarrocha-Oltra, D.; Canullo, L.; Soto-Penaloza, D.; Penarrocha-Diago, M. Influence of Facial Bone Thickness After Implant Placement into the Healed Ridges on the Remodeled Facial Bone and Considering Soft Tissue Recession: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2020, 35, 107–119. [Google Scholar] [CrossRef]
- Vera, C.; De Kok, I.J.; Chen, W.; Reside, G.; Tyndall, D.; Cooper, L.F. Evaluation of post-implant buccal bone resorption using cone beam computed tomography: A clinical pilot study. Int. J. Oral Maxillofac. Implant. 2012, 27, 1249–1257. [Google Scholar]
- Kaminaka, A.; Nakano, T.; Ono, S.; Kato, T.; Yatani, H. Cone-Beam Computed Tomography Evaluation of Horizontal and Vertical Dimensional Changes in Buccal Peri-Implant Alveolar Bone and Soft Tissue: A 1-Year Prospective Clinical Study. Clin. Implant Dent. Relat. Res. 2015, 17 (Suppl. 2), e576–e585. [Google Scholar] [CrossRef] [PubMed]
- Farronato, D.; Pasini, P.M.; Orsina, A.A.; Manfredini, M.; Azzi, L.; Farronato, M. Correlation between Buccal Bone Thickness at Implant Placement in Healed Sites and Buccal Soft Tissue Maturation Pattern: A Prospective Three-Year Study. Materials 2020, 13, 511. [Google Scholar] [CrossRef] [Green Version]
- Yan, Q.; Xiao, L.Q.; Su, M.Y.; Mei, Y.; Shi, B. Soft and Hard Tissue Changes Following Immediate Placement or Immediate Restoration of Single-Tooth Implants in the Esthetic Zone: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2016, 31, 1327–1340. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.G.; Sukekava, F.; Wennstrom, J.L.; Lindhe, J. Tissue modeling following implant placement in fresh extraction sockets. Clin. Oral Implant. Res. 2006, 17, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.G.; Wennstrom, J.L.; Lindhe, J. Modeling of the buccal and lingual bone walls of fresh extraction sites following implant installation. Clin. Oral Implant. Res. 2006, 17, 606–614. [Google Scholar] [CrossRef]
- Werbitt, M.J.; Goldberg, P.V. The immediate implant: Bone preservation and bone regeneration. Int. J. Periodontics Restor. Dent. 1992, 12, 206–217. [Google Scholar]
- Novaes, A.B., Jr.; Papalexiou, V.; Luczyszyn, S.M.; Muglia, V.A.; Souza, S.L.; Taba Junior, M. Immediate implant in extraction socket with acellular dermal matrix graft and bioactive glass: A case report. Implant Dent. 2002, 11, 343–348. [Google Scholar] [CrossRef]
- Lindeboom, J.A.; Tjiook, Y.; Kroon, F.H. Immediate placement of implants in periapical infected sites: A prospective randomized study in 50 patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 705–710. [Google Scholar] [CrossRef]
