
Influence of the Perception of Barriers in Practice of PA in Adolescents: Explanatory Model

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
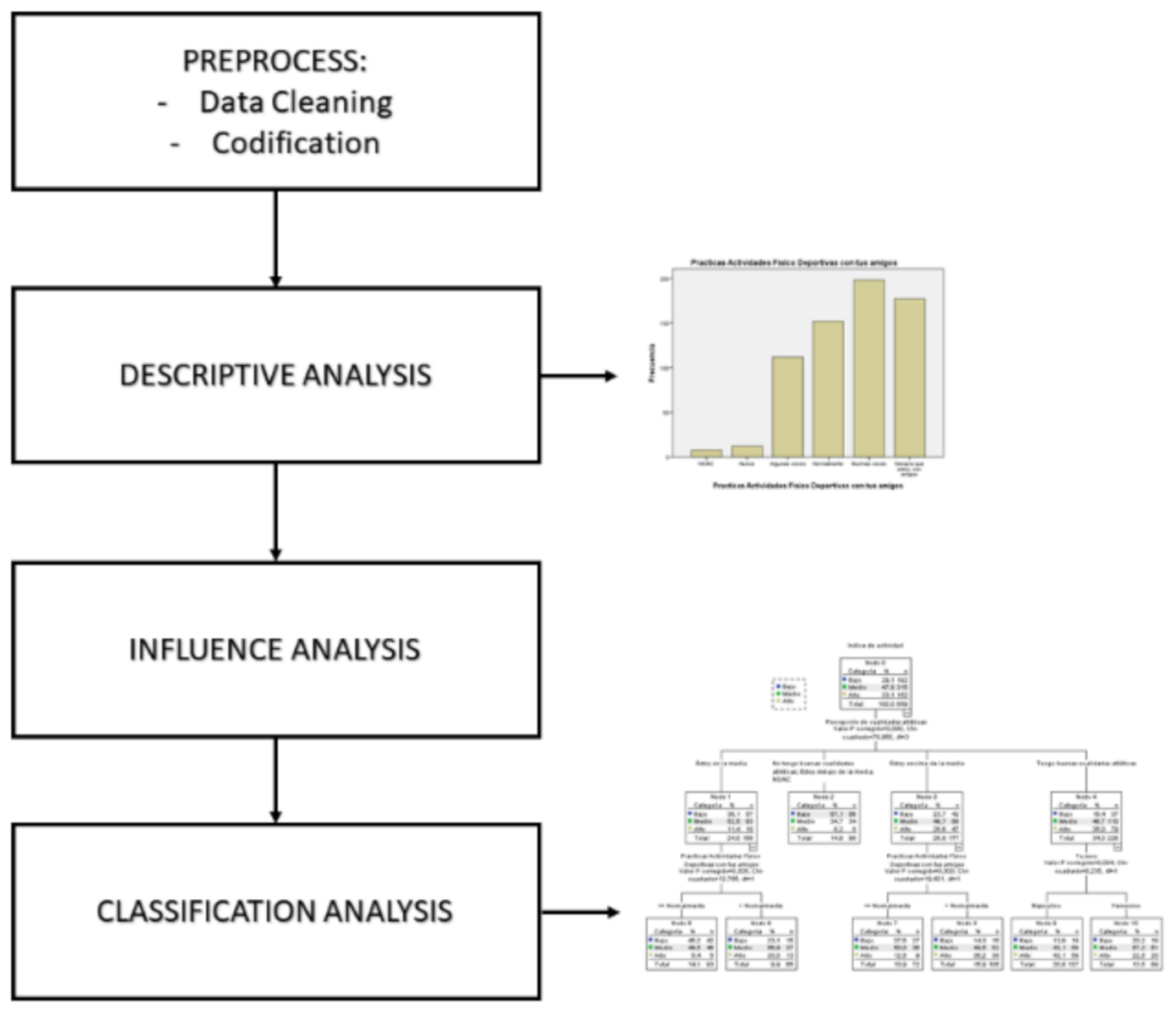
2.1. Design
2.2. Participants
2.3. Instrument
