
Part I: Relationship among Training Load Management, Salivary Immunoglobulin A, and Upper Respiratory Tract Infection in Team Sport: A Systematic Review

 ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Screening Strategy and Study Selection
2.3. Methodological Assessment
3. Results
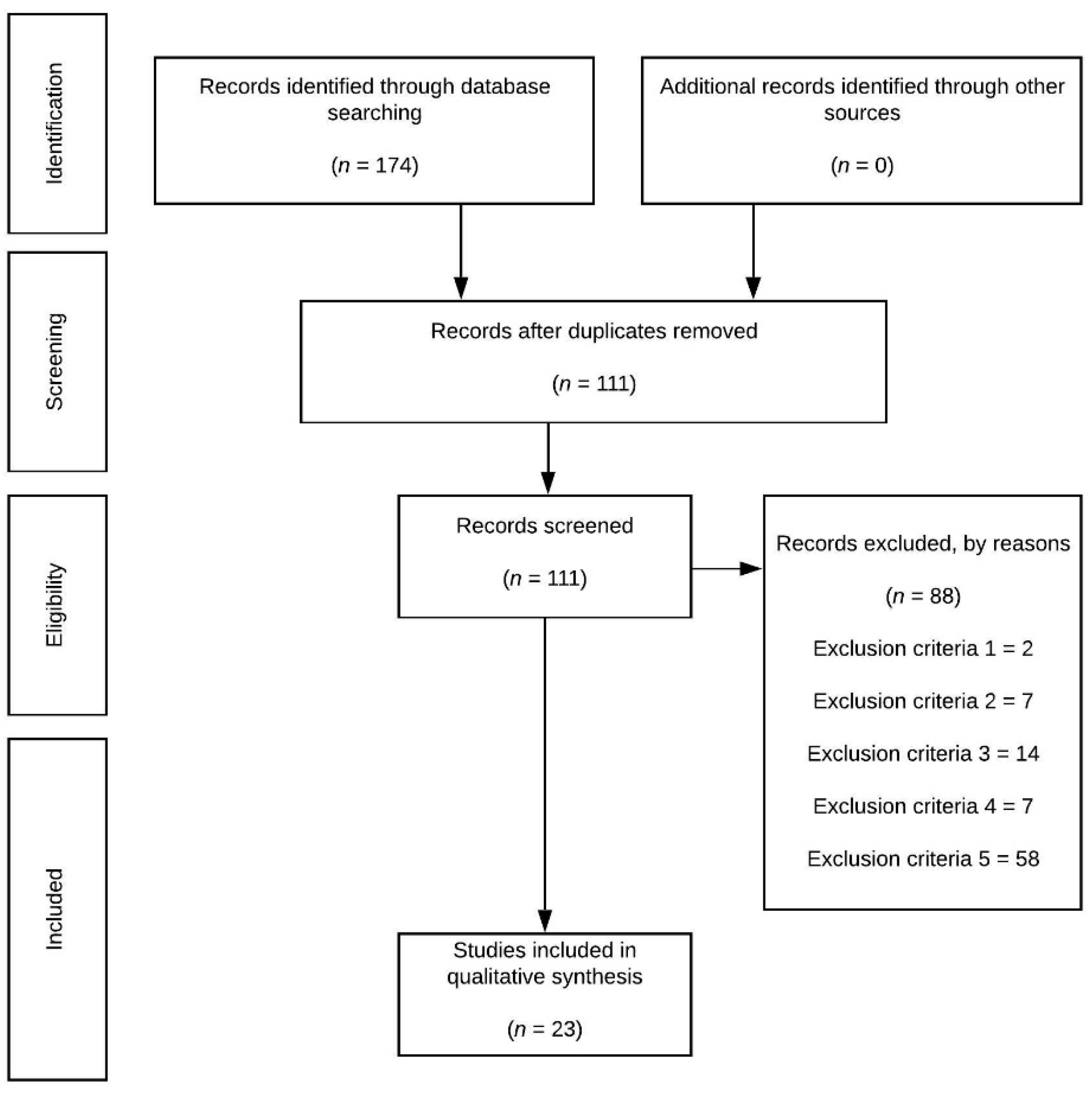
3.1. Identification and Selection of Studies
3.2. Methodological Quality
3.3. Study Characteristics
4. Discussion
4.1. IgA Outcomes
4.1.1. Official Matches
4.1.2. Training Matches
4.1.3. Official and Training Matches
4.1.4. General Training and Training with Strength/Resistance
4.1.5. Training and Official Matches
4.2. Relationship between Salivary IgA and URTI
4.3. Relationship between Salivary IgA and Training Load
4.4. Study Limits and Future Directions
5. Conclusions
Strength of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Ahmadi, S.; Brietzke, C.; Silveira, R. Aspects of Physical Training Related with Upper Respiratory Tract Infections: A Review. Man. Ther. Posturology Rehabil. J. 2018, 8. [Google Scholar] [CrossRef] [Green Version]
- Gleeson, M. Immune Function in Sport and Exercise. Immune Funct. Sport Exerc. 2007, 103, 7. [Google Scholar] [CrossRef] [Green Version]
- Nieman, D.C. Risk of Upper Respiratory Tract Infection in Athletes: An Epidemiologic and Immunologic Perspective. J. Athl. Train 1997, 32, 344–349. [Google Scholar] [PubMed]
- Keaney, L.C.; Kilding, A.E.; Merien, F.; Dulson, D.K. The Impact of Sport Related Stressors on Immunity and Illness Risk in Team-Sport Athletes. J. Sci. Med. Sport 2018, 21, 1192–1199. [Google Scholar] [CrossRef] [PubMed]
- Lamm, M.E. Interaction of antigens and antibodies at mucosal surfaces. Annu. Rev. Microbiol. 1997, 51, 311–340. [Google Scholar] [CrossRef]
- Lamm, M.E.; Nedrud, J.G.; Kaetzel, C.S.; Mazanec, M.B. IgA and Mucosal Defense. APMIS 1995, 103, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Underdown, B.J. Immunoglobulin A: Strategic Defense Initiative at the Mucosal Surface. APMIS 1986, 103, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Neville, V.; Gleeson, M.; Folland, J.P. Salivary IgA as a Risk Factor for Upper Respiratory Infections in Elite Professional Athletes. Med. Sci. Sports Exerc. 2008, 40, 1228–1236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blume, K.; Körber, N.; Hoffmann, D.; Wolfarth, B. Training Load, Immune Status, and Clinical Outcomes in Young Athletes: A Controlled, Prospective, Longitudinal Study. Front. Physiol. 2018, 9, 120. [Google Scholar] [CrossRef]
- Tiernan, C.; Lyons, M.; Comyns, T.; Nevill, A.M.; Warrington, G. Salivary IgA as a Predictor of Upper Respiratory Tract Infections and Relationship to Training Load in Elite Rugby Union Players. J. Strength Cond. Res. 2020, 34, 782–790. [Google Scholar] [CrossRef] [Green Version]
- Lindsay, A.; Lewis, J.; Scarrott, C.; Draper, N.; Gieseg, S.P. Changes in Acute Biochemical Markers of Inflammatory and Structural Stress in Rugby Union. J. Sports Sci. 2015, 33, 882–891. [Google Scholar] [CrossRef]
- Maya, J.; Marquez, P.; Peñailillo, L.; Contreras-Ferrat, A.; Deldicque, L.; Zbinden-Foncea, H. Salivary Biomarker Responses to Two Final Matches in Women’s Professional Football. J. Sports Sci. Med. 2016, 15, 365–371. [Google Scholar]
- Moreira, A.; Bacurau, R.F.P.; Napimoga, M.H.; Arruda, A.F.S.; Freitas, C.G.; Drago, G.; Aoki, M.S. Salivary il-21 and iga responses to a competitive match in elite basketball players. Biol. Sport 2013, 30, 243–247. [Google Scholar] [CrossRef] [Green Version]
- Freitas, C.G.; Aoki, M.S.; Arruda, A.F.S.; Franciscon, C.; Moreira, A. Monitoring Salivary Immunoglobulin A Responses to Official and Simulated Matches In Elite Young Soccer Players. J. Hum. Kinet. 2016, 53, 107–115. [Google Scholar] [CrossRef] [Green Version]
- Moreira, A.; Arsati, F.; de Oliveira Lima-Arsati, Y.B.; de Freitas, C.G.; de Araujo, V.C. Salivary Immunoglobulin a Responses in Professional Top-Level Futsal Players. J. Strength Cond. Res. 2011, 25, 1932–1936. [Google Scholar] [CrossRef] [PubMed]
- Peñailillo, L.; Maya, L.; Niño, G.; Torres, H.; Zbinden-Foncea, H. Salivary Hormones and IgA in Relation to Physical Performance in Football. J. Sports Sci. 2015, 33, 2080–2087. [Google Scholar] [CrossRef] [PubMed]
