
Age Estimation Using the Cameriere Methods of Open Apices: A Meta-Analysis




Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection Criteria
2.2. Search Method
2.3. Data Collection and Analysis
2.4. Quality Assessment and Risk of Bias
2.5. Statistical Analysis
3. Results
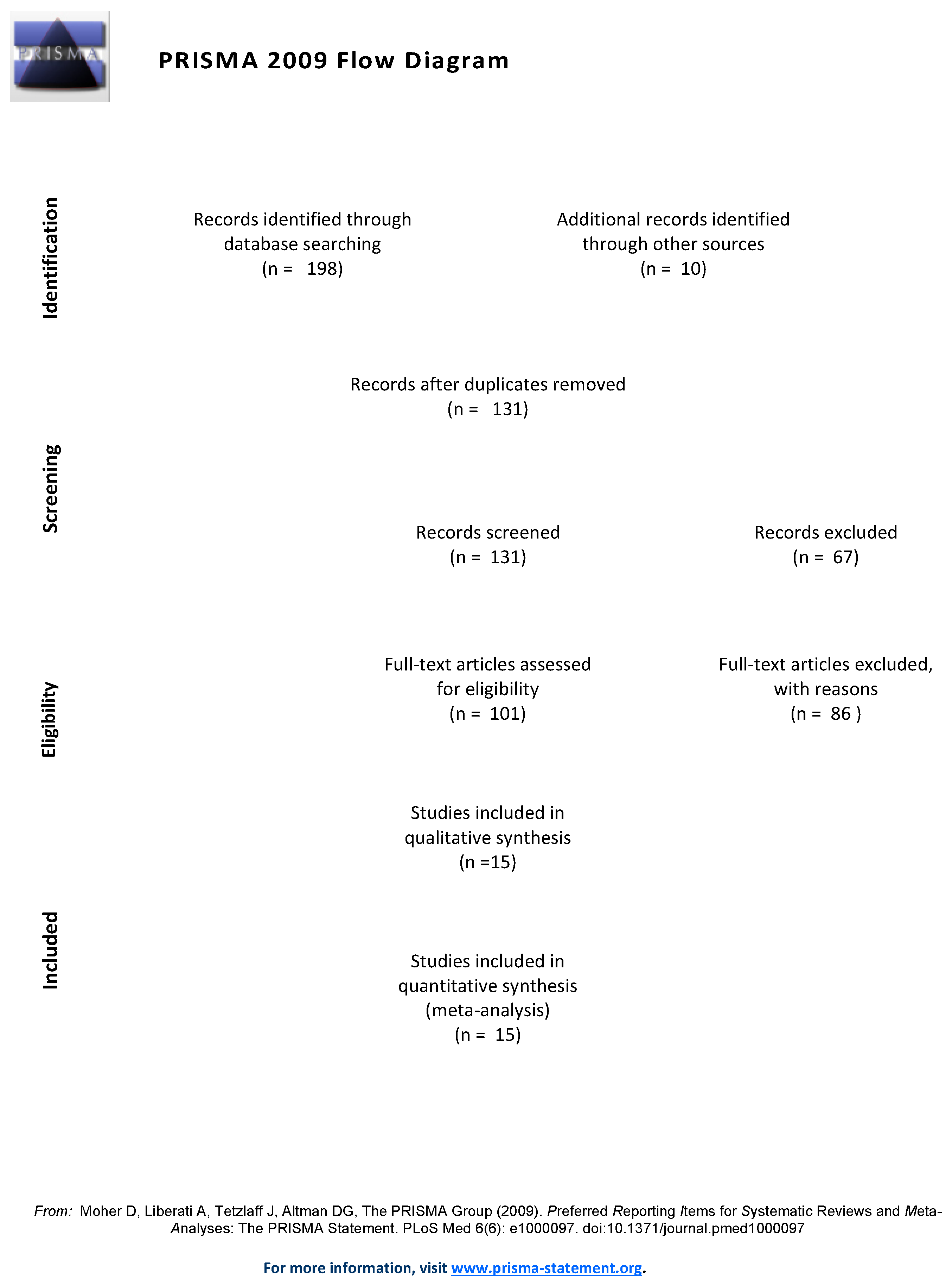
3.1. Search Synthesis
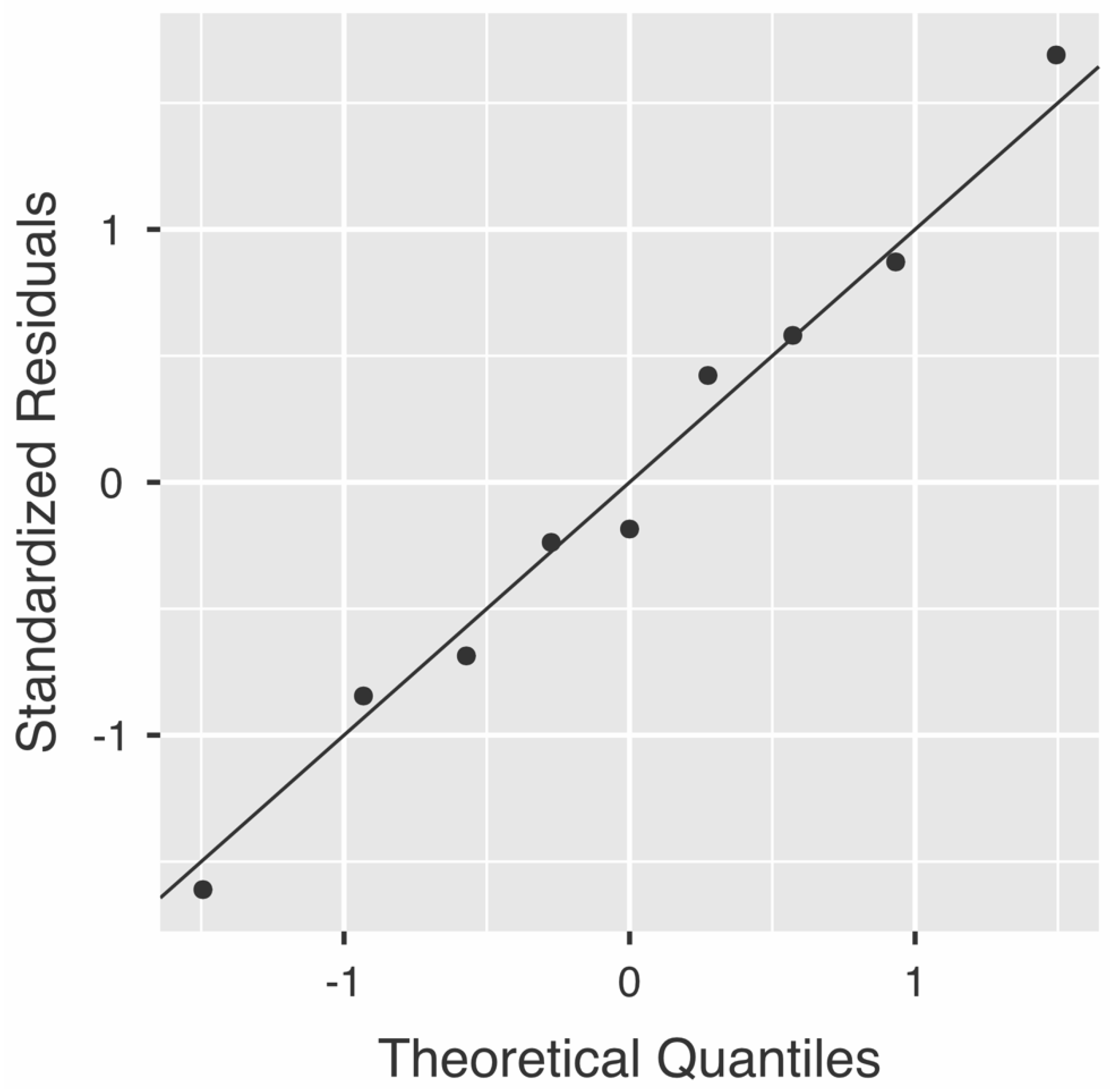
3.2. Quality Assessment and Risk of Bias
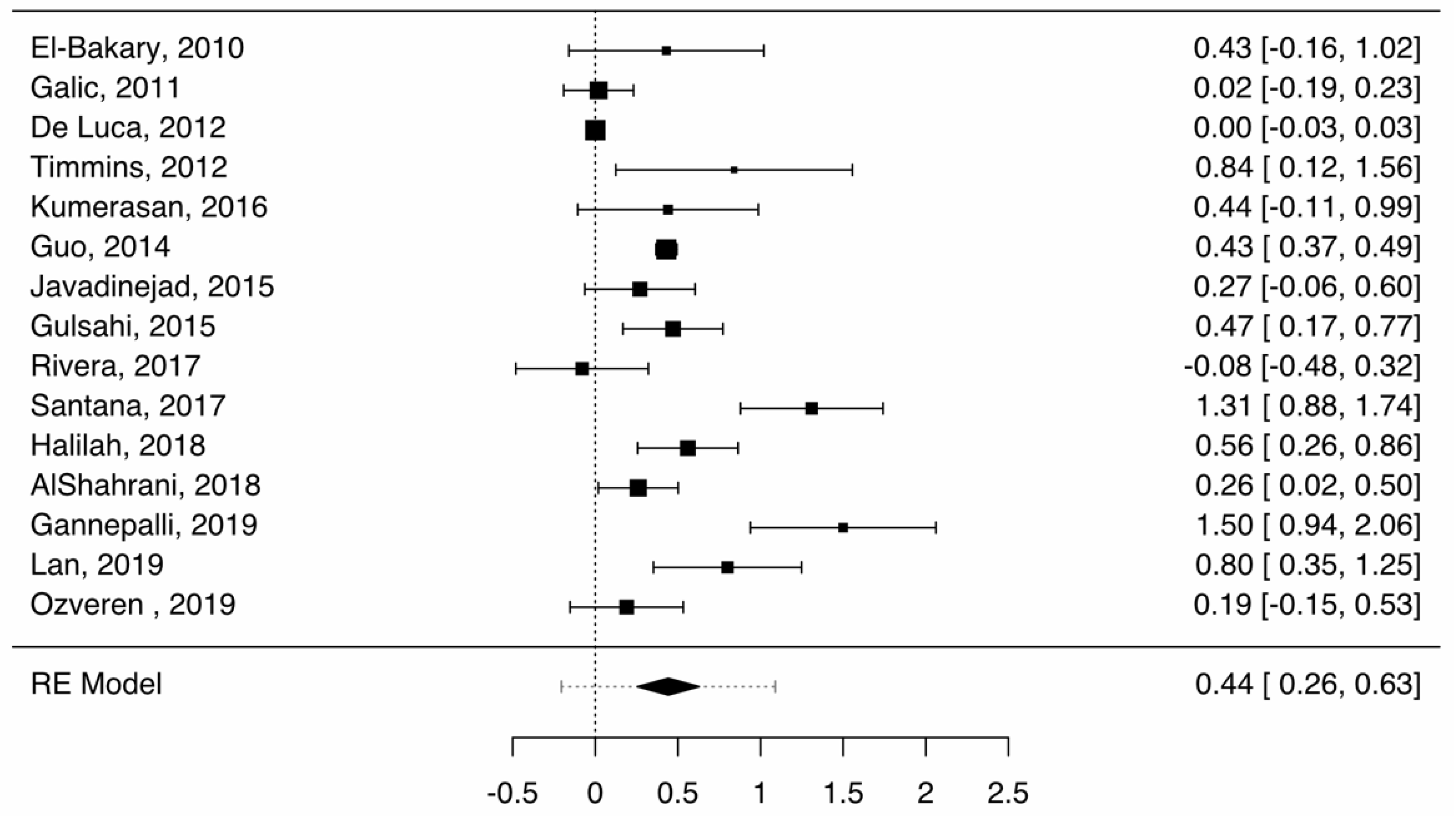
3.3. Accuracy of Cameriere Formulas Depending on Gender
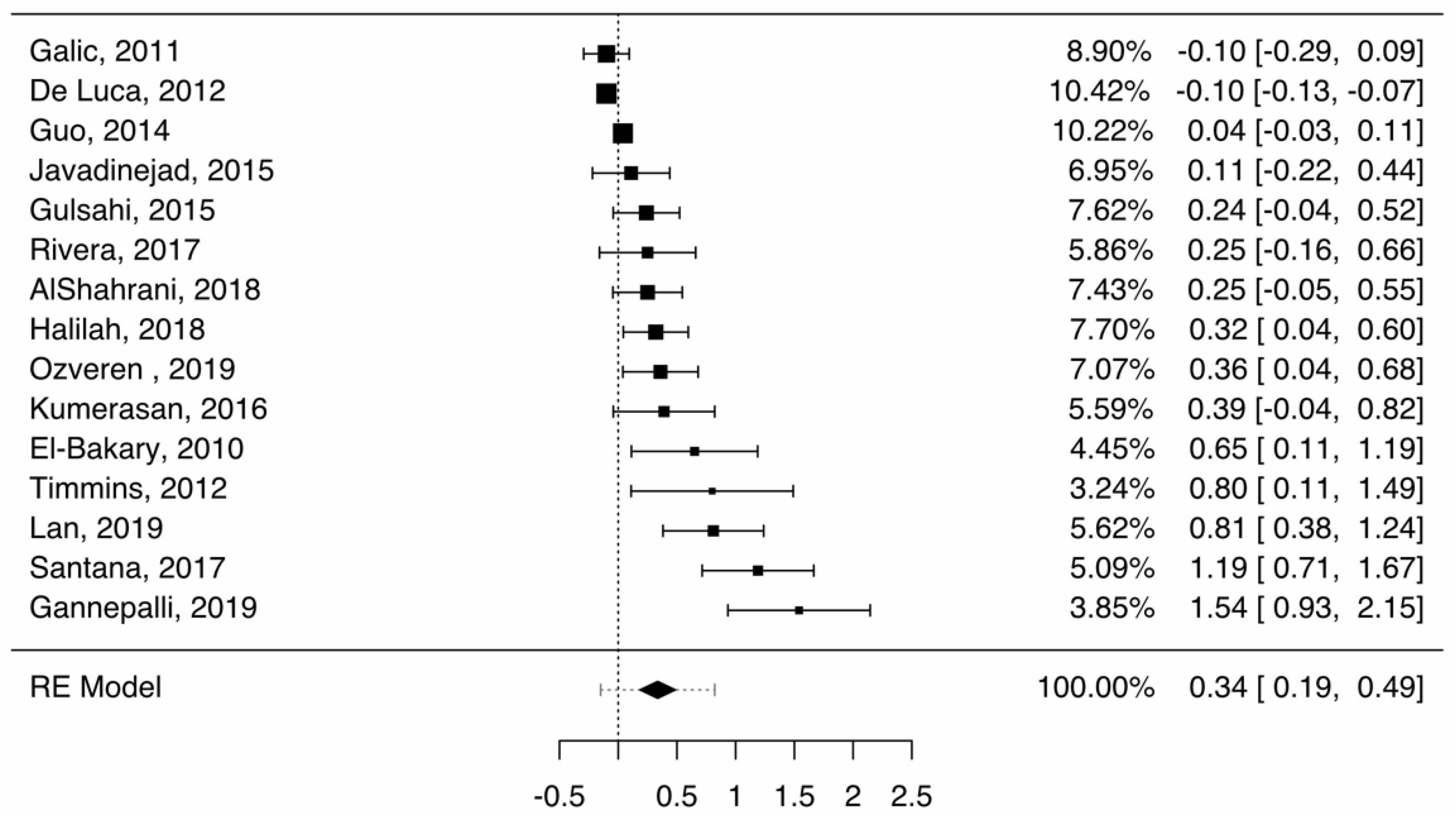
3.4. Accuracy of Cameriere Formulas in Age Groups
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cavrić, J.; Galić, I.; Vodanović, M.; Brkić, H.; Gregov, J.; Viva, S.; Rey, L.; Cameriere, R. Third molar maturity index (I3M) for assessing age of majority in a black African population in Botswana. Int. J. Leg. Med. 2016, 130, 1109–1120. [Google Scholar] [CrossRef]
- Cameriere, R.; Pacifici, A.; Viva, S.; Carbone, D.; Pacifici, L.; Polimeni, A. Adult or not? Accuracy of Cameriere’s cut-off value for third molar in assessing 18 years of age for legal purposes. Minerva Stomatol. 2014, 63, 283–294. [Google Scholar] [PubMed]
- Hostiuc, S.; Teodoru, D.; Isailă, O. Tratat de Medicină Legală Odontostomatologică; Hostiuc, S., Ed.; All: București, Romania, 2020. [Google Scholar]
- Sharma, P.; Wadhwan, V.; Prakash, R.; Goel, S.; Aggarwal, P. Age estimation in children by measurement of open apices in teeth: A study in North Indian population. Aust. J. Forensic Sci. 2016, 48, 592–600. [Google Scholar] [CrossRef]
- Franklin, D.; Karkhanis, S.; Flavel, A.; Collini, F.; DeLuca, S.; Cameriere, R. Accuracy of a cut-off value based on the third molar index: Validation in an Australian population. Forensic Sci. Int. 2016, 266, 575.e1–575.e6. [Google Scholar] [CrossRef]
- Cameriere, R.; Pacifici, A.; Polimeni, L.; Federici, F.; Cingolani, M.; Ferrante, L. Age estimation in children by measurement of open apices in teeth with Bayesian calibration approach. Forensic Sci. Int. 2016, 258, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Cameriere, R.; Ferrante, L.; Cingolani, M. Age estimation in children by measurement of open apices in teeth. Int. J. Leg. Med. 2006, 120, 49–52. [Google Scholar] [CrossRef] [Green Version]
