
Identifying and Managing Suicidality in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome


Abstract
:1. Introduction
2. Risk Factors for Suicide
2.1. What Factors in Maria’s Background Place Her at Higher Risk of Suicidality (e.g., Ideation, Attempts, Completed Suicide) Than the General Population?
2.2. What Risk Factors Are Unique or More Prominent in Patients with ME/CFS Compared to Patients Affected by Other Conditions?
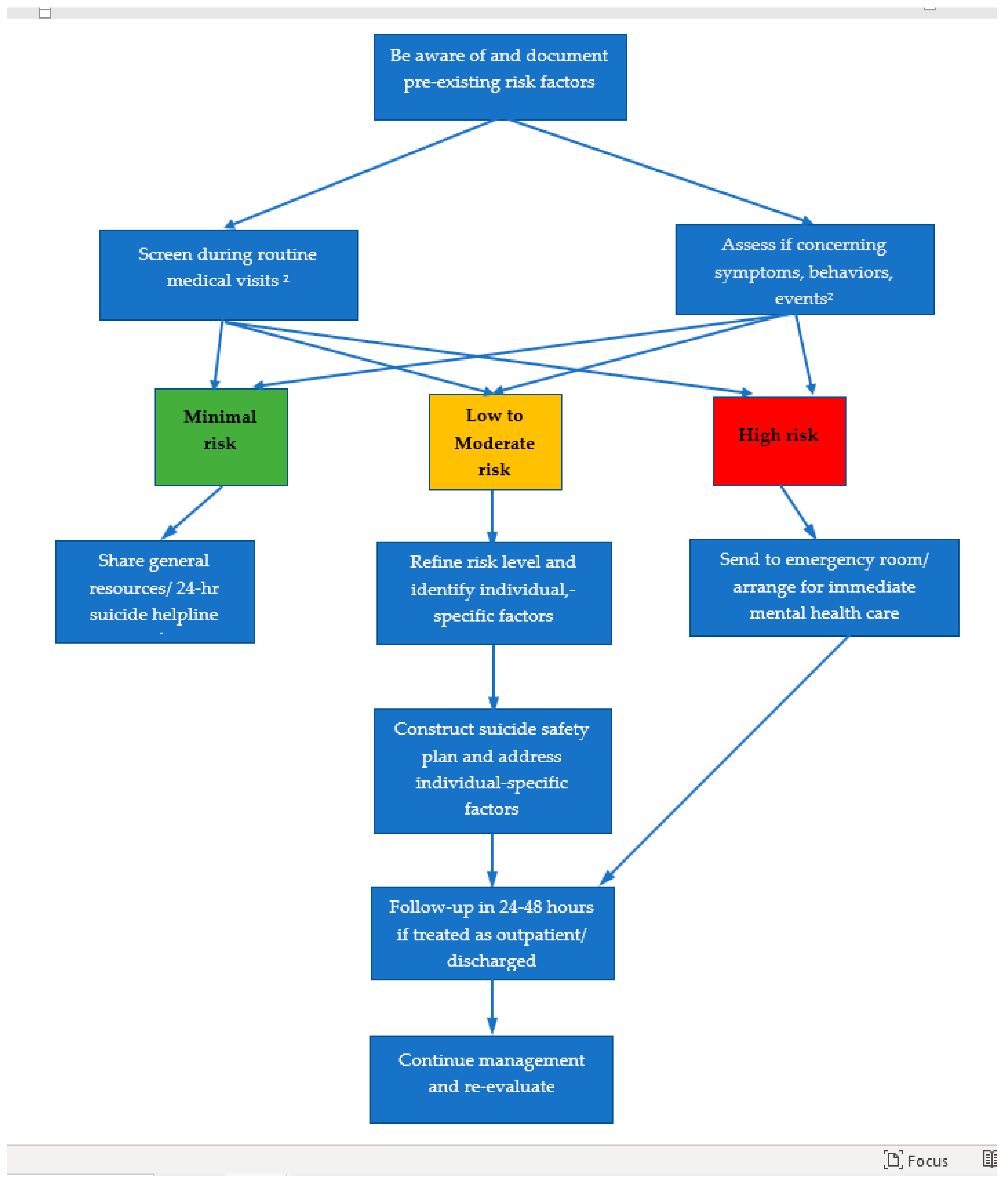
3. Initial Screening/Assessment of Suicide Risk: Is This Patient Currently at Risk of Suicide?
3.1. Who Should Be Assessed for Suicidality and When Should It Be Done?
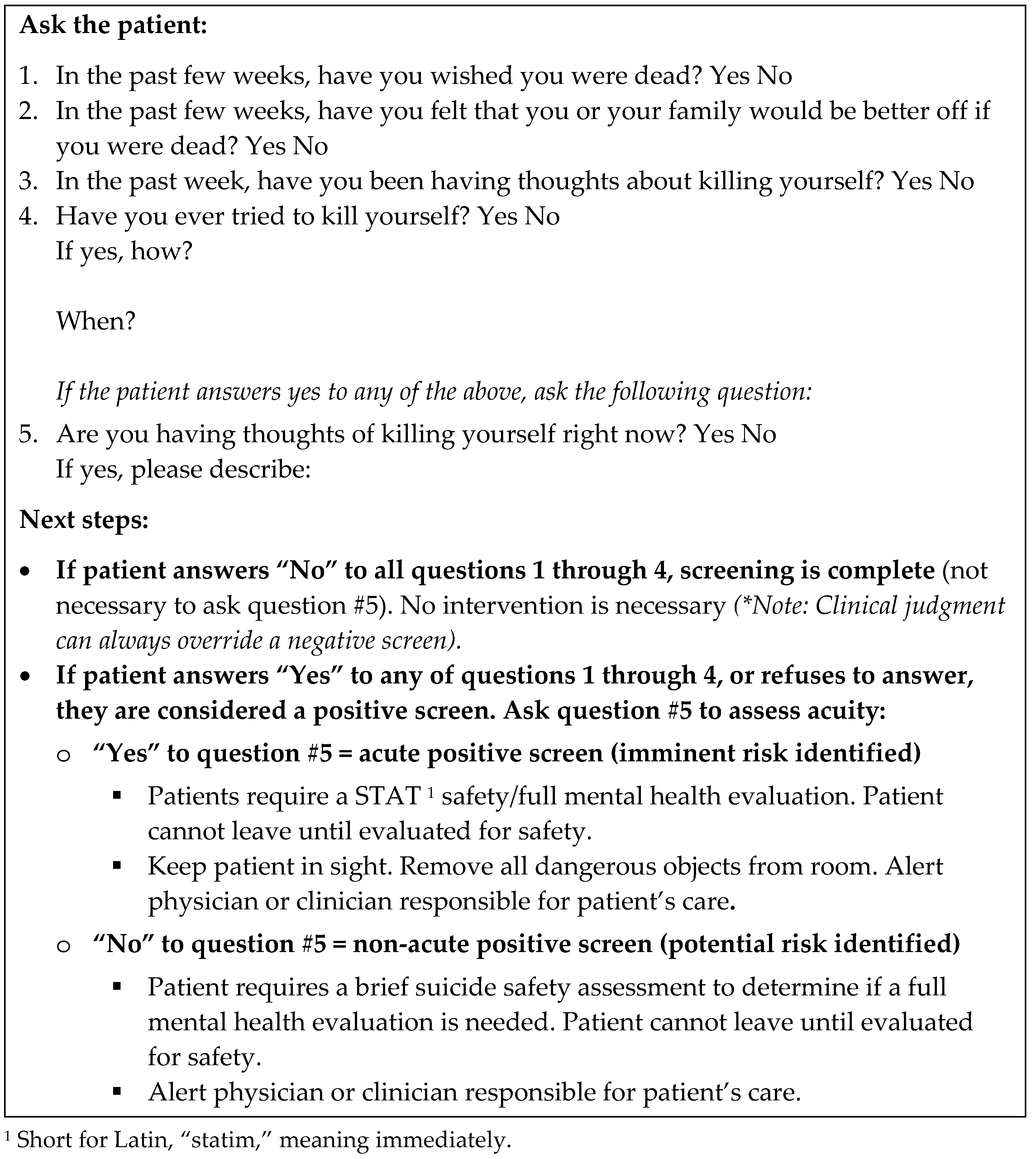
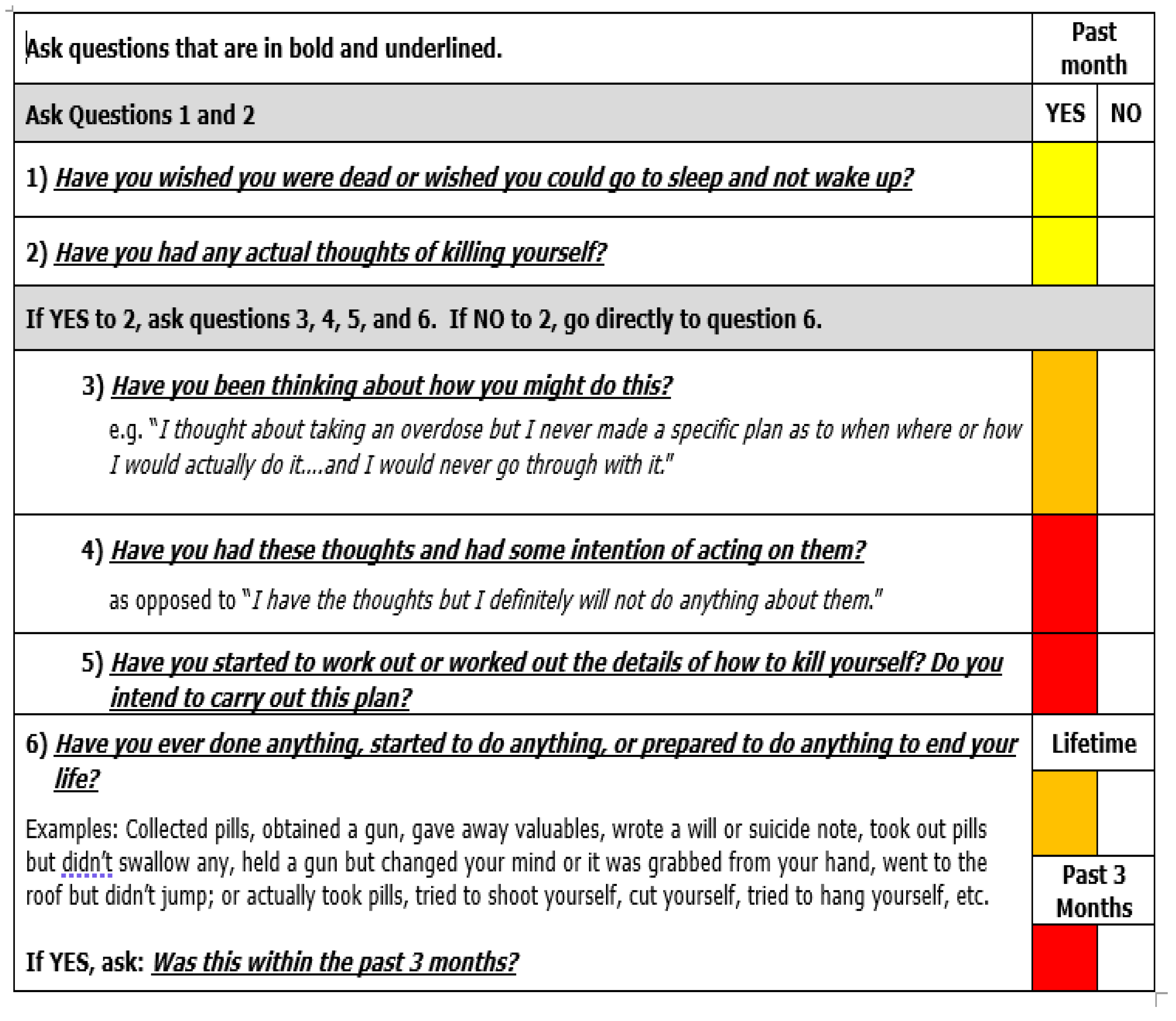
3.2. How Should Patients Be Screened or Assessed? What Issues Should Clinicians Pay Attention to or Ask about?
3.3. Why Should Clinicians Screen for Suicide Directly, Independent of Mood Disorders or Anxiety?
4. Secondary Assessment of Suicide
4.1. Is This Patient at Low, Moderate, or High Risk of Suicide?
4.2. How Can Risk Be Further Evaluated, Especially for Patients Deemed to Be at Moderate Risk?
5. Managing Suicidality
5.1. What Steps Would You Take Next? What Are Interventions All Suicidal Patients Should Receive?
5.2. What Are Individual-Specific Suicide Risk Factors? How Should They Be Addressed?
5.3. How Should Suicidal Patients Be Followed-Up?
6. Barriers, Gaps, and Opportunities
6.1. Research Barriers
6.2. Clinical Care Barriers
6.3. Societal Barriers
6.4. Emerging Opportunities
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Jason, L.A.; Richman, J.A.; Rademaker, A.W.; Jordan, K.M.; Plioplys, A.V.; Taylor, R.R.; McCready, W.; Huang, C.-F.; Plioplys, S. A Community-Based Study of Chronic Fatigue Syndrome. Arch. Intern. Med. 1999, 159, 2129–2137. [Google Scholar] [CrossRef] [Green Version]
- Dimmock, M.E.; Mirin, A.A.; Jason, L.A. Estimating the disease burden of ME/CFS in the United States and its relation to research funding. J. Med. 2016, 1. [Google Scholar] [CrossRef] [Green Version]
- Jason, L.; Mirin, A. Updating the National Academy of Medicine ME/CFS prevalence and economic impact figures to account for population growth and inflation. Fatigue Biomed. Health Behav. 2021, 9, 9–13. [Google Scholar] [CrossRef]
- Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining An Illness; Institute of Medicine (U.S.), Ed.; The National Academies Press: Washington, DC, USA, 2015; ISBN 9780309316897. [Google Scholar]
- Roberts, E.; Wessely, S.; Chalder, T.; Chang, C.-K.; Hotopf, M. Mortality of people with chronic fatigue syndrome: A retrospective cohort study in England and Wales from the South London and Maudsley NHS Foundation Trust Biomedical Research Centre (SLaM BRC) Clinical Record Interactive Search (CRIS) Register. Lancet 2016, 387, 1638–1643. [Google Scholar] [CrossRef] [Green Version]
- Ortiz, J.J.J. Depresión y Desesperanza en Personas Enfermas de Encefalomielitis Miálgica/Síndrome de Fatiga Crónica: Factores de Riesgo y de Protección; Facultad de Educación y Trabajo Social, Universidad de Valladolid: Valladolid, Spain, 2019. [Google Scholar]
- Carr, M.J.; Ashcroft, D.M.; White, P.D.; Kapur, N.; Webb, R.T. Prevalence of comorbid mental and physical illnesses and risks for self-harm and premature death among primary care patients diagnosed with fatigue syndromes. Psychol. Med. 2019, 50, 1156–1163. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, J.D.; Franklin, J.C.; Fox, K.R.; Bentley, K.H.; Kleiman, E.M.; Chang, B.P.; Nock, M.K. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: A meta-analysis of longitudinal studies. Psychol. Med. 2016, 46, 225–236. [Google Scholar] [CrossRef]
- Jason, L.A.; Corradi, K.; Gress, S.; Williams, S.; Torres-Harding, S. Causes of Death among Patients with Chronic Fatigue Syndrome. Health Care Women Int. 2006, 27, 615–626. [Google Scholar] [CrossRef]
- Bazalgette, L.; Bradley, W.; Ousbey, J. The Truth about Suicide. Available online: https://demosuk.wpengine.com/files/Suicide_-_web.pdf?1314370102 (accessed on 17 May 2021).
- Substance Abuse and Mental Health Services Administration. Results from the 2013 National Survey on Drug Use and Health: Mental Health Findings; NSDUH Series H-49, HHS Publication No. (SMA) 14-4887; Substance Abuse and Mental Health Services: Rockville, MD, USA, 2014. Available online: http://www.samhsa.gov/data/sites/default/files/NSDUHmhfr2013/NSDUHmhfr2013.pdf (accessed on 17 May 2021).
- Schulberg, H.C.; Bruce, M.L.; Lee, P.W.; Williams, J.W.; Dietrich, A.J. Preventing suicide in primary care patients: The primary care physician’s role. Gen. Hosp. Psychiatry 2004, 26, 337–345. [Google Scholar] [CrossRef] [PubMed]