- Rico-González, M.; Pino-Ortega, J.; Ardigò, L.P. Playing Non-Professional Football in COVID-19 Time: A Narrative Review of Recommendations, Considerations, and Best Practices. Int. J. Environ. Res. Public Health 2021, 18, 568. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Reilly, M.; Caulfield, B.; Ward, T.; Johnston, W.; Doherty, C. Wearable Inertial Sensor Systems for Lower Limb Exercise Detection and Evaluation: A Systematic Review. Sports Med. 2018, 48, 1221–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindsay, A.; Lewis, J.; Scarrott, C.; Gill, N.; Gieseg, S.; Draper, N. Assessing the Effectiveness of Selected Biomarkers in the Acute and Cumulative Physiological Stress Response in Professional Rugby Union through Non-Invasive Assessment. Int. J. Sports Med. 2015, 36, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Mariscal, G.; Vera, P.; Platero, J.L.; Bodí, F.; de la Rubia Ortí, J.E.; Barrios, C. Changes in Different Salivary Biomarkers Related to Physiologic Stress in Elite Handball Players: The Case of Females. Sci. Rep. 2019, 9, 19554. [Google Scholar] [CrossRef] [PubMed]
- Nunes, J.A.; Crewther, B.T.; Viveiros, L.; Jr, D.D.R.; Aoki, M.S. Effects of Resistance Training Periodization on Performance and Salivary Immune-Endocrine Responses of Elite Female Basketball Players. J. Sports Med. Phys. Fit. 2011, 51, 8. [Google Scholar]
- Milanez, V.F.; Ramos, S.P.; Okuno, N.M.; Boullosa, D.A. Evidence of a Non-Linear Dose-Response Relationship between Training Load and Stress Markers in Elite Female Futsal Players. J. Sports Sci. Med. 2014, 13, 9. [Google Scholar]
- Caetano Júnior, P.C.; Carvalho Aguiar, J.; Ferreira-Strixino, J.; José Raniero, L. Isokinetic Muscle Performance and Salivary Immune-Endocrine Responses in Handball Players by Fourier Transform Infrared Spectroscopy. Rev. Andal. De Med. Deporte 2017, 10, 125–131. [Google Scholar] [CrossRef] [Green Version]
- Moreira, A.; de Moura, N.R.; Coutts, A.; Costa, E.C.; Kempton, T.; Aoki, M.S. Monitoring Internal Training Load and Mucosal Immune Responses in Futsal Athletes. J. Strength Cond. Res. 2013, 27, 1253–1259. [Google Scholar] [CrossRef]
- Moreira, A.; Arsati, F.; de Oliveira Lima-Arsati, Y.B.; Simões, A.C.; de Araújo, V.C. Monitoring Stress Tolerance and Occurrences of Upper Respiratory Illness in Basketball Players by Means of Psychometric Tools and Salivary Biomarkers. Stress Health 2011, 27, e166–e172. [Google Scholar] [CrossRef]
- Nunes, J.A.; Moreira, A.; Crewther, B.T.; Nosaka, K.; Viveiros, L.; Aoki, M.S. Monitoring Training Load, Recovery-Stress State, Immune-Endocrine Responses, and Physical Performance in Elite Female Basketball Players During a Periodized Training Program. J. Strength Cond. Res. 2014, 28, 2973–2980. [Google Scholar] [CrossRef]
- Cunniffe, B.; Griffiths, H.; Proctor, W.; Davies, B.; Baker, J.S.; Jones, K.P. Mucosal Immunity and Illness Incidence in Elite Rugby Union Players across a Season. Med. Sci. Sports Exerc. 2011, 43, 388–397. [Google Scholar] [CrossRef]
- Orysiak, J.; Witek, K.; Zembron-Lacny, A.; Morawin, B.; Malczewska-Lenczowska, J.; Sitkowski, D. Mucosal Immunity and Upper Respiratory Tract Infections during a 24-Week Competitive Season in Young Ice Hockey Players. J. Sports Sci. 2017, 35, 1255–1263. [Google Scholar] [CrossRef] [PubMed]
- Coad, S.; Gray, B.; Wehbe, G.; McLellan, C. Physical Demands and Salivary Immunoglobulin A Responses of Elite Australian Rules Football Athletes to Match Play. Int. J. Sports Physiol. Perform. 2015, 10, 613–617. [Google Scholar] [CrossRef] [PubMed]
- He, C.-S.; Tsai, M.-L.; Ko, M.-H.; Chang, C.-K.; Fang, S.-H. Relationships among Salivary Immunoglobulin A, Lactoferrin and Cortisol in Basketball Players during a Basketball Season. Eur. J. Appl. Physiol. 2010, 110, 989–995. [Google Scholar] [CrossRef]
- de Arruda, A.F.S.; de Freitas, C.G.; de Moura, N.R.; Aoki, M.S.; Moreira, A. Resposta imuno-endócrina associada à partida de futsal. Mot. Rev. Educ. Fis. 2013, 19, 460–466. [Google Scholar] [CrossRef] [Green Version]
- Nunes, J.A.; Crewther, B.T.; Ugrinowitsch, C.; Tricoli, V.; Viveiros, L.; de Rose, D.; Aoki, M.S. Salivary Hormone and Immune Responses to Three Resistance Exercise Schemes in Elite Female Athletes. J. Strength Cond. Res. 2011, 25, 2322–2327. [Google Scholar] [CrossRef] [PubMed]
- Koch, A.J.; Wherry, A.D.; Petersen, M.C.; Johnson, J.C.; Stuart, M.K.; Sexton, W.L. Salivary immunoglobulin aresponse to a collegiate rugby game. J. Strength Cond. Res. 2007, 21, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Coad, S.; Gray, B.; McLellan, C. Seasonal Analysis of Mucosal Immunological Function and Physical Demands in Professional Australian Rules Footballers. Int. J. Sports Physiol. Perform. 2016, 11, 574–580. [Google Scholar] [CrossRef]
- Moreira, A.; Crewther, B.; Freitas, C.G.; Arruda, A.F.S.; Costa, E.C.; Aoki, M.S. Session RPE and Salivary Immune-Endocrine Responses to Simulated and Official Basketball Matches in Elite Young Male Athletes. J. Sports Med. Phys. Fit. 2012, 52, 7. [Google Scholar]
