
A Prospective Comparative Study of Mastication Predominance and Masticatory Performance in Kennedy Class I Patients


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Maximum Occlusal Force (MOF)
2.3. Test Food
2.4. Objective Evaluation of Mastication Predominance
2.5. Objective Evaluation of Masticatory Performance
2.6. Statistical Analysis
- Evaluation of the difference of the subject profiles: differences in age, the period required for second measurement after RPD delivery, the number of posterior occlusal supports, and MOF between KC I D+ and KC I D− (Mann–Whitney U test)
- Comparison of the initial MPI among HD, KC I D+, and D− without RPD (before RPD treatment: pre-MPI): differences among HD-MPI, pre-MPI in KC I D+, and KC I D− (Kruskal–Wallis with multiple comparison)
- Comparison of the initial masticatory performance among HD, KC I D+, and D− without RPD (before RPD treatment: pre-masticatory performance): differences among HD-masticatory performance, pre-masticatory performance in KC I D+, and KC I D− (Kruskal–Wallis with multiple comparison)
- Evaluation of the effect of RPD treatment on MPI: differences between pre-MPI and post-MPI in KC I D+ and KC I D−, respectively (Wilcoxon signed-rank test)
- Evaluation of the effect of RPD treatment on masticatory performance: difference between pre- and post-masticatory performance in KC I D+ and KC I D−, respectively (Wilcoxon signed-rank test)
- Comparison of MPI among HD, KC I D+, and D− with RPD (after RPD treatment: post-MPI): difference in among HD-MPI, post-MPI in KC I D+, and KC I D− (Kruskal–Wallis with multiple comparison)