- McManimen, S.L.; McClellan, D.; Stoothoff, J.; Jason, L.A. Effects of unsupportive social interactions, stigma, and symptoms on patients with myalgic encephalomyelitis and chronic fatigue syndrome. J. Community Psychol. 2018, 46, 959–971. [Google Scholar] [CrossRef] [PubMed]
- Geraghty, K.J.; Blease, C. Myalgic encephalomyelitis/chronic fatigue syndrome and the biopsychosocial model: A review of patient harm and distress in the medical encounter. Disabil. Rehabil. 2018, 41, 3092–3102. [Google Scholar] [CrossRef]
- Weber, A.N.; Michail, M.; Thompson, A.; Fiedorowicz, J.G. Psychiatric Emergencies. Med. Clin. N. Am. 2017, 101, 553–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmedani, B.K.; Peterson, E.L.; Hu, Y.; Rossom, R.C.; Lynch, F.; Lu, C.Y.; Waitzfelder, B.E.; Owen-Smith, A.A.; Hubley, S.; Prabhakar, D.; et al. Major Physical Health Conditions and Risk of Suicide. Am. J. Prev. Med. 2017, 53, 308–315. [Google Scholar] [CrossRef]
- Devendorf, A.R.; McManimen, S.L.; Jason, L.A. Suicidal ideation in non-depressed individuals: The effects of a chronic, misunderstood illness. J. Health Psychol. 2018, 25, 2106–2117. [Google Scholar] [CrossRef] [PubMed]
- McDowell, A.K.; Lineberry, T.W.; Bostwick, J.M. Practical Suicide-Risk Management for the Busy Primary Care Physician. Mayo Clin. Proc. 2011, 86, 792–800. [Google Scholar] [CrossRef] [Green Version]
- Probert-Lindström, S.; Berge, J.; Westrin, Å.; Öjehagen, A.; Pavulans, K.S. Long-term risk factors for suicide in suicide attempters examined at a medical emergency in patient unit: Results from a 32-year follow-up study. BMJ Open 2020, 10, e038794. [Google Scholar] [CrossRef] [PubMed]
- Government of Canada. S.C. Suicide among First Nations People, Métis and Inuit (2011–2016): Findings from the 2011 Canadian Census Health and Environment Cohort (CanCHEC). Available online: https://www150.statcan.gc.ca/n1/pub/99-011-x/99-011-x2019001-eng.htm (accessed on 17 May 2021).
- Grunbaum, J.A.; Kann, L.; Kinchen, S.; Ross, J.; Hawkins, J.; Lowry, R. Youth Risk Behavior Surveillance--United States, 2003. Psycextra Dataset 2004, 63, 1–168. [Google Scholar] [CrossRef] [PubMed]
- Movement Advancement Project Talking About Suicide & LGBT Populations. Available online: https://www.lgbtmap.org/talking-about-suicide-and-lgbt-populations (accessed on 10 March 2021).
