
Long-COVID Syndrome? A Study on the Persistence of Neurological, Psychological and Physiological Symptoms

 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Materials
2.3. Procedures
2.4. Statistical Analysis
3. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | N | % | |
|---|---|---|---|
| Sex | Male | 91 | 17.95% |
| Female | 416 | 82.05% | |
| Tot. | 507 | 100% | |
| Age | <20 | 1 | 0.20% |
| 20–29 | 62 | 12.23% | |
| 30–39 | 106 | 20.91% | |
| 40–49 | 156 | 30.77% | |
| 50–59 | 132 | 26.04% | |
| 60–69 | 42 | 8.28% | |
| >70 | 8 | 1.58% | |
| Educational Level | Elementary, middle, and high school education | 283 | 55.82% |
| Graduates, doctoral students, and master students | 224 | 44.18% | |
| COVID-19 status | I’ve never been tested positive | 33 | 6.51% |
| I am currently positive for COVID-19 | 20 | 3.94% | |
| I had COVID-19 but have not been positive (swab result: negative) for less than a month | 68 | 13.41% | |
| I had COVID-19 but have not been positive (swab result: negative) for at least a month | 74 | 14.60% | |
| I had COVID-19 but have not been positive (swab result: negative) for at least two months | 154 | 30.37% | |
| I had COVID-19 but have not been positive (swab result: negative) for at least three months | 152 | 29.98% | |
| Other | 6 | 1.18% | |
| Cases of COVID-19 within the family | none | 74 | 14.60% |
| 1 case | 133 | 26.23% | |
| 2 cases | 121 | 23.87% | |
| >3 cases | 179 | 35.31% |
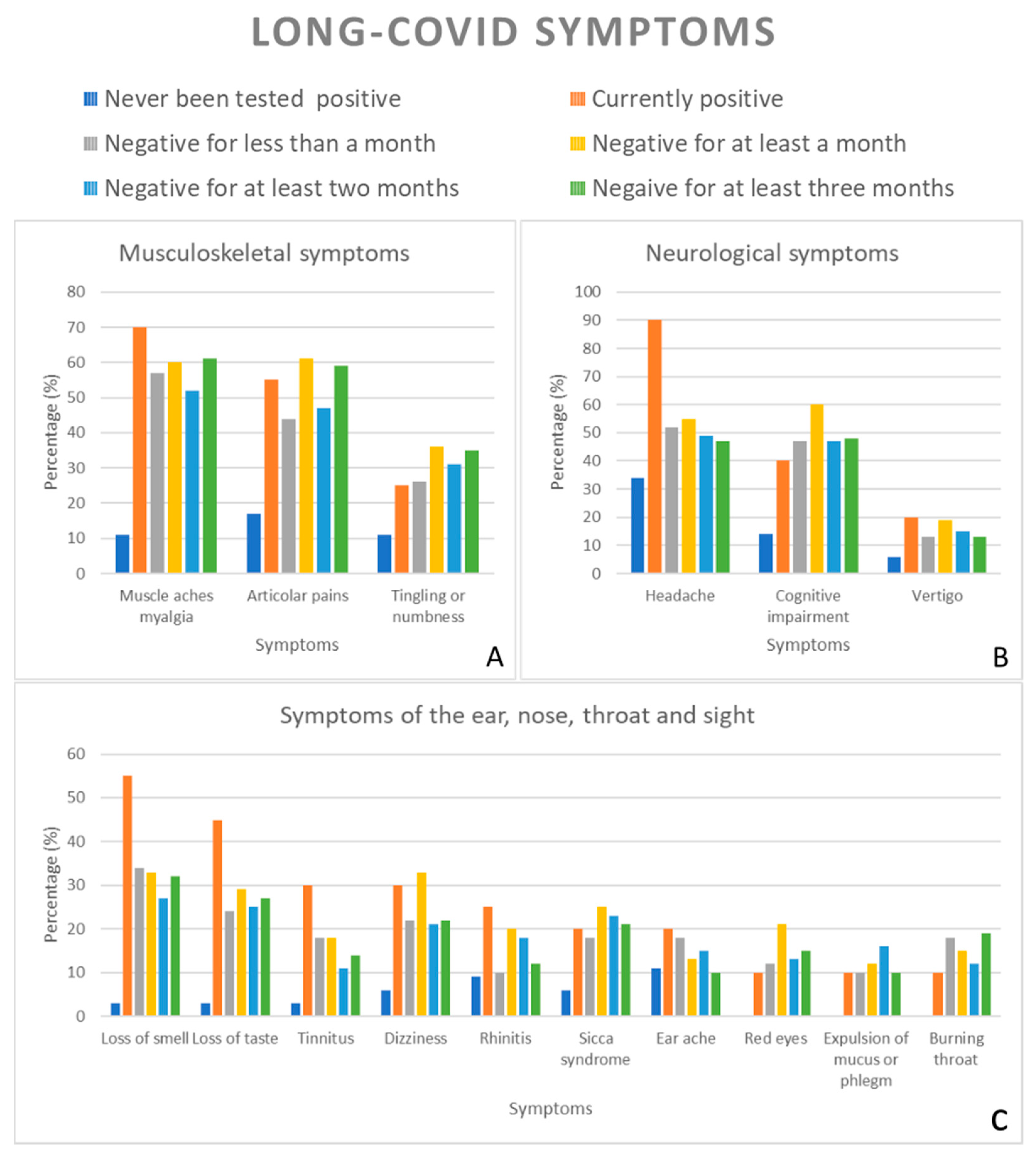
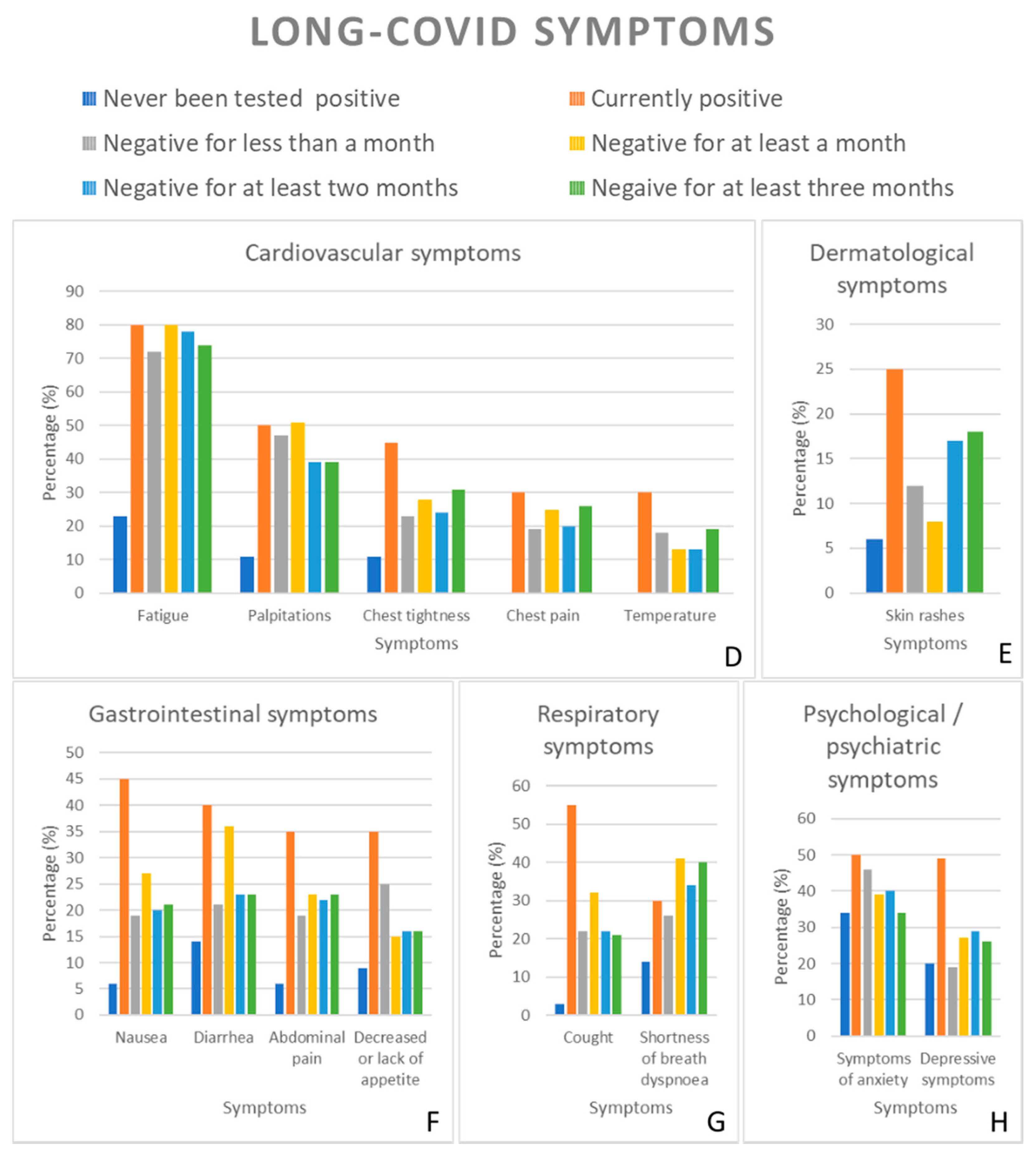
3.1. Symptoms Long-COVID-19 Syndrome
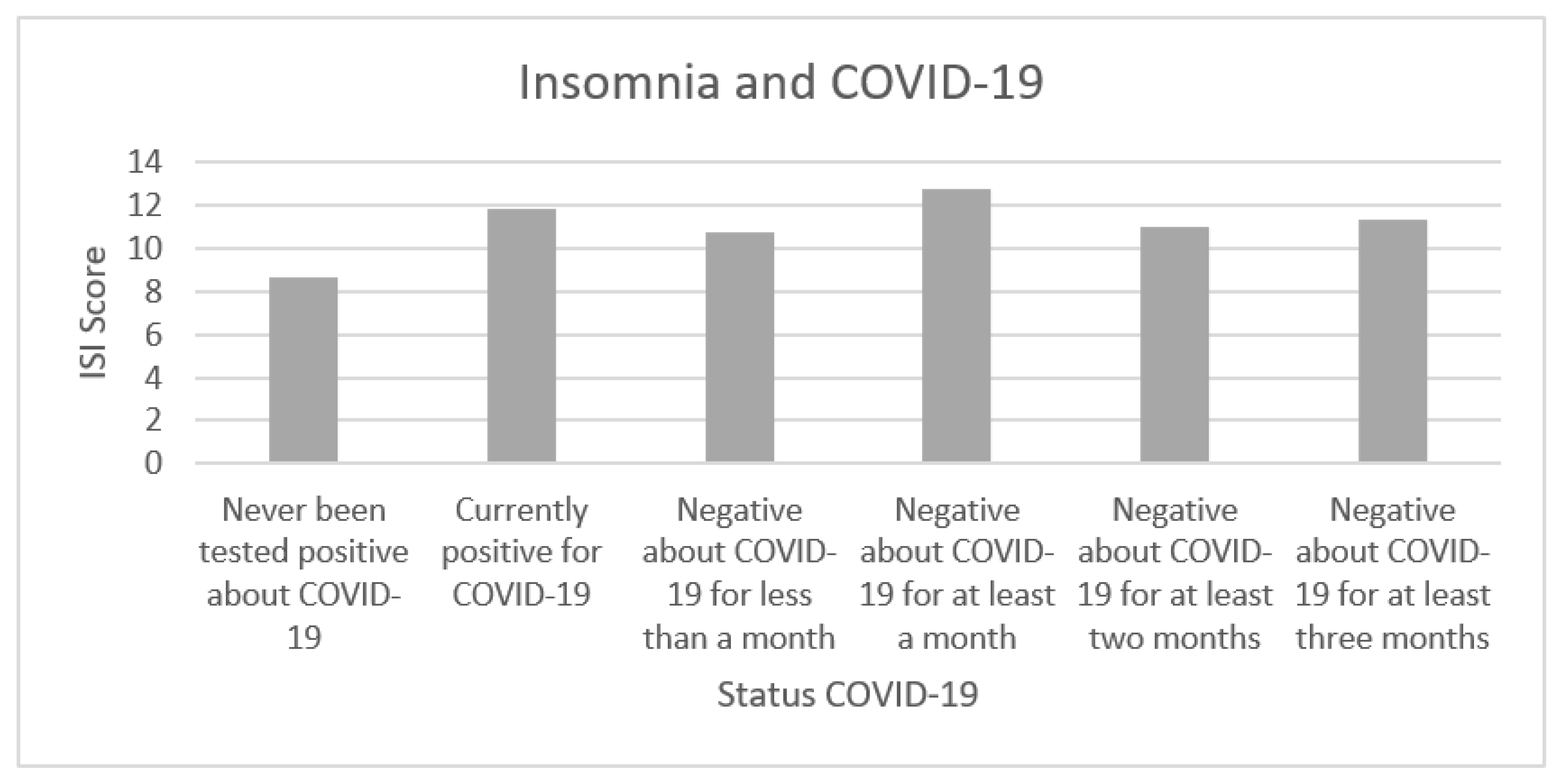
3.2. Insomnia and COVID-19
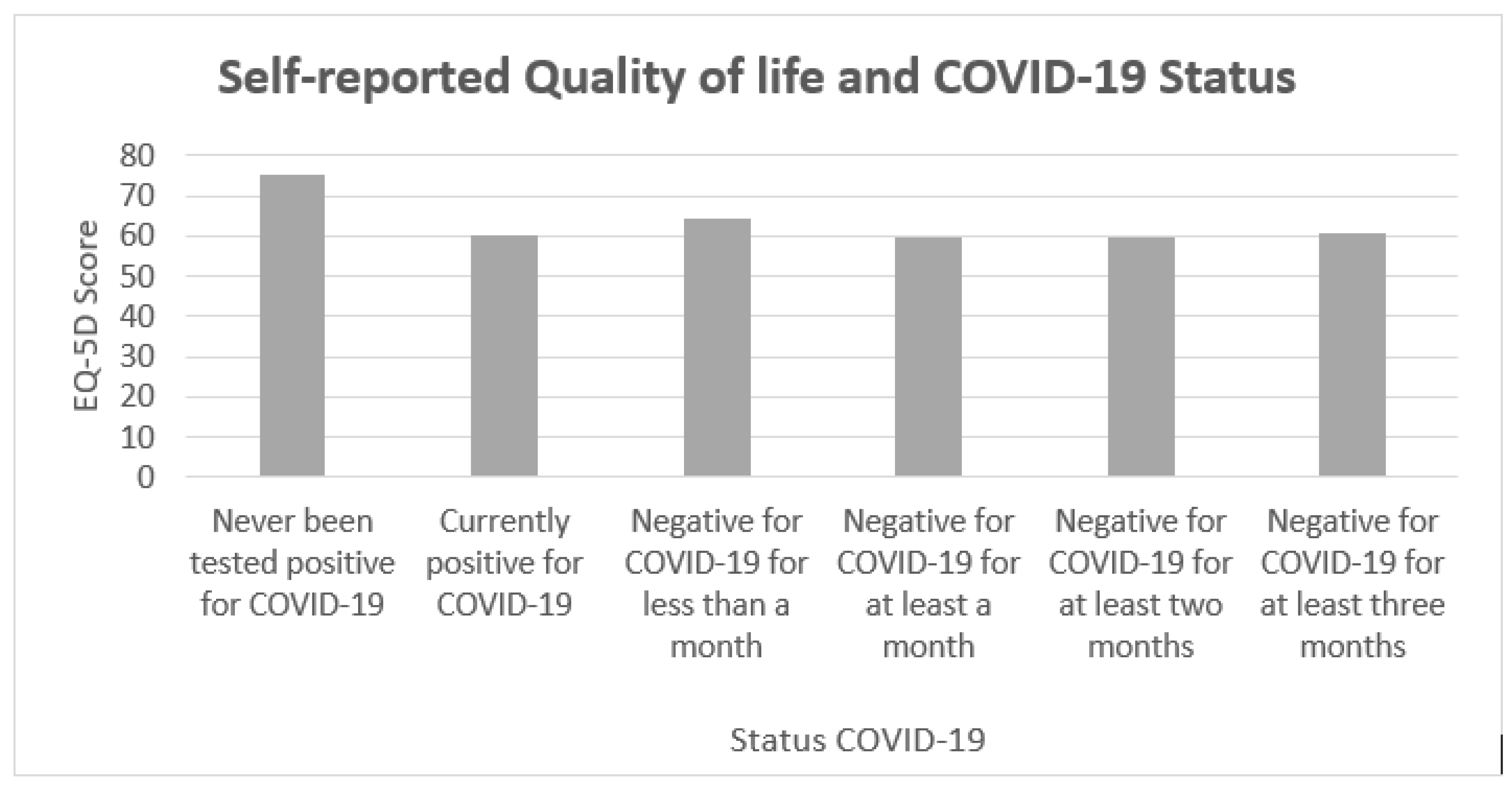
3.3. Long-COVID-19 Syndrome and Quality of Life