- Cameriere, R.; De Angelis, D.; Ferrante, L.; Scarpino, F.; Cingolani, M. Age estimation in children by measurement of open apices in teeth: A European formula. Int. J. Leg. Med. 2007, 121, 449–453. [Google Scholar] [CrossRef] [Green Version]
- Balla, S.B.; Lingam, S.; Kotra, A.; Hima, R.P.; Karuna, P.; Madhuri, N.N.; Cameriere, R. New regression models for dental age estimation in children using third molar maturity index: A preliminary analysis testing its usefulness as reliable age marker. Leg. Med. 2019, 39, 35–40. [Google Scholar] [CrossRef]
- Pratyusha, K.; Prasad, M.G.; Radhakrishna, A.N.; Saujanya, K.; Raviteja, N.V.K.; Chandrasekhar, S. Applicability of Demirjian’s Method and Modified Cameriere’s Methods for Dental Age Assessment in Children. J. Clin. Diagn. Res. 2017, 11, ZC40–ZC43. [Google Scholar] [CrossRef] [PubMed]
- Santana, S.A.; Bethard, J.D.; Moore, T.L. Accuracy of Dental Age in Nonadults: A Comparison of Two Methods for Age Estimation Using Radiographs of Developing Teeth. J. Forensic Sci. 2017, 62, 1320–1325. [Google Scholar] [CrossRef] [Green Version]
- Rai, B.; Kaur, J.; Cingolani, M.; Ferrante, L.; Cameriere, R. Age estimation in children by measurement of open apices in teeth: An Indian formula. Int. J. Leg. Med. 2010, 124, 237–241. [Google Scholar] [CrossRef] [Green Version]
- De Luca, S.; Alemán, I.; Bertoldi, F.; Ferrante, L.; Mastrangelo, P.; Cingolani, M.; Cameriere, R. Age estimation by tooth/pulp ratio in canines by peri-apical X-rays: Reliability in age determination of Spanish and Italian medieval skeletal remains. J. Archaeol. Sci. 2010, 37, 3048–3058. [Google Scholar] [CrossRef] [Green Version]
- Lauc, T.; Nakaš, E.; Latić-Dautović, M.; Džemidžić, V.; Tiro, A.; Rupić, I.; Kostić, M.; Galić, I. Dental Age in Orthodontic Patients with Different Skeletal Patterns. BioMed Res. Int. 2017, 2017, 1–7. [Google Scholar] [CrossRef] [PubMed]