- Pederson, C.L.; Brook, J.B. Sleep disturbance linked to suicidal ideation in postural orthostatic tachycardia syndrome. Nat. Sci. Sleep 2017, 9, 109–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen-Smith, A.A.; Ahmedani, B.K.; Peterson, E.; Simon, G.E.; Rossom, R.C.; Lynch, F.L.; Lu, C.Y.; Waitzfelder, B.E.; Beck, A.; DeBar, L.L.; et al. The mediating effect of sleep disturbance on the relationship between nonmalignant chronic pain and suicide death. Pain Pract. 2019, 19, 382–389. [Google Scholar] [CrossRef]
- Onyeka, I.N.; Maguire, A.; Ross, E.; O’Reilly, D. Does physical ill-health increase the risk of suicide? A census-based follow-up study of over 1 million people. Epidemiol. Psychiatr. Sci. 2020, 29, 140. [Google Scholar] [CrossRef]
- Karasouli, E.; Latchford, G.; Owens, D. The impact of chronic illness in suicidality: A qualitative exploration. Health Psychol. Behav. Med. 2013, 2, 899–908. [Google Scholar] [CrossRef] [Green Version]
- Jason, L.A.; Ohanian, D.; Brown, A.; Sunnquist, M.; McManimen, S.; Klebek, L.; Fox, P.; Sorenson, M. Differentiating multiple sclerosis from myalgic encephalomyelitis and chronic fatigue syndrome. Insights Biomed. 2017, 2, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kingdon, C.; Bowman, E.W.; Curran, H.; Nacul, L.; Lacerda, E.M. Functional status and well-being in people with myalgic encephalomyelitis/chronic fatigue syndrome compared with people with multiple sclerosis and healthy controls. Pharm. Open 2018, 2, 381–392. [Google Scholar] [CrossRef] [Green Version]
- Johnson, M.L.; Cotler, J.; Terman, J.M.; Jason, L.A. Risk factors for suicide in chronic fatigue syndrome. Death Stud. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- McManimen, S.L.; Devendorf, A.R.; Brown, A.A.; Moore, B.C.; Moore, J.H.; Jason, L.A. Mortality in patients with myalgic encephalomyelitis and chronic fatigue syndrome. Fatigue Biomed. Health Behav. 2016, 4, 195–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braden, J.B.; Sullivan, M.D. Suicidal Thoughts and Behavior among Adults with Self-Reported Pain Conditions in the National Comorbidity Survey Replication. J. Pain 2008, 9, 1106–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuller-Thomson, E.; Nimigon, J. Factors associated with depression among individuals with chronic fatigue syndrome: Findings from a nationally representative survey. Fam. Pract. 2008, 25, 414–422. [Google Scholar] [CrossRef] [Green Version]
- Kingdon, C.; Giotas, D.; Nacul, L.; Lacerda, E. Health care responsibility and compassion-visiting the housebound patient severely affected by ME/CFS. Healthcare 2020, 8, 197. [Google Scholar] [CrossRef]
- Strassheim, V.; Lambson, R.; Hackett, K.L.; Newton, J.L. What is known about severe and very severe chronic fatigue syndrome? A scoping review. Fatigue Biomed. Health Behav. 2017, 5, 167–183. [Google Scholar] [CrossRef]
- Chronic Fatigue Syndrome/Myalgic Encephalomyelitis. Primer for Clinical Practitioners. 2014 Edition. International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis. Available online: https://growthzonesitesprod.azureedge.net/wp-content/uploads/sites/1869/2020/10/Primer_Post_2014_conference.pdf (accessed on 17 May 2021).
- Bavington, J.; Darbishire, L.; White, P. Graded Exercise Therapy for CFS/ME; Version 7 (MREC Version 2; PACE Trial Management Group. 2004. Available online: https://me-pedia.org/images/8/89/PACE-get-therapist-manual.pdf (accessed on 17 May 2021).
- Geraghty, K.; Jason, L.; Sunnquist, M.; Tuller, D.; Blease, C.; Adeniji, C. The ’cognitive behavioural model’ of chronic fatigue syndrome: Critique of a flawed model. Health Psychol. Open 2019, 6, 6. [Google Scholar] [CrossRef]
- Wiborg, J.F.; Van Der Werf, S.; Prins, J.B.; Bleijenberg, G. Being homebound with chronic fatigue syndrome: A multidimensional comparison with outpatients. Psychiatry Res. 2010, 177, 246–249. [Google Scholar] [CrossRef]
- Bentall, R.P.; Powell, P.; Nye, F.J.; Edwards, R.H.T. Predictors of response to treatment for chronic fatigue syndrome. Br. J. Psychiatry 2002, 181, 248–252. [Google Scholar] [CrossRef] [Green Version]
- CDC. Improving Health and Quality of Life—Chronic Fatigue Syndrome (CFS). Available online: https://web.archive.org/web/20150905080404/http://www.cdc.gov/cfs/management/quality-of-life.html (accessed on 10 March 2021).
- Maksoud, R.; Du Preez, S.; Eaton-Fitch, N.; Thapaliya, K.; Barnden, L.; Cabanas, H.; Staines, D.; Marshall-Gradisnik, S. A systematic review of neurological impairments in myalgic encephalomyelitis/ chronic fatigue syndrome using neuroimaging techniques. PLoS ONE 2020, 15, e0232475. [Google Scholar] [CrossRef] [PubMed]
- Eaton-Fitch, N.; Du Preez, S.; Cabanas, H.; Staines, D.; Marshall-Gradisnik, S. A systematic review of natural killer cells profile and cytotoxic function in myalgic encephalomyelitis/chronic fatigue syndrome. Syst. Rev. 2019, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, G.; Manning, P.; Newton, J.L. Understanding Muscle Dysfunction in Chronic Fatigue Syndrome. J. Aging Res. 2016, 2016, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geraghty, K.; Hann, M.; Kurtev, S. Myalgic encephalomyelitis/chronic fatigue syndrome patients’ reports of symptom changes following cognitive behavioural therapy, graded exercise therapy and pacing treatments: Analysis of a primary survey compared with secondary surveys. J. Health Psychol. 2017, 24, 1318–1333. [Google Scholar] [CrossRef]
- McInnis, O.A.; Matheson, K.; Anisman, H. Living with the unexplained: Coping, distress, and depression among women with chronic fatigue syndrome and/or fibromyalgia compared to an autoimmune disorder. Anxiety Stress. Coping 2014, 27, 601–618. [Google Scholar] [CrossRef]
- Hvidberg, M.F.; Brinth, L.S.; Olesen, A.V.; Petersen, K.D.; Ehlers, L. The Health-Related Quality of Life for Patients with Myalgic Encephalomyelitis / Chronic Fatigue Syndrome (ME/CFS). PLoS ONE 2015, 10, e0132421. [Google Scholar] [CrossRef]
- Pederson, C.L.; Gorman-Ezell, K.; Mayer, G.H.; Brookings, J.B. Development and Preliminary Validation of a Tool for Screening Suicide Risk in Chronically Ill Women. Meas. Eval. Couns. Dev. 2021, 54, 130–140. [Google Scholar] [CrossRef]
- The Joint Commission. Detecting and treating suicide ideation in all settings. Sentin. Event Alert 2016, 56, 1–7. [Google Scholar]
- United States Preventive Services Taskforce. Recommendation: Suicide Risk in Adolescents, Adults and Older Adults: Screening. Available online: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/suicide-risk-in-adolescents-adults-and-older-adults-screening (accessed on 19 March 2021).