- Moreira, A.; Arsati, F.; Cury, P.R.; Franciscon, C.; Simões, A.C.; de Oliveira, P.R.; de Araújo, V.C. The Impact of a 17-Day Training Period for an International Championship on Mucosal Immune Parameters in Top-Level Basketball Players and Staff Members. Eur. J. Oral Sci. 2008, 116, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Orysiak, J.; Witek, K.; Malczewska-Lenczowska, J.; Zembron-Lacny, A.; Pokrywka, A.; Sitkowski, D. Upper Respiratory Tract Infection and Mucosal Immunity in Young Ice Hockey Players During the Pretournament Training Period. J. Strength Cond. Res. 2019, 33, 3129–3135. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, R.; Shimizu, K.; Kimura, F.; Takemura, M.; Suzuki, K.; Akama, T.; Kono, I.; Akimoto, T. Virus Activation and Immune Function during Intense Training in Rugby Football Players. Int. J. Sports Med. 2011, 32, 393–398. [Google Scholar] [CrossRef]
- Moraes, H.; Aoki, M.; Freitas, C.; Arruda, A.; Drago, G.; Moreira, A. SIgA Response and Incidence of Upper Respiratory Tract Infections during Intensified Training in Youth Basketball Players. Biol. Sport 2017, 1, 49–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortatti, A.L.; Moreira, A.; Aoki, M.S.; Crewther, B.T.; Castagna, C.; de Arruda, A.F.S.; Filho, J.M. Effect of Competition on Salivary Cortisol, Immunoglobulin A, and Upper Respiratory Tract Infections in Elite Young Soccer Players. J. Strength Cond. Res. 2012, 26, 1396–1401. [Google Scholar] [CrossRef]
- Nehlsen-Cannarella, S.L.; Nieman, D.C.; Fagoaga, O.R.; Kelln, W.J.; Henson, D.A.; Shannon, M.; Davis, J.M. Saliva Immunoglobulins in Elite Women Rowers. Eur. J. Appl. Physiol. 2000, 81, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.; Freitas, C.G.; Nakamura, F.Y.; Drago, G.; Drago, M.; Aoki, M.S. Effect of Match Importance on Salivary Cortisol and Immunoglobulin A Responses in Elite Young Volleyball Players. J. Strength Cond. Res. 2013, 27, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Teeuw, W.; Bosch, J.A.; Veerman, E.C.I.; Nieuw Amerongen, A.V. Neuroendocrine Regulation of Salivary IgA Synthesis and Secretion: Implications for Oral Health. Biol. Chem. 2004, 385, 1137–1146. [Google Scholar] [CrossRef]
- Hucklebridge, F.; Clow, A.; Evans, P. The Relationship between Salivary Secretory Immunoglobulin A and Cortisol: Neuroendocrine Response to Awakening and the Diurnal Cycle. Int. J. Psychophysiol. 1998, 31, 69–76. [Google Scholar] [CrossRef]
- Papacosta, E.; Nassis, G.P. Saliva as a Tool for Monitoring Steroid, Peptide and Immune Markers in Sport and Exercise Science. J. Sci. Med. Sport 2011, 14, 424–434. [Google Scholar] [CrossRef]
- Mazanec, M.; Nedrud, J.; Kaetzel, C.; Lamm, M. A Threetiered View of the Role of IgA in Mucosal Defense. Immunol Today 1993, 14, 430–435. [Google Scholar] [CrossRef]
- Gleeson, M.; Bishop, N.; Oliveira, M.; McCauley, T.; Tauler, P.; Muhamad, A.S. Respiratory Infection Risk in Athletes: Association with Antigen-Stimulated IL-10 Production and Salivary IgA Secretion: Biomarkers of Infection Risk in Athletes. Scand. J. Med. Sci. Sports 2012, 22, 410–417. [Google Scholar] [CrossRef]
- Bishop, N.C. Acute and Chronic Effects of Exercise on Markers of Mucosal Immunity. Front. Biosci. 2009, 4444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novas, A.M.; Rowbottom, D.G.; Jenkins, D.G. Tennis, Incidence of URTI and Salivary IgA. Int. J. Sports Med. 2003, 24, 223–229. [Google Scholar] [CrossRef]
- Moreira, A.; Mortatti, A.L.; Arruda, A.F.S.; Freitas, C.G.; de Arruda, M.; Aoki, M.S. Salivary IgA Response and Upper Respiratory Tract Infection Symptoms During a 21-Week Competitive Season in Young Soccer Players. J. Strength Cond. Res. 2014, 28, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Morgans, R.; Orme, P.; Anderson, L.; Drust, B.; Morton, J.P. An Intensive Winter Fixture Schedule Induces a Transient Fall in Salivary IgA in English Premier League Soccer Players. Res. Sports Med. 2014, 22, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Fahlman, M.M.; Engels, H.-J. Mucosal IgA and URTI in American College Football Players: A Year Longitudinal Study. Med. Sci. Sports Exerc. 2005, 37, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M. Immune Function and Exercise. Eur. J. Sport Sci. 2004, 4, 52–66. [Google Scholar] [CrossRef]


{kind=link}
| No. | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| 1 | Samples were taken from salivary test | Samples collected from non-salivary test (e.g., blood samples) |
| 2 | Biomarkers related to immunology (IgA) | Biomarkers related to hormones (testosterone, cortisol) or immunology (not IgA) |
| 3 | Articles in which the relationship between training load and IgA was assessed without other factors | Articles that assessed the influence of another factor (e.g., nutritional intervention, recovery strategies) in IgA response or the effects of IgA in other contexts (e.g., oral health) |