- De Luca, S.; Bautista, J.; Alemán, I.; Cameriere, R. Age-at-Death Estimation by Pulp/Tooth Area Ratio in Canines: Study of a 20th-Century Mexican Sample of Prisoners to Test Cameriere’s Method. J. Forensic Sci. 2011, 56, 1302–1309. [Google Scholar] [CrossRef]
- Angelakopoulos, N.; De Luca, S.; Palacio, L.A.V.; Coccia, E.; Ferrante, L.; Pinchi, V.; Cameriere, R. Age estimation by measuring open apices in teeth: A new formula for two samples of South African black and white children. Int. J. Leg. Med. 2019, 133, 1529–1536. [Google Scholar] [CrossRef]
- Javadinejad, S.; Sekhavati, H.; Ghafari, R. A Comparison of the Accuracy of Four Age Estimation Methods Based on Panoramic Radiography of Developing Teeth. J. Dent. Res. Dent. Clin. Dent. Prospect. 2015, 9, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Cugati, N.; Kumaresan, R.; Srinivasan, B.; Karthikeyan, P. Dental age estimation of growing children by measurement of open apices: A Malaysian formula. J. Forensic Dent. Sci. 2015, 7, 227–231. [Google Scholar] [CrossRef] [Green Version]
- De Luca, S.; de Giorgio, S.; Butti, A.C.; Biagi, R.; Cingolani, M.; Cameriere, R. Age estimation in children by measurement of open apices in tooth roots: Study of a Mexican sample. Forensic Sci. Int. 2012, 221, 155.e1–155.e7. [Google Scholar] [CrossRef]
- Rivera, M.; De Luca, S.; Aguilar, L.; Palacio, L.A.V.; Galić, I.; Cameriere, R. Measurement of open apices in tooth roots in Colombian children as a tool for human identification in asylum and criminal proceedings. J. Forensic Leg. Med. 2017, 48, 9–14. [Google Scholar] [CrossRef]
- Ozveren, N.; Serindere, G. Comparison of the applicability of Demirjian and Willems methods for dental age estimation in children from the Thrace region, Turkey. Forensic Sci. Int. 2018, 285, 38–43. [Google Scholar] [CrossRef]
- Moher, D.; Altman, D.G.; Liberati, A.; Tetzlaff, J. PRISMA Statement. Epidemiology 2011, 22, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, F.T.S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeks, J.; Higgins, J.; Altman, D. Chapter 10: Analysing Data and Undertaking Meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions, 6th ed.; Higgins, J., Thomas, J., Eds.; John Wiley and Sons: Chicester, UK, 2019; pp. 241–284. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Bakary, A.A.; Hammad, S.M.; Mohammed, F. Dental age estimation in Egyptian children, comparison between two methods. J. Forensic Leg. Med. 2010, 17, 363–367. [Google Scholar] [CrossRef]
- Galić, I.; Vodanović, M.; Cameriere, R.; Nakaš, E.; Galić, E.; Selimović, E.; Brkić, H. Accuracy of Cameriere, Haavikko, and Willems radiographic methods on age estimation on Bosnian–Herzegovian children age groups 6–13. Int. J. Leg. Med. 2011, 125, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Timmins, K.; Liversidge, H.; Farella, M.; Herbison, P.; Kieser, J. The usefulness of dental and cervical maturation stages in New Zealand children for Disaster Victim Identification. Forensic Sci. Med. Pathol. 2011, 8, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.-C.; Yan, C.-X.; Lin, X.-W.; Zhou, H.; Li, J.-P.; Pan, F.; Zhang, Z.-Y.; Wei, L.; Tang, Z.; Chen, T. Age estimation in northern Chinese children by measurement of open apices in tooth roots. Int. J. Leg. Med. 2014, 129, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Gulsahi, A.; Tirali, R.E.; Cehreli, S.B.; De Luca, S.; Ferrante, L.; Cameriere, R. The reliability of Cameriere’s method in Turkish children: A preliminary report. Forensic Sci. Int. 2015, 249, 319.e1–319.e5. [Google Scholar] [CrossRef]
- Kumaresan, R.; Cugati, N.; Chandrasekaran, B.; Karthikeyan, P. Reliability and validity of five radiographic dental-age estimation methods in a population of Malaysian children. J. Investig. Clin. Dent. 2014, 7, 102–109. [Google Scholar] [CrossRef]
- Halilah, T.; Khdairi, N.; Jost-Brinkmann, P.-G.; Bartzela, T. Age estimation in 5–16-year-old children by measurement of open apices: North German formula. Forensic Sci. Int. 2018, 293, 103.e1–103.e8. [Google Scholar] [CrossRef]
- Alshahrani, I.; Yassin, S.M.; Togoo, R.A.; Tikare, S.; Khader, M.A.; Alkahtani, Z.M. Age estimation by measurement of open apices in tooth roots: Study using Saudi Arabian samples. J. Forensic Leg. Med. 2019, 62, 63–68. [Google Scholar] [CrossRef]