- Suicide Prevention: A Review and Policy Recommendations; CAMH. 2020. Available online: https://www.camh.ca/-/media/files/pdfs---public-policy-submissions/suicide-prevention-review-and-policy-recommendations-pdf.pdf?la=en&hash=A43E96FBFEFDEC87F40EB0E203D2A605323407E0 (accessed on 17 May 2021).
- Yawn, B.; Dietrich, A.; Wollan, P.; Bertram, S.; Kurland, M.; Pace, W.; Graham, D.; Huff, J. Immediate action protocol: A tool to help your practice assess suicidal patients. Fam. Pr. Manag. 2009, 16, 17. [Google Scholar]
- Snyder, D.J.; Ballard, E.; Stanley, I.H.; Ludi, E.; Kohn-Godbout, J.; Pao, M.; Horowitz, L.M. Patient Opinions About Screening for Suicide Risk in the Adult Medical Inpatient Unit. J. Behav. Health Serv. Res. 2017, 44, 364–372. [Google Scholar] [CrossRef] [PubMed]
- LeCloux, M.A.; Weimer, M.; Culp, S.L.; Bjorkgren, K.; Service, S.; Campo, J.V. The Feasibility and Impact of a Suicide Risk Screening Program in Rural Adult Primary Care: A Pilot Test of the Ask Suicide-Screening Questions Toolkit. J. Psychosom. Res. 2020, 61, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Pederson, C.L. The importance of screening for suicide risk in chronic invisible illness. J. Health Sci. Educ. 2018, 2, 141. [Google Scholar] [CrossRef]
- Busch, K.A.; Fawcett, J.; Jacobs, D.G. Clinical Correlates of Inpatient Suicide. J. Clin. Psychiatry 2003, 64, 14–19. [Google Scholar] [CrossRef]
- Dazzi, T.; Gribble, R.; Wessely, S.; Fear, N.T. Does asking about suicide and related behaviours induce suicidal ideation? What is the evidence? Psychol. Med. 2014, 44, 3361–3363. [Google Scholar] [CrossRef] [Green Version]
- Blades, C.A.; Stritzke, W.G.; Page, A.C.; Brown, J.D. The benefits and risks of asking research participants about suicide: A meta-analysis of the impact of exposure to suicide-related content. Clin. Psychol. Rev. 2018, 64, 1–12. [Google Scholar] [CrossRef]
- Common Characteristics of Suicide. Suicide & Crisis Center of North Texas. Available online: https://www.sccenter.org/facts-and-resources/common-characteristics-of-suicide/ (accessed on 23 March 2021).
- Firestone, L. Busting the Myths about Suicide. Available online: https://www.psychalive.org/busting-the-myths-about-suicide/ (accessed on 17 May 2021).
- KGO Second Chances: I Survived Jumping Off the Golden Gate Bridge. Available online: https://abc7news.com/2010562/ (accessed on 26 March 2021).
- Ortegren, A. Farewell—A Last Post from Anne Örtegren. Available online: https://www.healthrising.org/blog/2018/01/10/farewelll-last-post-anne-ortegren/ (accessed on 17 May 2021).
- Colby, J. False Allegations of Child Abuse in Cases of Childhood Myalgic Encephalomyelitis (ME). Available online: https://www.argumentcritique.com/uploads/1/0/3/1/10317653/colby_j.pdf (accessed on 17 May 2021).
- Neuropathology Report: Sophia Mirza. Available online: http://www.sophiaandme.org.uk/neuropathologicalreport.html (accessed on 19 March 2021).
- Ahmedani, B.K.; Vannoy, S. National Pathways for Suicide Prevention and Health Services Research. Am. J. Prev. Med. 2014, 47, S222–S228. [Google Scholar] [CrossRef] [Green Version]
- Elzinga, E.; De Kruif, A.J.T.C.M.; De Beurs, D.P.; Beekman, A.T.F.; Franx, G.; Gilissen, R. Engaging primary care professionals in suicide prevention: A qualitative study. PLoS ONE 2020, 15, e0242540. [Google Scholar] [CrossRef]
- Leavey, G.; Mallon, S.; Rondon-Sulbaran, J.; Galway, K.; Rosato, M.; Hughes, L. The failure of suicide prevention in primary care: Family and GP perspectives—A qualitative study. BMC Psychiatry 2017, 17, 369. [Google Scholar] [CrossRef] [Green Version]
- Horowitz, L.M.; Bridge, J.A.; Teach, S.J.; Ballard, E.; Klima, J.; Rosenstein, D.L.; Wharff, E.A.; Ginnis, K.; Cannon, E.; Joshi, P.; et al. Ask Suicide-Screening Questions (ASQ). Arch. Pediatr. Adolesc. Med. 2012, 166, 1170–1176. [Google Scholar] [CrossRef]
- Horowitz, L.M.; Snyder, D.J.; Boudreaux, E.D.; He, J.-P.; Harrington, C.J.; Cai, J.; Claassen, C.A.; Salhany, J.E.; Dao, T.; Chaves, J.F.; et al. Validation of the Ask Suicide-Screening Questions for Adult Medical Inpatients: A Brief Tool for All Ages. J. Psychosom. Res. 2020, 61, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Posner, K.; Brent, D.; Lucas, C.; Gould, M.; Stanley, B.; Brown, G.; Mann, J. Columbia-Suicide Severity Rating Scale (C.-SSRS); Columbia University Medical Center: New York, NY, USA, 2008; p. 10. [Google Scholar]
- NIMH. Adult Outpatient Brief Suicide Safety Assessment Worksheet. Available online: https://www.nimh.nih.gov/research/research-conducted-at-nimh/asq-toolkit-materials/adult-outpatient/adult-outpatient-brief-suicide-safety-assessment-worksheet.shtml (accessed on 24 March 2021).
- C-SSRS Training—English (USA) (Most Recent Version). Available online: https://www.youtube.com/watch?v=epTDFFv3uwc&list=PLZ6DpvOfzN1kV1F_lDw9-26JifBSDlIbF&index=2 (accessed on 23 March 2021).
- Greist, J.H.; Mundt, J.C.; Gwaltney, C.J.; Jefferson, J.W.; Posner, K. Predictive Value of Baseline Electronic Columbia–Suicide Severity Rating Scale (eC–SSRS) Assessments for Identifying Risk of Prospective Reports of Suicidal Behavior During Research Participation. Innov. Clin. Neurosci. 2014, 11, 23–31. [Google Scholar] [PubMed]
- Lukaschek, K.; Frank, M.; Halfter, K.; Schneider, A.; Gensichen, J. A Systematic Review of Brief Screeners for Suicidal Behaviour in Primary Care, 2019; in review.