- Naves, M.M.; Horbylon, B.Z.; Gomes, C.F.; Menezes, H.H.; Bataglion, C.; Magalhaes, D. Immediate implants placed into infected sockets: A case report with 3-year follow-up. Braz. Dent. J. 2009, 20, 254–258. [Google Scholar] [CrossRef] [Green Version]
- Agliardi, E.; Panigatti, S.; Clerico, M.; Villa, C.; Malo, P. Immediate rehabilitation of the edentulous jaws with full fixed prostheses supported by four implants: Interim results of a single cohort prospective study. Clin. Oral Implant. Res. 2010, 21, 459–465. [Google Scholar] [CrossRef]
- Atieh, M.A.; Alsabeeha, N.H.; Duncan, W.J.; de Silva, R.K.; Cullinan, M.P.; Schwass, D.; Payne, A.G. Immediate single implant restorations in mandibular molar extraction sockets: A controlled clinical trial. Clin. Oral Implant. Res. 2013, 24, 484–496. [Google Scholar] [CrossRef] [PubMed]
- Grandi, T.; Guazzi, P.; Samarani, R.; Grandi, G. Immediate provisionalisation of single post-extractive implants versus implants placed in healed sites in the anterior maxilla: 1-year results from a multicentre controlled cohort study. Eur. J. Oral Implantol. 2013, 6, 285–295. [Google Scholar]
- Esposito, M.; Grusovin, M.G.; Polyzos, I.P.; Felice, P.; Worthington, H.V. Interventions for replacing missing teeth: Dental implants in fresh extraction sockets (immediate, immediate-delayed and delayed implants). Cochrane Database Syst. Rev. 2010, CD005968. [Google Scholar] [CrossRef]
- Fuentes, R.; Flores, T.; Navarro, P.; Salamanca, C.; Beltran, V.; Borie, E. Assessment of buccal bone thickness of aesthetic maxillary region: A cone-beam computed tomography study. J. Periodontal. Implant Sci. 2015, 45, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Sathapana, S.; Forrest, A.; Monsour, P.; Naser-ud-Din, S. Age-related changes in maxillary and mandibular cortical bone thickness in relation to temporary anchorage device placement. Aust. Dent. J. 2013, 58, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Masumoto, T.; Hayashi, I.; Kawamura, A.; Tanaka, K.; Kasai, K. Relationships among facial type, buccolingual molar inclination, and cortical bone thickness of the mandible. Eur. J. Orthod. 2001, 23, 15–23. [Google Scholar] [CrossRef] [Green Version]
- Ozdemir, F.; Tozlu, M.; Germec-Cakan, D. Cortical bone thickness of the alveolar process measured with cone-beam computed tomography in patients with different facial types. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Hu, Y.; Huang, M.; Chen, J.; Ding, X.; Zheng, L. A three-dimensional analysis of skeletal and dental characteristics in skeletal class III patients with facial asymmetry. J. Xray Sci. Technol. 2018, 26, 449–462. [Google Scholar] [CrossRef]