- Gannepalli, A.; Balla, S.B.; Pacha, V.B.; Babu, D.B.G.; Vinay, B.H.; Perkari, S. Applicability of Cameriere European formula for age estimation of 10–15 years legal threshold in South Indian population. J. Forensic Dent. Sci. 2019, 11, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Lan, L.M.; Yang, Z.D.; Sun, S.L.; Wen, D.; Kureshi, A.; Zeye, M.M.J.; Zha, L.; Li, M. Application of Demirjian’s and Cameriere’s Method in Dental Age Estimation of 8–16 Year Old Adolescents from Hunan Han Nationality. J. Forensic Med. 2019, 35, 406–410. [Google Scholar]
- Ozveren, N.; Serindere, G.; Meric, P.; Cameriere, R. A comparison of the accuracy of Willems’ and Cameriere’s methods based on panoramic radiography. Forensic Sci. Int. 2019, 302, 109912. [Google Scholar] [CrossRef] [PubMed]
- Cameriere, R.; Ferrante, L.; Liversidge, H.; Prieto, J.; Brkic, H. Accuracy of age estimation in children using radiograph of developing teeth. Forensic Sci. Int. 2008, 176, 173–177. [Google Scholar] [CrossRef]
- Wolf, T.G.; Briseño-Marroquín, B.; Callaway, A.; Patyna, M.; Müller, V.T.; Willershausen, I.; Ehlers, V.; Willershausen, B. Dental age assessment in 6- to 14-year old German children: Comparison of Cameriere and Demirjian methods. BMC Oral Health 2016, 16, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apaydin, B.K.; Yasar, F. Accuracy of the demirjian, willems and cameriere methods of estimating dental age on turkish children. Niger. J. Clin. Pract. 2018, 21, 257–263. [Google Scholar]
- De Micco, F.; Martino, F.; Campobasso, C.P. Ethical issues in age assessment by the third molar development. Aust. J. Forensic Sci. 2020, 1–12. [Google Scholar] [CrossRef]
- Malmqvist, E.; Furberg, E.; Sandman, L. Ethical aspects of medical age assessment in the asylum process: A Swedish perspective. Int. J. Leg. Med. 2018, 132, 815–823. [Google Scholar] [CrossRef] [Green Version]
- Kangaude, G.D.; Skelton, A. (De)Criminalizing Adolescent Sex: A Rights-Based Assessment of Age of Consent Laws in Eastern and Southern Africa. SAGE Open 2018, 8, 215824401880603. [Google Scholar] [CrossRef] [Green Version]