- Druss, B.; Pincus, H. Suicidal Ideation and Suicide Attempts in General Medical Illnesses. Arch. Intern. Med. 2000, 160, 1522–1526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavanagh, J.T.O.; Carson, A.J.; Sharpe, M.; Lawrie, S.M. Psychological autopsy studies of suicide: A systematic review. Psychol. Med. 2003, 33, 395–405. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Viguera, A.C.; Milano, N.; Laurel, R.; Thompson, N.R.; Griffith, S.D.; Baldessarini, R.J.; Katzan, I.L. Comparison of Electronic Screening for Suicidal Risk With the Patient Health Questionnaire Item 9 and the Columbia Suicide Severity Rating Scale in an Outpatient Psychiatric Clinic. J. Psychosom. Res. 2015, 56, 460–469. [Google Scholar] [CrossRef]
- Hjelmeland, H.; Dieserud, G.; Dyregrov, K.; Knizek, B.L.; Leenaars, A.A. Psychological Autopsy Studies as Diagnostic Tools: Are they Methodologically Flawed? Death Stud. 2012, 36, 605–626. [Google Scholar] [CrossRef]
- Shahtahmasebi, S. Homicides and Suicides by Mentally Ill People. Sci. World J. 2003, 3, 684–693. [Google Scholar] [CrossRef] [Green Version]
- CDC More than a Mental Health Problem. Available online: https://www.cdc.gov/vitalsigns/suicide/index.html (accessed on 24 March 2021).
- Risk Assessment Page. Available online: https://cssrs.columbia.edu/documents/risk-assessment-page/ (accessed on 24 March 2021).
- Edemekong, P.F.; Bomgaars, D.L.; Sukumaran, S.; Levy, S.B. Activities of Daily Living; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The patient health questionnaire-2. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief measure for assessing generalized anxiety disorder. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, L.L.; Karabin, B.L.; Malone, A.C. Postural Orthostatic Tachycardia Syndrome (POTS): Assess, diagnose, and evaluate for POTS treatment (ADEPT). Integr. Med. Int. 2017, 4, 142–153. [Google Scholar] [CrossRef] [Green Version]
- Brown, G.K.; Jager-Hyman, S. Evidence-Based Psychotherapies for Suicide Prevention. Am. J. Prev. Med. 2014, 47, S186–S194. [Google Scholar] [CrossRef]
- Collaborative Assessment & Management of Suicidality (CAMS). About. Available online: https://cams-care.com/about-cams/ (accessed on 24 March 2021).
- Méndez-Bustos, P.; Calati, R.; Rubio-Ramírez, F.; Olié, E.; Courtet, P.; Lopez-Castroman, J. Effectiveness of psychotherapy on suicidal risk: A systematic review of observational studies. Front. Psychol. 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- National Action Alliance for Suicide Prevention, Transforming Health Systems Initiative Work Group. Recommended Standard Care for People with Suicide Risk: Making Health Care Suicide Safe. 2018. Available online: https://theactionalliance.org/sites/default/files/action_alliance_recommended_standard_care_final.pdf (accessed on 17 May 2021).
- Pavulans, K.S.; Bolmsjö, I.; Edberg, A.-K.; Öjehagen, A. Being in want of control: Experiences of being on the road to, and making, a suicide attempt. Int. J. Qual. Stud. Health Well-Being 2012, 7, 16288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanley, B.; Brown, G.K. Safety Planning Intervention: A Brief Intervention to Mitigate Suicide Risk. Cogn. Behav. Pr. 2012, 19, 256–264. [Google Scholar] [CrossRef]
- Moscardini, E.H.; Hill, R.M.; Dodd, C.G.; Do, C.; Kaplow, J.B.; Tucker, R.P. Suicide Safety Planning: Clinician Training, Comfort, and Safety Plan Utilization. Int. J. Environ. Res. Public Health 2020, 17, 6444. [Google Scholar] [CrossRef]
- CALM: Counseling on Access to Lethal Means | Suicide Prevention Resource Center. Available online: https://www.sprc.org/resources-programs/calm-counseling-access-lethal-means (accessed on 24 March 2021).
- Stanley, B.; Brown, G.K.; Brenner, L.A.; Galfalvy, H.; Currier, G.W.; Knox, K.L.; Chaudhury, S.R.; Bush, A.L.; Green, K.L. Comparison of the Safety Planning Intervention With Follow-up vs Usual Care of Suicidal Patients Treated in the Emergency Department. JAMA Psychiatry 2018, 75, 894–900. [Google Scholar] [CrossRef]
- Rudd, M.D.; Mandrusiak, M.; Joiner, T.E., Jr. The case against no-suicide contracts: The commitment to treatment statement as a practice alternative. J. Clin. Psychol. 2005, 62, 243–251. [Google Scholar] [CrossRef]
- Stein, E. Psychiatric conditions comorbid with myalgic encephalomyelitis and/or fibromyalgia. Psychiatr. Times 2013, 30, 14. [Google Scholar]
- Chu, L.; Valencia, I.J.; Garvert, D.W.; Montoya, J.G. Onset patterns and course of myalgic encephalomyelitis/chronic fatigue syndrome. Front. Pediatr. 2019, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Stein, E. Assessment and treatment of patients with ME/CFS: Clinical guidelines for psychiatrists. Hentet 2005, 11, 13. [Google Scholar]
- Cuijpers, P.; Quero, S.; Dowrick, C.; Arroll, B. Psychological treatment of depression in primary care: Recent developments. Curr. Psychiatry Rep. 2019, 21, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dis, E.A.M.; Van Veen, S.C.; Hagenaars, M.A.; Batelaan, N.M.; Bockting, C.L.H.; Heuvel, R.M.V.D.; Cuijpers, P.; Engelhard, I.M. Long-term Outcomes of Cognitive Behavioral Therapy for Anxiety-Related Disorders. JAMA Psychiatry 2020, 77, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Mohr, D.C.; Ho, J.; Duffecy, J.; Reifler, D.; Sokol, L.; Burns, M.N.; Jin, L.; Siddique, J. Effect of Telephone-Administered vs Face-to-face Cognitive Behavioral Therapy on Adherence to Therapy and Depression Outcomes Among Primary Care Patients. JAMA 2012, 307, 2278–2285. [Google Scholar] [CrossRef]
- Marshall, R.; Paul, L.; McFadyen, A.K.; Rafferty, D.; Wood, L. Pain Characteristics of People with Chronic Fatigue Syndrome. J. Musculoskelet. Pain 2010, 18, 127–137. [Google Scholar] [CrossRef]
- Carruthers, B.M.; Jain, A.K.; De Meirleir, K.L.; Peterson, D.L.; Klimas, N.G.; Lerner, A.M.; Bested, A.C.; Flor-Henry, P.; Joshi, P.; Powles, A.C.P.; et al. Myalgic encephalomyelitis/chronic fatigue syndrome. J. Chronic Fatigue Syndr. 2003, 11, 7–115. [Google Scholar] [CrossRef]
- Stein, E.; Stormorken, E.; Karlsson, B. How to Improve Therapeutic Encounters between Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Health Care Practitioners. Available online: https://s3.amazonaws.com/kajabi-storefronts-production/sites/90617/themes/1534791/downloads/4t2GsiASLGVtbwaM1qDc_Improving-Therapeutic-Relationships.pdf (accessed on 17 May 2021).