- Fu, J.H.; Yeh, C.Y.; Chan, H.L.; Tatarakis, N.; Leong, D.J.; Wang, H.L. Tissue biotype and its relation to the underlying bone morphology. J. Periodontol. 2010, 81, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Stappert, D.; Geiman, R.; Zadi, Z.H.; Reynolds, M.A. Gingival clefts revisited: Evaluation of the characteristics that make one more susceptible to gingival clefts. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 677–682. [Google Scholar] [CrossRef]
- Digregorio, M.V.; Fastuca, R.; Zecca, P.A.; Caprioglio, A.; Lagravere, M.O. Buccal bone plate thickness after rapid maxillary expansion in mixed and permanent dentitions. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Vanderstuyft, T.; Tarce, M.; Sanaan, B.; Jacobs, R.; de Faria Vasconcelos, K.; Quirynen, M. Inaccuracy of buccal bone thickness estimation on cone-beam CT due to implant blooming: An ex-vivo study. J. Clin. Periodontol. 2019, 46, 1134–1143. [Google Scholar] [CrossRef] [PubMed]
- Furman, E. On a multivariate gamma distribution. Stat. Probab. Lett. 2008, 78. [Google Scholar] [CrossRef]
- Dvorkin, D. Lcmix-Package: Layered and Chained Mixture Models; R Package Documentation; Anschutz Medical Campus, University of Colorado: Denver, CO, USA, 2019. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Patients | Geographic Location | Men | Women | Teeth | Height | Maxilla (Mean ± SD) | Mandible (Mean ± SD) |
|---|---|---|---|---|---|---|---|---|
| Adiguzel 2017 [20] | 113 | Turkey | 55 | 58 | 451 | Apex | 1st premolar: 2.12 ± 0.78 2nd premolar: 3.16 ± 0.84 1st molar: 2.47 ± 0.92 2nd molar: 3.47 ± 1.06 | |
| Al-Jandan 2013 [21] | 50 | USA (PA) | 22 | 28 | 250 | Apex | Canine: 3.3 ± 0.84 1st premolar: 3.7 ± 0.89 2nd premolar: 3.14 ± 0.81 1st molar: 3.8 ± 0.81 2nd molar: 6.58 ± 1.27 | |
| AlMasri 2015 [22] | 16 | Syria | 5 | 11 | 32 | 1 mm from alveolar crest, Apex | Central incisor: 1 (mm) 0.17 ± 0.29 (Apex) 3.64 ± 1.18 | |
| AlTarawneh 2018 [23] | 120 | Jordan | 39 | 81 | 720 | 3 mm from alveolar crest, Apex | Central incisor 3 (mm) 0.73 ± 0.25 (Apex) 0.59 ± 0.29 Lateral incisor: 3 (mm) 0.69 ± 0.28 (Apex) 0.49 ± 0.29 Canine: 3 (mm) 0.74 ± 0.29 (Apex) 0.39 ± 0.30 | |
| Amid 2017 [24] | 144 | Iran | 60 | 84 | 621 | 2/4/6 mm from CEJ | Central incisor: 2 (mm) 0.35 ± 0.4 4 (mm) 0.77 ± 0.25 6 (mm) 0.75 ± 0.23 Lateral incisor: 2 (mm) 0.29 ± 0.39 4 (mm) 0.78 ± 0.36 6 (mm) 0.75 ± 0.31 Canine: 2 (mm) 0.36 ± 0.44 4 (mm) 0.76 ± 0.36 6 (mm) 0.79 ± 0.33 | |