| 4 | Original articles | Nonoriginal research papers (i.e., systematic reviews, conferences, or meetings) |
| 5 | Articles developed with team sport athletes (rugby, basketball, futsal, Australian football, ice hockey, or handball) more than 18 years old. | Articles developed with soccer players or with non-team sport athletes |
| Reference | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lindsay et al. [20] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | Low |
| Lindsay et al. [11] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | High |
| Mariscal et al. [21] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | High |
| Nunes et al. [22] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | High |
| Milanez et al. [23] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | High |
| Caetano Júnior et al. [24] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | High |
| Moreira et al. [25] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | High |
| Moreira et al. [26] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | High |
| Nunes et al. [27] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | High |
| Cunniffe et al. [28] | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | Low |
| Orysiak et al. [29] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | High |
| Coad et al. [30] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | Low |
| He et al. [31] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | Low |
| Arruda et al. [32] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | High |
| Nunes et al. [33] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | High |
| Tiernan et al. [10] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | Low |
| Moreira et al. [13] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | High |
| Koch et al. [34] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | Low |
| Coad et al. [35] | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | High |
| Moreira et al. [36] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | High |
| Moreira et al. [37] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | High |
| Orysiak et al. [38] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | High |
| Yamauchi et al. [39] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | High |
| Ref. | Sample | Stressor | Immunoglobulin (IgA) | Study Limits | Lessons Learned and Concluding Remarks | ||||
|---|---|---|---|---|---|---|---|---|---|
| Test | Volume | Intensity | Salivary Test | Outcomes | IgA–URTI Relationship | ||||
| Official Matches | |||||||||
| Rugby | |||||||||
| Lindsay et al. [11] | 24 professional rugby players from New Zealand provincial team. | 3 professional rugby games. | Game 1 = 72.1 ± 15.4; Game 2 = 66.6 ± 17.0; Game 3 = 74.4 ± 18.4 min. | Game time, total distance covered (m), player load (au), and number of impacts were as follows: Game 1 = 5191, 544.7, 25; Game 2 = 5368, 565.2, 22; Game 3 = 5346, 585.2, 26. | Saliva samples were collected ~120 min pre-game and ~30–40 min post-game. | Post-game decrements (p < 0.001). sIgA decreases for game 2 (p = 0.019). Mean sIgA decreases following all games. | No. | Small sample size and only 3 games were analyzed. | Significant decreases in sIgA concentration and secretion were observed for game 2. Post-game secretion rate is affected by pre-game rate and number of impacts. |
| Koch et al. [34] | 16 men’s college rugby players. | 1 regulation rugby game. | 80 min. | Intensity of the match was not controlled. | Saliva samples were collected ~10 min before pre-match warm-up and within 5 min post-game. | No significant pre-post-game changes in sIgA were observed (−13%). | No. | No load quantification by athlete and fluid consumption during the game. | Strenuous physical activity, such as a competitive rugby game, does not affect sIgA. |
| Australian Football | |||||||||
| Coad et al. [35] | 18 elite male Australian Rules Football League athletes. | 16 consecutive matches. | 1 match per week (4 × 30 min quarters). | Player load range values from 1392.14 ± 139.46 to 1263.89 ± 180.69 AU. | sIgA was measured at 36 h post-match before daily activities. | Significant (p < 0.05) effects compared with pre-season baseline sIgA. After matches, a substantial suppression of sIgA was found compared with pre-season baseline. | No. | Small sample size. Only 36 h post-match periods were monitored, which can influence the results interpretation. | Matches may delay sIgA recovery beyond 36 h post-match for full recovery and may be at higher risk of illness during the initial 36 h post-match. |
| Basketball | |||||||||
