
How Did the COVID-19 Pandemic Effect Dental Patients? An Italian Observational Survey Study

 ,
, 
 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Type
2.2. Study Population
2.3. Data Collection Technique
2.4. Data Analysis Procedure
3. Results
3.1. Part A—Geographic, Demographic, and Personal Data (Questions n = 10)
3.2. Part B—Patients’ Attitude toward Oral Health Selfcare and Lifestyle (n = 16)
3.3. Part C—Patients’ Attitude toward Dental Practice (n = 13)
3.4. Regression Models
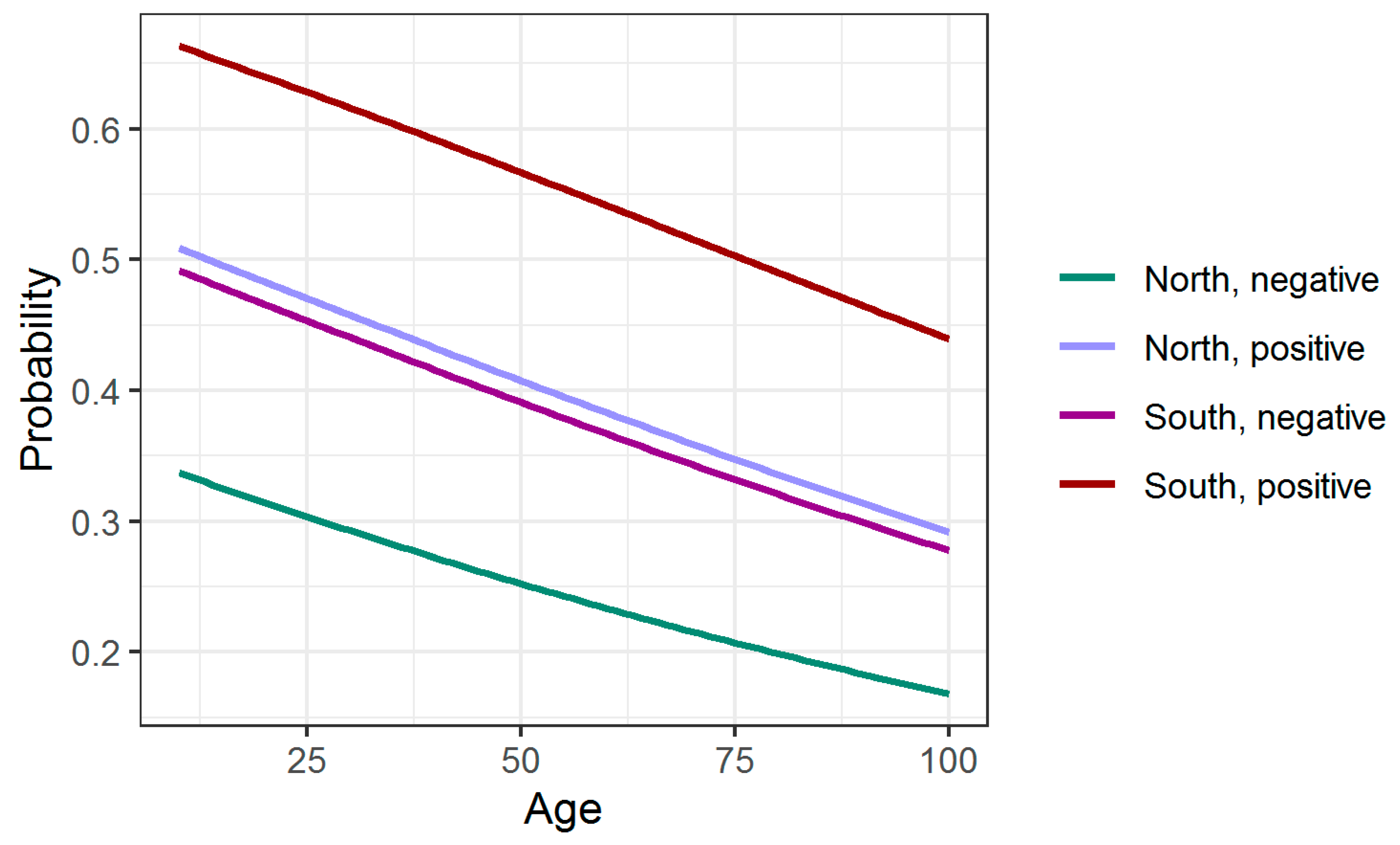
3.4.1. Probability of Eating Too Much