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baud, D.; Qi, X.; Nielsen-Saines, K.; Musso, D.; Pomar, L.; Favre, G. Real estimates of mortality following COVID-19 infection. Lancet Infect. Dis. 2020, 20, 773. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Kala, M.P.; Jafar, T.H. Factors associated with psychological distress during the coronavirus disease 2019 (COVID-19) pandemic on the predominantly general population: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0244630. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Correction to: Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 1294–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sivan, M.; Halpin, S.; Hollingworth, L.; Snook, N.; Hickman, K.; Clifton, I.J. Development of an integrated rehabilitation pathway for individuals recovering from COVID-19 in the community. J. Rehabil. Med. 2020, 52, jrm00089. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, I.; Rathore, F.A. Neurological manifestations and complications of COVID-19: A literature review. J. Clin. Neurosci. 2020, 77, 8–12. [Google Scholar] [CrossRef]
- Filatov, A.; Sharma, P.; Hindi, F.; Espinosa, P.S. Neurological Complications of Coronavirus Disease (COVID-19): Encephalopathy. Cureus 2020, 12, e7352. [Google Scholar] [CrossRef] [Green Version]
- Orrù, G.; Conversano, C.; Malloggi, E.; Francesconi, F.; Ciacchini, R.; Gemignani, A. Neurological complications of COVID-19 and possible neuroinvasion pathways: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 6688. [Google Scholar] [CrossRef]
- Orru, G.; Marzetti, F.; Conversano, C.; Vagheggini, G.; Miccoli, M.; Ciacchini, R.; Panait, E.; Gemignani, A. Secondary Traumatic Stress and Burnout in Healthcare Workers during COVID-19 Outbreak. Int J. Environ. Res. Public Health 2021, 18, 337. [Google Scholar] [CrossRef]