- Comparison of masticatory performance among HD, KC I D+, and D− with RPD (after RPD treatment: post-masticatory performance): difference in post-masticatory performance among HD-masticatory performance, post-masticatory performance in KC I D+, and KC I D− (Kruskal–Wallis with multiple comparison)
3. Results
3.1. Subjects
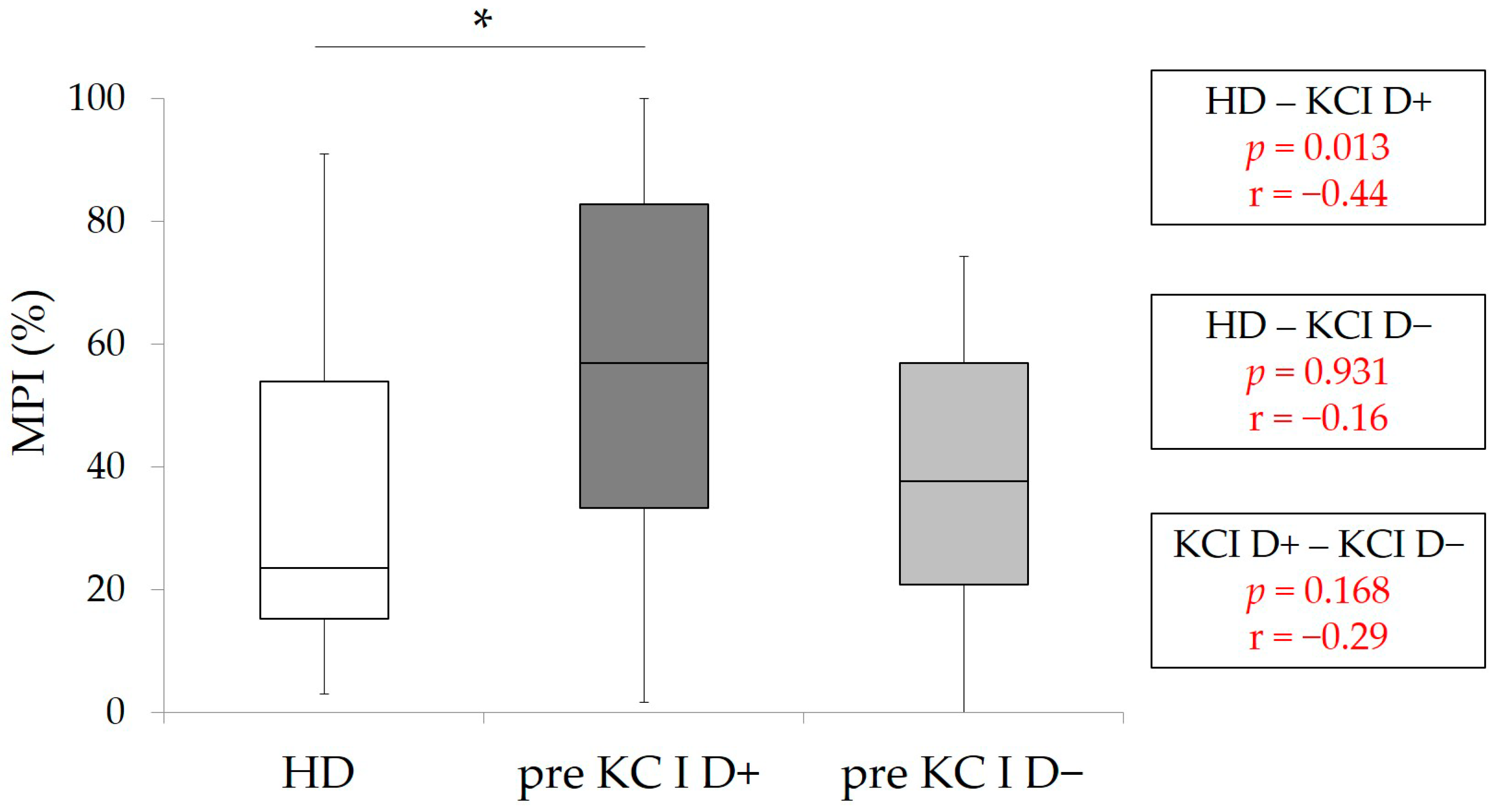
3.2. Comparisons of MPI and Masticatory Performance among the Patients in Pre-KC I (D+ and D−) and HD
3.3. Comparisons of MPI and Masticatory Performance in Patients with KC I (D+ and D−) between Pre- and Post-RPD Treatment
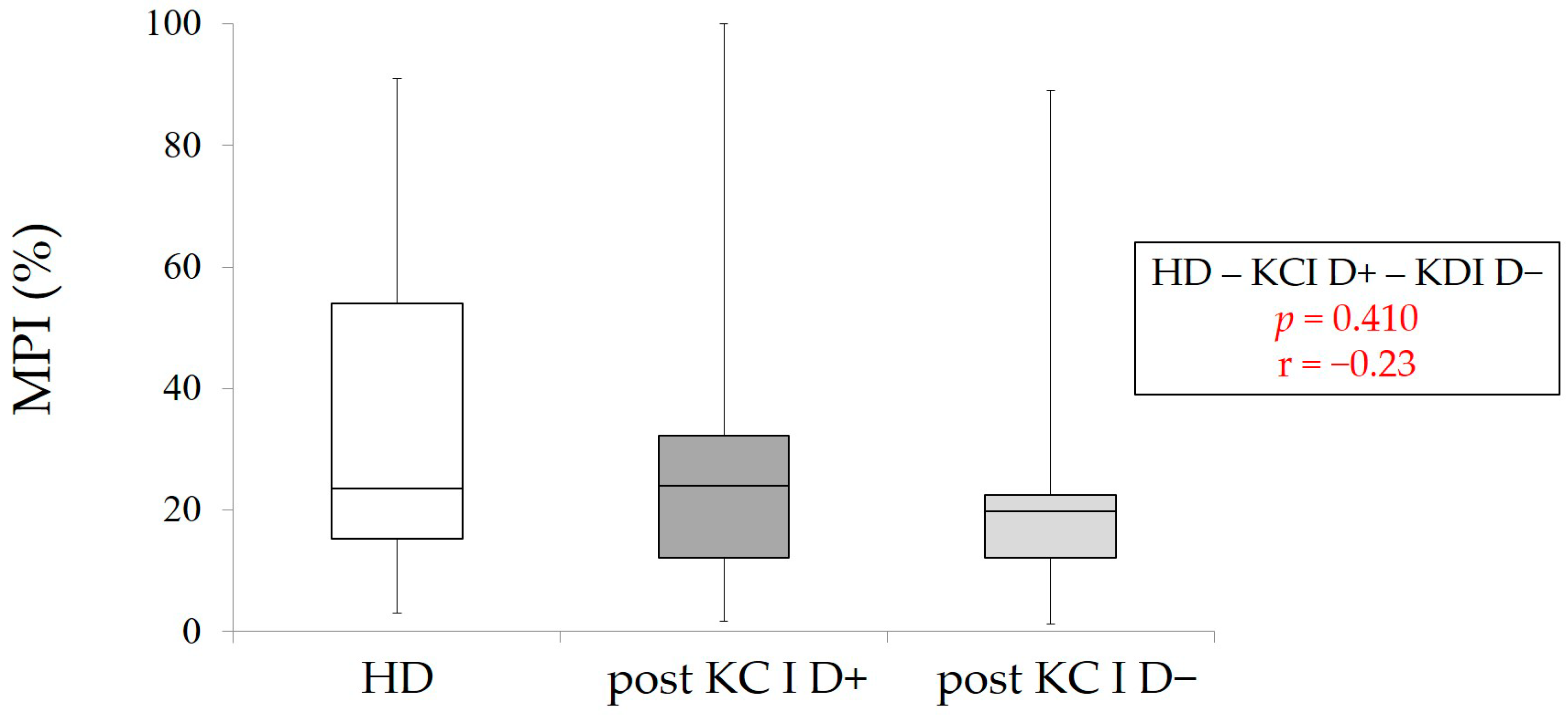
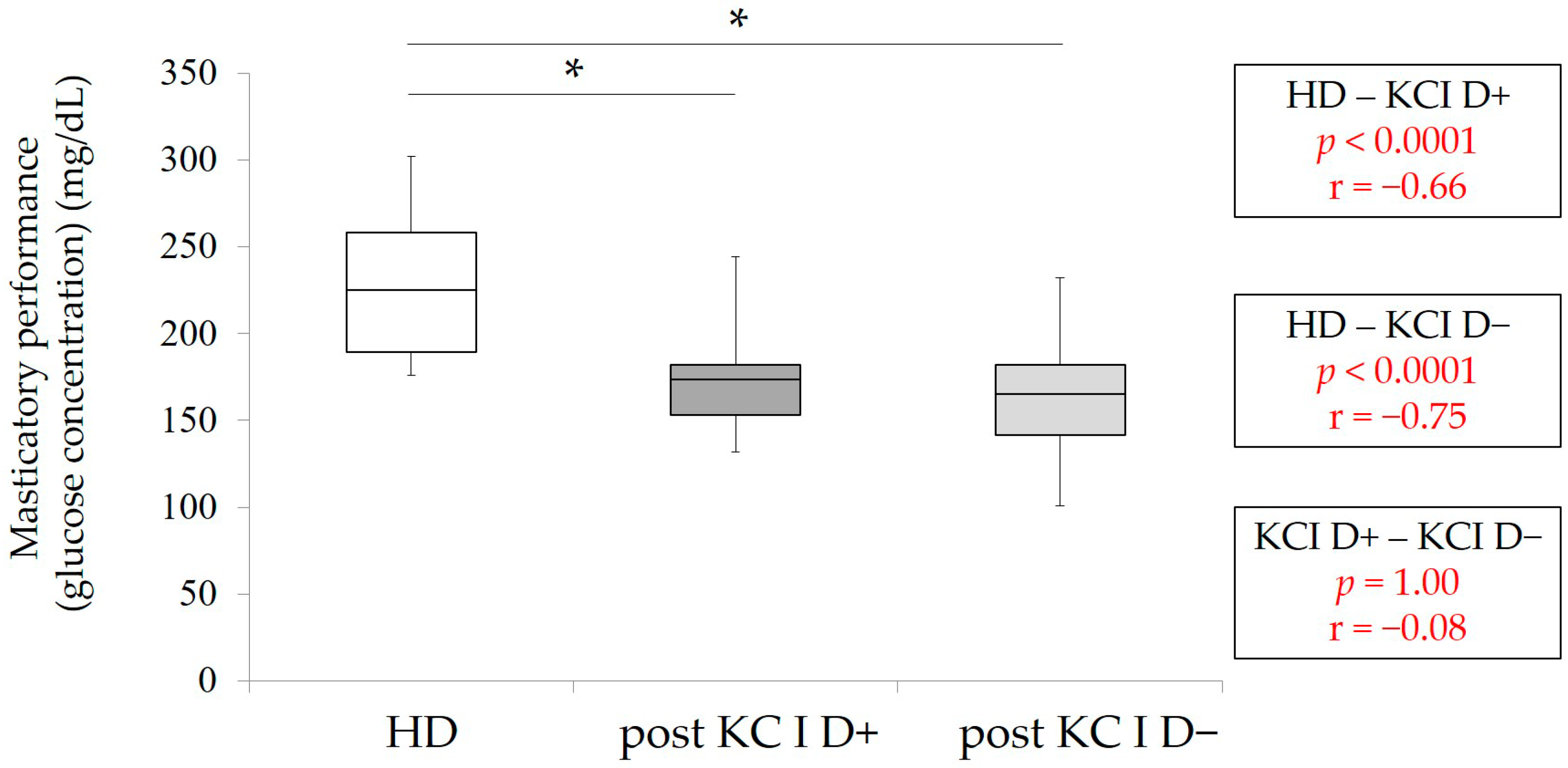
3.4. Comparisons of MPI and Masticatory Performance between the Patients in Post-KC I and HD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wictorin, L.; Hedegard, B.; Lundberg, M. Masticatory function—A cineradiographic study. 3. Position of the bolus in individuals with full complement of natural teeth. Acta Odontol. Scand. 1968, 26, 213–222. [Google Scholar] [CrossRef]
- Wilding, R.J.; Lewin, A. A model for optimum functional human jaw movements based on values associated with preferred chewing patterns. Arch. Oral Biol. 1991, 36, 519–523. [Google Scholar] [CrossRef]
- Ratnasari, A.; Hasegawa, K.; Oki, K.; Kawakami, S.; Yanagi, Y.; Asaumi, J.I.; Minagi, S. Manifestation of preferred chewing side for hard food on TMJ disc displacement side. J. Oral Rehabil. 2011, 38, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Zamanlu, M.; Khamnei, S.; Salarilak, S.; Oskoee, S.S.; Shakouri, S.K.; Houshyar, Y.; Salekzamani, Y. Chewing side preference in first and all mastication cycles for hard and soft morsels. Int. J. Clin. Exp. Med. 2012, 5, 326–333. [Google Scholar] [PubMed]