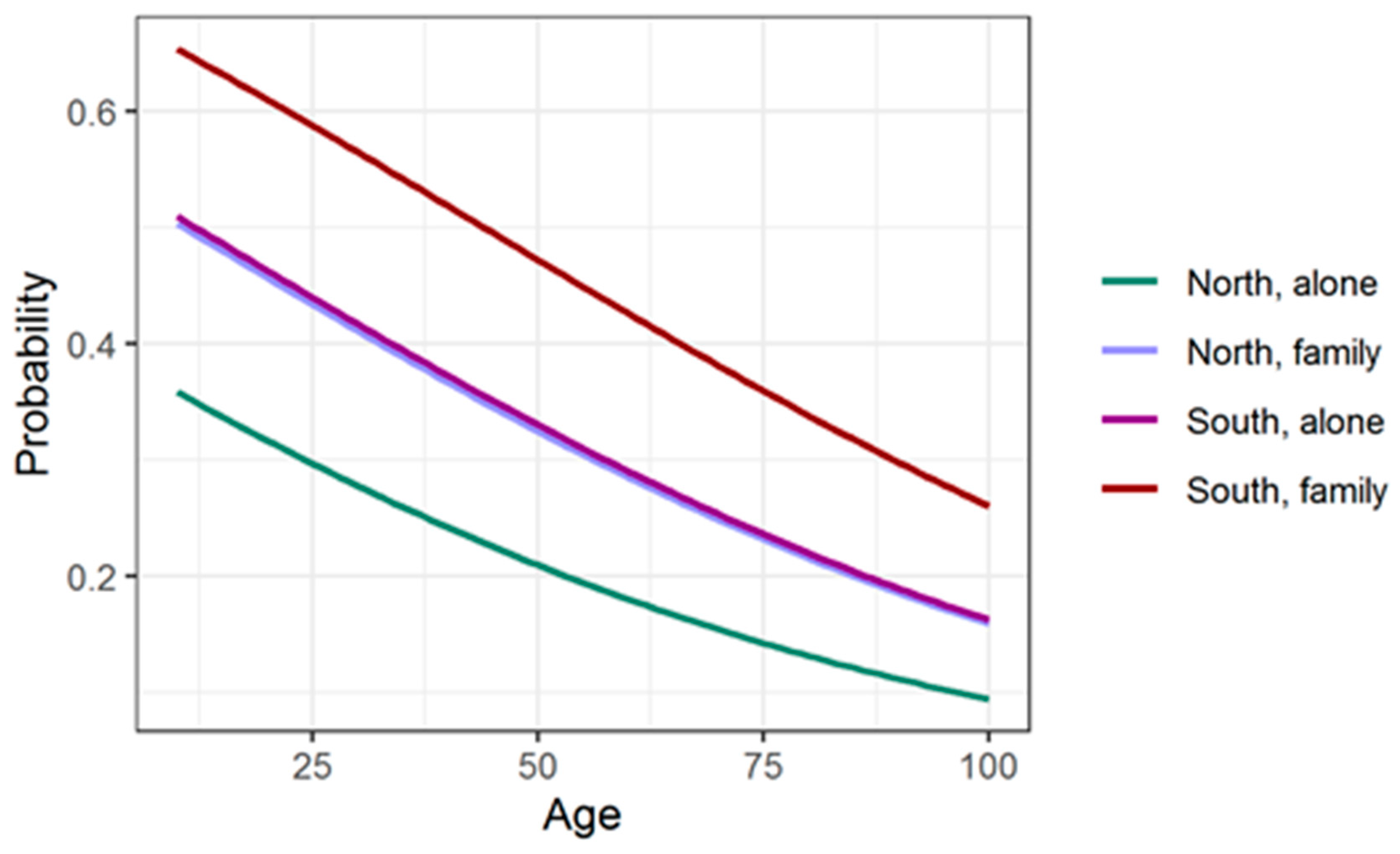
3.4.2. Probability of Introducing Cariogenic Food
4. Discussion
4.1. Limitations
4.2. Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mavragani, A. Tracking COVID-19 in Europe: Infodemiology approach. JMIR Public Health Surveill 2020, 6, e18941. [Google Scholar] [CrossRef] [Green Version]
- Specktor, B. LiveScience. 2020 Mar. Coronavirus: What Is ‘Flattening the Curve,’ and Will It Work? Available online: https://www.livescience.com/coronavirus-flatten-the-curve.html (accessed on 1 October 2021).