- Focardi, M.; Pinchi, V.; De Luca, F.; Norelli, G.-A. Age estimation for forensic purposes in Italy: Ethical issues. Int. J. Leg. Med. 2014, 128, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Rudolf, E. Comments to Focardi et al., Age estimation for forensic purposes in Italy: Ethical issues. Int. J. Leg. Med. 2014, 129, 1271–1273. [Google Scholar] [CrossRef] [PubMed]
- Dalessandri, D.; Tonni, I.; Laffranchi, L.; Migliorati, M.; Isola, G.; Visconti, L.; Bonetti, S.; Paganelli, C. 2D vs. 3D Radiological Methods for Dental Age Determination around 18 Years: A Systematic Review. Appl. Sci. 2020, 10, 3094. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Prediction intervals. In Introduction to Meta-Analysis; Borenstein, M., Ed.; John Wiley & Sons: Chichester, UK, 2009; pp. 127–133. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Age Range | Country | No. Subjects | Inclusion Criteria | Exclusion Criteria | Quality Score |
|---|---|---|---|---|---|---|
| El-Bakary, 2010 [27] | 5–16 | Egypt | 286 | Age range, good quality radiographs, no agenesis or extractions in the left lower quadrant | Hypodontia, hyperdontia | 13.5 |
| Galic, 2011 [28] | 6–14 | Serbia, Croatia, Bosnia | 498 | Born after 2000 | Systemic disease, premature birth, congenital anomalies, hypodontia of permanent teeth except third molar | 17.75 |
| De Luca, 2012 [19] | 5–15 | Mexico | 248 | Good quality radiographs, no agenesis or extractions in the left lower quadrant. | Incomplete dental or medical history, evident systemic diseases and congenital anomalies, premature birth, hypodontia of permanent teeth except third molars and hyperdontia. | 19.5 |
| Timmins, 2012 [29] | 7–17 | New Zeeland | 200 | Healthy children | 14 | |
| Guo, 2014 [30] | 5–15 | China | 229 | Northern Chinese, healthy, no medical pathologies affecting tooth development | 18 | |
| Javadinejad, 2015 [17] | 3–15 | Iran | 537 | Absence of systemic diseases, dental anomalies, nutritional and endocrine problems, premature birth, birth defects, clear birth date and date of radiography | 12 | |
| Gulsahi, 2015 [31] | 8–15 | Turkey | 573 | Good quality radiographs, healthy subjects with known and precise age, no systemic diseases, normal teeth eruption, no pathological conditions associated with the alveolar jaw | Systemic diseases, congenital anomalies, dental anomalies, premature birth, obesity, patients undergoing orthodontic treatments, extraction in the lower left quadrant, | 18.25 |
| Kumaresan, 2016 [32] | 5–16 | Malaysia | 426 | Malaysian for at least two generations | Radiographs of poor quality, genetic or congenital anomalies, history of orthodontic treatment | 18 |
| Rivera, 2017 [20] | 6–14 | Colombia | 457 | Patients seeking orthodontic treatment, excellent quality of the ortopanthogram, good general and dental health | Unknown date of birth or date of ortopanthogram, agenesys, hypodontia, missing tooth on the left inside, dental anomalies | 16.25 |
| Santana, 2017 [11] | 7–17 | Mexico | 360 | Hypodontia, hyperdontia, systemic diseases, congenital abnormalities, evidence of extraction, unclear radiographs | 16.5 | |
| Halilah,2018 [33] | 5–16 | Germany | 800 | Good quality radiographs, children growing up in north Germany, caucasians | Aplasia of at least two corresponding teeth bilaterally in the mandible, extraction in the lower left quadrant, systemic diseases, congenital and genetic anomalies, radiographs with all apices closed | 20 |
| AlShahrani, 2018 [34] | 6–16 | Saudi Arabia | 788 | Saudi nationality, complete case records | Incomplete medical or dental history, documented tooth extractions or agenesis especially in left lower quadrant, distorted radiographs, radiographic evidence of periapical lesions, fractured teeth and internal tooth resorption, evidence of systemic diseases, congenital anomalies, premature birth, hypodontia of permanent teeth except third molars and hypertonia | 14.75 |
| Gannepalli, 2019 [35] | 10–15 | India | 100 | inadequate quality for assessment, signs of gross pathology, hypodontia, and previous history of orthodontic treatment were | 19 | |
| Lan, 2019 [36] | 8–16 | China | 480 | Good Rx, no history of drug use or surgery, unaffected teeth, the presence of left mandibular permanent teeth | Maxillofacial malformation, located in Hunan province, no cysts or tumors affecting the development of teeth | 18.5 |
| Ozveren, 2019 [37] | 6–15 | Turkey | 636 | Systemic diseases, previous restorative, endodontic, orthodontic treatment history, dental trauma history, dental anomalies, missing lower teeth (except the third molar), jaw bone pathologies such as cysts or tumors were | 19.25 | |
| Age Group | Mean Difference, CI (95%) | I2% | Publication Bias Z | Publication Bias p | References |
|---|---|---|---|---|---|
| 6–7 | −0.38 (−0.56–−0.21) | 67.45 | 2.599 | 0.009 | [19,20,33,37] |
| 7–8 | −0.09 (−0.21–0.04) | 43.53 | 1.969 | 0.049 | [19,20,33,37] |
| 8–9 | 0.14 (−0.01–0.29) | 62.76 | −0.908 | 0.364 | [19,20,31,33,36,37] |
| 9–10 | −0.03 (−0.26–0.20) | 85.74 | 0.136 | 0.892 | [19,20,31,33,36,37] |
| 10–11 | 0.16 (0.01–0.32) | 81.36 | 0.850 | 0.395 | [19,20,31,33,36,37] |
| 11–12 | 0.39 (0.18–0.60) | 83.7 | 0.111 | 0.912 | [19,20,31,33,36,37] |
| 12–13 | 0.45 (0.08–0.82) | 94.91 | 0.109 | 0.913 | [19,20,31,33,36,37] |
| 13–14 | 0.56 (0.24–0.89) | 94.19 | 0.276 | 0.783 | [19,20,31,33,36,37] |
| 14–15 | 0.87 (0.65–1.09) | 86.28 | −0.826 | 0.409 | [19,20,31,33,36,37] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hostiuc, S.; Diaconescu, I.; Rusu, M.C.; Negoi, I. Age Estimation Using the Cameriere Methods of Open Apices: A Meta-Analysis. Healthcare 2021, 9, 237. https://doi.org/10.3390/healthcare9020237
Hostiuc S, Diaconescu I, Rusu MC, Negoi I. Age Estimation Using the Cameriere Methods of Open Apices: A Meta-Analysis. Healthcare. 2021; 9(2):237. https://doi.org/10.3390/healthcare9020237
Chicago/Turabian StyleHostiuc, Sorin, Ioana Diaconescu, Mugurel Constantin Rusu, and Ionut Negoi. 2021. "Age Estimation Using the Cameriere Methods of Open Apices: A Meta-Analysis" Healthcare 9, no. 2: 237. https://doi.org/10.3390/healthcare9020237
APA StyleHostiuc, S., Diaconescu, I., Rusu, M. C., & Negoi, I. (2021). Age Estimation Using the Cameriere Methods of Open Apices: A Meta-Analysis. Healthcare, 9(2), 237. https://doi.org/10.3390/healthcare9020237