- Heath, C.; Sommerfield, A.; von Ungern-Sternberg, B.S. Resilience strategies to manage psychological distress among healthcare workers during the COVID-19 pandemic: A narrative review. Anaesthesia 2020, 75, 1364–1371. [Google Scholar] [CrossRef]
- Perrin, J.M.; Gnanasekaran, S.; Delahaye, J. Psychological aspects of chronic health conditions. Pediatr. Rev. 2012, 33, 99–109. [Google Scholar] [CrossRef]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, M.; Gemignani, A.; Conversano, C. Psychological resources against the traumatic experience of COVID-19. Clin. Neuropsychiatry 2020, 17, 85–87. [Google Scholar]
- Giusti, E.M.; Pedroli, E.; D’Aniello, G.E.; Stramba Badiale, C.; Pietrabissa, G.; Manna, C.; Stramba Badiale, M.; Riva, G.; Castelnuovo, G.; Molinari, E. The Psychological Impact of the COVID-19 Outbreak on Health Professionals: A Cross-Sectional Study. Front. Psychol. 2020, 11, 1684. [Google Scholar] [CrossRef]
- Orrù, G.; Rebecca, C.; Gemignani, A.; Conversano, C. Psychological intervention measures during the COVID-19 pandemic. Clin. Neuropsychiatry 2020, 17, 76–79. [Google Scholar] [CrossRef]
- Pandey, D.; Bansal, S.; Goyal, S.; Garg, A.; Sethi, N.; Pothiyill, D.I.; Sreelakshmi, E.S.; Sayyad, M.G.; Sethi, R. Psychological impact of mass quarantine on population during pandemics-The COVID-19 Lock-Down (COLD) study. PLoS ONE 2020, 15, e0240501. [Google Scholar] [CrossRef] [PubMed]
- Conversano, C.; Di Giuseppe, M.; Miccoli, M.; Ciacchini, R.; Gemignani, A.; Orrù, G. Mindfulness, age and gender as protective factors against psychological distress during Covid-19 pandemic. Front. Psychol. 2020, 11, 1900. [Google Scholar] [CrossRef]