- To, K.K.; Tsang, O.T.; Yip, C.C.; Chik-Yan Yip, C.; Chan, K.; Wu, T.; Chan, J.M.C.; Leung, W.S.; Chik, T.S.H.; Choi, C.Y.C.; et al. Consistent detection of 2019 novel coronavirus in saliva. Clin. Infect. Dis. 2020, 71, 841–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral. Sci. 2020, 12, 9. [Google Scholar] [CrossRef]
- Fallahi, H.R.; Keyhan, S.O.; Zandian, D.; Kim, S.G.; Cheshmi, B. Being a front-line dentist during the Covid-19 pandemic: A literature review. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 12. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing; R Team: Vienna, Austria, 2020. [Google Scholar]
- Akaike, H. Information theory and an extension of the maximum likelihood principle. In Selected Papers of Hirotugu Akaike; Parzen, E., Tanabe, K., Kitagawa, G., Eds.; Springer: New York, NY, USA, 1998; pp. 199–213. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Decreto Natale—Governo IT. Available online: https://www.governo.it/sites/new.governo.it/files/16-9-decreto-natale1534.pdf (accessed on 1 October 2021).
- Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. “Pandemic fear” and COVID-19: Mental health burden and strategies. Braz. J. Psychiatry 2020, 42, 232–235. [Google Scholar] [CrossRef] [Green Version]
- Duś-Ilnicka, I.; Krala, E.; Cholewińska, P.; Radwan-Oczko, M. The use of saliva as a biosample in the light of COVID-19. Diagnostics 2021, 11, 1769. [Google Scholar] [CrossRef] [PubMed]
- Mazur, M.; Duś-Ilnicka, I.; Jedliński, M.; Ndokaj, A.; Janiszewska-Olszowska, J.; Ardan, R.; Radwan-Oczko, M.; Guerra, F.; Luzzi, V.; Vozza, I.; et al. Facial and oral manifestations following COVID-19 vaccination: A survey-based study and a first perspective. Int. J. Environ. Res. Public Health 2021, 18, 4965. [Google Scholar] [CrossRef]
- Campus, G.; Diaz Betancourt, M.; Cagetti, M.G.; Giacaman, R.A.; Manton, D.J.; Douglas, G.V.A.; Carvalho, T.S.; Carvalho, J.C.; Vukovic, A.; Cortés-Martinicorena, F.J.; et al. The COVID-19 pandemic and its global effects on dental practice. An international survey. J. Dent. 2021, 114, 103749. [Google Scholar] [CrossRef] [PubMed]
- Amankwah-Amoah, J.; Khan, Z.; Wood, G. COVID-19 and business failures: The paradoxes of experience, scale, and scope for theory and practice. Eur. Manag. J. 2020, 39, 179–184. [Google Scholar] [CrossRef]
- Survey Finds Shortcomings in Oral Health Habits. Available online: http://www.ada.org/en/publications/ada-news/2014-archive/october/survey-finds-shortcomings-in-oral-health-habits (accessed on 2 December 2021).