| Moreira et al. [13] | 20 under-19 male basketball players competing in the State Basketball Championship (São Paulo, Brazil). | 1 basketball match, plus 30-min warm-up. | Each match included 4 × 10 min quarters with an interval of 2 min between quarter, plus a 30 min warm-up. | Intensity of the match was not controlled. | Saliva samples were collected before the warm-up and approximately 10–15 min after the end of the match. | sIgA did not change in response to the match. | No. | Small sample size, and changes in the hydration status and their possible influence on saliva flow rate were not controlled. | A basketball match does not compromise sIgA. |
| Mariscal et al. [21] | 21 elite female handball players in the Spanish national league divided into two groups: wingers/forwards (n = 10), and defenders (n = 11). | 1 official match. | Mean playing time was 25.2 min which was 42% of the match’s duration (60 min with 15 min rest between halves). | Intensity was not controlled. | Saliva samples were collected 5 min before and 10 min after the last official match | IgA fell (p < 0.01) at the end of the match. Defenders exhibited the lowest IgA concentrations after the match. Larger changes in IgA were seen in those who played for more than 30 min. | No. | Small sample size and only 1 game was analyzed. Moreover, the phase of the menstrual cycle was not controlled. | Competitive handball matches increase physiologic stress in females, resulting in decreased immunocompetence. |
| Training matches | |||||||||
| Rugby | |||||||||
| Lindsay et al. [20] | 11 rugby players from 2 senior men’s division in New Zealand. | Elite amateur rugby game that may be used to manage player recovery. | 80 min | Impacts = 46 ± 25. Distance = 6029 ± 690 (47% at <8 km/h, 27% at 8–13 km/h, 17% at 13–18 km/h, 6% at 18–23 km/h, and 2% at >23 km/h). | Saliva samples were collected 24 h before the game, immediately post-game, and at 17, 25, 38, 62, and 86 h post-game. | No significant differences in sIgA concentration before and after the game (409 ± 223 to 414 ± 255 μg/mL). | No. | Small sample size, and only one game was analyzed. | Low-intensity matches led to lack of change in sIgA. |
| Australian Football | |||||||||
| Coad et al. [30] | 11 elite Australian Rules Football League athletes. | 3 matches during the pre-season. | Each match, 4 × 30 min quarters. | Player load during match 3 (1266 ± 124.6 AU) was significantly (p < 0.01) greater than in match 1 (1096 ± 115.1 AU) and match 2 (1082 ± 90.4 AU). | Saliva samples were collected across each match 24 h and 1 h pre-match and 1, 12, 36, and 60 h post-match. | Across match 3, sIgA was significantly (p < 0.01) suppressed at 2 post-match measures (12 and 36 h) compared with pre-match measures (24 and 1 h), which coincided with significantly (p < 0.01) elevated player load. | No. | Small sample size, and only 3 matches were analyzed from pre-season. | The findings indicated that an increase in player load during the match resulted in compromised post-match mucosal immunological function. |
| Handball | |||||||||
| Caetano Júnior et al. [24] | 14 male handball players. | 1 simulated handball match. | 20 min of warm-up, 1 match composed of two halves of 30 min with 5 min interval for recovering. | Players indicated that match intensity was difficult or very difficult according to the rated perceived exertion scale. | Saliva samples were collected ~10 min before (~4:00 p.m.), ~5 min after the match, and after 2 h of recovery. | The saliva samples collected before and after match showed no significant difference. | No. | Small sample size, and only 1 match was analyzed. | No significant spectral differences to saliva sample collected pre- and post-match, as well as after 2 h of recovery. |
| Futsal | |||||||||
| Arruda et al. [32] | 10 elite futsal players from a Brazilian under-20 team. | 1 simulated futsal match. | 80 min. | Session rated perceived exertion revealed 400.00 ± 37.71 AU of training load. | At rest, before the start of the match and 5–10 min after the match. | sIgA before = 715.6 ± 214.8; sIgA after = 463.9 ± 154.6 μg/mL (p < 0.05). | No | Small sample size, and only 1 match was analyzed. | Simulated futsal matches induce a high level of stress, moderated by the high-magnitude internal load and by decreasing the level of SIgA. |
| Studies with both official and training matches | |||||||||
| Basketball | |||||||||
| Moreira et al. [36] | 10 elite young male basketball under-19 players playing in the main São Paulo (Brazil) competition. | 15 weeks with 3 simulated training matches and 2 official matches. | 5 days, 2 trainings/day, 90–120 min/training 1 match (4 × 10 min quarters, with 2 min rest and 30 min warm up). | Match intensity was controlled through session rated perceived exertion and revealed that official matches were significantly (p < 0.05) greater than the simulated training match. | 30 min before the pre-match warm-up and 10 min after each match. | No significant changes in sIgA concentrations were observed across either the simulated or official matches. | No. | Small sample size. | No changes or differences in sIgA were noted between pre- and post-moments across all matches. |