- Rovira-Lastra, B.; Flores-Orozco, E.I.; Ayuso-Montero, R.; Peraire, M.; Martinez-Gomis, J. Peripheral, functional and postural asymmetries related to the preferred chewing side in adults with natural dentition. J. Oral Rehabil. 2016, 43, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Haralur, S.B.; Majeed, M.I.; Chaturvedi, S.; Alqahtani, N.M.; Alfarsi, M. Association between preferred chewing side and dynamic occlusal parameters. J. Int. Med. Res. 2019, 47, 1908–1915. [Google Scholar] [CrossRef] [PubMed]
- Santana-Mora, U.; Lopez, J.; Mora, M.J.; Xosé, L.O.; Santana-Penín, U. Temporomandibular disorders: The habitual chewing side syndrome. PLoS ONE 2013, 8, e59980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diernberger, S.; Bernhardt, O.; Schwahn, C.; Kordass, B. Self-reported chewing side preference and its associations with occlusal, temporomandibular and prosthodontic factors: Results from the population-based Study of Health in Pomerania (SHIP-0). J. Oral Rehabil. 2008, 35, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Farias, G.S.G.; Custodio, W.; Moura, J.J.S.; Der Ber Cury, A.A. Rodrigues GRCM. Correlation of mastication and masticatory movements and effect of chewing side preference. Braz. Dent. J. 2010, 21, 351–355. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, C.; Machado, B.; Borges, C.; Silva, M.; Sforza, C.; Felicio, C. Impaired orofacial motor functions on chronic temporomandibular disorders. J. Electromyogr. Kinesiol. 