- Brodsky, B.S.; Spruch-Feiner, A.; Stanley, B. The Zero Suicide model: Applying evidence-based suicide prevention practices to clinical care. Front. Psychiatry 2018, 9, 33. [Google Scholar] [CrossRef] [Green Version]
- Luxton, D.D.; June, J.D.; Comtois, K.A. Can Postdischarge Follow-Up Contacts Prevent Suicide and Suicidal Behavior? Crisis 2013, 34, 32–41. [Google Scholar] [CrossRef]
- National Action Alliance for Suicide Prevention. Best Practices in Care Transitions for Individuals with Suicide Risk: Inpatient Care to Outpatient Care; Education Development Center, Inc.: Washington, DC, USA, 2019. [Google Scholar]
- Chung, D.; Hadzi-Pavlovic, D.; Wang, M.; Swaraj, S.; Olfson, M.; Large, M. Meta-analysis of suicide rates in the first week and the first month after psychiatric hospitalisation. BMJ Open 2019, 9, e023883. [Google Scholar] [CrossRef] [Green Version]
- Richards, J.E.; Whiteside, U.; Ludman, E.J.; Pabiniak, C.; Kirlin, B.; Hidalgo, R.; Simon, G. Understanding why patients may not report suicidal ideation at a health care visit prior to a suicide attempt: A qualitative study. Psychiatr. Serv. 2019, 70, 40–45. [Google Scholar] [CrossRef]
- Sudol, K.; Mann, J.J. Biomarkers of suicide attempt behavior: Towards a biological model of risk. Curr. Psychiatry Rep. 2017, 19, 31. [Google Scholar] [CrossRef] [PubMed]
- CDC. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Available online: https://www.cdc.gov/me-cfs/index.html (accessed on 25 March 2021).
- US ME/CFS Clinician Coalition Diagnosing and Treating Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). 2020. Available online: https://batemanhornecenter.org/wp-content/uploads/filebase/Diagnosing-and-Treating-MECFS-Handout-V2.pdf (accessed on 5 March 2021).
- Roaten, K.; Johnson, C.; Genzel, R.; Khan, F.; North, C.S. Development and implementation of a universal suicide risk screening program in a safety-net hospital system. Jt. Comm. J. Qual. Patient Saf. 2018, 44, 4–11. [Google Scholar] [CrossRef]
- National Alliance on Mental Illness. Understanding Health Insurance, What Is Mental Health Parity? Available online: https://www.nami.org/Your-Journey/Individuals-with-Mental-Illness/Understanding-Health-Insurance/What-is-Mental-Health-Parity. (accessed on 25 March 2021).
- Mental Health Parity in the US: Have We Made Any Real Progress? Available online: https://www.psychiatrictimes.com/view/mental-health-parity-in-the-us-have-we-made-any-real-progress (accessed on 25 March 2021).
- Canadian Mental Health Association. Mental Health in the Balance: Ending the Health Care Disparity in Canada; Canadian Mental Health Association: Toronto, ON, Canada, 2018. [Google Scholar]
- Mental Health Action Plan: Better Access and System Performance for Mental Health Services in Canada. Available online: https://cmha.ca/news/mental-health-action-plan-better-access-and-system-performance-for-mental-health-services-in-canada (accessed on 25 March 2021).
- The Right Way to Avoid Malpractice Lawsuits. Available online: https://www.psychiatrictimes.com/view/the-right-way-to-avoid-malpractice-lawsuits (accessed on 25 March 2021).
- Zonana, J.; Simberlund, J.; Christos, P.; Information, R. The impact of safety plans in an outpatient clinic. Crisis 2018, 39, 304–309. [Google Scholar] [CrossRef]
- Murphy, C. Gun Laws Are the Key to Addressing America’s Suicide Crisis. Available online: https://www.theatlantic.com/ideas/archive/2020/09/gun-control-key-addressing-americas-suicide-crisis/615889/ (accessed on 25 March 2021).
- Barnhorst, A. Opinion. In The Empty Promise of Suicide Prevention; The New York Times: New York, NY, USA, 2019. [Google Scholar]
- Cherkis, J. Opinion. In What Happens to Your Mental Health When You Can’t Pay Your Rent? The New York Times: New York, NY, USA, 2021. [Google Scholar]
- Reckrey, J.M.; DeCherrie, L.V.; Dugue, M.; Rosen, A.; Soriano, T.A.; Ornstein, K.A. Meeting the Mental Health Needs of the Homebound: A Psychiatric Consult Service Within a Home-Based Primary Care Program. Care Manag. J. 2015, 16, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Pozzilli, C.; Brunetti, M.; Amicosante, A.M.V.; Gasperini, C.; Ristori, G.; Palmisano, L.; Battaglia, M. Home based management in multiple sclerosis: Results of a randomised controlled trial. J. Neurol. Neurosurg. Psychiatry 2002, 73, 250–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watts, S.; Newby, J.M.; Mewton, L.; Andrews, G. A clinical audit of changes in suicide ideas with internet treatment for depression. BMJ Open 2012, 2, e001558. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.D.; Andrews, G. The Effectiveness of Internet Cognitive Behavioural Therapy (iCBT) for Depression in Primary Care: A Quality Assurance Study. PLoS ONE 2013, 8, e57447. [Google Scholar] [CrossRef] [Green Version]
- Charova, E.; Dorstyn, D.; Tully, P.; Mittag, O. Web-based interventions for comorbid depression and chronic illness: A systematic review. J. Telemed. Telecare 2015, 21, 189–201. [Google Scholar] [CrossRef]
- Miller, I.W.; Camargo, C.A.; Arias, S.A.; Sullivan, A.F.; Allen, M.H.; Goldstein, A.B.; Manton, A.P.; Espinola, J.A.; Jones, R.; Hasegawa, K.; et al. Suicide Prevention in an Emergency Department Population. JAMA Psychiatry 2017, 74, 563–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Potentially Modifiable | Non-Modifiable |
|---|---|
| Chronic, serious illness 1 Sleep disturbances/problems Pain Other severe symptoms (e.g., cognitive dysfunction, hypersensitivity to stimuli) Depression Anxiety Substance Abuse Other comorbid medical conditions (e.g., fibromyalgia, orthostatic intolerance syndromes) Low quality of life Limited function 1 Social isolation, loneliness 1 Lack of supportive relationships 1 Thwarted belongingness 1 Unstable, challenging social circumstances (e.g., homelessness, poverty, unemployment) 1 Unsupportive social and healthcare provider interactions 1 Lack of/poor coping skills Personal beliefs | Older age Male sex Caucasian Native American/Alaskan Native background Identifying as LGBTQ 2 History of self-harm History of suicide attempts Recently discharged from inpatient psychiatric care Personality disorder Past traumatic events (e.g., adverse childhood experiences, sexual abuse, domestic violence) Family history of suicide, mental health disorder Exposure to other people who have committed suicide |
| Statements |
| Passive suicidal ideation: “I wish I could go to sleep one day and not wake up.” |
| Active suicide ideation: “I am tired of living and looking for a way out.” |
| Depression: “I feel sad/cry all the time.” |
| Feeling like a burden to family/others: “My family would be better off if I were dead.” |
| Hopelessness: “I have nothing to look forward to.” “Life is meaningless.” |
| Loneliness: “There is no one I can talk to about my problems.” “I don’t have any friends.” |
| Symptoms |
| Changes in mood, including onset/exacerbation of depression anxiety; dramatic fluctuations |
| Worsening somatic symptoms, especially pain and insomnia |
| Anger, irritability |
| Behaviors |
| Agitated actions: pacing, shaking, rapid/loud speech |
| Impulsive behaviors |
| Withdrawal from care: stopping treatments, missing appointments, avoiding contact |
| Repetitive self-harm |
| Drinking or abusing other substances more than usual |
| Decreasing social contact |
| Giving away items which are important/meaningful to patient |
| Ceasing activities previously enjoyed |
| Events |
| Unemployment |
| Loss of significant relationships (e.g., divorce, death of loved one) |
| Denial of disability benefits |
| Homelessness |
| Anticipated treatment is not effective |
| Recent suicide attempt |
| Recent discharge from inpatient/outpatient psychiatric care |
| Potentially Modifiable | Non-Modifiable |
|---|---|
| Religious background/personal beliefs | Younger age |
| Positive coping behaviors | Female Sex |
| Strong relationships | Having children |
| Stable social circumstances (e.g., financial status, housing) | Marriage |
| Supportive clinical interactions | Pregnancy |
| Component | Ask Patient | Example Answers | Comment |
|---|---|---|---|
| 1. Warning signs | How will you know when the safety plan should be used? | “Feeling hopeless.” “Thinking life is all downhill from here.” “Lying in bed more than usual.” | Thoughts, behaviors, moods, events that lead to suicidality. |
| 2. Internal strategies | What activities can you do on your own if you become suicidal again, to help yourself not to act on your thoughts or urges? | Sit outside in the sun, listen to relaxing music, take a warm bath. | |
| 3. People and settings that provide distraction | Who helps you take your mind off your problems at least for a little while? Where can you go where you will be around people in a safe environment? | Knitting group, the park near my home, online patient support group. | People named need not know about the patient’s suicidal feelings. Places may allow casual interactions. |
| 4. People whom I can contact for help | Who is supportive of you and who do you feel that you can talk with when you are under stress? | My neighbor Sarah, my church’s pastor. | These are people who are aware of or could be trusted with the individual’s suicidal thoughts/feelings. |
| 5. Professionals and agencies I can call in a crisis | Who are the medical/mental health professionals that we should identify to be on your safety plan? | Springfield Emergency Room, my psychiatrist Dr Joseph Lopez, National Suicide Prevention Lifeline, 911 | List contact information. |
| 6. Making the environment safe | What items do you have around you that you might use to hurt/kill yourself? How can we make your surroundings safe for you? | Doctor/pharmacy will limit number of medications mailed to one week at a time. Place kitchen knives in locked cabinet. | Always ask about firearms. Means restriction should be matched to the methods the individual names. |
| 7. My reasons for living 1 | What makes your life worth living? What brings joy to your life? | My children, my faith, my pets, enjoying nature. |
| Category | Examples of Specific Factor | Examples of Interventions | Comments |
|---|---|---|---|
| ME/CFS 1 symptoms | Sleep Pain | Cognitive behavioral therapy—insomnia Blue light filters Exposure to natural light 2 Amitriptyline 3 Trazodone 3 Re-positioning Massage Heat/ice Gabapentin 3 Tricyclic antidepressant 3 | Evaluate for pain and sleep conditions with specific treatments (e.g., obstructive sleep apnea, migraine). |
| Comorbid psychiatric conditions | Major depressive disorder | Referral to mental health professional CBT 4 Citalopram 3 Venlafaxine 3 | |
| Comorbid medical conditions | Multiple chemical sensitivity Postural orthostatic tachycardia syndrome (POTS) | Avoid/reduce exposure to concerning stimuli Isotonic fluids, support hose, awareness/prevention of exacerbating factors, recumbent exercises, fluoxetine 3 | Exercise may not be suitable for many patients. If used, start at a low level and continue/increase only if patient tolerates. |
| Isolation/loneliness/social support | Healthcare professionals Family/caregiver Community support | Validation of patient experience Reflective listening Caring contacts Educate about ME/CFS Educate about caregiver stress In-person activity/support groups Electronic forums specific for ME/CFS Virtual support groups | Caring contacts are brief, intermittent e-mails, cards, phone calls to patients by staff between visits. Caregivers need respite/support to provide support. |
| Functional Limitations | Ambulation Bathing | Refer to physical therapy Bedside commode Wheelchair Refer to occupational therapy Hand-held shower head Shower chair | |
| Other Support | Poverty Homelessness | Food banks, vouchers Apply for disability financial support Home-sharing/roommate arrangements Government-supported housing vouchers | Clinic/facility-based medical social workers can help patients find and apply for programs. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, L.; Elliott, M.; Stein, E.; Jason, L.A. Identifying and Managing Suicidality in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Healthcare 2021, 9, 629. https://doi.org/10.3390/healthcare9060629
Chu L, Elliott M, Stein E, Jason LA. Identifying and Managing Suicidality in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Healthcare. 2021; 9(6):629. https://doi.org/10.3390/healthcare9060629
Chicago/Turabian StyleChu, Lily, Meghan Elliott, Eleanor Stein, and Leonard A. Jason. 2021. "Identifying and Managing Suicidality in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome" Healthcare 9, no. 6: 629. https://doi.org/10.3390/healthcare9060629
APA StyleChu, L., Elliott, M., Stein, E., & Jason, L. A. (2021). Identifying and Managing Suicidality in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Healthcare, 9(6), 629. https://doi.org/10.3390/healthcare9060629