
Clinico-Epidemiological Profile and Outcome of Children with IgA Vasculitis in Aseer Region, Southwestern Saudi Arabia

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design and Patient Selection
2.2. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lardhi, A.A. Henoch-Schonlein purpura in children from the eastern province of Saudi Arabia. Saudi Med. J. 2012, 33, 973–978. [Google Scholar]
- Abushhaiwia, A.M.; Rhuma, N.R.; Zletni, M.A.; Ebtisam, S. SM Gr up Clinico-Epidemological Profile of Research Children with Henoch-Schonlein Purpura at Tripoli Children’s Hospital. SM J. Arthritis 2018, 2, 1006. [Google Scholar]
- Chen, J.-Y.; Mao, J.-H. Henoch-Schönlein purpura nephritis in children: Incidence, pathogenesis and management. World J. Pediatrics 2014, 11, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Trapani, S.; Micheli, A.; Grisolia, F.; Resti, M.; Chiappini, E.; Falcini, F.; De Martino, M. Henoch Schonlein Purpura in Childhood: Epidemiological and Clinical Analysis of 150 Cases Over a 5-year Period and Review of Literature. Semin. Arthritis Rheum. 2005, 35, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Ozen, S.; Pistorio, A.; Iusan, S.M.; Bakkaloglu, A.; Herlin, T.; Buoncompagni, A.; Brik, R.; Paediatric Rheumatology International Trials Organisation. EULAR/PRINTO/PRES criteria for Henoch Schönlein purpura, childhood polyarteritis nodosa, childhood Wegener granulomatosis and childhood Takayasu arteritis: Ankara 2008. Part II Final Classif. Cation Criteria 2010, 1, 798–806. [Google Scholar]
- Yang, Y.-H.; Yu, H.-H.; Chiang, B.-L. The diagnosis and classification of Henoch–Schönlein purpura: An updated review. Autoimmun. Rev. 2014, 13, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Kiliç, B.D.; Demir, B.K. Determination of Risk Factors in Children Diagnosed With Henoch-Schönlein Purpura. Arch. Rheumatol. 2018, 33, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Jennette, J.C. Overview of the 2012 revised International Chapel Hill Consensus Conference nomenclature of vasculitides. Clin. Exp. Nephrol. 2013, 17, 603–606. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, T. New algorithm (KAWAKAMI algorithm) to diagnose primary cutaneous vasculitis. J. Dermatol. 2010, 37, 113–124. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, H.J.; Tizard, E.J. Clinical practice. Eur. J. Nucl. Med. Mol. Imaging 2009, 169, 643–650. [Google Scholar] [CrossRef]
- Saulsbury, F.T. Henoch-Schönlein Purpura in Children: Report of 100 Patients and Review of the Literature. Medicine 1999, 78, 395–409. [Google Scholar] [CrossRef]
- Chan, H.; Tang, Y.-L.; Lv, X.-H.; Zhang, G.-F.; Wang, M.; Yang, H.-P.; Li, Q. Risk Factors Associated with Renal Involvement in Childhood Henoch-Schönlein Purpura: A Meta-Analysis. PLoS ONE 2016, 11, e0167346. [Google Scholar] [CrossRef]
