
The European Health Union: European Union’s Concern about Health for All. Concepts, Definition, and Scenarios


Abstract
:1. Introduction
- Refine the sense of purpose
- Understand the driving forces or key patterns and trends
- Develop scenario plots
- Plot strategy, rehearse, and converse [30].
2. Materials and Methods
3. Results
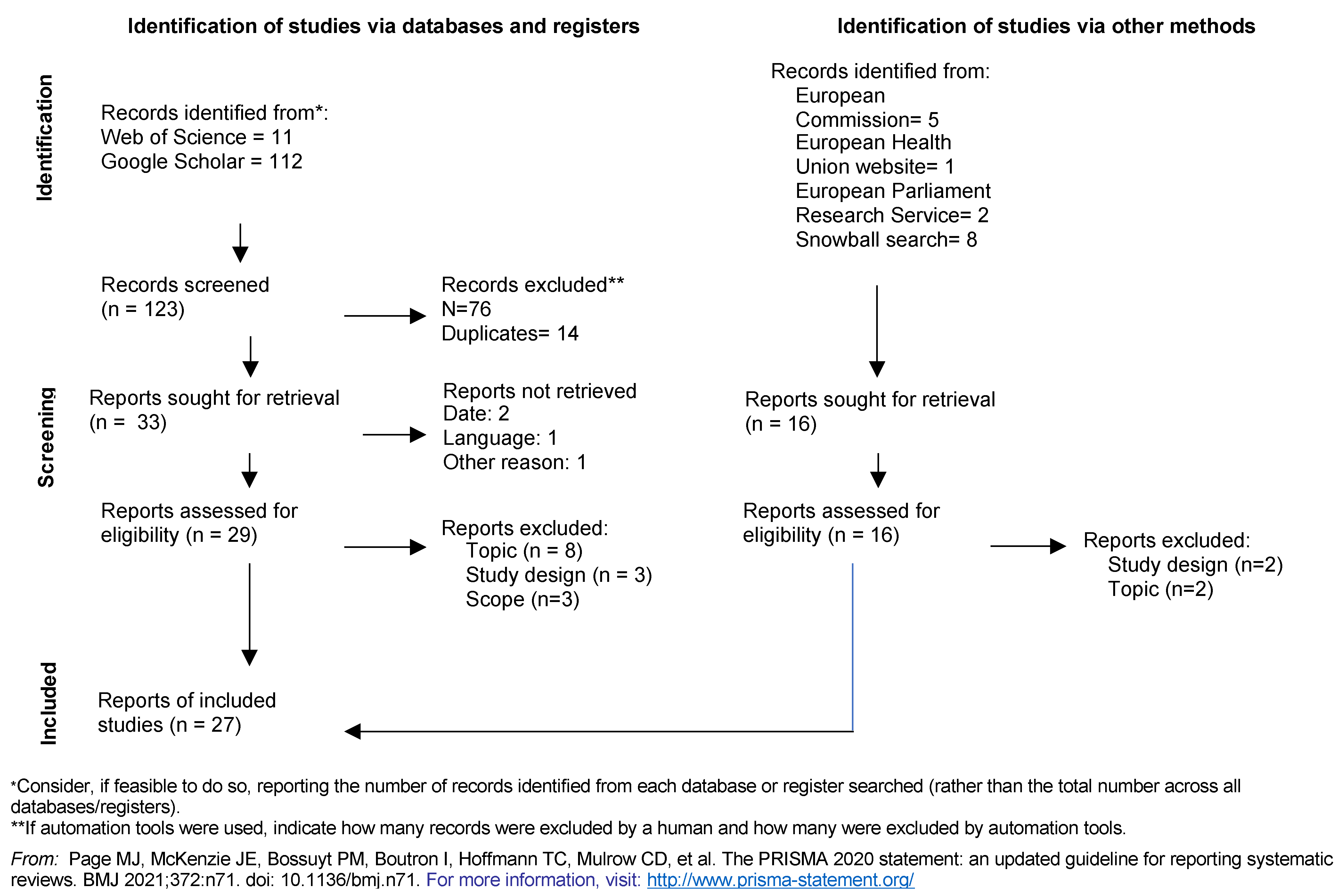
3.1. Systematic Literature Review

3.1.1. Components and Concepts of a European Health Union
3.1.2. The Definition of a European Health Union
3.2. Driving Forces, Key Patterns, and Trends
3.3. Scenario Plots
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CFR | Charter of Fundamental Rights |
| EC | European Commission |
| ECDC | European Centre for Disease Prevention and Control |
| EHU | European Health Union |
| EMA | European Medicines Agency |
| EP | European Parliament |
| EPRS | European Parliament Research Service |
| EU | European Union |
| HERA | European Health Emergency Preparedness and Response Authority |
| HiAP | Health in All Policies |
| HSC | Health Security Committee |
| IHR | International Health Regulations |
| JPA | Joint Procurement Agreement |
| MS | Member States |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-analyses |
| SANRA | Scale for the Assessment of Narrative Review Articles |
| SARS | Severe Acute Respiratory Syndrome |
| SDGs | Sustainable Development Goals |
| TEU | Treaty of the European Union |
| TFEU | Treaty on the Functioning of the European Union |
| WHO | World Health Organization |
References
- Davesne, A.; Guigner, S. La Communauté européenne de la santé (1952–1954). Polit. Eur. 2013, 41, 40–63. [Google Scholar] [CrossRef]
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 30 May 2021).
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-13 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-mission-briefing-on-covid-19---13-march-2020 (accessed on 30 May 2021).
- Anderson, M.; McKee, M.; Mossialos, E. Covid-19 exposes weaknesses in European response to outbreaks. BMJ 2020, 368, m1075. [Google Scholar] [CrossRef] [Green Version]
- European Union Consolidated Version of the Treaty on European Union. Off. J. Eur. Union 2016, 204. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A12012M%2FTXT (accessed on 21 November 2021).
- European Union Consolidated Version of the Treaty on the Functioning of the European Union. Off. J. Eur. Union 2012, 344. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A12012E%2FTXT (accessed on 21 November 2021).
- European Union Charter of Fundamental Rights of the European Union. Off. J. Eur. Union 2012, 17.
- European Parliament The Principle of Subsidiarity|Fact Sheets on the European Union. Available online: https://www.europarl.europa.eu/factsheets/en/sheet/7/the-principle-of-subsidiarity (accessed on 30 May 2021).