| Ref. | Sample | Stressor | Immunoglobulin (IgA) | Study Limits | Lessons Learned and Concluding Remarks | ||||
|---|---|---|---|---|---|---|---|---|---|
| Test | Volume | Intensity | Salivary Test | Outcomes | IgA–URTI Relationship | ||||
| Training | |||||||||
| Rugby | |||||||||
| Tiernan et al. [10] | 19 male elite rugby union players. | 10 week training. | Players were trained 4–5 days a week, with multiple training sessions a day. | Approximately 1800–2600 AU weekly rated perceived exertion. | Saliva samples were collected twice a week, Monday and Friday, within 1 h of the players waking up. before training. | No significant differences in weekly sIgA levels were found over the 10 week period. | The likelihood of suffering from an URTI increased when sIgA significantly decreased (p = 0.046). | The data collection was only related to the pre-season. Moreover, the sample size was small. | A decrease in >65% of sIgA meant players were at risk within the following 2 weeks of contracting an URTI. |
| Yamauchi et al. [39] | 32 male collegiate rugby football players. | 1 month training camp. | 2 training sessions (morning and afternoon sessions) each day and lasted approximately 2 h. | Intensity was not controlled. | All saliva samples were collected every day before breakfast at 6:30 a.m. | sIgA secretion rate was significantly decreased from baseline 1 day before and 1, 2, 3 days after the day of first Epstein–Barr virus expression during the camp (p < 0.05). | No. | The lack of control of medications and supplementations, along with the small sample size. | The number of URTIs increased along with the Epstein–Barr virus expression and the decrease in sIgA, suggesting that the appearance of symptoms is associated with reactivation of Epstein–Barr virus and reduction in sIgA during training. |
| Basketball | |||||||||
| Nunes et al. [27] | 19 elite female basketball players on the Brazilian National Team. | 12 weeks. | Volume and intensity progression along the periodization plan. | Weeks 1–3 = moderate. Weeks 4–6 = moderate to high intensity. Weeks 8–12 = speed agility. | 1 day before and 1 day after 12 week intervention. | Salivary measures did not change despite the fluctuations in the training program. | No. | The frequency of saliva sampling could influence the results obtained. | The periodized training plan promoted improvement in physical performance avoiding major variations on IgA. |
| Moreira et al. [37] | 10 athletes and staff members from a national basketball team. | 17 day training period. | Athletes completed a mean training volume of ~25–30 h per week. | Coaches assumed that the athletes performed all sessions with maximal intensity, and, in this case, the training volume would represent the actual training intensity. | Saliva samples were collected at the beginning of the preparation for the Pan American Games, and 1 day before the first game, at rest, in the afternoon (3:30 p.m.). | Decrease in sIgA levels following training was greater in athletes than in support staff; however, no significant differences between the 2 groups were detected. Significant decreases were found after the period analyzed (p < 0.05). | No. | No training program exercises were revealed. There was an absence of observations in sIgA levels on motor performance tests. The sample size was small. | A situation of combined stress for an important championship was found to decrease the level of sIgA-mediated immune protection at the mucosal surface in team members, with greater changes observed in the athletes. |
| Ice Hockey | |||||||||
| Orysiak et al. [38] | 12 young Polish ice hockey national team members. | 17 day training period with 2 phases: (1) intensification phase: (days 1–8); (2) tapering (days 9–17). | Both phases of training were ~41.5 h: 13.5 h of strength training and 28 h of training on ice. On days 14 and 15, they played (full-time) friendly international matches. | Session rated of perceived exertion range values: 1260 ± 721 AU and 990 ± 719 AU in phase 1 and phase 2, respectively. | Before training camp. 9 days after the training intensification and on day 13. Saliva collection took place after a minimum of 12 h after the last training. | A significant increase from sIgA1 to sIgA2 in the third collection compared with the second (114.45 ± 33.00 vs. 77.49 ± 27.29 and 88.97 ± 25.33 vs. 71.65 ± 32.44 U, respectively). | There were no statistically significant correlations between the URTI incidence and sIgA. | Food and alimentary habits were not controlled, along with the small sample size. | The tapering period positively affects the mucosal immune function, especially sIgA1 and sIgA2 concentrations, with no significant change in frequency of URTI in young ice hockey players. |