2014, 24, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Mohl, N.; Zarb, G.; Carlsson, G.; Rugh, J. A Textbook of Occlusion; Quintessence Publishing Co Inc.: Chicago, IL, USA, 1988; p. 143. [Google Scholar]
- Wilding, R.J.; Adams, L.P.; Lewin, A. Absence of association between a preferred chewing side and its area of functional occlusal contact in the human dentition. Arch. Oral Biol. 1992, 37, 423–428. [Google Scholar] [CrossRef]
- Bates, J.F.; Stafford, G.D.; Harrison, A. Masticatory function—A review of the literature. 1. The form of the masticatory cycle. J. Oral Rehabil. 1975, 2, 281–301. [Google Scholar] [CrossRef] [PubMed]
- Fueki, K.; Baba, K. Shortened dental arch and prosthetic effect on oral health-related quality of life: A systematic review and meta-analysis. J. Oral Rehabil. 2017, 44, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Reissmann, D.R.; Wolfart, S.; John, M.T.; Birgit Marré, B.; Walter, M.; Kern, M.; Kohal, R.; Nothdurft, F.; Stark, H.; Schierz, O.; et al. Impact of shortened dental arch on oral health-related quality of life over a period of 10 years—A randomized controlled trial. J. Dent. 2019, 80, 55–62. [Google Scholar] [CrossRef]
- Yamasaki, Y.; Kuwatsuru, R.; Tsukiyama, Y.; Oki, K.; Koyano, K. Objective assessment of mastication predominance in healthy dentate subjects and patients with unilateral posterior missing teeth. J. Oral Rehabil. 2016, 43, 575–582. [Google Scholar] [CrossRef]