- Zoorob, R.; Sidani, M.A.; Fremont, R.D.; Kihlberg, C. Antibiotic use in acute upper respiratory tract infections. Am. Fam. Physician 2012, 86, 817–822. [Google Scholar] [PubMed]
- Alharthi, A.A. Henoch-Schonlein purpura in Saudi Arabia: A retrospective study of 27 children in Taif region. Curr. Pediatric Res. 2016, 20, 126–131. [Google Scholar]
- Bukhari, E.M.; Al-Sofyani, K.A.; Muzaffer, M.A. Spectrum of Henoch-Schonlein Purpura in Children: A Single-Center Experience from Western Provence of Saudi Arabia. Open J. Rheumatol. Autoimmune Dis. 2015, 5, 17–22. [Google Scholar] [CrossRef]
- Akl, K. Childhood Henoch Schonlein purpura in Middle East countries. Saudi J. Kidney Dis. Transplant. 2007, 18, 151–158. [Google Scholar]
- Haghighat, M.; Hashemi, G. Henoch-Schonlein Purpura In Children: Our Experience With 165 Cases From Southern Iran. Med. J. Islamic Repub. Iran 2002, 16, 5–8. [Google Scholar]
- Al Harbi, N.N. Henoch-Schoenlein syndrome in children: Experience from southern part of Saudi Arabia. East Afr. Med. J. 1996, 73, 191. [Google Scholar] [PubMed]
- Gardner-Medwin, J.M.; Doležalová, P.; Cummins, C.; Southwood, T.R. Incidence of Henoch-Schonlein purpura, Kawasaki disease, and rare vasculitides in children of different ethnic origins. Lancet 2002, 360, 1197–1202. [Google Scholar] [CrossRef]
- Narchi, H. Risk of long term renal impairment and duration of follow up recommended for Henoch-Schonlein purpura with normal or minimal urinary findings: A systematic review. Arch. Dis. Child. 2005, 90, 916–920. [Google Scholar] [CrossRef]
- Huang, X.; Wu, X.; Le, W.-B.; Hao, Y.; Wu, J.; Zeng, C.; Liu, Z.; Tang, Z. Renal Prognosis and Related Risk Factors for Henoch-Schönlein Purpura Nephritis: A Chinese Adult Patient Cohort. Sci. Rep. 2018, 8, 5585. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Sun, X.; Cao, Y.; Dai, L.; Sun, F.; Yu, P.; Dong, L. Risk factors for renal involvement and severe kidney disease in 2731 Chinese children with Henoch–Schönlein purpura. Medicine 2018, 97, e12520. [Google Scholar] [CrossRef]
- Jauhola, O.; Ronkainen, J.; Koskimies, O.; Ala-Houhala, M.; Arikoski, P.; Hölttä, T.; Jahnukainen, T.; Rajantie, J.; Örmälä, T.; Turtinen, J.; et al. Renal manifestations of Henoch-Schonlein purpura in a 6-month prospective study of 223 children. Arch. Dis. Child. 2010, 95, 877–882. [Google Scholar] [CrossRef]
- Gül, Ş.; Sönmez, H.E.; Çakmak, F.; Aysel, K.; Yavuz, S. The clinical spectrum of Henoch Schönlein purpura in children: A single-center study. Clin. Rheumatol. 2019, 1707–1714. [Google Scholar]
- Peru, H.; Söylemezoglu, O.; Bakkaloğlu, S.A.; Elmas, S.; Bozkaya, D.; Elmaci, A.M.; Kara, F.; Buyan, N.; Hasanoğlu, E. Henoch Schonlein purpura in childhood: Clinical analysis of 254 cases over a 3-year period. Clin. Rheumatol. 2008, 27, 1087–1092. [Google Scholar] [CrossRef]
- Chen, S.-Y.; Kong, M.-S. Gastrointestinal manifestations and complications of Henoch-Schönlein purpura. Chang. Gung Med. J. 2004, 27, 175–181. [Google Scholar] [PubMed]
- Gupta, V.; Aggarwal, A.; Gupta, R.; Chowdhury, A.C.; Agarwal, V.; Lawrence, A.; Misra, R. Differences between adult and pediatric onset Henoch-Schonlein purpura from North India. Int. J. Rheum. Dis. 2018, 21, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, R.M.K.; Balcı, S.; Mart, O.O.; Tumgor, G.; Yavuz, S.; Celik, H.; Dogruel, D.; Altintas, D.U.; Yilmaz, M. Is Henoch–Schönlein purpura a susceptibility factor for functional gastrointestinal disorders in children? Rheumatol. Int. 2018, 39, 317–322. [Google Scholar] [CrossRef]
- Mao, Y.; Yin, L.; Huang, H.; Zhou, Z.; Chen, T.; Zhou, W. Henoch–Schönlein purpura in 535 Chinese children: Clinical features and risk factors for renal involvement. J. Int. Med. Res. 2014, 42, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Pohl, M. Henoch–Schönlein purpura nephritis. Pediatric Nephrol. 2014, 30, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Elmas, A.T.; Tabel, Y. Platelet Counts in Children With Henoch-Schonlein Purpura-Relationship to Renal Involvement. J. Clin. Lab. Anal. 2016, 30, 71–74. [Google Scholar] [CrossRef]
- González-Gay, M.A.; Ortiz-Sanjuán, F.; Armesto, S.; Loricera, J.; González-Vela, M.C.; Palmou-Fontana, N.; González-Gay, M.A. Relapses in patients with Henoch–Schönlein purpura. Medicine 2016, 95, e4217. [Google Scholar]
- Liao, C.-H.; Tsai, M.; Yang, Y.-H.; Chiang, B.-L.; Wang, L.-C. Onset age is a risk factor for refractory pediatric IgA vasculitis: A retrospective cohort study. Pediatric Rheumatol. 2020, 18, 1–10. [Google Scholar] [CrossRef]
- Hung, S.-P.; Yang, Y.-H.; Lin, Y.-T.; Wang, L.-C.; Lee, J.-H.; Chiang, B.-L. Clinical Manifestations and Outcomes of Henoch-Schönlein Purpura: Comparison between Adults and Children. Pediatr. Neonatol. 2009, 50, 162–168. [Google Scholar] [CrossRef]
- Bluman, J.; Goldman, R.D. Child Health Update Henoch-Schönlein purpura in children Limited benefit of corticosteroids. Can. Fam. Physician 2014, 60, 1007–1009. [Google Scholar] [PubMed]
- Jauhola, O.; Ronkainen, J.; Koskimies, O.; Ala-Houhala, M.; Arikoski, P.; Hölttä, T.; Jahnukainen, T.; Rajantie, J.; Örmälä, T.; Nuutinen, M. Outcome of Henoch–Schönlein purpura 8 years after treatment with a placebo or prednisone at disease onset. Pediatric Nephrol. 2012, 27, 933–939. [Google Scholar] [CrossRef]
- Shin, J., II; Lee, J.S. Treatment of Severe Henoch-Schoenlein Purpura Nephritis in Children. J. Korean Soc. Pediatric Nephrol. 2010, 14, 10. [Google Scholar] [CrossRef]
- Dudley, J.; Smith, G.; Llewelyn-Edwards, A.; Bayliss, K.; Pike, K.; Tizard, J.; Tuthill, D.; Millar-Jones, L.; Bowler, I.; Williams, T.; et al. Randomised, double-blind, placebo-controlled trial to determine whether steroids reduce the incidence and severity of nephropathy in Henoch-Schonlein Purpura (HSP). Arch. Dis. Child. 2013, 98, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Chartapisak, W.; Opastiraku, S.L.; Willis, N.S.; Craig, J.; Hodson, E.M. Prevention and treatment of renal disease in Henoch-Schonlein purpura: A systematic review. Arch. Dis. Child. 2008, 94, 132–137. [Google Scholar] [CrossRef]
- Zaffanello, M.; Brugnara, M.; Franchini, M. Therapy for Children with Henoch-Schonlein Purpura Nephritis: A Systematic Review. Sci. World J. 2007, 7, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.S.; Chung, H.S.; Kang, K.-S.; Han, K.H. High-dose methylprednisolone pulse therapy for treatment of refractory intestinal involvement caused by Henoch-Schönlein purpura: A case report. J. Med. Case Rep. 2015, 9, 65. [Google Scholar] [CrossRef] [PubMed]
- Hou, L.; Zhang, Z.; Du, Y. Leflunomide therapy for IgA vasculitis with nephritis in children. BMC Pediatrics 2021, 21, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Weiss, P.F.; Klink, A.J.; Localio, R.; Hall, M.; Hexem, K.; Burnham, J.M.; Keren, R.; Feudtner, C. Corticosteroids May Improve Clinical Outcomes During Hospitalization for Henoch-Schonlein Purpura. Pediatrics 2010, 126, 674–681. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | ||
|---|---|---|
| Age in Years | ||
| Range | 1–12 | |
| Mean | 5.87 ± 2.812 | |
| Age | No | % |
| ≤6 | 53 | 59.56 |
| >6 to <10 | 29 | 32.59 |
| >10 | 7 | 7.85 |
| Gender | No | % |
| Male | 50 | 56.2 |
| Female | 39 | 43.8 |
| Male to female ratio | 1.28:1 | |
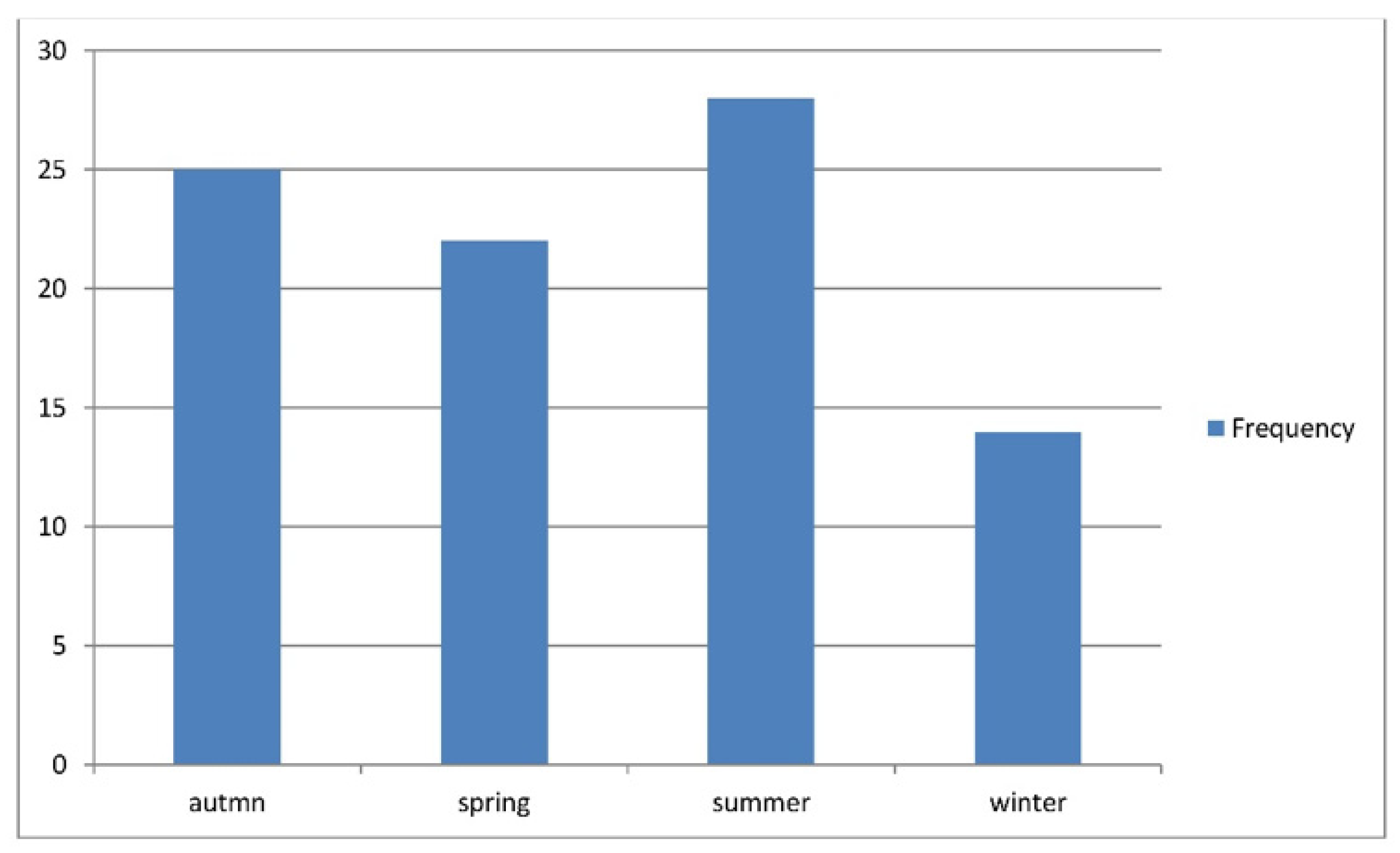
| Seasonal distribution | No | % |
| Autumn | 25 | 28.1 |
| Spring | 22 | 24.7 |
| Summer | 28 | 31.5 |
| Winter | 14 | 15.7 |
| Illness before appearance of disease | No | % |
| No illness | 63 | 70.8 |
| URTI | 22 | 24.7 |
| Gastroenteritis | 4 | 4.5 |
| Mean duration of admission in days | 4.88 ± 2.767 | |
| Mean duration of illness before admission | 5.66 ± 4.722 | |
| Skin Rash | N | % |
|---|---|---|
| Skin rash | 89 | 100 |
| Arthritis | ||
| arthritis | 66 | 74.2 |
| Without arthritis | 23 | 25.8 |
| Joints involved | ||
| Ankle | 30 | 45.46 |
| Ankle + Elbow | 1 | 1.5 |
| Ankle E + Wrist | 3 | 4.6 |
| Elbow + Knee | 1 | 1.5 |
| Elbow+ Wrist | 3 | 4.6 |
| Knee | 8 | 12.3 |
| Knee + Ankle | 19 | 29.3 |
| Wrist | 1 | 1.5 |
| GIT involvement | 54 | 60.7 |