- Gupta, M. Ozone: An emerging prospect in dentistry. Indian J. Dent. Sci. 2012, 1, 47–50. [Google Scholar]
- Nardi, G.M.; Cesarano, F.; Papa, G.; Chiavistelli, L.; Ardan, R.; Jedlinski, M.; Mazur, M.; Grassi, R.; Grassi, F.R. Evaluation of salivary Matrix Metalloproteinase (MMP-8) in periodontal patients undergoing non-surgical periodontal therapy and mouthwash based on ozonated olive oil: A randomized clinical trial. Int. J. Environ. Res. Public Health 2020, 17, 6619. [Google Scholar] [CrossRef] [PubMed]
- Bains, V.K.; Bains, R. Is oral hygiene as important as hand hygiene during COVID-19 pandemic? Asian J. Oral Health Allied Sci. 2020, 10, 5. [Google Scholar] [CrossRef]
- Salamone, K.; Yacoub, E.; Mahoney, A.M.; Edward, K.L. Oral care of hospitalised older patients in the acute medical setting. Nurs. Res. Pract. 2013, 2013, 827670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coke, C.J.; Davison, B.; Fields, N.; Fletcher, J.; Rollings, J.; Roberson, L.; Challagundla, K.B.; Sampath, C.; Cade, J.; Farmer-Dixon, C.; et al. SARS-CoV-2 Infection and oral health: Therapeutic opportunities and challenges. J. Clin. Med. 2021, 10, 156. [Google Scholar] [CrossRef]
- Docimo, R.; Costacurta, M.; Gualtieri, P.; Pujia, A.; Leggeri, C.; Attinà, A.; Cinelli, G.; Giannattasio, S.; Rampello, T.; Di Renzo, L. Cariogenic risk and COVID-19 lockdown in a paediatric population. Int. J. Environ. Res. Public Health 2021, 18, 7558. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Silva-Boghossian, C.M.; Dezonne, R.S. What are the clinical and systemic results of periodontitis treatment in obese individuals? Curr. Oral Health Rep. 2021, 1, 1–18. [Google Scholar] [CrossRef]
- Al Mohaya, M.A.; Almaziad, M.M.; Al-Hamad, K.A.; Mustafa, M. Telemedicine among oral medicine practitioners during covid-19 pandemic and its future impact on the specialty. Risk Manag. Healthc. Policy 2021, 14, 4369–4378. [Google Scholar] [CrossRef] [PubMed]
- Ndokaj, A.; Iacono, R.; Pasqualotto, D.; Stamegna, C.; Capocci, M.; Guerra, F. Trends in sustainable dentistry. Clin. Ter. 2021, 172, 523–524. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Questionnaire Part A: Characteristics of Respondents | ||
|---|---|---|
| Q1: Age | 14–20 | 34 (3%) |
| 20–40 | 588 (51.8%) | |
| 40–60 | 434 (38.2%) | |
| 60–80 | 79 (7%) | |
| Q2: Gender | Female | 782 (68.9%) |
| Male | 353 (31.1%) | |
| Q3: Area of geographic origin | North Italy | 233 (20.6%) |
| Center Italy | 614 (54.1%) | |
| South Italy | 288 (25.3%) | |
| Q5: Civil status | Married | 725 (63.9%) |
| Single | 294 (25.9%) | |
| In separation | 97 (8.6%) | |
| Widow(er) | 19 (1.6%) | |
| Q6: Do you have any children? | Yes | 539 (45.8%) |
| No | 596 (54.2%) | |
| Q7: Do you live with your family? | Yes | 910 (80.2%) |
| No | 225 (19.8%) | |
| Q8: Level of education | Basic | 68 (6%) |
| Secondary | 534 (47%) | |
| Higher | 533 (46.7%) | |