- Greer, S.L.; Fahy, N.; Jarman, H.; Elliott, H.A.; Wismar-European, M.; Rozenblum, S.; Palm, W.; Wismar, M. Everything You Always Wanted to Know about the European Union Health Policies but Were Afraid to Ask; European Observatory on Health Systems and Policies: Geneva, Switzerland, 2019; 202p. [Google Scholar]
- European Union Tobacco Products Directive. Off. J. Eur. Union 2014, 127, 38.
- Bartlett, O.; Naumann, A. Reinterpreting the health in all policies obligation in Article 168 TFEU: The first step towards making enforcement a realistic prospect. Health Econ. Policy Law 2021, 16, 8–22. [Google Scholar] [CrossRef]
- Purnhagen, K.P.; de Ruijter, A.; Flear, M.L.; Hervey, T.K.; Herwig, A. More competences than you knew? The web of health competence for European Union action in response to the COVID-19 outbreak. Eur. J. Risk Regul. 2020, 11, 297–306. [Google Scholar] [CrossRef] [Green Version]
- Merkel, B. The new EU health strategy: A step forward or another example of “bureaucracy total control”? Clin. Med. J. R. Coll. Physicians Lond. 2008, 8, 280–282. [Google Scholar] [CrossRef]
- Birt, C.A.; Gunning-Schepers, L.; Hayes, A.; Joyce, L. How should public health policy be developed? A case study in european public health. J. Public Health 1997, 19, 262–267. [Google Scholar] [CrossRef] [Green Version]
- Brand, H. A new agenda for health in Europe. Eur. J. Public Health 2013, 23, 904–905. [Google Scholar] [CrossRef] [Green Version]
- Vollaard, H.; Martinsen, D.S. The rise of a European healthcare union. Comp. Eur. Polit. 2017, 15, 337–351. [Google Scholar] [CrossRef]
- Duncan, B. Health policy in the European Union: How it’s made and how to influence it. BMJ 2002, 324, 1027–1030. [Google Scholar] [CrossRef] [Green Version]
- Rosenkötter, N.; Clemens, T.; Sørensen, K.; Brand, H. Twentieth anniversary of the European Union health mandate: Taking stock of perceived achievements, failures and missed opportunities—A qualitative study. BMC Public Health 2013, 13, 1074. [Google Scholar] [CrossRef] [Green Version]
- Andriukaitis, V. The European Health Union is an initiative with potential to shape European politics for decades to come. Eurohealth 2020, 26, 29–30. [Google Scholar]
- Townend, D.; van de Pas, R.; Bongers, L.; Haque, S.; Wouters, B.; Pilot, E.; Stahl, N.; Schröder-Bäck, P.; Shaw, D.; Krafft, T. What is the role of the european union in the COVID-19 pandemic? Med. Law 2020, 39, 249–268. [Google Scholar]
- European Parliament Resolution of 10 July 2020 on the EU’s Public Health Strategy Post-COVID-19 (2020/2691(RSP)). Available online: https://www.europarl.europa.eu/doceo/document/TA-9-2020-0205_EN.html (accessed on 22 June 2021).
- European Parliament. Uncertainty/EU/Hope: Public Opinion in Times of COVID-19; European Parliament: Brussels, Belgium, 2020. [Google Scholar]
- European Commission Standard Eurobarometer 94-Winter 2020-2021-Public Opinion in the European Union. Available online: https://europa.eu/eurobarometer/surveys/detail/2355 (accessed on 12 May 2021).
- von der Leyen, U. State of the Union Address by President von der Leyen. Available online: https://ec.europa.eu/commission/presscorner/detail/en/SPEECH_20_1655 (accessed on 17 December 2020).
- European Commission. Communication: Building a European Health Union: Reinforcing the EU’s Resilience for Cross-Border Health Threats; European Commission: Brussels, Belgium, 2020; pp. 1–43. [Google Scholar]
- European Commission. Proposal for a Regulation of the European Parliament and of the Council on Serious Cross-border threats to health and repealing Decision No 1082/2013/EU; European Commission: Brussels, Belgium, 2020. [Google Scholar]
- European Commission. Proposal for a Regulation of the European Parliament and of the Council Amending Regulation (EC) No 851/2004 Establishing a European Centre for Disease Prevention and Control; European Commission: Brussels, Belgium, 2020. [Google Scholar]
- European Commission. Proposal for a Regulation of the European Parliament and of the Council on a Reinforced Role for the European Medicines Agency in Crisis Preparedness and Management for Medicinal Products and Medical Devices; European Commission: Brussels, Belgium, 2020. [Google Scholar]
- European Commission. White Paper on the Future of Europe. Reflections and Scenarios for the EU27 by 2025; European Commission: Brussels, Belgium, 2017; 32p. [Google Scholar]
- Neiner, J.A.; Howze, E.H.; Greaney, M.L. Using scenario planning in public health: Anticipating alternative futures. Health Promot. Pract. 2004, 5, 69–79. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- European Health Union. Available online: https://europeanhealthunion.eu/ (accessed on 30 June 2021).
- European Commission. European Health Union. Available online: https://ec.europa.eu/info/strategy/priorities-2019-2024/promoting-our-european-way-life/european-health-union_en (accessed on 30 June 2021).
- European Parliament Think Tank. Available online: https://www.europarl.europa.eu/thinktank/en/home.html (accessed on 30 June 2021).
- McArthur, A.; Klugárová, J.; Yan, H.; Florescu, S. Innovations in the systematic review of text and opinion. Int. J. Evid. Based. Healthc. 2015, 13, 188–195. [Google Scholar] [CrossRef] [Green Version]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA—A scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Kosow, H.; Gaßner, R. Methods of Future and Scenario Analysis; German Development Institute: Bonn, Germany, 2008; 133p. [Google Scholar]
- PRISMA. Available online: http://prisma-statement.org/prismastatement/flowdiagram.aspx (accessed on 23 November 2020).
- Kickbusch, I. If you want a stronger EU: Build a European Health Union. Eurohealth 2020, 26, 32. [Google Scholar]
- Brooks, E.; de Ruijter, A.; Greer, S.L. COVID-19 and European health policy: From crisis to collective action. In Social Policy in the European Union: State of Play 2020. Facing the Pandemic; Vanhercke, B., Spasova, S., Fronteddu, B., Eds.; European Trade Union Institute (ETUI) and European Social Observatory (OSE): Brussels, Belgium, 2021; pp. 33–52. ISBN 978-2-87452-588-9. [Google Scholar]
- Quaglio, G. Forestalling future health crises. In Towards a More Resilient Europe Post-Coronavirus. Options to Enhance the Eu’s Resilience to Structural Risks; European Parliamentary Research Service (EPRS) and the Directorates-General for Internal Policies (IPOL) and External Policies (EXPO): Brussels, Belgium, 2021; ISBN 978-92-846-7985-0. [Google Scholar]
- Brooks, E.; Geyer, R. The development of EU health policy and the COVID-19 pandemic: Trends and implications. J. Eur. Integr. 2020, 42, 1057–1076. [Google Scholar] [CrossRef]
- Greer, S.; De Ruijter, A. EU health law and policy in and after the COVID-19 crisis. Eur. J. Public Health 2020, 30, 623–624. [Google Scholar] [CrossRef]
- Renda, A.; Castro, R. Towards stronger EU governance of health threats after the COVID-19 pandemic. Eur. J. Risk Regul. 2020, 11, 273–282. [Google Scholar] [CrossRef] [Green Version]
- Villa, S.; van Leeuwen, R.; Gray, C.C.; van der Sande, M.; Konradsen, F.; Fröschl, G.; Nord, D.G.; da Costa, C.P.; Ramirez-Rubio, O.; Abubakar, I.; et al. HERA: A new era for health emergency preparedness in Europe? Lancet 2021, 397, 2145–2147. [Google Scholar] [CrossRef]
- Manifesto for a European Health Union. Available online: https://www.ehfg.org/documents/EHFG2020/partners/Manifesto-European-Health-Union/#page=1 (accessed on 29 April 2021).
- Medialdea Carrera, R. The importance of cross-border pandemic preparedness. Eurohealth 2020, 26, 34. [Google Scholar]
- Vervoort, D.; van Daalen, K.R. The European Union, economies and public health: Not one without the other. Public Health 2021, 194, 1–3. [Google Scholar] [CrossRef]
- Guy, M. Towards a European Health Union: What Role for Member States? Eur. J. Risk Regul. 2020, 11, 757–765. [Google Scholar] [CrossRef]
- Anderson, M.; Mossialos, E. Time to strengthen capacity in infectious disease control at the European level. Int. J. Infect. Dis. 2020, 99, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Beaussier, A.L.; Cabane, L. Strengthening the EU’s response capacity to health emergencies: Insights from eu crisis management mechanisms. Eur. J. Risk Regul. 2020, 11, 808–820. [Google Scholar] [CrossRef]
- Clemens, T.; Brand, H. Will COVID-19 lead to a major change of the EU Public Health mandate? A renewed approach to EU’s role is needed. Eur. J. Public Health 2020, 30, 624–625. [Google Scholar] [CrossRef]
- Bazzan, G. Exploring Integration Trajectories for a European Health Union. Eur. J. Risk Regul. 2020, 11, 736–746. [Google Scholar] [CrossRef]
- Kickbusch, I.; de Ruijter, A. How a European health union can strengthen global health. Lancet Reg. Health Eur. 2021, 1, 100025. [Google Scholar] [CrossRef]
- Sipido, K.R.; Antoñanzas, F.; Celis, J.; Degos, L.; Frackowiak, R.; Fuster, V.; Ganten, D.; Gay, S.; Hofstraat, H.; Holgate, S.T.; et al. Overcoming fragmentation of health research in Europe: Lessons from COVID-19. Lancet 2020, 395, 1970–1971. [Google Scholar] [CrossRef]
- Quaglio, G. EU Public Health Policy. PE 652.027; European Parliament Research Service: Brussels, Belgium, 2020. [Google Scholar]
- De Ruijter, A. What do we actually mean by a “European Health Union”? Eurohealth 2020, 26, 30–31. [Google Scholar]
- McEvoy, E.; Ferri, D. The role of the joint procurement agreement during the COVID-19 Pandemic: Assessing Its usefulness and discussing its potential to support a european health union. Eur. J. Risk Regul. 2020, 11, 851–863. [Google Scholar] [CrossRef]
- Biondi, A.; Stefan, O. EU Health Union and State Aid Policy: With Great(er) Power Comes Great Responsibility. Eur. J. Risk Regul. 2020, 11, 894–902. [Google Scholar] [CrossRef]
- Brand, A.; Stöckel, S. Die öffentliche Sorge um die Gesundheit aller-ein sinnvoller Anspruch? In Individuelle Gesundheit versus Public Health? Brand, A., Engelhardt, D.V., Simon, A., Wehkamp, K.-H., Eds.; LIT Verlag: Münster, Germany, 2002; pp. 11–28. [Google Scholar]
- World Health Organization. Regional Office for Europe. In Health21. The Health for All Policy Framework for the WHO European Region; WHO: Copenhagen, Denmark, 1999. [Google Scholar]
- Jones, E.; Kelemen, R.D.; Meunier, S. Failing Forward? The Euro Crisis and the Incomplete Nature of European Integration. Comp. Polit. Stud. 2016, 49, 1010–1034. [Google Scholar] [CrossRef]
- Rhodes, M. ‘Failing forward’: A critique in light of COVID-19. J. Eur. Public Policy 2021, 28, 1537–1554. [Google Scholar] [CrossRef]
- Hervey, T.; de Ruijter, A. The Dynamic Potential of European Union Health Law. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- European Commission. Commission Decision Establishing the Health Emergency Preparedness and Response Authority; European Commission: Brussels, Belgium, 2021. [Google Scholar]
- European Commission. EU4Health 2021–2027—A vision for a healthier European Union | Public Health. Available online: https://ec.europa.eu/health/funding/eu4health_en (accessed on 17 December 2020).
- European Council Conference on the Future of Europe. Available online: https://www.consilium.europa.eu/en/policies/conference-on-the-future-of-europe/ (accessed on 3 August 2021).
- Conference on the Future of Europe. Available online: https://futureu.europa.eu/?locale=en (accessed on 3 August 2021).
- Fitch, K.; Bernstein, S.J.; Burnand, B.; Aguilar, M.D.; LaCalle, J.R.; Lázaro, P.; van het Loo, M.; McDonnell, J.; Vader, J.P.; Kahan, J.P. RAND/UCLA Appropriateness Method User’s Manual; RAND Corporation: Santa Monica, CA, USA, 2001; ISBN 0-8330-2918-5. [Google Scholar]
- Directorate-General for Research and Innovation; Varnai, P.S. The Scientific, Technological and Societal Conditions for the End of the COVID-19 Crisis; Publications Office of the EU: Brussels, Belgium, 2021.

{kind=link}
| Factors/Drivers | Example: Making a Full Move towards Supranational Action | Scenario 1 | Scenario 2 | Scenario 3 | Scenario 4 |
|---|---|---|---|---|---|
| Example of pre-determined factor: funding | Funding is thought to support fully the supranational level. | ||||
| Pre-determined factor 1 | |||||
| Pre-determined factor 2 | |||||
| Unpredictable factor 1 | |||||
| Unpredictable factor 2 |
| Scenario 1 Making a Full Move towards Supranational Action | Scenario 2 Improving Efficiency in the Actual Framework | Scenario 3 More Coordination but No Real Change | Scenario 4 in a Full Inter-governmentalism Direction | Scenario 5 Fragmentation of the European Union (EU) | ||
|---|---|---|---|---|---|---|
| Predetermined forces | Surveillance and monitoring | The European Center of Disease Control (ECDC) has the power to coordinate the action of all Member States (MS). | The MS give regular and up-to-date reports to the ECDC and coordinate their actions following the agency recommendations. Binding possibilities. | Merely incentives to encourage MS to deliver data. ECDC support. | The MS coordinate on their own or through intergovernmental mechanisms. | Coordination is at its lowest, and surveillance and monitoring are managed only at the national level. |
| Crisis preparedness | A new agency (e.g., European Health Emergency Preparedness and Response Authority (HERA)) is at the center and coordinate MS and EU actions. | Having binding coordination plans but leaving the decision-making to the MS. Possible extension of the Health Security Committee (HSC) and creation of HERA. | Staying on incentives. | Crisis preparedness at the national level. No EU coordination plans. Possibility of coordination between neighboring countries. | Crisis preparedness at the national level. Strictly bilateral agreements. | |
| Funding | Funding is thought to support fully the supranational level. | Funding is made sufficient to support the action of the European agencies and European research to its best. | Funding is insufficient to support the planned European actions. The level of funding is non-consensual between the European institutions and/or the MS. | Funding of the EU level is kept at a minimal level and stays at MS level. | Funding is invested back at national level. | |
| Scenario 1 Making a Full Move towards Supranational Action | Scenario 2 Improving Efficiency in the Actual Framework | Scenario 3 More Coordination but No Real Change | Scenario 4 in a Full Intergovernmentalism Direction | Scenario 5 Fragmentation of the European Union | ||
|---|---|---|---|---|---|---|
| Unpredictable forces | Political will | The MS all agree to develop EU action in public health. The President of the European Commission (EC) is ready to continue in the same direction and change the EU treaties to recognize the importance of health. The EC continues its engagement towards health. | The MS decide with the EC to develop the EU action in public health inside the current treaties provision and agree to follow the EC’s lead as long as the national competence is respected. | Divergences between MS and between the European institutions. Change of the importance of public health depending on the political agenda. | The MS decide to keep full public health power and action at the national level. | Euroscepticism is at its fullest and the European level is removed from the equation. |
| Vision of public health expenditures | Public health is envisioned as an investment for protecting all EU citizens. | Vision of public health evolves towards investment. | Public health is still envisioned mainly as a cost at the European and national levels. | No willingness to invest at the European level. | No willingness to invest at the European level. | |
| Population interest and awareness | European citizens ask for more competence at the EU level and expect a European coordinated action. They are aware of the possibilities of European public health. | European citizens ask for more competence at the EU level and expect a European coordinated action. They are aware of the possibilities of European public health. | Differences between awareness and knowledge of European citizens on EU health competences. | Lack of knowledge of the EU competence and/or disinterest for the EU level of action. | Lack of knowledge of the EU competence and/or disinterest for the EU level of action and/or important Euroscepticism. | |
| Global health | The EU can speak and act as one voice because of the development of a central competence. | Possible use of other legislations to act on global health and set standards. Intend for more common statements between MS. | No real position of the EU on global health. Difficulty to coordinate with international agencies. | No European position through the EC or institutions. Possible coordination between some countries or through the World Health Organization (WHO). | No European position. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nabbe, M.; Brand, H. The European Health Union: European Union’s Concern about Health for All. Concepts, Definition, and Scenarios. Healthcare 2021, 9, 1741. https://doi.org/10.3390/healthcare9121741
Nabbe M, Brand H. The European Health Union: European Union’s Concern about Health for All. Concepts, Definition, and Scenarios. Healthcare. 2021; 9(12):1741. https://doi.org/10.3390/healthcare9121741
Chicago/Turabian StyleNabbe, Marie, and Helmut Brand. 2021. "The European Health Union: European Union’s Concern about Health for All. Concepts, Definition, and Scenarios" Healthcare 9, no. 12: 1741. https://doi.org/10.3390/healthcare9121741
APA StyleNabbe, M., & Brand, H. (2021). The European Health Union: European Union’s Concern about Health for All. Concepts, Definition, and Scenarios. Healthcare, 9(12), 1741. https://doi.org/10.3390/healthcare9121741