- Spinelli, C.; Wisener, M.; Khoury, B. Mindfulness training for healthcare professionals and trainees: A meta-analysis of randomized controlled trials. J. Psychosom. Res. 2019, 120, 29–38. [Google Scholar] [CrossRef]
- Santacroce, L.; Bottalico, L.; Charitos, I.A. The Impact of COVID-19 on Italy: A Lesson for the Future. Int. J. Occup. Environ. Med. 2020, 11, 151–152. [Google Scholar] [CrossRef]
- Iasevoli, M.; Giantin, V.; Voci, A.; Valentini, E.; Zurlo, A.; Maggi, S.; Siviero, P.; Orru, G.; Crepaldi, G.; Pegoraro, R.; et al. Discussing end-of-life care issues with terminally ill patients and their relatives: Comparisons among physicians, nurses and psychologists. Aging Clin. Exp. Res. 2012, 24, 35–42. [Google Scholar]
- Marshall, M. The lasting misery of coronavirus long-haulers. Nature 2020, 585, 339–341. [Google Scholar] [CrossRef]
- Perego, E.; Callard, F.; Stras, L.; Melville-Jóhannesson, B.; Pope, R.; Alwan, N.A. Why the Patient-Made Term ‘Long Covid’ is needed. Wellcome Open Res. 2020, 5, 224. [Google Scholar] [CrossRef]
- Oronsky, B.; Larson, C.; Hammond, T.C.; Oronsky, A.; Kesari, S.; Lybeck, M.; Reid, T.R. A Review of Persistent Post-COVID Syndrome (PPCS). Clin. Rev. Allergy Immunol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Barillaro, C.; Bellieni, A.; Brandi, V.; Carfi, A.; D’Angelo, M.; Fusco, D.; Landi, G.; Lo Monaco, R.; Martone, A.M.; et al. The New Challenge of Geriatrics: Saving Frail Older People from the SARS-COV-2 Pandemic Infection. J. Nutr. Health Aging 2020, 24, 466–470. [Google Scholar] [CrossRef] [Green Version]
- Carfi, A.; Bernabei, R.; Landi, F.; Gemelli Against, C.-P.-A.C.S.G. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and Stress during COVID-19: Associations with Changes in Physical Activity, Sleep, Tobacco and Alcohol Use in Australian Adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Islam, M.S.; Ferdous, M.Z.; Islam, U.S.; Mosaddek, A.S.M.; Potenza, M.N.; Pardhan, S. Treatment, Persistent Symptoms, and Depression in People Infected with COVID-19 in Bangladesh. Int. J. Environ. Res. Public Health 2021, 18, 1453. [Google Scholar] [CrossRef]
- Kokou-Kpolou, C.K.; Megalakaki, O.; Laimou, D.L.; Kousouri, M. Insomnia during COVID-19 pandemic and lockdown: Prevalence, severity, and associated risk factors in French population. Psychiatry Res. 2020, 290, 113128. [Google Scholar] [CrossRef]
- Taboada, M.; Moreno, E.; Carinena, A.; Rey, T.; Pita-Romero, R.; Leal, S.; Sanduende, Y.; Rodriguez, A.; Nieto, C.; Vilas, E.; et al. Quality of life, functional status, and persistent symptoms after intensive care of COVID-19 patients. Br. J. Anaesth. 2021, 126, e110–e113. [Google Scholar] [CrossRef]
- Moreno-Perez, O.; Merino, E.; Leon-Ramirez, J.M.; Andres, M.; Ramos, J.M.; Arenas-Jimenez, J.; Asensio, S.; Sanchez, R.; Ruiz-Torregrosa, P.; Galan, I.; et al. Post-acute COVID-19 syndrome. Incidence and risk factors: A Mediterranean cohort study. J. Infect. 2021, 82, 378–383. [Google Scholar] [CrossRef]
- Garg, P.; Arora, U.; Kumar, A.; Wig, N. The “post-COVID” syndrome: How deep is the damage? J. Med. Virol. 2021, 93, 673–674. [Google Scholar] [CrossRef] [PubMed]
- Istituto Superiore Sanità. Sorveglianza Integrata COVID-19 in Italia. Published 2020. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Infografica_3giugno%20ITA.pdf (accessed on 8 June 2020).
- Mandal, S.; Barnett, J.; Brill, S.E.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; Hillman, T.E.; Jacob, J.; Jarvis, H.C.; et al. ‘Long-COVID’: A cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax 2020. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Fine, M.J.; Schulz, R.; Marrie, T.J.; Coley, C.M.; Kapoor, W.N.; Singer, D.E. Measuring symptomatic and functional recovery in patients with community-acquired pneumonia. J. Gen. Intern. Med. 1997, 12, 423–430. [Google Scholar] [CrossRef] [Green Version]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Group EuroQol. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Shah, W.; Hillman, T.; Playford, E.D.; Hishmeh, L. Managing the long term effects of covid-19: Summary of NICE, SIGN, and RCGP rapid guideline. BMJ 2021, 372, n136. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Bowe, B. High-dimensional characterization of post-acute sequalae of COVID-19. Nature 2021. [Google Scholar] [CrossRef] [PubMed]
- Mazza, C.; Orru, G.; Burla, F.; Monaro, M.; Ferracuti, S.; Colasanti, M.; Roma, P. Indicators to distinguish symptom accentuators from symptom producers in individuals with a diagnosed adjustment disorder: A pilot study on inconsistency subtypes using SIMS and MMPI-2-RF. PLoS ONE 2019, 14, e0227113. [Google Scholar] [CrossRef] [Green Version]
- Yarkoni, T.; Westfall, J. Choosing prediction over explanation in psychology: Lessons from machine learning. Perspect. Psychol. Sci. 2017, 12, 1100–1122. [Google Scholar] [CrossRef]




| Symptoms | Have You Ever Been Affected by COVID-19? | ||||||
|---|---|---|---|---|---|---|---|
| I’ve Never Been Tested Positive for COVID-19 | I Am Currently Positive for COVID-19 | I Had COVID-19 But Have Not Been Positive (Swab Result: Negative) for Less Than a Month | I Had COVID-19 But Have Not Been Positive (Swab Result: Negative) for at Least a Month | I Had COVID-19 But Have Not Been Positive (Swab Result: Negative) for at Least Two Months | I Had COVID-19 But Have Not Been Positive (Swab Result: Negative) for at Least Three Months | Other | |
| Shortness of breath (dyspnea) | 5 (15.15%) | 6 (30%) | 18 (26.47%) | 30 (40.54%) | 52 (33.77%) | 61 (40.13%) | 3 (50%) |
| Cough | 1 (3.03%) | 11 (55%) | 15 (22.06%) | 23 (31.08%) | 35 (22.73%) | 32 (21.05%) | 1 (16.67%) |
| Chest tightness | 4 (12.12%) | 9 (45%) | 16 (23.53%) | 21 (28.38%) | 38 (24.68%) | 48 (31.58%) | 3 (50%) |
| Chest pain | 0 (0%) | 6 (30%) | 13 (19.12%) | 19 (25.68%) | 31 (20.13%) | 40 (26.32%) | 3 (50%) |
| Palpitations | 4 (12.12%) | 10 (50%) | 32 (47.06%) | 37 (50%) | 60 (38.96%) | 59 (38.82%) | 2 (33.33%) |
| Headache | 12 (36.36%) | 18 (90%) | 36 (52.94%) | 40 (54.05) | 76 (49.35%) | 71 (46.71%) | 2 (33.33%) |
| Fatigue | 8 (24.24%) | 16 (80%) | 49 (72.06%) | 59 (79.73%) | 121 (78.57%) | 113 (74.34%) | 6 (100%) |
| Temperature | 0 (0%) | 6 (30%) | 12 (17.65%) | 9 (12.16%) | 19 (12.34%) | 29 (19.07%) | 1 (16.67%) |
| Cognitive impairment (brain fog, loss of concentration) | 5 (15.15%) | 8 (40%) | 32 (47.06%) | 44 (59.46%) | 73 (47.40%) | 74 (48.68%) | 6 (100%) |
| Tingling or numbness | 4 (12.12%) | 5 (25%) | 18 (26.47%) | 26 (35.14%) | 48 (31.17%) | 53 (34.87%) | 2 (33.33%) |
| Dizziness | 2 (6.06%) | 6 (30%) | 15 (22.06%) | 25 (33.78%) | 33 (21.43%) | 34 (22.37%) | 1 (16.67%) |
| Abdominal pain | 2 (6.06%) | 7 (35%) | 13 (19.12%) | 17 (22.97%) | 35 (22.73%) | 35 (23.03%) | 2 (33.33%) |
| Nausea | 2 (6.06%) | 9 (45%) | 13 (19.12%) | 19 (25.68%) | 30 (19.48%) | 31 (20.39%) | 3 (50%) |
| Diarrhea | 5 (15.15%) | 8 (40%) | 14 (20.59%) | 27 (36.49%) | 36 (23.38%) | 34 (22.37%) | 1 (16.67%) |
| Decreased or lack of appetite | 3 (9.09%) | 7 (35%) | 17 (25%) | 10 (13.61%) | 24 (15.58%) | 24 (15.79%) | 0 (0%) |
| Articular pains | 6 (18.18%) | 11 (55%) | 30 (44.12%) | 45 (60.81%) | 73 (47.40%) | 90 (59.21%) | 3 (50%) |
| Muscle aches (myalgia) | 4 (12.12%) | 14 (70%) | 39 (57.35%) | 44 (59.46%) | 81 (52.60%) | 93 (61.18%) | 5 (83.33%) |
| Depressive symptoms | 7 (21.21%) | 8 (49%) | 13 (19.12%) | 20 (27.03%) | 46 (29.87%) | 39 (25.66%) | 3 (50%) |
| Symptoms of anxiety | 11 (33.33%) | 10 (50%) | 31 (45.59%) | 28 (37.84%) | 62 (40.26%) | 52 (34.21%) | 2 (33.33%) |
| Earache | 4 (12.12%) | 4 (20%) | 12 (17.65%) | 10 (13.61%) | 24 (15.58%) | 15 (9.87%) | 0 (0%) |
| Expulsion of mucus or phlegm from the nose and/or mouth | 0 (0%) | 2 (10%) | 7 (10.29%) | 9 (12.16%) | 24 (15.58%) | 15 (9.87%) | 0 (0%) |
| Rhinitis (runny nose and nasal obstruction) | 3 (9.09%) | 5 (25%) | 7 (10.29%) | 15 (20.27%) | 28 (18.18%) | 18 (11.84%) | 1 (16.67%) |
| Sicca syndrome (the most common eye symptoms are dryness, foreign body and burning sensation) | 2 (6.06%) | 4 (20%) | 12 (17.65%) | 19 (25.68%) | 36 (23.38%) | 32 (21.05%) | 1 (16.67%) |
| Tinnitus (ringing in the ear) | 1 (3.03%) | 6 (30%) | 12 (17.65%) | 13 (17.57%) | 17 (11.04%) | 22 (14.47%) | 0 (0%) |
| Burning throat | 0 (0%) | 2 (10%) | 12 (17.65%) | 11 (14.86%) | 18 (11.69%) | 27 (17.76%) | 0 (0%) |
| Loss of taste | 1 (3.03%) | 9 (45%) | 16 (23.53%) | 21 (28.38%) | 39 (25.32%) | 41 (26.97%) | 2 (33.33%) |
| Loss of smell | 1 (3.03%) | 11 (55%) | 23 (33.82%) | 24 (32.43%) | 42 (27.27%) | 47 (30.92%) | 2 (33.33%) |
| Red eyes | 0 (0%) | 2 (10%) | 8 (11.76) | 16 (21.62%) | 21 (13.64%) | 24 (15.79%) | 0 (0%) |
| Skin rashes | 2 (6.06%) | 5 (25%) | 8 (11.76) | 6 (8.11%) | 26 (16.88%) | 28 (18.42%) | 1 (16.67%) |
| Vertigo | 2 (6.06%) | 4 (20%) | 9 (13.24%) | 13 (17.57%) | 22 (14.29%) | 20 (13.16%) | 1 (16.67%) |
| Anything | 13 (39.39%) | 0 (0%) | 3 (4.41%) | 0 (0%) | 3 (1.95%) | 4 (2.63%) | 0 (0%) |
| Other | 1 (3.03%) | 3 (15%) | 12 (17.65%) | 8 (10.81%) | 17 (11.04%) | 21 (13.82%) | 1 (16.67%) |
| Status Positivity COVID-19 | ISI Score |
|---|---|
| M (SD) | |
| Never been tested positive for COVID-19 | 8.67 (6.37) |
| Currently positive for COVID-19 | 11.85 (5.98) |
| Negative for COVID-19 for less than a month | 10.78 (5.48) |
| Negative for COVID-19 for at least a month | 12.81 (4.90) |
| Negative for COVID-19 for at least two months | 11.01 (5.86) |
| Negative for COVID-19 for at least three months | 11.38 (5.95) |
| Other | 14 (3.63) |
| T-Value Status COVID-19 | Never Been Tested Positive about COVID-19 |
|---|---|
| Currently positive for COVID-19 | 1.80 |
| Negative for COVID-19 for less than a month | 1.63 |
| Negative for COVID-19 for at least a month | 3.32 ** |
| Negative for COVID-19 for at least two months | 1.95 * |
| Negative for COVID-19 for at least three months | 2.24 * |
| Other | 1.98 |
| EQ-5D Scales | Severity | Status Positivity COVID-19 | ||||||
|---|---|---|---|---|---|---|---|---|
| Never Tested Positive for COVID-19 N (%) | Currently Positive for COVID-19 N (%) | Negative for COVID-19 for Less Than a Month N (%) | Negative for COVID-19 for at Least a Month N (%) | Negative for COVID-19 for at Least Two Months N (%) | Negative for COVID-19 for at Least Three Months N (%) | Other N (%) | ||
| Movement ability | No problem | 29 (87.88%) | 15 (75%) | 53 (77.94%) | 43 (58.11%) | 110 (71.43%) | 115 (75.66%) | 4 (66.67%) |
| Moderate Problems | 4 (12.12%) | 4 (20%) | 15 (22.06%) | 31 (41.89%) | 43 (27.92%) | 37 (24.34%) | 2 (33.33%) | |
| Serious problems | 0 (0%) | 1 (5%) | 0 (0%) | 0 (0%) | 1 (0.65%) | 0 (0%) | 0 (0%) | |
| Self-care | No problem | 30 (90.91%) | 18(90%) | 63 (92.65%) | 66 (89.19%) | 141 (91.56%) | 136 (89.47%) | 6 (100%) |
| Moderate Problems | 3 (9.09%) | 2 (10%) | 5 (7.35%) | 8 (10.81%) | 12 (7.79%) | 15 (9.87%) | 0 (0%) | |
| Serious problems | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (0.65%) | 1 (0.66%) | 0 (0%) | |
| Daily activities | No problem | 20 (60.61%) | 8 (40%) | 30 (44.12%) | 48 (64.86%) | 53 (34.41%) | 48 (31.58%) | 3 (50%) |
| Moderate Problems | 13 (39.39%) | 9 (45%) | 31 (45.59%) | 19 (25.68%) | 95 (61.69%) | 98 (64.47%) | 3 (50%) | |
| Serious problems | 0 (%) | 3 (15%) | 7 (10.29%) | 7 (9.46%) | 6 (3.90%) | 6 (3.95%) | 0 (0%) | |
| Pain, discomfort | No problem | 21 (63.64%) | 14 (70%) | 17 (25%) | 12 (16.22%) | 29 (18.83%) | 31 (20.39%) | 2 (33.33%) |
| Moderate Problems | 10 (30.30%) | 4 (20%) | 48 (70.59%) | 51 (68.92%) | 113 (73.38%) | 109 (71.71%) | 4 (66.67%) | |
| Serious problems | 2 (6.06%) | 2 (10%) | 3 (4.41%) | 11 (14.86%) | 12 (7.79%) | 12 (7.89%) | 0 (0%) | |
| Anxiety and/or Depression | No problem | 9 (27.27%) | 8 (40%) | 26 (38.24%) | 24 (32.43%) | 51 (33.12%) | 60 (39.47%) | 3 (50%) |
| Moderate Problems | 19 (57.58%) | 8 (40%) | 37 (54.41%) | 39 (52.70%) | 90 (58.44%) | 76 (50%) | 3 (50%) | |
| Serious problems | 5 (15.15%) | 4 (20%) | 5 (7.35%) | 11 (14.86%) | 13 (8.44%) | 16 (10.53%) | 0 (0%) | |
| Positivity for COVID-19 | EQ-5D Score |
|---|---|
| M (SD) | |
| Never been tested positive for COVID-19 | 75.54 (17.09) |
| Currently positive for COVID-19 | 60.45 (17.18) |
| Negative for COVID-19 for less than a month | 64.59 (18.88) |
| Negative for COVID-19 for at least a month | 59.85 (16.88) |
| Negative for COVID-19 for at least two months | 59.65 (16.52) |
| Negative for COVID-19 for at least three months | 60.85 (19.96) |
| Other | 60 (19.71) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orrù, G.; Bertelloni, D.; Diolaiuti, F.; Mucci, F.; Di Giuseppe, M.; Biella, M.; Gemignani, A.; Ciacchini, R.; Conversano, C. Long-COVID Syndrome? A Study on the Persistence of Neurological, Psychological and Physiological Symptoms. Healthcare 2021, 9, 575. https://doi.org/10.3390/healthcare9050575
Orrù G, Bertelloni D, Diolaiuti F, Mucci F, Di Giuseppe M, Biella M, Gemignani A, Ciacchini R, Conversano C. Long-COVID Syndrome? A Study on the Persistence of Neurological, Psychological and Physiological Symptoms. Healthcare. 2021; 9(5):575. https://doi.org/10.3390/healthcare9050575
Chicago/Turabian StyleOrrù, Graziella, Davide Bertelloni, Francesca Diolaiuti, Federico Mucci, Mariagrazia Di Giuseppe, Marco Biella, Angelo Gemignani, Rebecca Ciacchini, and Ciro Conversano. 2021. "Long-COVID Syndrome? A Study on the Persistence of Neurological, Psychological and Physiological Symptoms" Healthcare 9, no. 5: 575. https://doi.org/10.3390/healthcare9050575
APA StyleOrrù, G., Bertelloni, D., Diolaiuti, F., Mucci, F., Di Giuseppe, M., Biella, M., Gemignani, A., Ciacchini, R., & Conversano, C. (2021). Long-COVID Syndrome? A Study on the Persistence of Neurological, Psychological and Physiological Symptoms. Healthcare, 9(5), 575. https://doi.org/10.3390/healthcare9050575