- Iwashita, H.; Tsukiyama, Y.; Kori, H.; Kuwatsuru, R.; Yamasaki, Y.; Koyano, K. Comparative cross-sectional study of masticatory performance and mastication predominance for patients with missing posterior teeth. J. Prosthodont. Res. 2014, 58, 223–229. [Google Scholar] [CrossRef]
- Yamashita, S.; Sakai, S.; Hatch, J.P.; Rugh, J.D. Relationship between oral function and occlusal support in denture wearers. J. Oral Rehabil. 2000, 27, 881–886. [Google Scholar] [CrossRef]
- Shinogaya, T.; Toda, S. Rehabilitation of occlusal support by removable partial dentures with free-end saddles. Eur. J. Prosthodont Restor Dent. 2003, 11, 107–113. [Google Scholar]
- Berretin-Felix, G.; Nary Filho, H.; Padovani, C.R.; Trindade, A.S., Jr.; Machado, W.M. Electromyographic evaluation of mastication and swallowing in elderly individuals with mandibular fixed implant-supported prostheses. J. Appl. Oral Sci. 2008, 16, 116–121. [Google Scholar] [CrossRef] [Green Version]
- Oki, K.; Ogino, Y.; Tsukiyama, Y.; Yamasaki, Y.; Koyano, K. The impacts of prosthetic interventions on mastication predominance in Kennedy Class II patients. J. Prosthodont. Res. 2021, in press. [Google Scholar] [CrossRef]
- Ikebe, K.; Matsuda, K.; Murai, S.; Maeda, Y.; Nokubi, T. Validation of the Eichner index in relation to occlusal force and masticatory performance. Int. J. Prosthodont. 2010, 23, 521–524. [Google Scholar] [PubMed]
- Kosaka, T.; Ono, T.; Kida, M.; Kikui, M.; Yamamoto, M.; Yasui, S.; Nokubi, T.; Maeda, Y.; Kokubo, Y.; Watanabe, M.; et al. A multifactorial model of masticatory performance: The Suita study. J. Oral Rehabil. 2016, 43, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Kosaka, T.; Kida, M.; Kikui, M.; Hashimoto, S.; Fujii, K.; Yamamoto, M.; