
Mortality, Severity, and Hospital Admission among COVID-19 Patients with ACEI/ARB Use: A Meta-Analysis Stratifying Countries Based on Response to the First Wave of the Pandemic





Abstract
:1. Background
2. Methods
2.1. Literature Search and Data Extraction
2.2. Data Synthesis and Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| NPIs | Non-pharmaceutical interventions |
| COVID-19 | Novel coronavirus |
| Rt | Reproduction number |
| t | Time |
| k | estimate |
| ACEIs | Angiotensin-converting enzyme inhibitors |
| ARBs | Angiotensin-receptor blockers |
| ACE2 | Angiotensin-converting enzyme-2 |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| OR | Odds ratio |
| ORp | Pooled odds ratio |
| CI | Confidence Interval |
| NOS | Newcastle–Ottawa Scale |
| ICU | Intensive care unit |
References
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W.; et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature 2020, 584, 257–261. [Google Scholar] [CrossRef]
- Giesecke, J. The invisible pandemic. Lancet 2020, 395, e98. [Google Scholar] [CrossRef]
- Ramachandran, R. COVID-19-a very visible pandemic. Lancet 2020, 396, e13–e14. [Google Scholar] [CrossRef]
- Chaudhry, R.; Dreanitsaris, G.; Mubashir, T.; Bartoszko, J.; Riazi, S. A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes. EClinicalMedicine 2020, 25, 100464. [Google Scholar] [CrossRef]
- Fang, L.; Karakiulakis, G.; Roth, M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir. Med. 2020, 8, e21. [Google Scholar] [CrossRef]
- Feng, Y.; Ling, Y.; Bai, T.; Xie, Y.; Huang, J.; Li, J.; Xiong, W.; Yang, D.; Chen, R.; Lu, F.; et al. COVID-19 with Different Severities: A Multicenter Study of Clinical Features. Am. J. Respir. Crit. Care Med. 2020, 201, 1380–1388. [Google Scholar] [CrossRef]
- Rico-Mesa, J.S.; White, A.; Anderson, A.S. Outcomes in Patients with COVID-19 Infection Taking ACEI/ARB. Curr. Cardiol. Rep. 2020, 22, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Yu, J.; Pan, L.Y.; Jiang, H.Y. ACEI/ARB use and risk of infection or severity or mortality of COVID-19: A systematic review and meta-analysis. Pharmacol. Res. 2020, 158, 104927. [Google Scholar] [CrossRef]
- Kansagara, D.; Mackey, K.; Vela, K. Update Alert: Risks and Impact of Angiotensin-Converting Enzyme Inhibitors or Angiotensin-Receptor Blockers on SARS-CoV-2 Infection in Adults. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Mackey, K.; King, V.J.; Gurley, S.; Kiefer, M.; Liederbauer, E.; Vela, K.; Sonnen, P.; Kansagara, D. Risks and Impact of Angiotensin-Converting Enzyme Inhibitors or Angiotensin-Receptor Blockers on SARS-CoV-2 Infection in Adults. Ann. Intern. Med. 2020, 173, 195–203. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Heal. Serv. Res. 2014, 14, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- China NHCotPsRo. Diagnosis and Treatment Protocol for COVID-19 Patients, 8th ed.; China NHCotPsRo: Beijing, China, 2020.
- World Health Organization. Clinical Management of COVID-19; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Metlay, J.P.; Waterer, G.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef] [PubMed]
- Ashby, D. Practical Statistics for Medical Research. In Statistics in Medicine; Douglas, G., Ed.; Altman, Chapman and Hall: London, UK, 1991; p. 611. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Cochrane Statistical Methods Group: Cardiff, UK, 2019; pp. 241–284. [Google Scholar]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Évid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Wells, G. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analysis. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 August 2020).
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Worldodometer Coronavirus. Available online: https://www.worldometers.info/coronavirus/country/uk/ (accessed on 15 September 2020).
- Bean, D.M.; Kraljevic, Z.; Searle, T.; Bendayan, R.; Kevin, O.G.; Pickles, A.; Folarin, A.; Roguski, L.; Noor, K.; Dobson, R.J.; et al. ACE-inhibitors and Angiotensin-2 Receptor Blockers are not associated with severe SARS-COVID19 infection in a multi-site UK acute Hospital Trust. Eur. J. Heart Fail. 2020, 22, 967–974. [Google Scholar] [CrossRef]
- Governor Cuomo Issues Guidance on Essential Services Under The ’New York State on PAUSE’ Executive Order. 2020. Available online: https://www.governor.ny.gov/news/governor-cuomo-issues-guidance-essential-services-under-new-york-state-pause-executive-order (accessed on 1 August 2020).
- Chinazzi, M.; Davis, J.T.; Ajelli, M.; Gioannini, C.; Litvinova, M.; Merler, S.; Piontti, A.P.Y.; Mu, K.; Rossi, L.; Sun, K.; et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 2020, 368, 395–400. [Google Scholar] [CrossRef] [Green Version]
- Oh, J.; Lee, J.K.; Schwarz, D.; Ratcliffe, H.L.; Markuns, J.F.; Hirschhorn, L.R. National Response to COVID-19 in the Republic of Korea and Lessons Learned for Other Countries. Heal. Syst. Reform 2020, 6, e1753464. [Google Scholar] [CrossRef]
- Lippi, G.; Lavie, C.J.; Henry, B.M.; Sanchis-Gomar, F. Do genetic polymorphisms in angiotensin converting enzyme 2 (ACE2) gene play a role in coronavirus disease 2019 (COVID-19)? Clin. Chem. Lab Med. 2020, 58, 1415–1422. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Young, D.; Coupland, C.; Channon, K.M.; Tan, P.S.; Harrison, D.; Rowan, K.; Aveyard, P.; Pavord, I.D.; Watkinson, P. Risk of severe COVID-19 disease with ACE inhibitors and angiotensin receptor blockers: Cohort study including 8.3 million people. Heart 2020, 106, 1503–1511. [Google Scholar] [CrossRef]
- Martini, M.; Gazzaniga, V.; Bragazzi, N.L.; Barberis, I. The Spanish Influenza Pandemic: A lesson from history 100 years after 1918. J. Prev. Med. Hyg. 2019, 60, E64–E67. [Google Scholar] [CrossRef] [PubMed]
- Grubaugh, N.D.; Hanage, W.P.; Rasmussen, A.L. Making Sense of Mutation: What D614G Means for the COVID-19 Pandemic Remains Unclear. Cell 2020, 182, 794–795. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.Y.; Brown, S.T.; Cooley, P.; Grefenstette, J.J.; Zimmerman, R.K.; Zimmer, S.M.; Potter, A.M.; Rosenfeld, R.; Wheaton, D.W.; Wiringa, A.E.; et al. Vaccination deep into a pandemic wave potential mechanisms for a “third wave” and the impact of vaccination. Am. J. Prev. Med. 2010, 39, e21–e29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, J.P.; Klasse, P.J. COVID-19 Vaccines: “Warp Speed” Needs Mind Melds, Not Warped Minds. J. Virol. 2020, 94, e01083-20. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome/Source | Studies 2 | ORp [95% CI] 3 | I2 (if k ≥ 2) |
|---|---|---|---|
| Mortality | |||
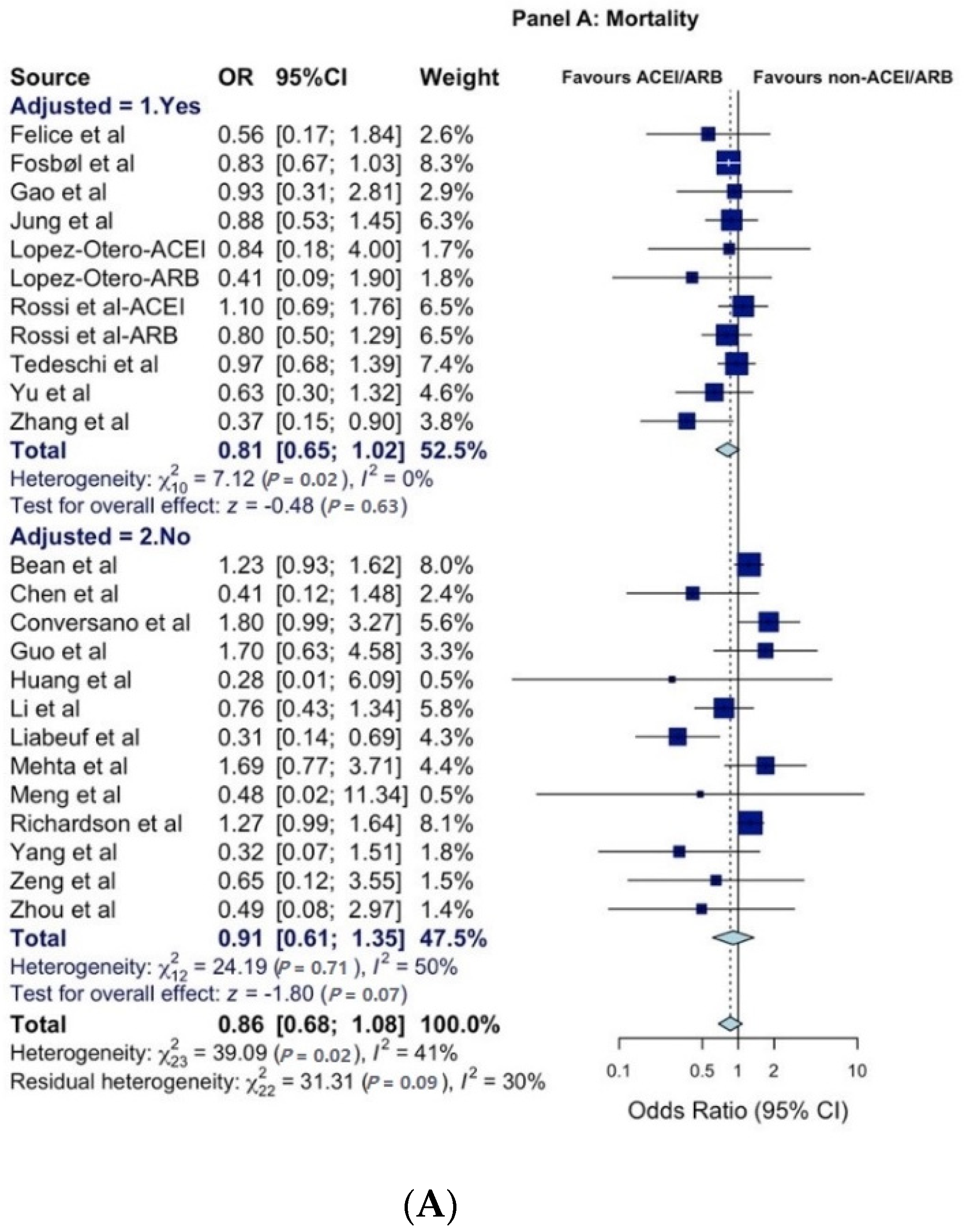
| All reports 4 | 24 | 0.86 [0.68; 1.08] | 41% |
| Adjusted | 11 | 0.81 [0.65; 1.02] | 0% |
| Unadjusted 5 | 13 | 0.91 [0.61; 1.35] | 50% |
| By country/cluster | |||
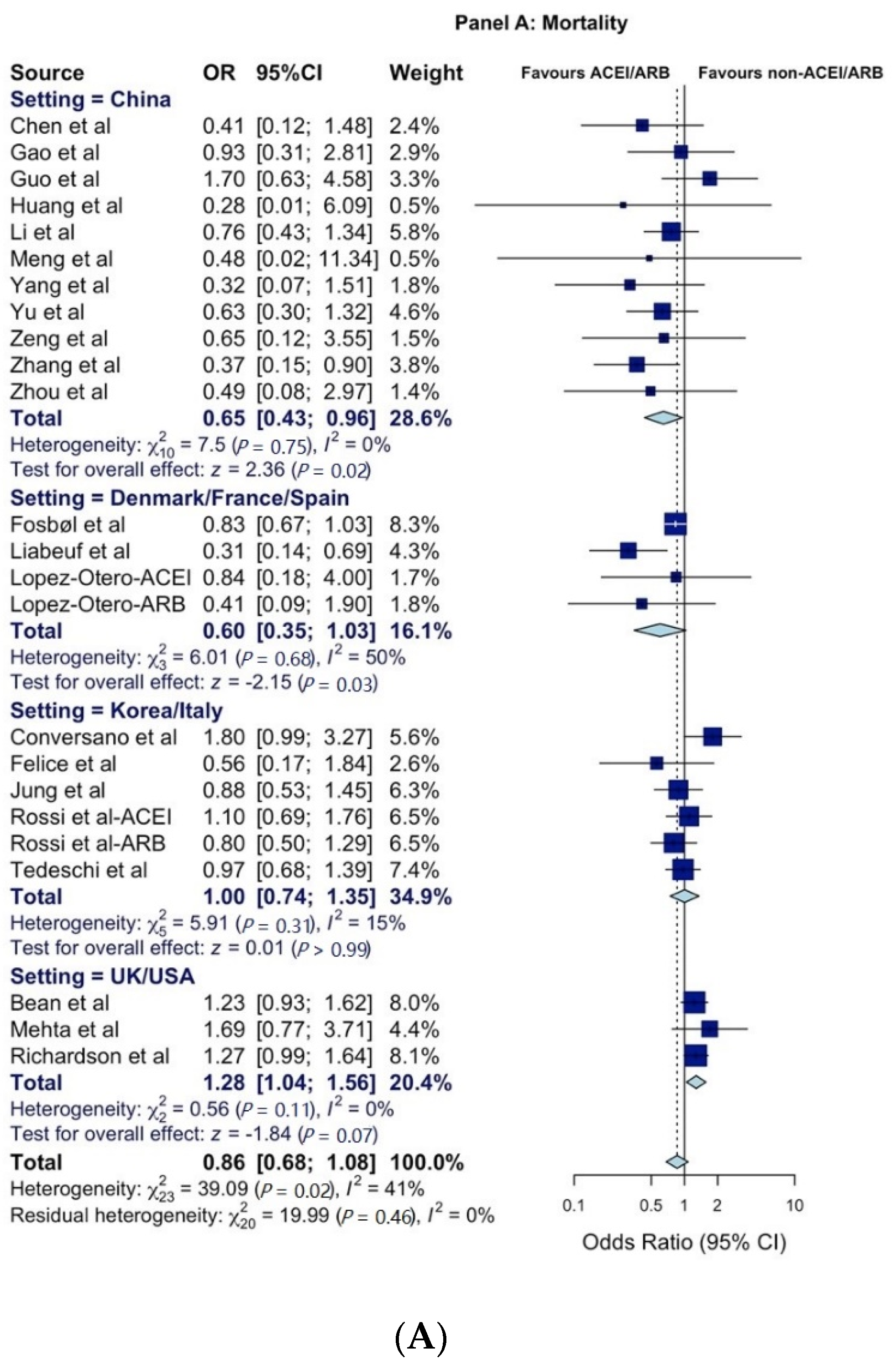
| China | 11 | 0.65 [0.43; 0.96] | 0% |
| Korea | 1 | 0.88 [0.53; 1.45] | - |
| Italy | 5 | 1.03 [0.71; 1.46] | 29% |
| Denmark | 1 | 0.83 [0.67; 1.03] | - |
| France | 1 | 0.31 [0.14; 0.69] | - |
| Spain | 2 | 0.58 [0.19; 1.81] | 0% |
| UK | 1 | 1.23 [0.93; 1.62] | - |
| US | 2 | 1.32 [0.99; 1.75] | 0% |
| Korea/Italy | 6 | 1.00 [0.74; 1.36] | 15% |
| Denmark/France/Spain | 4 | 0.60 [0.35; 1.03] | 50% |
| UK/US | 3 | 1.28 [1.04; 1.56] | 0% |
| Severity | |||
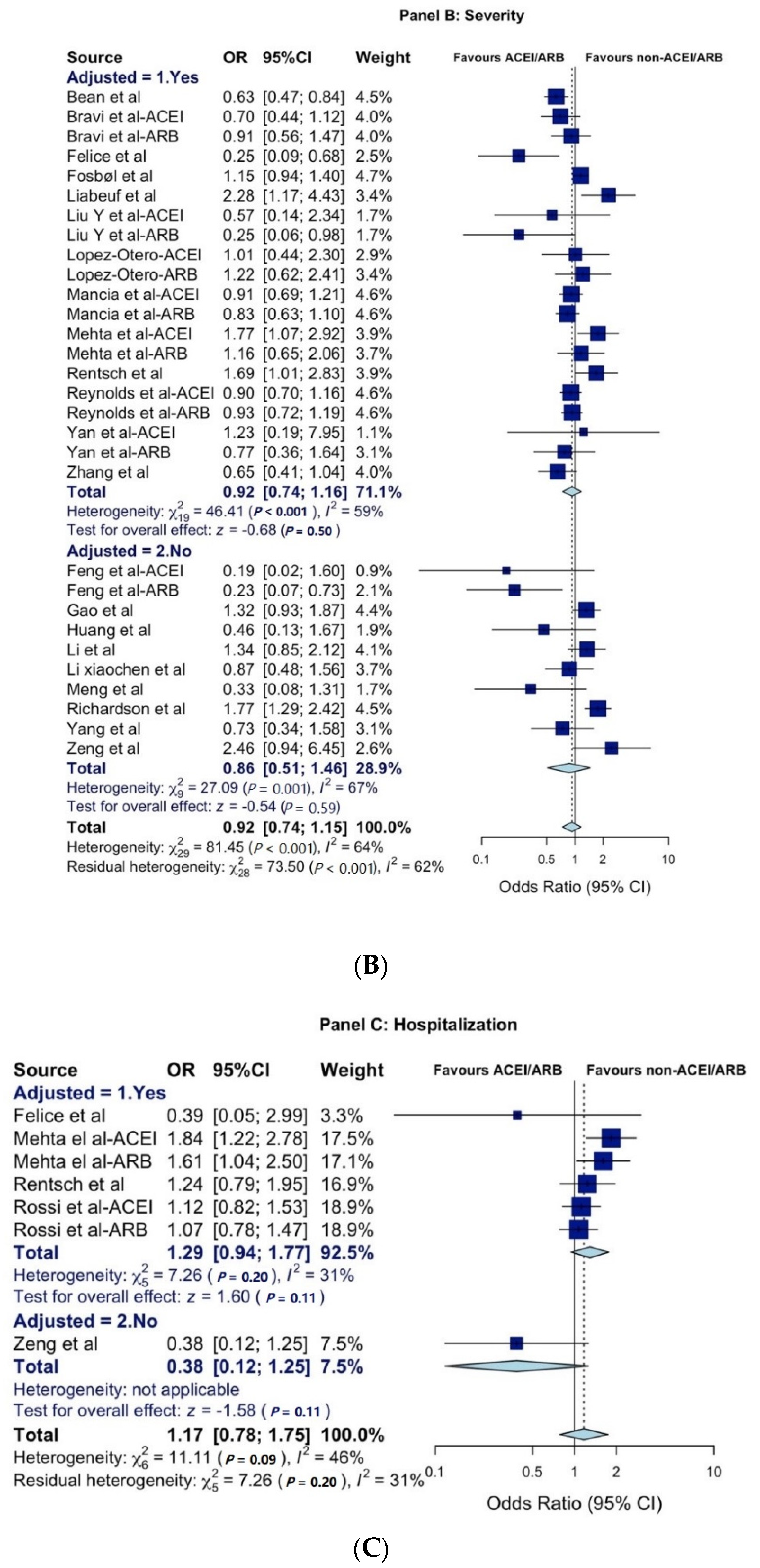
| All reports 4 | 30 | 0.92 [0.74; 1.15] | 64% |
| Adjusted | 20 | 0.92 [0.74; 1.16] | 59% |
| Unadjusted 5 | 10 | 0.90 [0.61; 1.33] | 67% |
| By country/cluster | |||