| Abdominal pains | 54 | 60.7 |
| Bleeding (lower GIT) | 16 | 29.6 |
| Bleeding (upper) | 2 | 3.7 |
| Vomiting and diarrhea | 18 | 33.3 |
| Intussusception | 5 | 9.2 |
| Renal involvement | 21 | 23.6 |
| Microscopic hematuria | 18 | 85.7 |
| Macroscopic hematuria | 3 | 14.3 |
| WBC in urine | 11 | 52.3 |
| Proteinuria | 5 | 23.8 |
| Hypertension | 5 | 23.8 |
| Nephrotic syndrome | 0 | 0 |
| Nephritis with renal impairment | 3 | 14.2 |
| Testicular involvement | 6 | 6.7 |
| Laboratory Findings | Number of Positive Tested Cases | % |
|---|---|---|
| Anemia (hemoglobin < 110 g/L) | 0 (89) | 0 |
| Thrombocytosis (platelets > 500, 109/L) | 31 (89) | 34.8 |
| Thrombocytosis (platelets > 700, 109/L) | 7 | 7.9 |
| Leukocytosis (WBC > 11, 109/L) | 41 (89) | 46 |
| Elevated ESR (ESR > 20 mm/h) | 35 (74) | 47 |
| Positive C-reactive protein | 15 (35) | 43 |
| Positive ASO titer | 13 (27) | 48 |
| t-Test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Test Description | Levene’s Test for Equality of Variances | t-Test for Equality of Means | ||||||||
| F | Sig. | t | Df | Sig. (2-Tailed) | Mean Difference | Std. Error Difference | 95% Confidence Interval of the Difference | |||
| Lower | Upper | |||||||||
| duration of illness | Equal variances assumed | 7.861 | 0.006 | 11.698 | 87 | 0.000 | 17.46328 | 1.49290 | 14.49598 | 20.43057 |
| Equal variances not assumed | 12.742 | 73.377 | 0.000 | 17.46328 | 1.37054 | 14.73204 | 20.19452 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dawood, S.A.; Abodiah, A.M.; Alqahtani, S.M.; Shati, A.A.; Alqahtani, Y.A.; Alshehri, M.A.; Mahmood, S.E. Clinico-Epidemiological Profile and Outcome of Children with IgA Vasculitis in Aseer Region, Southwestern Saudi Arabia. Healthcare 2021, 9, 1694. https://doi.org/10.3390/healthcare9121694
Dawood SA, Abodiah AM, Alqahtani SM, Shati AA, Alqahtani YA, Alshehri MA, Mahmood SE. Clinico-Epidemiological Profile and Outcome of Children with IgA Vasculitis in Aseer Region, Southwestern Saudi Arabia. Healthcare. 2021; 9(12):1694. https://doi.org/10.3390/healthcare9121694
Chicago/Turabian StyleDawood, Samy A., Abdoh M. Abodiah, Saleh M. Alqahtani, Ayed A. Shati, Youssef A. Alqahtani, Mohammed A. Alshehri, and Syed E. Mahmood. 2021. "Clinico-Epidemiological Profile and Outcome of Children with IgA Vasculitis in Aseer Region, Southwestern Saudi Arabia" Healthcare 9, no. 12: 1694. https://doi.org/10.3390/healthcare9121694
APA StyleDawood, S. A., Abodiah, A. M., Alqahtani, S. M., Shati, A. A., Alqahtani, Y. A., Alshehri, M. A., & Mahmood, S. E. (2021). Clinico-Epidemiological Profile and Outcome of Children with IgA Vasculitis in Aseer Region, Southwestern Saudi Arabia. Healthcare, 9(12), 1694. https://doi.org/10.3390/healthcare9121694