2.4. Variables
2.5. Procedure
2.6. Statistics Analysis
3. Results
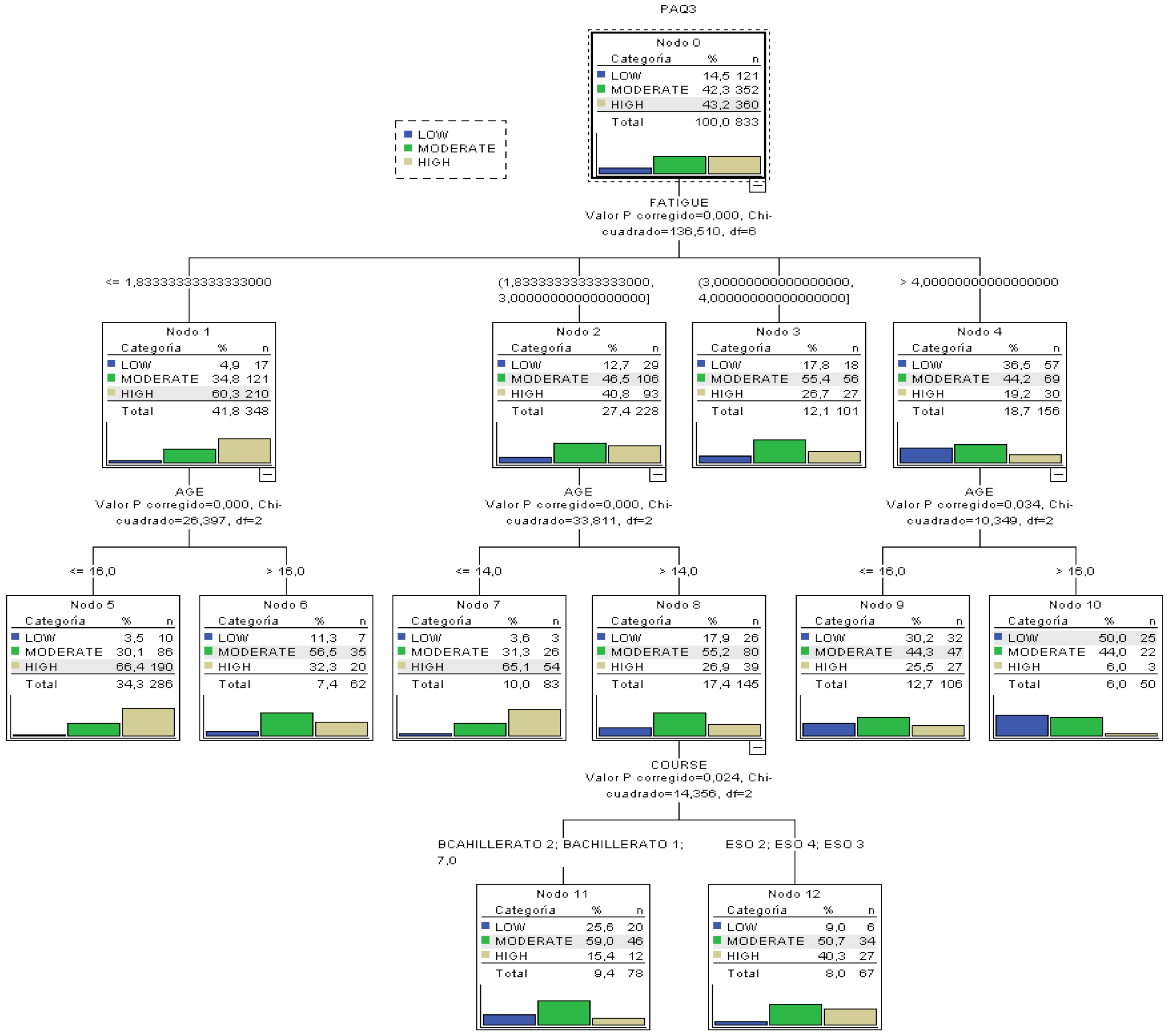
- The most important variable to categorize the level of PA is the Tiredness and Laziness barrier, because it is higher up in the tree.
- From the ANOVA and correlation analyses (Pearson correlation coefficient) before constructing the tree, the variables with the highest degree of influence in PA had been determined. The tree confirms such analysis because the variables different from age, school year and tiredness barriers do not appear as influential in the tree.
- The most probable case (50%) for a low level of PA can be extracted: a subject with a value in the tiredness and laziness barrier over 4 and over 16 years of age.
- The most probable case of having a high index of PA can be determined: subjects with a value of tiredness barrier over 1.83 and less than 16 years of age present a probability of 66.4% of having a high index of PA.
- Classification rules for the three types of PA can be extracted, besides the most extreme cases previously mentioned.
- In the variable Age, we can see that the threshold value that limits the classification is 16 years, so that is the most important age in the variability of PA.
- In the variable school year, the creation of a group with the oldest students (Baccalaureate) and the youngest (CSE) can clearly be seen. Therefore, in that second group we find a higher probability of having a high index of PA (40%).
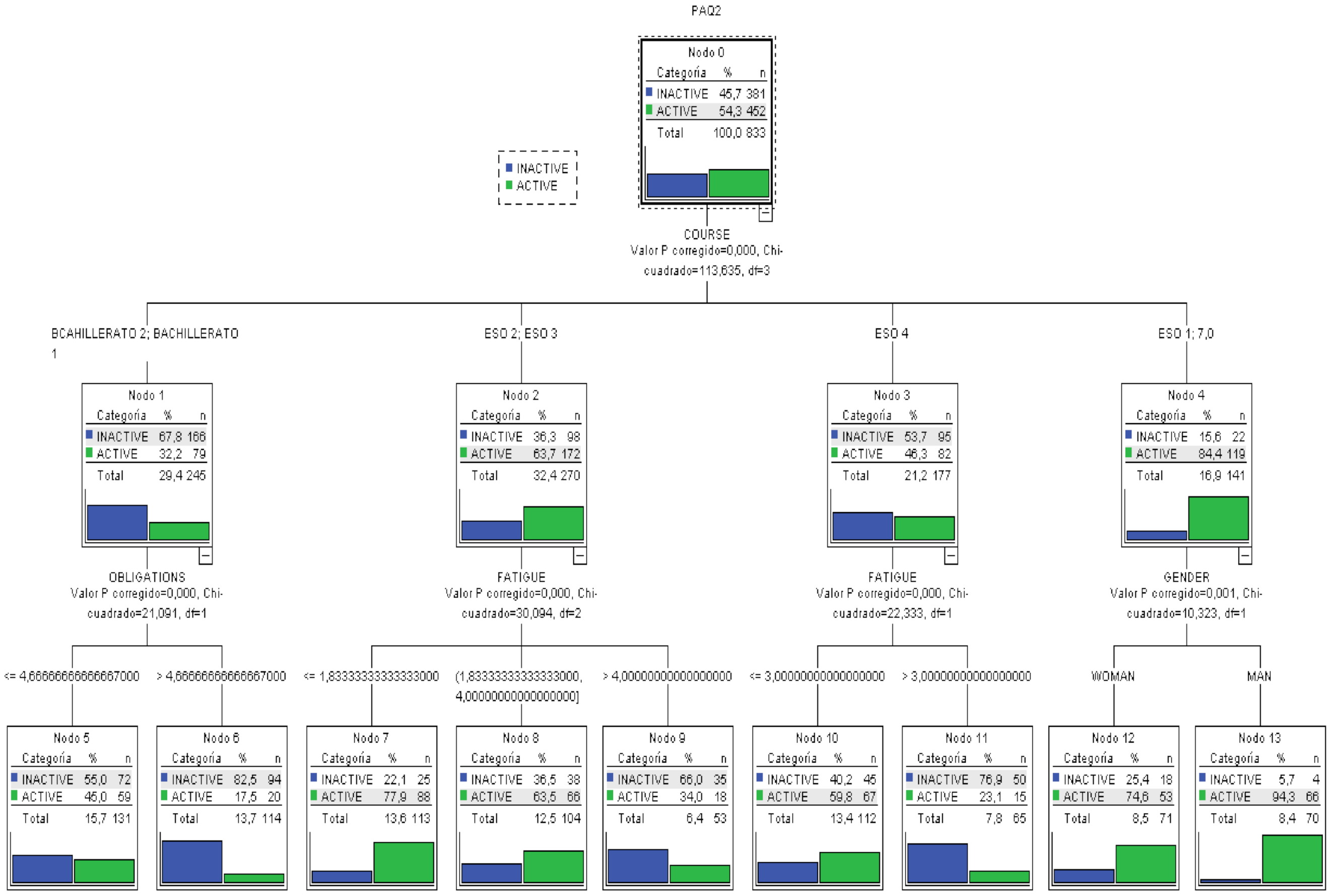
- The most important variable in the categorization of the level of PA is school year, because it is higher up.
- The variables that the ANOVA and correlation analysis had determined not to be influential maintain that status in the model, because they do not appear in any level of the tree.
- The most probable case (82.5%) for a low level of PA can be extracted: a subject in a late school year (Baccalaureate) and many responsibilities.
- The most probable case for a high index of PA can be determined: male subjects in an early school year (CSE 1º) show a probability of 94.3% of having a high index of PA.
- Any classification rules for the three types of PA besides the extreme cases previously discussed.
- In this model, the error rate of the tress as a classification model is 15%, that is, given a new subject, after measuring the different variables, it could be categorized in its level of PA with an error margin of 15%.
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ledezma, J.C.R.; Barrera, J.H.; Díaz, J.R.G.; Jaén, A.L.; García, L.I.M.; Medina, M.S.H.; Vázquez, J.R. Factores desencadenantes de obesidad infantil, un problema de salud pública. J. Negat. No Posit. Results 2018, 3, 614–626. [Google Scholar] [CrossRef]
- Ramírez, J.C.; Rojas, L.A.; Romero, O.C.; Reynoso, J. Análisis situacional de la prevalencia e incidencia de la obesidad en Latinoamérica: Caso México y Colombia. Educ. Y Salud Boletín Científico Inst. Cienc. Salud Univ. Autónoma Estado Hidalgo 2017, 6. [Google Scholar] [CrossRef]
- Pate, R. Compliance with Physical Activity Guidelines Prevalence in a Population of Children and Youth. Ann. Epidemiol. 2002, 12, 303–308. [Google Scholar] [CrossRef]
- Fox, A.M.; Mann, D.M.; Ramos, M.A.; Kleinman, L.C.; Horowitz, C.R. Barriers to Physical Activity in East Harlem, New York. J. Obes. 2012, 2012, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tompkins, C.L.; Seablom, M.; Brock, D.W. Parental Perception of Child’s Body Weight: A Systematic Review. J. Child Fam. Stud. 2014, 24, 1384–1391. [Google Scholar] [CrossRef]
- Awadalla, N.; AboElyazed, A.; Hassanein, M.; Khalil, S.; Aftab, R.; Gaballa, I.; Mahfouz, A. Assessment of physical inactivity and perceived barriers to physical activity among health college students, south-western Saudi Arabia. East. Mediterr. Health J. 2014, 20, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Herazo-Beltrán, Y.; Pinillos, Y.; Vidarte, J.; Crissien, E.; Suarez, D.; García, R. Predictors of perceived barriers to physical activity in the general adult population: A cross-sectional study. Braz. J. Phys. 2017, 21, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Ploughman, M. Breaking down the barriers to physical activity among people with multiple sclerosis—A narrative review. Phys. Rev. 2017, 22, 124–132. [Google Scholar] [CrossRef]
- Zaragoza, J.; Generelo, E.; Julián, J.A.; Abarca-Sos, A. Barriers to adolescent girls’ participation in PA defined by PA levels. J. Sports Med. Phys. Fit. 2011, 51, 128–135. [Google Scholar]
- Smits, J.A.J.; Tart, C.D.; Presnell, K.; Rosenfield, D.; Otto, M.W. Identifying Potential Barriers to Physical Activity Adherence: Anxiety Sensitivity and Body Mass as Predictors of Fear During Exercise. Cogn. Behav. 2010, 39, 28–36. [Google Scholar] [CrossRef]
- Watts, A.S.; Mortby, M.E.; Burns, J.M. Depressive symptoms as a barrier to engagement in physical activity in older adults with and without Alzheimer’s disease. PLoS ONE 2018, 13, e0208581. [Google Scholar] [CrossRef]
- Shin, C.-N.; Lee, Y.-S.; Belyea, M. Physical activity, benefits, and barriers across the aging continuum. Appl. Nurs. Res. 2018, 44, 107–112. [Google Scholar] [CrossRef]
- Van Stappen, V.; Latomme, J.; Cardon, G.; De Bourdeaudhuij, I.; Lateva, M.; Chakarova, N.; Kivelä, J.; Lindström, J.; Androutsos, O.; González-Gil, E.; et al. Barriers from Multiple Perspectives Towards Physical Activity, Sedentary Behaviour, Physical Activity and Dietary Habits When Living in Low Socio-Economic Areas in Europe. The Feel4Diabetes Study. Int. J. Env. Res. Public Health 2018, 15, 2840. [Google Scholar] [CrossRef] [Green Version]
- Blake, H.; Stanulewicz, N.; McGill, F. Predictors of physical activity and barriers to exercise in nursing and medical students. J. Adv. Nurs. 2016, 73, 917–929. [Google Scholar] [CrossRef] [Green Version]
- Taylor, L.G.; Clark, A.F.; Gilliland, J.A. Context Matters: Examining children’s perceived barriers to physical activity across varying Canadian environments. Health Place 2018, 54, 221–228. [Google Scholar] [CrossRef]
- Al-Baho, A.K.; Al-Naar, A.; Al-Shuaib, H.; Panicker, J.K.; Gaber, S. Levels of Physical Activity among Kuwaiti Adults and Perceived Barriers. Open Public Health J. 2016, 9, 77–87. [Google Scholar] [CrossRef]
- Farahani, L.A.; Hasanpoor-Azgahdy, S.B.; Taghizadeh, Z. Iranian Women’s Perceptions and Experiences of Barriers to and Facilitators of Physical Activity. Shiraz E Med. J. 2018, 19, 7. [Google Scholar] [CrossRef] [Green Version]
- Jodkowska, M.; Mazur, J.; Oblacińska, A. Perceived barriers to PA among Polish adolescents. Przegl. Epidemiol. 2015, 69, 73–78. [Google Scholar]
- Serra Puyal, J.R.; Generelo Lanaspa, E.; Zaragoza Casterad, J. Barreras para la realización de actividad física en adolescentes en la provincia de Huesca. Int. J. Med. Sci. PA Sport 2010, 10, 470–482. [Google Scholar]
- Moreno Murcia, J.A.; Pardo, M.; Jorge, P.; Huéscar, E. Motivos de práctica físico-deportiva en mujeres: Diferencias entre practicantes y no practicantes. Rev. Psicol. Deporte 2016, 25, 35–41. [Google Scholar]
- Anjali, A.; Sabharwal, M. Perceived Barriers of Young Adults for Participation in Physical Activity. Curr. Res. Nutr. Food Sci. J. 2018, 6, 437–449. [Google Scholar] [CrossRef] [Green Version]
- Planchard, J.-H.; Corrion, K.; Lehmann, L.; D’Arripe-Longueville, F. Worksite Physical Activity Barriers and Facilitators: A Qualitative Study Based on the Transtheoretical Model of Change. Front. Public Health 2018, 6, 326. [Google Scholar] [CrossRef] [PubMed]
- Keegan, J.; Brooks, J.; Blake, J.; Muller, V.; Fitzgerald, S.; Chan, F. Perceived Barriers to Physical Activity and Exercise for Individuals with Spinal Cord Injury. Aust. J. Rehabil. Couns. 2014, 20, 69–80. [Google Scholar] [CrossRef] [Green Version]
- Brinthaupt, T.M.; Kang, M.; Anshel, M.H. A delivery model for overcoming psycho-behavioral barriers to exercise. Psychol. Sport Exerc. 2010, 11, 259–266. [Google Scholar] [CrossRef]
- Buman, M.P.; Yasova, L.D.; Giacobbi, P.R. Descriptive and narrative reports of barriers and motivators to physical activity in sedentary older adults. Psychol. Sport Exerc. 2010, 11, 223–230. [Google Scholar] [CrossRef]
- Hernández, R.; Fernández, C.; Baptista, P. Metodología de la Investigación; Mc Graw Hill: Mexico City, Mexico, 2006. [Google Scholar]
- Cohen, L.; Manion, L.; Morrison, K. Research Methods in Education; Routledge/Falmer: Abingdon, UK, 2007. [Google Scholar] [CrossRef]
- Capdevila, L. Actividad Física y Salud; Miracle: Barcelona, Spain, 2005. [Google Scholar]
- Niñerola, J.; Capdevila, L.; Pintanel, M. Barreras percibidas y actividad física: El autoinforme de barreras para la práctica de ejercicio físico. Rev. Psicol. Deporte 2006, 15, 53–69. [Google Scholar]
- Domínguez-Alonso, J.; López-Castelo, A.; Portela-Pino, I. Propiedades Psicométricas Del Autoinforme De Barreras Para La Práctica Del Ejercicio Físico (ABPEF). Rev. Int. Med. Cienc. Act. Física Deporte 2018, 18, 737–752. [Google Scholar] [CrossRef] [Green Version]
- Kowalski, K.C.; Crocker, P.R.; Faulkner, R.A. Validation of the Physical Activity Questionnaire for Older Children. Pediatr. Exerc. Sci. 1997, 9, 174–186. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.-R.; Lee, Y.-J.; Chiu, H.-W.; Jeng, C. Impact of physical activity on heart rate variability in children with type 1 diabetes. Childs Nerv. Syst. 2007, 24, 741–747. [Google Scholar] [CrossRef]
- Gomes, T.N.; Dos Santos, F.K.; Zhu, W.; Eisenmann, J.; Maia, J.A.R. Multilevel Analyses of School and Children’s Characteristics Associated with Physical Activity. J. Sch. Health 2014, 84, 668–676. [Google Scholar] [CrossRef]
- Chahla, S.E.; Frohnert, B.I.; Thomas, W.; Kelly, A.S.; Nathan, B.M.; Polgreen, L.E. Higher daily physical activity is associated with higher osteocalcin levels in adolescents. Prev. Med. Rep. 2015, 2, 568–571. [Google Scholar] [CrossRef] [Green Version]
- Benítez-Porres, J.; Alvero-Cruz, J.R.; Sardinha, L.B.; López-Fernández, I.; Carnero, E.A. Valores de corte para clasificar niños y adolescentes activos utilizando el Cuestionario de Actividad Física: PAQ-C y PAQ-A. Nutr. Hosp. 2016, 33, 1036–1044. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0212-16112016000500005 (accessed on 29 March 2021).
- Portela-Pino, I.; López Castedo, A. Percepción de barreras para la práctica del ejercicio físico en adolescentes gallegos. Rev. Estud. Investig. Psicol. Educ. 2017, 14, 174–177. [Google Scholar] [CrossRef] [Green Version]
- Eng, L.; Pringle, D.; Su, J.; Shen, X.; Mahler, M.; Niu, C.; Charow, R.; Tiessen, K.; Lam, C.; Halytskyy, O.; et al. Patterns, perceptions, and perceived barriers to physical activity in adult cancer survivors. Support. Care Cancer 2018, 26, 3755–3763. [Google Scholar] [CrossRef]
- Troped, P.J.; Tamura, K.; McDonough, M.H.; Starnes, H.A.; James, P.; Ben-Joseph, E.; Cromley, E.; Puett, R.; Melly, S.J.; Laden, F. Direct and Indirect Associations Between the Built Environment and Leisure and Utilitarian Walking in Older Women. Ann. Behav. Med. 2017, 51, 282–291. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Castruita, R.M.; González Castro, J.C.A.; Raimundi, M.J.; Enríquez-Reyna, M.C. Beneficios, barreras y apoyo social para el ejercicio: Diferencias por grado escolar. Rev. Psicol. Deporte 2017, 26, 165–171. [Google Scholar]
- American Academy of Pediatrics. Committee on Public Education Children, Adolescents, and Television. Pediatrics 2001, 107, 423–426. [CrossRef] [PubMed] [Green Version]
- Alghadir, A.H.; A Gabr, S.; A Iqbal, Z. Television watching, diet and body mass index of school children in Saudi Arabia. Pediatr. Int. 2015, 58, 290–294. [Google Scholar] [CrossRef]
- Hamilton, K.; Hatzis, D.; Kavanagh, D.J.; White, K.M. Exploring Parents’ Beliefs About Their Young Child’s Physical Activity and Screen Time Behaviours. J. Child Fam. Stud. 2014, 24, 2638–2652. [Google Scholar] [CrossRef]
- Martínez Gatica, C.G. Patrones del Ciclo Sueño/Vigilia en Lactantes Influyen en el Estado Nutricional de Adolescentes. Ph.D. Thesis, Universidad de Chile, Santiago de Chile, Chile, 2018. [Google Scholar]
- Smetaniuk, P. A preliminary investigation into the prevalence and prediction of problematic cell phone use. J. Behav. Addict. 2014, 3, 41–53. [Google Scholar] [CrossRef] [Green Version]
- López-Fernández, O. Problem Mobile Phone Use in Spanish and British Adolescents: First steps towards a cross-cultural re-search in Europe. Psychol. Soc. Netw. 2015, 2, 186–201. [Google Scholar]
- Morón, C.; Ferrández, D.; Saiz, P.; Pérez, Á. Influencia de los hábitos de sueño en los alumnos de primer ciclo de Educación Secundaria = Influence of sleep habits in students of the first cycle of Secondary Education. Adv. Build. Educ. 2018, 2, 9–24. [Google Scholar] [CrossRef]
- Quevedo-Blasco, V.J.; Quevedo-Blasco, R. Influencia del grado de somnolencia, cantidad y calidad de sueño sobre el rendi-miento académico en adolescentes. Int. J. Clin. Health Psychol. 2011, 11, 49–65. [Google Scholar]
- Davidson, E.A. The contribution of manure and fertilizer nitrogen to atmospheric nitrous oxide since 1860. Nat. Geosci. 2009, 2, 659–662. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 29 March 2021).




{kind=link}
{kind=link}
{kind=link}
| CSE 1 | CSE 2 | CSE 3 | CSE 4 | BAC 1 | BAC 2 | Total | |
|---|---|---|---|---|---|---|---|
| Frequency | 140 | 130 | 140 | 177 | 151 | 95 | 833 |
| Percentage | 16.8 | 15.6 | 16.8 | 21.2 | 18.1 | 11.4 | 100.0 |
| Variable | Category | N | Mean PA | F | p-Value |
|---|---|---|---|---|---|
| Gender | Man | 407 | 3.031 | 24.90 | 0.002 |
| Woman | 426 | 2.744 | |||
| School year | CSE 1 | 140 | 3.402 | 30.59 | 0.001 |
| CSE 2 | 130 | 3.131 | |||
| CSE 3 | 140 | 2.993 | |||
| CSE 4 | 177 | 2.738 | |||
| BAC 1 | 151 | 2.614 | |||
| BAC 2 | 95 | 2.323 |
| Chi-Square = 130.943; Sign. = 0.002 | PAQ | Total | ||||
|---|---|---|---|---|---|---|
| Low | Moderate | High | ||||
| SCHOOL YEAR | CSE 1 | Count | 5 | 35 | 100 | 140 |
| % of SCHOOL YEAR | 3.6% | 25.0% | 71.4% | 100.0% | ||
| CSE 2 | Count | 11 | 45 | 74 | 130 | |
| % of SCHOOL YEAR | 8.5% | 34.6% | 56.9% | 100.0% | ||
| CSE 3 | Count | 14 | 55 | 71 | 140 | |
| % of SCHOOL YEAR | 10.0% | 39.3% | 50.7% | 100.0% | ||
| CSE 4 | Count | 31 | 85 | 61 | 177 | |
| % of SCHOOL YEAR | 17.5% | 48.0% | 34.5% | 100.0% | ||
| BAC 1 | Count | 29 | 78 | 44 | 151 | |
| % of SCHOOL YEAR | 19.2% | 51.7% | 29.1% | 100.0% | ||
| BAC 2 | Count | 31 | 54 | 10 | 95 | |
| % of SCHOOL YEAR | 32.6% | 56.8% | 10.5% | 100.0% | ||
| Total | Count | 121 | 352 | 360 | 833 | |
| % of SCHOOL YEAR | 14.5% | 42.3% | 43.2% | 100.0% | ||
| Chi-Squared = 26.193; Sign. = 0.001 | PAQ | Total | ||||
|---|---|---|---|---|---|---|
| Low | Moderate | High | ||||
| Gender | Man | Count | 46 | 149 | 212 | 407 |
| % for Gender | 11.3% | 36.6% | 52.1% | 100.0% | ||
| Woman | Count | 75 | 203 | 148 | 426 | |
| % for Gender | 17.6% | 47.7% | 34.7% | 100.0% | ||
| Total | Count | 121 | 352 | 360 | 833 | |
| % for Gender | 14.5% | 42.3% | 43.2% | 100.0% | ||
| Variable | Correlation Coeff. | p-Value |
|---|---|---|
| Age | −0.388 | 0.001 |
| BMI | 0.0049 | 0.887 |
| Environment Barrier | −0.0963 | 0.005 |
| Tiredness and Laziness Barrier | −0.3897 | 0.002 |
| Body Image Barrier | −0.1446 | 0.001 |
| Responsibilities Barrier | −0.2577 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Portela-Pino, I.; Alvariñas-Villaverde, M.; Martínez-Torres, J.; Pino-Juste, M. Influence of the Perception of Barriers in Practice of PA in Adolescents: Explanatory Model. Healthcare 2021, 9, 380. https://doi.org/10.3390/healthcare9040380
Portela-Pino I, Alvariñas-Villaverde M, Martínez-Torres J, Pino-Juste M. Influence of the Perception of Barriers in Practice of PA in Adolescents: Explanatory Model. Healthcare. 2021; 9(4):380. https://doi.org/10.3390/healthcare9040380
Chicago/Turabian StylePortela-Pino, Iago, Myriam Alvariñas-Villaverde, Javier Martínez-Torres, and Margarita Pino-Juste. 2021. "Influence of the Perception of Barriers in Practice of PA in Adolescents: Explanatory Model" Healthcare 9, no. 4: 380. https://doi.org/10.3390/healthcare9040380
APA StylePortela-Pino, I., Alvariñas-Villaverde, M., Martínez-Torres, J., & Pino-Juste, M. (2021). Influence of the Perception of Barriers in Practice of PA in Adolescents: Explanatory Model. Healthcare, 9(4), 380. https://doi.org/10.3390/healthcare9040380