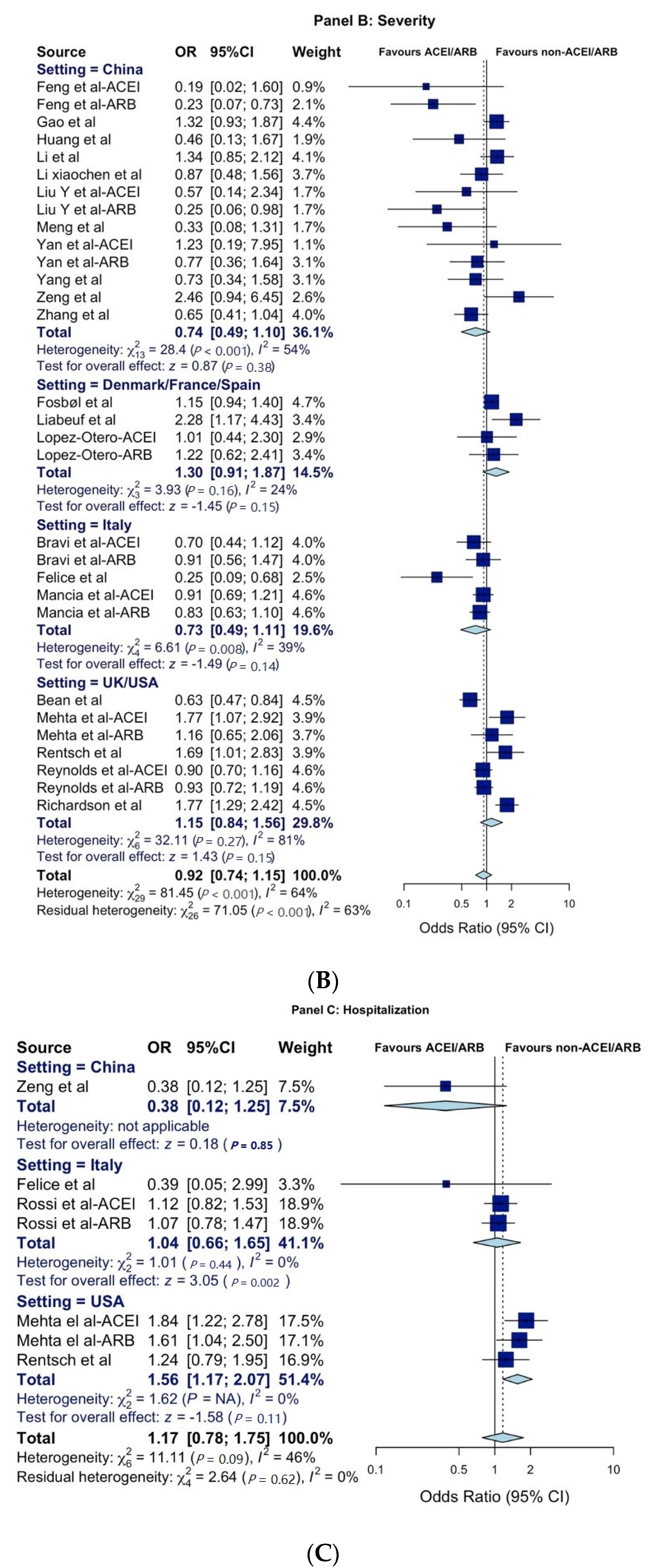
| China | 14 | 0.74 [0.50; 1.10] | 54% |
| Italy | 5 | 0.74 [0.49; 1.11] | 40% |
| Denmark | 1 | 1.15 [0.94; 1.40] | - |
| France | 1 | 2.28 [1.17; 4.43] | - |
| Spain | 2 | 1.13 [0.67; 1.91] | 0% |
| UK | 1 | 0.63 [0.47; 0.84] | - |
| US | 6 | 1.27 [0.96; 1.66] | 73% |
| Denmark/France/Spain | 4 | 1.30 [0.91; 1.87] | 24% |
| UK/US | 7 | 1.15 [0.84; 1.56] | 81% |
| Hospitalization | |||
| All reports 4 | 7 | 1.17 [0.78; 1.75] | 46% |
| Adjusted | 6 | 1.29 [0.94; 1.77] | 31% |
| Unadjusted 5 | 1 | 0.38 [0.12; 2.91] | - |
| By country | |||
| China | 1 | 0.38 [0.12; 1.25] | - |
| Italy | 3 | 1.04 [0.66; 1.65] | 0% |
| US | 3 | 1.56 [1.17; 2.07] | 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alamer, A.A.; Almulhim, A.S.; Alrashed, A.A.; Abraham, I. Mortality, Severity, and Hospital Admission among COVID-19 Patients with ACEI/ARB Use: A Meta-Analysis Stratifying Countries Based on Response to the First Wave of the Pandemic. Healthcare 2021, 9, 127. https://doi.org/10.3390/healthcare9020127
Alamer AA, Almulhim AS, Alrashed AA, Abraham I. Mortality, Severity, and Hospital Admission among COVID-19 Patients with ACEI/ARB Use: A Meta-Analysis Stratifying Countries Based on Response to the First Wave of the Pandemic. Healthcare. 2021; 9(2):127. https://doi.org/10.3390/healthcare9020127
Chicago/Turabian StyleAlamer, Ahmad A., Abdulaziz S. Almulhim, Ahmed A. Alrashed, and Ivo Abraham. 2021. "Mortality, Severity, and Hospital Admission among COVID-19 Patients with ACEI/ARB Use: A Meta-Analysis Stratifying Countries Based on Response to the First Wave of the Pandemic" Healthcare 9, no. 2: 127. https://doi.org/10.3390/healthcare9020127
APA StyleAlamer, A. A., Almulhim, A. S., Alrashed, A. A., & Abraham, I. (2021). Mortality, Severity, and Hospital Admission among COVID-19 Patients with ACEI/ARB Use: A Meta-Analysis Stratifying Countries Based on Response to the First Wave of the Pandemic. Healthcare, 9(2), 127. https://doi.org/10.3390/healthcare9020127