| Q9: In this moment, you are positive for COVID-19? | Yes | 16 (1.4%) |
| No | 736 (64.8%) | |
| I don’t know | 383 (33.7%) | |
| Q10: Have you ever tested positive for COVID-19 in the past? | Yes | 39 (3.4%) |
| No | 903 (79.5%) | |
| I don’t know | 193 (17.1%) | |
| Questionnaire Part B: Respondents’ Attitude toward Oral Health Selfcare and Lifestyle | ||||
|---|---|---|---|---|
| Q11: How many times a year do you have an oral hygiene session (before COVID-19)? | 0 | 84 (7.4%) | ||
| 1 | 527 (46.5%) | |||
| 2 | 416 (36.7%) | |||
| 3 | 83 (7.3%) | |||
| 4 | 22 (2%) | |||
| Q12: Did you have had an oral hygiene session from March 2020 to November 2020? | Yes | 602 (53%) | ||
| No | 533 (47%) | |||
| Q13: What type of therapy have you been subjected to? | Ultrasound tartar ablation | 433 (38.2%) | ||
| Manual tartar ablation | 449 (39.6%) | |||
| Whitening | 43 (3.8%) | |||
| Dentin hypersensitivity treatment | 37 (3.3%) | |||
| Q14: When was the last time you went to the dentist? | Don’t remember | 47 (4.1%) | ||
| Last 3 months | 471 (41.5%) | |||
| Last 6 months | 230 (20.3%) | |||
| Last year | 267 (23.5%) | |||
| Last 2 years | 120 (10.6%) | |||
| Q15: From March 2020, on a scale of 0 to 10, how much has your fear of undergoing dental procedures increased (due to COVID-19 contagion)? | Q15 | Q16 | Q17 | |
| 0 | 444 (39.1%) | 106 (9.3%) | 368 (32.4%) | |
| 1 | 68 (6%) | 42 (3.7%) | 53 (4.7%) | |
| 2 | 104 (9.2%) | 64 (5.6%) | 47 (4.1%) | |
| Q16: How much does the fear of contagion affect your lifestyle (scale from 0 to 10)? | 3 | 84 (7.4%) | 94 (8.3%) | 64 (5.6%) |
| 4 | 53 (4.7%) | 93 (8.2%) | 49 (4.3%) | |
| 5 | 93 (8.2%) | 173 (15.2%) | 129 (11.4%) | |
| 6 | 84 (7.4%) | 126 (11.1%) | 85 (7.5%) | |
| Q17: How much has your attention changed towards home oral hygiene maneuvers (scale from 0 to 10)? | 7 | 66 (5.8%) | 121 (10.7%) | 90 (8%) |
| 8 | 78 (6.9%) | 173 (15.2%) | 107 (9.4%) | |
| 9 | 24 (2.1%) | 82 (7.2%) | 51 (4.5%) | |
| 10 | 37 (3.3%) | 65 (5.7%) | 99 (8.1%) | |
| Q18: How worried were you about contracting the coronavirus during a dental hygiene session? | Not at all | 389 (34.3%) | ||
| A little | 484 (42.6%) | |||
| Somewhat | 163 (14.4%) | |||
| A lot | 64 (5.6%) | |||
| Very | 18 (1.6%) | |||
| I don’t know | 16 (1.4%) | |||
| Q19: Which aids did you use for at-home oral hygiene during the first lockdown (March–May 2020). More than one answer was possible. | Manual brush | 605 (53.3%) | ||
| Electric brush | 435 (38.4%) | |||
| Floss | 532 (46.9%) | |||
| Tongue cleaner | 12 (1.1%) | |||
| Plaque detector | 47 (4.1%) | |||
| I don’t know | 64 (5.6%) | |||
| Q20: Did you use rinse at home during the first lockdown? | No | 520 (45.8%) | ||
| Chlorhexidine-based | 54 (4.8%) | |||
| Ozone-based | 330 (29.1%) | |||
| Iodopovidone-based | 200 (17.6%) | |||
| Hydrogen peroxide-based | 5 (0.4%) | |||
| Commercial mouthwash | 26 (2.3%) | |||