| Training with strength/resistance | |||||||||
| Basketball | |||||||||
| Nunes et al. [22] | 14 female basketball players Brazilian National Team. | 3 different resistance exercise protocols. | Participants attended 4 assessments over a period of 40 day. | Endurance (4 × 12, 60% of 1RM, 1 min rest) Hypertrophy (1 set of 5RM, 1 set of 4RM, 1 set of 3RM, 1 set of 2RM, and 1 set of 1RM. 3 min rest followed by 3 sets of 10RM with 2 min rest period). Power (3 sets of 10 reps, 50% 1RM, 3 min rest). | sIgA samples were collected at 7:30 a.m., pre-exercise at 9:30 a.m., postexercise, and at 5:30 p.m. | No differences in sIgA concentrations were observed across the 3 schemes at any time (p > 0.05). | No. | Menstrual cycle not controlled, small sample size, and no randomized order in schemes. | There were no changes in sIgA concentrations for any workout scheme. |
| Nunes et al. [33] | 12 elite female basketball players. | 50 day period of resistance training. | The volume of the 50 day period of resistance training was not described. | Endurance: 3 weeks (3/4 × 15/20). Strength: 2 weeks (3/6 × 1/10). Power: 2 weeks (3/6 × 6/10, 30–50% 1RM). | Saliva samples were collected at 7:00 a.m., 9:30 a.m., 11:00 a.m., and 5:30 p.m. both pre- and post-training, after 2 full days of complete rest. | IgA concentrations were lowered at 9:30 and 11:00 a.m. (p < 0.05). | No. | Small sample size, and participants were subjected to other conditioning practices. | A periodized approach to resistance training increased muscle performance in elite female basketball players and only minor changes in the salivary IgA were noted. |
| Futsal | |||||||||
| Milanez et al. [23] | 13 top-level professional female futsal players who were second place in the Brazilian National League in 2009. | 5 training weeks in pre-season period. | Resistance: 4 times/week (30–40 min/day). Together, 5 technical/tactic sessions/week (80–120 min). Week 4: resistance decrease to 2 times. Last 2 weeks: volume maintenance. | Resistance (3 × 15 at 70%, rest 45 s. Progressive load in the 3 first weeks (~360–425 AU) while weeks 4 and 5 had a load decrease to ~300 and 250 AU for rated perceived exertion, respectively. | Saliva samples were collected 1 week before the start and prior the last training session of each week at the same time of the day. | There was a significant increase in training load, monotony, and training strain in week 3, with a concomitant and significant reduction in percentage variation of sIgA concentration and secretion rate (p < 0.05). | No. | Small sample size. | A link among training load, sIgA levels, and stress symptoms was evident in a nonlinear fashion. Above ~435 and ~3160 AU per session rated perceived exertion and strain, there was a decrease in SIgA levels. |
| Moreira et al. [25] | 12 elite Brazilian futsal players. | 4 weeks of intensive training during the competitive season with 27 training sessions performed. | Week 1 = 8 sessions (1095 min). Week 2 = 9 sessions (12,967 min). Week 3 = 6 sessions (755 min). Week 4 = 4 sessions (555 min). | First 2 weeks, higher intensity. Weeks 3–4, load (frequency/volume) was reduced. | Before each week start and at least 36 h after the last training). | No significant differences were observed for sIgA during the study (p > 0.05). | The relative change in sIgA absolute was associated with the URTI severity during week 4 (r = −0.74; p < 0.05). | The collection of samples after fasting overnight was not applied along with the small sample size. | Futsal athletes were more susceptible to high URTI symptom severity in the periods of higher training intensity and volume. A reduction in training load before competitions is an appropriate strategy to minimize URTI symptoms, ensuring the athlete’s ability to train and compete. |
| Ref. | Sample | Stressor | Immunoglobulin (IgA) | Study Limits | Lessons Learned and Concluding Remarks | ||||
|---|---|---|---|---|---|---|---|---|---|
| Test | Volume | Intensity | Salivary Test | Outcomes | IgA–URTI Relationship | ||||
| Rugby | |||||||||
| Cunniffe et al. [28] | 31 elite rugby union players. | 48 weeks (full season). | 34 games and 345 h of scheduled training. | Monthly comparisons during the season. The peak values were reported for February (10,914 ± 831 AU) before decreasing again until the close of the season (May = 5177 ± 369 AU). | Saliva IgA (n = 11) was taken at regular monthly intervals across the season. | Decreases in sIgA were observed during August (20%), December (29%), and February (9%). | Despite lower mean sIgA concentration in players who reported incidences of URTI, no significant correlation was found between absolute sIgA and URTI incidence. | The nonuse of a control group. | Higher stress-induced contributed to reductions in mucosal immunity, which, when lowered, predisposed rugby players to increased risk of illness. |
| Basketball | |||||||||
| Moreira et al. [26] | 15 basketball players. | 4 weeks during the competitive season with 1 game per week. | 90–120 min per session, 2 sessions per day, and 5 days per week. | Weeks 1–4: 656 ± 92, 680± 83, 548 ± 37, and 479 ± 34 AU of rated perceived exertion, respectively. | Saliva samples were collected at rest, in the afternoon, at the same time of day both before and after the investigated period. | Decreases in sIgA secretion reduced, while absolute sIgA concentration increased after four weeks (587 ± 94 to 720 ± 153 and 106 ± 20 to 92 ± 21 μg/mL, respectively). | No. | The inability to monitor the salivary parameters each week. Correlations over the 4 time points were not applied, and the sample size was small. | Initial levels of sIgA secretion were negatively and significantly correlated with the signs and symptoms of stress at week 4, which could indicate that the athletes with low levels of sIgA secretion were more susceptible to be affected by different stressors. |
| He et al. [31] | 8 members of National Taichung University basketball team in Taiwan. | 11 weeks were analyzed (4 weeks of training, 3 weeks of competition, and 4 weeks of recovery with no training sessions). | Weeks 1–4: duration was ~540 min per week; weeks 5–7: duration was 300 min per week. | Weeks 1–4: higher-intensity training sessions. Weeks 5–7: intensity reduced where 2 matches were played but no metric was used to control intensity. | Saliva samples were collected at rest and before the start of practice or competition, in the afternoon, at 7 time points during the intense training, competition and recovery period. | Significant decreases in sIgA secretion rates and absolute concentrations were observed during the training and competition period. | No. | Small sample size. | Intensive training and competition have adverse effects on the mucosal immunity in basketball players. |
| Ice Hockey | |||||||||
| Orysiak et al. [29] | 27 under-17 ice hockey players from the Athletic High School of the Polish Ice Hockey Federation | 24 weeks from competitive season. | In competitive phases, the hockey players participated in 5 weekly training sessions (120–180 min). They also played 1 or 2 matches per week. | Highest training load was found at the beginning of the period (from sampling 1 to 2), and then lower until sampling4. High training loads were observed between sampling 5 and 6, as well as between 7 and 8. | 8 times every 3–4 weeks for 21 weeks (before start of the season, weeks 4, 6, 8, 11, 14, 18, 21). A minimum of 12 h after the last training. | Athletes had a lower sIgA concentration at the time when they had symptoms of URTI. | No. | There were some congested periods which were not analyzed, specifically. Moreover, the sample size was small. | Lower concentrations of sIgA during URTI in athletes were observed, which may confirm the suppression of mucosal immunity and initiation responses to pathogenic infections by innate immunity. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rico-González, M.; Clemente, F.M.; Oliveira, R.; Bustamante-Hernández, N.; Pino-Ortega, J. Part I: Relationship among Training Load Management, Salivary Immunoglobulin A, and Upper Respiratory Tract Infection in Team Sport: A Systematic Review. Healthcare 2021, 9, 366. https://doi.org/10.3390/healthcare9040366
Rico-González M, Clemente FM, Oliveira R, Bustamante-Hernández N, Pino-Ortega J. Part I: Relationship among Training Load Management, Salivary Immunoglobulin A, and Upper Respiratory Tract Infection in Team Sport: A Systematic Review. Healthcare. 2021; 9(4):366. https://doi.org/10.3390/healthcare9040366
Chicago/Turabian StyleRico-González, Markel, Filipe Manuel Clemente, Rafael Oliveira, Naia Bustamante-Hernández, and José Pino-Ortega. 2021. "Part I: Relationship among Training Load Management, Salivary Immunoglobulin A, and Upper Respiratory Tract Infection in Team Sport: A Systematic Review" Healthcare 9, no. 4: 366. https://doi.org/10.3390/healthcare9040366
APA StyleRico-González, M., Clemente, F. M., Oliveira, R., Bustamante-Hernández, N., & Pino-Ortega, J. (2021). Part I: Relationship among Training Load Management, Salivary Immunoglobulin A, and Upper Respiratory Tract Infection in Team Sport: A Systematic Review. Healthcare, 9(4), 366. https://doi.org/10.3390/healthcare9040366