| Behnia 2015 [25] | 18 | Iran | 11 | 7 | 108 | 1/4/8 mm from alveolar crest | Central incisor: 1 (mm) 0.78 ± 0.23 4 (mm) 0.66 ± 0.2 8 (mm) 0.69 ± 0.43 Lateral incisor: 1 (mm) 0.86 ± 0.39 4 (mm) 0.78 ± 0.54 8 (mm) 0.71 ± 0.59 Canine: 1 (mm) 0.69 ± 0.35 4 (mm) 0.77 ± 0.42 8 (mm) 0.7 ± 0.31 | |
| Botelho 2020 [26] | 87 | Brazil | 24 | 63 | 522 | 3/5/7 mm from CEJ | Central incisor: 3 (mm) 0.6 ± 0.5 5 (mm) 0.8 ± 0.4 7 (mm) 0.7 ± 0.5 Lateral incisor: 3 (mm) 0.6 ± 0.6 5 (mm) 0.9 ± 0.6 7 (mm) 0.7 ± 0.6 Canine: 3 (mm) 0.5 ± 0.5 5 (mm) 0.9 ± 0.5 7 (mm) 0.8 ± 0.6 | |
| Chen 2017 [27] | 16 | Taiwan | 6 | 5 | 96 | Apex | Central incisor: 1.12 ± 0.45 Lateral incisor: 0.85 ± 0.49 Canine: 1.50 ± 1.49 | |
| D’Silva 2020 [28] | 66 | USA (NY) | 37 | 29 | 363 | 4 mm from CEJ | Central incisor: 0.96 ± 0.39 Lateral incisor: 1.1 ± 0.56 Canine: 1.04 ± 0.63 | |
| Demircan 2015 [29] | 60 | Turkey | 30 | 30 | 230 | 1/2/5 mm from alveolar crest | Central incisor: 1 (mm) 0.7 ± 0.17 3 (mm) 0.84 ± 0.179 5 (mm) 0.76 ± 0.21 Lateral incisor: 1 (mm) 0.78 ± 0.22 3 (mm) 0.85 ± 0.26 5 (mm) 0.69 ± 0.2 | |
| El Nahass 2015 [30] | 93 | Egypt | 31 | 62 | 350 | 1/2/4 mm from alveolar crest | Central incisor: 1 (mm) 0.72 ± 0.19 2 (mm) 0.78 ± 0.18 4 (mm) 0.81 ± 0.1 Lateral incisor: 1 (mm) 0.73 ± 0.19 2 (mm) 0.84 ± 0.25 4 (mm) 0.84 ± 0.25 | |
| Eraydin 2018 [31] | 24 | Turkey | 10 | 14 | 48 | 3 mm from CEJ, Apex | Central incisor: 3 (mm) 0.19 ± 0.38 (Apex) 4.21 ± 1.36 Lateral incisor: 3 (mm) 0.39 ± 0.57 (Apex) 4.27 ± 1.64 | |
| Farahamnd 2017 [32] | 132 | Tehran | 65 | 67 | 792 | 2/5/8 mm from alveolar crest | Central incisor: 2 (mm) 0.69 ± 0.63 5 (mm) 0.66 ± 0.62 8 (mm) 0.54 ± 0.61 Lateral incisor: 2 (mm) 0.81 ± 0.64 5 (mm) 0.76 ± 0.66 8 (mm) 0.51 ± 0.53 Canine: 2 (mm) 0.9 ± 0.72 5 (mm) 0.79 ± 0.64 8 (mm) 0.58 ± 0.61 | |
| Foosiri 2018 [33] | 51 | NA | 21 | 30 | 306 | 3/6 mm from CEJ, Apex | Central incisor: 3 (mm) 0.38 ± 0.22 6 (mm) 0.8 ± 0.55 (Apex) 4.44 ± 1.27 Lateral incisor: 3 (mm) 0.49 ± 0.3 6 (mm) 1.28 ± 0.83 (Apex) 4.39 ± 1.18 Canine: 3 (mm) 1.33 ± 0.9 6 (mm) 2.25 ± 1.06 (Apex) 5.53 ± 1.44 | |
| Gakonyo 2018 [34] | 184 | Kenya | 85 | 90 | 1104 | 4 mm from CEJ | Central incisor: 0.58 ± 0.4 Lateral incisor: 0.54 ± 0.42 Canine: 0.52 ± 0.47 | |
| Ganji 2019 [35] | 32 | Saudi Arabia | 9 | 7 | 128 | 3 mm from CEJ | 1st premolar: 1.06 ± 0.47 2nd premolar: 1.37 ± 0.36 | |
| Gluckman 2018 [36] | 150 | South Africa | 67 | 63 | 591 | 1 mm from alveolar crest, Apex | Central incisor: 1 (mm) 0.6 ± 0.3 (Apex) 1.2 ± 0.8 Lateral incisor: 1 (mm) 0.7 ± 0.3 (Apex) 1.5 ± 1.2 Canine: 1 (mm) 0.6 ± 0.3 (Apex) 1.4 ± 1.0 | |
| Januário 2011 [37] | 250 | Brazil | 118 | 132 | 1500 | 1/3/5 mm from CEJ | Central incisor: 1 (mm) 0.6 ± 0.3 3 (mm) 0.6 ± 0.4 5 (mm) 0.5 ± 0.3 Lateral incisor: 1 (mm) 0.7 ± 0.3 3 (mm) 0.7 ± 0.4 5 (mm) 0.5 ± 0.4 Canine: 1 (mm) 0.6 ± 0.3 3 (mm) 0.6 ± 0.4 5 (mm) 0.6 ± 0.4 | |
| Jin 2005 [38] | 66 | Korea | 33 | 33 | 1806 | Apex | Central incisor: 2.05 ± 0.49 Lateral incisor: 1.84 ± 0.47 Canine: 1.64 ± 0.45 1st premolar: 1.68 ± 0.5 2nd premolar: 1.99 ± 0.69 1st molar: 2.73 ± 1.74 2nd molar: 3.61 ± 1.11 | Central incisor: 2.07 ± 0.52 Lateral incisor: 2.31 ± 0.55 Canine: 2.48 ± 0.72 1st premolar: 3.02 ± 0.91 2nd premolar: 3.68 ± 1.22 1st molar: 4.09 ± 1.25 2nd molar: 7.34 ± 1.65 |
| Kheur 2016 [39] | 150 | India | NA | NA | 150 | 3 mm from CEJ, Apex | Central incisor 3 (mm) 0.93 ± 0.39 (Apex) 1.57 ± 0.89 | |
| Khoury 2016 [40] | 47 | Lebanon | 16 | 31 | 282 | 4/6/8/10 mm from CEJ | Central incisor: 4 (mm) 1.05 ± 0.37 6 (mm) 0.97 ± 0.34 8 (mm) 0.91 ± 0.28 10 (mm) 0.91 ± 0.38 Lateral incisor: 4 (mm) 1.07 ± 0.54 6 (mm) 0.9 ± 0.63 8 (mm) 0.63 ± 0.61 10 (mm) 0.59 ± 0.7 Canine: 4 (mm) 0.95 ± 0.51 6 (mm) 0.81 ± 0.6 8 (mm) 0.66 ± 0.58 10 (mm) 0.51 ± 0.46 | |
| Lau 2011 [41] | 170 | China | 76 | 94 | 340 | Apex | Central incisor: 2.04 ± 1.0.1 | |
| Lee 2019 [42] | 20 | Korea | 9 | 11 | 80 | 3/5 mm from CEJ, Apex | Central incisor: 3 (mm) 1.1 ± 0.3 5 (mm) 1.0 ± 0.4 (Apex) 2.3 ± 0.8 Lateral incisor: 3 (mm) 1.2 ± 0.4 5 (mm) 1.0 ± 0.4 (Apex) 2.2 ± 0.8 | |
| Lin 2018 [43] | 21 | Taiwan | 9 | 12 | 126 | 3/5 mm from CEJ | Central incisor: 3 (mm) 0.98 ± 0.48 5 (mm) 0.72 ± 0.63 Lateral incisor: 3 (mm) 0.97 ± 0.66 5 (mm) 0.42 ± 0.53 Canine: 3 (mm) 1.14 ± 0.76 5 (mm) 0.61 ± 0.71 | |
| López-Jarana 2018 [44] | 49 | Spain | 19 | 30 | 403 | 4 mm from alveolar crest, Apex | Central incisor: 4 (mm) 1.02 ± 0.49 (Apex) 1.61 ± 0.95 Canine: 4 (mm) 1.27 ± 1.95 (Apex) 1.26 ± 0.68 1st premolar: 4 (mm) 1.43 ± 0.95 (Apex) 2.19 ± 1.68 1st molar: 4 (mm) 1.55 ± 1.41 (Apex) 2.15 ± 1.68 | Central incisor: 4 (mm) 0.94 ± 0.77 (Apex) 3.19 ± 1.91 Canine: 4 (mm) 1.08 ± 0.86 (Apex) 3.54 ± 1.87 1st premolar: 4 (mm) 1.49 ± 0.97 (Apex) 3.81 ± 1.83 1st molar: 4 (mm) 3.12 ± 2.03 (Apex) 6.78 ± 2.93 |
| Matsuda 2016 [45] | 95 | USA (CA) | 32 | 63 | 150 | 3 mm from alveolar crest | 1st molar: 1.58 ± 0.6 | |
| Nahás-Scocate 2014 [46] | 30 | Brazil | 12 | 18 | 60 | Apex | Central incisor: 0.99 ± 0.59 | |
| Nowzari 2012 [47] | 101 | USA (LA) | 53 | 48 | 202 | 1/2/3/4/5/6/7/8/9/10 mm from alveolar crest | Centra incisor: 1 (mm) 1.0 ± 0.3 2 (mm) 1.2 ± 0.4 3 (mm) 1.2 ± 0.4 4 (mm) 1.1 ± 0.4 5 (mm) 1.1 ± 0.4 6 (mm) 1.0 ± 0.4 7 (mm) 1.0 ± 0.5 8 (mm) 1.0 ± 0.7 9 (mm) 1.0 ± 0.7 10 (mm) 1.2 ± 1.0 | |
| Nucera 2017 [48] | 30 | Italy | 15 | 15 | 120 | 6/11 mm from CEJ | 1st molar: 6 (mm) 0.25 ± 0.44 11 (mm) 2.18 ± 1.46 2nd molar: 6 (mm) 3.76 ± 2.53 11 (mm) 5.57 ± 2.42 | |
| Park 2014 [49] | 20 | Korea | 9 | 11 | 120 | 3/5 mm from alevolar crest, Apex | Canine: 3 (mm) 0.7 ± 0.44 5 (mm) 0.6 ± 0.54 (Apex) 4.11 ± 1.55 1st premolar: 3 (mm) 0.73 ± 0.42 5 (mm) 0.79 ± 0.44 (Apex) 4.05 ± 1.24 2nd premolar: 3 (mm) 1.48 ± 0.72 5 (mm) 1.76 ± 0.74 (Apex) 5.15 ± 1.18 | |
| Pascual 2017 [50] | 15 | Spain | 8 | 7 | 180 | 4 mm from CEJ, Apex | Central incisor: 4 (mm) 1.07 ± 0.96 (Apex) 1.69 ± 0.65 Lateral incisor: 4 (mm) 1.31 ± 0.44 Apex) 1.98 ± 0.79 Canine: 4 (mm) 1.19 ± 0.44 (Apex) 1.71 ± 0.81 | Central incisor: 4 (mm) 1.21 ± 1.05 (Apex) 3.94 ± 1.79 Lateral incisor: 4 (mm) 1.23 ± 1.09 (Apex) 3.69 ± 1.58 Canine: 4 (mm) 1.47 ± 1.42 (Apex) 3.7 ± 1.64 |
| Porto 2020 [51] | 422 | Brazil | 28 | 394 | 1400 | Apex | Central incisor: 1.59 ± 0.67 Lateral incisor: 2.3 ± 1.2 Canine: 1.49 ± 0.86 1st premolar: 1.13 ± 0.68 2nd premolar: 2.20 ± 1.21 1st molar: 1.98 ± 3.3 2nd molar: 3.51 ± 2.15 | Central incisor: 2.72 ± 1.3 Lateral incisor: 3.06 ± 1.29 Canine: 3.43 ± 1.31 1st premolar: 3.27 ± 1.04 2nd premolar: 3.65 ± 1.35 1st molar: 4.45 ± 1.46 2nd molar: 6.65 ± 4.47 |
| Ramanauskaite 2020 [52] | 60 | Germany | 29 | 31 | 707 | Alveolar crest, Apex | Incisor: (AC) 0.56 ± 0.21 (Apex) 1.4 ± 0.93 Premolar: (AC) 0.84 ± 0.42 (Apex) 1.45 ± 1.35 Molar: (AC) 0.97 ± 0.6 (Apex) 1.64 ± 1.40 | Incisor: (AC) 0.55 ± 0.27 (Apex) 3.64 ± 1.63 Premolar: (AC) 0.51 ± 0.29 (Apex) 3.48 ± 1.45 Molar: (AC) 0.97 ± 1.1 (Apex) 6.7 ± 2.31 |
| Rojo-Sanchis 2017 [53] | 44 | Spain | 25 | 19 | 144 | 3/5 mm from CEJ | 1st premolar: 3 (mm) 1.71 ± 0.89 5 (mm) 1.44 ± 1.00 2nd premolar: 3 (mm) 2.43 ± 0.82 5 (mm) 2.31 ± 1.06 | |
| Sendyk 2017 [54] | 35 | Brazil | 16 | 19 | 980 | 3/8 mm from CEJ | Central incisor: 3 (mm) 0.9 ± 0.2 8 (mm) 1.1 ± 0.4 Lateral incisor: 3 (mm) 0.8 ± 0.3 8 (mm) 1.0 ± 0.4 Canine: 3 (mm) 0.6 ± 0.2 8 (mm) 0.9 ± 0.3 1st premolar: 3 (mm) 0.7 ± 0.3 8 (mm) 1.0 ± 0.4 2nd premolar: 3 (mm) 1.3 ± 0.5 8 (mm) 1.5 ± 0.6 1st molar: 3 (mm) 1.0 ± 0.4 8 (mm) 1.2 ± 0.6 2nd molar: 3 (mm) 1.3 ± 0.6 8 (mm) 2.1 ± 1.0 | Central incisor: 3 (mm) 0.5 ± 0.1 8 (mm) 1.5 ± 0.7 Lateral incisor: 3 (mm) 0.5 ± 0.1 8 (mm) 1.0 ± 0.5 Canine: 3 (mm) 0.5 ± 0.1 8 (mm) 0.9 ± 0.4 1st premolar: 3 (mm) 0.5 ± 0.1 8 (mm)1.2 ± 0.7 2nd premolar: 3 (mm) 0.8 ± 0.3 8 (mm) 1.8 ± 0.8 1st molar: 3 (mm) 1.0 ± 0.4 8 (mm) 2.3 ± 1.0 2nd molar: 3 (mm) 2.8 ± 1.5 8 (mm) 5.6 ± 1.6 |
| Shrestha 2019 [55] | 146 | China | 65 | 81 | 876 | 4 mm from CEJ | Central incisor: 0.89 ± 0.51 Lateral incisor: 0.85 ± 1.12 Canine: 0.84 ± 0.68 | |
| Temple 2016 [56] | 265 | USA | 119 | 146 | 934 | 1/3/5 mm apical to alveolar crest | 1st premolar: 1 (mm) 0.95 ± 0.38 3 (mm) 0.81 ± 0.43 5 (mm) 0.66 ± 0.38 2nd premolar: 1 (mm) 1.46 ± 0.66 3 (mm) 1.44 ± 0.79 5 (mm) 1.18 ± 0.67 1st molar: 1 (mm) 0.98 ± 0.40 3 (mm) 0.86 ± 0.48 5 (mm) 0.76 ± 0.54 2nd molar: 1 (mm) 1.58 ± 0.67 3 (mm) 1.92 ± 0.86 5 (mm) 2.13 ± 1.08 | 1st premolar: 1 (mm) 0.54 ± 0.37 3 (mm) 0.61 ± 0.55 5 (mm) 0.90 ± 0.69 2nd premolar: 1 (mm) 0.66 ± 0.45 3 (mm) 0.71 ± 0.53 5 (mm) 1.08 ± 0.68 1st molar: 1 (mm) 0.61 ± 0.29 3 (mm) 1.07 ± 0.85 5 (mm) 1.65 ± 1.29 2nd molar: 1 (mm) 0.88 ± 0.68 3 (mm) 2.03 ± 1.46 5 (mm) 3.65 ± 1.67 |
| Üner 2019 [57] | 160 | Turkey | 80 | 80 | 320 | 3/6/9 mm from CEJ | Central incisor: 3 (mm) 1.19 ± 0.4 6 (mm) 1.15 ± 0.44 9 (mm) 1.06 ± 0.5 | |
| Wang 2014 [58] | 300 | China | 133 | 167 | 2400 | 4 mm from CEJ | Central incisor: 0.8 ± 0.4 Lateral incisor: 0.7 ± 0.4 Canine: 0.7 ± 0.5 1st premolar: 1.2 ± 0.6 2nd premolar: 1.7 ± 0.8 | |
| Yoshimine 2012 [59] | 30 | Japan | 8 | 22 | 240 | Apex | 1st premolar: 0.76 ± 0.57 2nd premolar: 2.13 ± 1.26 1st molar: 2.39 ± 1.47 2nd molar: 4.3 ± 2.1 | |
| Younes 2016 [60] | 21 | Belgium | 7 | 14 | 126 | 1/2/3/4/5 from alveolar crest | Central incisor: 1 (mm) 0.97 ± 0.28 2 (mm) 1.1 ± 0.38 3 (mm) 1.1 ± 0.43 4 (mm) 1.1 ± 0.41 5 (mm) 1.08 ± 0.43 Lateral incisor: 1 (mm) 0.95 ± 0.34 2 (mm) 1.21 ± 0.43 3 (mm) 1.27 ± 0.63 4 (mm) 1.22 ± 0.6 5 (mm) 1.15 ± 0.76 Canine: 1 (mm) 0.89 ± 0.24 2 (mm) 0.99 ± 0.3 3 (mm) 1.04 ± 0.4 4 (mm) 1.00 ± 0.53 5 (mm) 0.96 ± 0.57 | |
| Yuan 2018 [61] | 40 | China | 16 | 24 | 80 | 1/3/5 mm from alveolar crest | Central incisor: 1 (mm) 0.89 ± 0.30 3 (mm) 0.81 ± 0.30 5 (mm) 0.67 ± 0.28 Lateral incisor: 1(mm) 0.8 ± 0.33 3 (mm) 0.85 ± 0.46 5 (mm) 0.43 ± 0.34 | |
| Zahedi 2018 [62] | 170 | Iran | 69 | 101 | 1354 | Apex | 1st premolar: 0.85 ± 0.88 2nd premolar: 1.3 ± 1.05 1st molar: 1.43 ± 1.28 2nd molar: 5.54 ± 2.12 | |
| Zekry 2012 [63] | 200 | China | 74 | 126 | 2400 | 1/3/5 mm from alveolar crest | Central incisor: 1 (mm) 0.9 ± 0.28 3 (mm) 0.89 ± 0.3 5 (mm) 0.81 ± 0.3 Lateral incisor: 1 (mm) 0.94 ± 0.34 3 (mm) 0.88 ± 0.36 5 (mm) 0.68 ± 0.29 Canine: 1 (mm) 1.09 ± 0.34 3 (mm) 1.08 ± 0.47 5 (mm) 0.84 ± 0.39 1st premolar: 1 (mm) 1.23 ± 0.40 3 (mm) 1.26 ± 0.51 5 (mm) 1.16 ± 0.49 2nd premolar: 1 (mm) 1.63 ± 0.62 3 (mm) 2.01 ± 0.83 5 (mm) 1.99 ± 0.92 1st molar: 1 (mm) 1.49 ± 0.57 3 (mm) 1.79 ± 0.78 5 (mm) 1.73 ± 0.88 | Central incisor: 1 (mm) 0.96 ± 0.36 3 (mm) 0.83 ± 0.43 5 (mm) 0.8 ± 0.37 Lateral incisor: 1 (mm) 0.98 ± 0.35 3 (mm) 0.83 ± 0.4 5 (mm) 0.75 ± 0.32 Canine: 1 (mm) 0.99 ± 0.35 3 (mm) 0.77 ± 0.35 5 (mm) 0.68 ± 0.38 1st premolar: 1 (mm) 0.91 ± 0.33 3 (mm) 0.9 ± 0.34 5 (mm) 1.0 ± 0.38 2nd premolar: 1 (mm) 1.21 ± 0.41 3 (mm) 1.30 ± 0.48 5 (mm) 1.49 ± 0.65 1st molar: 1 (mm) 1.08 ± 0.41 3 (mm) 1.31 ± 0.52 5 (mm) 1.62 ± 0.66 |
| Zhang 2015 [64] | 105 | China | 69 | 46 | 1260 | 1 mm from alveolar crest, Apex | Central incisor: 1 (mm) 0.95 ± 0.39 (Apex) 0.86 ± 0.23 Lateral incisor: 1 (mm) 0.76 ± 0.38 (Apex) 0.9 ± 0.29 Canine: 1 (mm) 0.67 ± 0.42 (Apex) 0.98 ± 0.31 | Central incisor: 1 (mm) 1.55 ± 0.52 (Apex) 0.87 ± 0.25 Lateral incisor: 1 (mm) 1.53 ± 0.55 (Apex) 0.91 ± 0.29 Canine: 1 (mm) 1.77 ± 0.6 (Apex) 0.81 ± 0.27 |
| Jaw | Teeth | Height [mm] | Proportion < 1 mm | Standard Deviation | Mean Thickness [mm] | Standard Deviation [mm] |
|---|---|---|---|---|---|---|
| Maxilla | Central incisor–canine | 1–3 | 74.4% | 0.8% | 0.76 | 0.49 |
| 4–9 | 70.1% | 1.2% | 0.84 | 0.56 | ||
| Apex | 38.5% | 1.2% | 1.46 | 0.98 | ||
| 1st premolar–2nd premolar | 1–3 | 33.1% | 1.5% | 1.40 | 0.75 | |
| 4–9 | 438% | 2.4% | 1.28 | 0.80 | ||
| Apex | 25,5% | 1.8% | 1.84 | 1.16 | ||
| 1st molar–2nd molar | 1–3 | 31,6% | 2.0% | 1.42 | 0.74 | |
| 4–9 | 35.3% | 2.4% | 1.56 | 1.05 | ||
| Apex | 19.1% | 1.5% | 2.78 | 2.04 | ||
| Mandible | Central incisor–canine | 1–3 | 61.2% | 1.9% | 0.95 | 0.58 |
| 4–9 | 68.3% | 2.2% | 0.92 | 0.66 | ||
| Apex | 12.3% | 0.8% | 2.90 | 1.58 | ||
| 1st premolar–2nd premolar | 1–3 | 66.3% | 1.9% | 0.86 | 0.51 | |
| 4–9 | 46.7% | 2.4% | 1.18 | 0.70 | ||
| Apex | 13.1% | 0.9% | 2.97 | 1.56 | ||
| 1st molar–2nd molar | 1–3 | 51.9% | 2.3% | 1.20 | 0.96 | |
| 4–9 | 18.2% | 2.0% | 2.62 | 2.02 | ||
| Apex | 6.4% | 0.7% | 5.17 | 3.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heimes, D.; Schiegnitz, E.; Kuchen, R.; Kämmerer, P.W.; Al-Nawas, B. Buccal Bone Thickness in Anterior and Posterior Teeth—A Systematic Review. Healthcare 2021, 9, 1663. https://doi.org/10.3390/healthcare9121663
Heimes D, Schiegnitz E, Kuchen R, Kämmerer PW, Al-Nawas B. Buccal Bone Thickness in Anterior and Posterior Teeth—A Systematic Review. Healthcare. 2021; 9(12):1663. https://doi.org/10.3390/healthcare9121663
Chicago/Turabian StyleHeimes, Diana, Eik Schiegnitz, Robert Kuchen, Peer W. Kämmerer, and Bilal Al-Nawas. 2021. "Buccal Bone Thickness in Anterior and Posterior Teeth—A Systematic Review" Healthcare 9, no. 12: 1663. https://doi.org/10.3390/healthcare9121663
APA StyleHeimes, D., Schiegnitz, E., Kuchen, R., Kämmerer, P. W., & Al-Nawas, B. (2021). Buccal Bone Thickness in Anterior and Posterior Teeth—A Systematic Review. Healthcare, 9(12), 1663. https://doi.org/10.3390/healthcare9121663