| Q21: Did you use probiotics during the first lockdown? | Yes | 158 (13.9%) | ||
| No | 977 (86.1%) | |||
| Q22: Do you think you have eaten too much of any type of food during the lockdown? | Yes | 442 (38.9%) | ||
| No | 693 (61.1%) | |||
| Q23: If you have abused any food, write which one. | Sweets | 729 (64.2%) | ||
| Bread, pizza | 615 (54.2%) | |||
| Wine | 106 (9.3%) | |||
| Meat | 115 (10.1%) | |||
| Q24: Do you think you smoked more during the lockdown than before? | Yes | 134 (11.8%) | ||
| No | 364 (32.1%) | |||
| I have never smoked | 370 (32.6%) | |||
| Now I do not smoke | 165 (14.5%) | |||
| More than 10 a day | 47 (4.1% | |||
| Less than 10 a day | 55 (4.8%) | |||
| Q25: Did you implement cariogenic foods during the lockdown (pasta, bread, sugars, sweets, snacks, chocolate)? | Yes | 533 (47%) | ||
| No | 602 (53%) | |||
| Questionnaire Part C: Respondents’ Attitude toward Dental Practice | |||||
|---|---|---|---|---|---|
| Q26: Which coronavirus prevention measures do you pay attention to most when you go to the dentist? Doing which of the previously listed procedures make you feel safer? | Q26 | Q27 | |||
| Sanitation of environments | 225 (19.8%) | 364 (32.1%) | |||
| Room ventilation | 40 (3.5%) | 69 (6.1%) | |||
| Temperature control | 80 (7%) | 33 (2.9%) | |||
| Use of protective equipment | 375 (33%) | 325 (28.6%) | |||
| Limitation of entries to the waiting area | 219 (19.3%) | 226 (19.9%) | |||
| Providing patients with masks and disinfectants | 49 (4.3%) | 43 (3.8%) | |||
| Telephone Pre-visit medical history check-up | 78 (6.9%) | 44 (3.9%) | |||
| All answers | 15 (1.3%) | 9 (0.8%) | |||
| Q28: Are you worried about going to visit a dentist to have a dental procedure? | Not at all | 422 (37.2%) | |||
| A little | 493 (43.4%) | ||||
| Somewhat | 142 (12.5%) | ||||
| A lot | 44 (3.9%) | ||||
| Very | 12 (1.1%) | ||||
| Don’t visit a dentist | 9 (0.8%) | ||||
| Don’t know | 12 (1.1%) | ||||
| Q29: Have you ever postponed the appointment for fear of becoming infected with COVID-19? | Yes | 129 (11.4%) | |||
| No | 978 (86.2%) | ||||
| I haven’t visited a dentist in this period | 28 (2.5%) | ||||
| I don’t feel it | I feel it lightly | I feel it in a moderate way | I feel it in an extreme way | ||
| Q30: What emotions stir in you to think about the coronavirus? | Fear | 269 (23.7%) | 494 (43.5%) | 343 (30.2%) | 30 (2.6%) |
| Anxiety | 300 (26.4%) | 432 (38.1%) | 339 (29.9%) | 64 (5.6%) | |
| Worry | 125 (11%) | 502 (44.2%) | 446 (39.3%) | 62 (5.5%) | |
| Sadness | 287 (25.3%) | 384 (33.8%) | 353 (31.1%) | 111 (9.8%) | |
| Anger | 434 (38.2%) | 280 (24.7%) | 292 (25.7%) | 129 (11.4%) | |
| Powerlessness | 292 (25.7%) | 312 (27.5%) | 352 (31%) | 179 (15.8%) | |
| Distress | 440 (38.8%) | 377 (33.2%) | 254 (22.4%) | 64 (5.6%) | |
| Aggression | 804 (70.8%) | 232 (20.4%) | 77 (6.8%) | 22 (1.9%) | |
| Shame | 907 (79.9%) | 154 (13.6%) | 67 (5.9%) | 7 (0.6%) | |
| Disbelief | 518 (45.6%) | 329 (29%) | 197 (17.4%) | 91 (8%) | |
| Isolation | 383 (33.7%) | 381 (33.6%) | 284 (25%) | 89 (7.8%) | |
| Never | Sometimes | Often | Always | ||
| Q31: Please indicate how often each of the following problems have bothered you in the past two weeks (Spitzer et al., 2006) [9] | Feeling more nervous anxious tense than usual | 262 (23.1%) | 648 (57.1%) | 163 (14.4%) | 62 (5.5%) |
| Not being able to stop worrying or keep worries under control | 438 (38.6%) | 501 (44.1%) | 154 (13.6%) | 42 (3.7%) | |
| Worrying too much about various things | 339 (29.9%) | 516 (45.5%) | 214 (18.9%) | 66 (5.8%) | |
| Having trouble relaxing and sleeping well | 394 (34.7%) | 484 (42.6%) | 190 (16.7%) | 68 (6.0%) | |
| Difficulty concentrating | 472 (41.6%) | 470 (41.4%) | 144 (12.7%) | 49 (4.3%) | |
| I find it difficult to make decisions | 579 (51.0%) | 392 (34.5%) | 126 (11.1%) | 38 (3.3%) | |
| Difficulty enjoying daily activities | 395 (34.8%) | 431 (38.0%) | 221 (19.5%) | 89 (7.8%) | |
| Tired out | 292 (25.7%) | 487 (42.9%) | 263 (23.2%) | 93 (8.2%) | |
| Getting scared easily | 650 (57.3%) | 350 (30.8%) | 96 (8.5%) | 37 (3.3%) | |
| Feeling unhappy | 482 (42.5%) | 451 (39.7%) | 148 (13.0%) | 54 (4.8%) | |
| Trouble thinking straight | 692 (61%) | 339 (29.9%) | 79 (7.0%) | 24 (2.1%) | |
| Being so restless that it is difficult to sit still | 787 (69.3%) | 241 (21.2%) | 86 (7.6%) | 22 (1.9%) | |
| Easily annoyed or irritated | 450 (39.6%) | 482 (42.5%) | 148 (13.0%) | 56 (4.9%) | |
| Being afraid that something terrible might happen | 499 (44.0%) | 442 (38.9%) | 136 (12.0%) | 59 (5.2%) | |
| Q32: What worries you the most? Choose 2 most relevant responses. | Not knowing when the emergency will end | 644 (56.7%) | |||
| Possibility of sickness of a family member | 701 (61.8%) | ||||
| Reduced economic availability | 205 (18.1%) | ||||
| Possibility of losing the future, planning | 299 (26.3%) | ||||
| Possibility of getting sick | 256 (22.6%) | ||||
| Q33: Do you feel safe visiting your dentist? | No | 111 (9.8%) | |||
| Somewhat | 512 (45.1%) | ||||
| Very | 471 (41.5%) | ||||
| Don’t know | 41 (3.6%) | ||||
| Q34: At the dentist’s office you go to, are the staff tested for COVID-19? | Yes | 295 (26%) | |||
| No | 1 (0,09%) | ||||
| I don’t know | 789 (69.5%) | ||||
| Never | 50 (4.4%) | ||||
| Q35: What type of instrument does your hygienist use during the COVID-19 pandemic? (Manual or mechanic) | Manual | 268 (23.6%) | |||
| Mechanic | 217 (19.1%) | ||||
| Both, but mostly mechanic | 256 (22.6%) | ||||
| Both, but mostly manual | 240 (21.2%) | ||||
| Q36: Knowing that in this pandemic situation in which social distancing is fundamental it is also essential to wear very personal protective equipment that covers almost the entire body and face, communication with your dentist/hygienist is: | Easy | 831 (73.2%) | |||
| Complicated | 235 (20.7%) | ||||
| Q37: Which of these additional treatments would you like to be able to use during this period? | Telemedicine | 264 (23.3%) | |||
| Telephone consultation | 186 (16.4%) | ||||
| Home hygiene instructions video | 277 (24.4%) | ||||
| I don’t know | 407 (35.9%) | ||||
| Q38: Do you know anyone who has contracted the coronavirus? | Nobody | 143 (12.6%) | |||
| Myself | 48 (4.2%) | ||||
| Family members | 151 (13.3%) | ||||
| Friends | 793 (69.9%) | ||||
| Variable | Estimate | Std. Error | z-Value | p-Value |
|---|---|---|---|---|
| Intercept | −0.574 | 0.328 | −1.751 | 0.080 |
| Age | −0.010 | 0.007 | −1.426 | 0.154 |
| Male gender | −0.320 | 0.178 | −1.796 | 0.072 |
| Center of Italy | 0.203 | 0.220 | 0.925 | 0.355 |
| South of Italy | 0.643 | 0.248 | 2.587 | 0.010 |
| Having children | 0.353 | 0.187 | 1.888 | 0.059 |
| Being positive to COVID-19 in the past | 0.712 | 0.346 | 2.057 | 0.040 |
| Model characteristics | AIC: 900.28 | |||
| McFadden’s R2 = 0.019 | ||||
| Variable | Estimate | Std. Error | z-Value | p-Value |
|---|---|---|---|---|
| Intercept | −0.395 | 0.349 | −1.133 | 0.257 |
| Age | −0.019 | 0.006 | −3.030 | 0.002 |
| Center of Italy | 0.535 | 0.214 | 2.503 | 0.012 |
| South of Italy | 0.620 | 0.243 | 2.555 | 0.011 |
| Live with family | 0.595 | 0.205 | 2.903 | 0.004 |
| Model characteristics | AIC: 935.16 | |||
| McFadden’s R2 = 0.031 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nardi, G.M.; Grassi, R.; Grassi, F.R.; Di Giorgio, R.; Guerra, F.; Ottolenghi, L.; Acito, G.; Basari, N.; Bisegna, S.; Chiavistelli, L.; et al. How Did the COVID-19 Pandemic Effect Dental Patients? An Italian Observational Survey Study. Healthcare 2021, 9, 1748. https://doi.org/10.3390/healthcare9121748
Nardi GM, Grassi R, Grassi FR, Di Giorgio R, Guerra F, Ottolenghi L, Acito G, Basari N, Bisegna S, Chiavistelli L, et al. How Did the COVID-19 Pandemic Effect Dental Patients? An Italian Observational Survey Study. Healthcare. 2021; 9(12):1748. https://doi.org/10.3390/healthcare9121748
Chicago/Turabian StyleNardi, Gianna Maria, Roberta Grassi, Felice Roberto Grassi, Roberto Di Giorgio, Fabrizio Guerra, Livia Ottolenghi, Giovanna Acito, Nasrin Basari, Simone Bisegna, Lorella Chiavistelli, and et al. 2021. "How Did the COVID-19 Pandemic Effect Dental Patients? An Italian Observational Survey Study" Healthcare 9, no. 12: 1748. https://doi.org/10.3390/healthcare9121748
APA StyleNardi, G. M., Grassi, R., Grassi, F. R., Di Giorgio, R., Guerra, F., Ottolenghi, L., Acito, G., Basari, N., Bisegna, S., Chiavistelli, L., Cimarossa, R., Colavito, A., Figlia, L., Gabrielli, C., Sabatini, S., Jedliński, M., & Mazur, M. (2021). How Did the COVID-19 Pandemic Effect Dental Patients? An Italian Observational Survey Study. Healthcare, 9(12), 1748. https://doi.org/10.3390/healthcare9121748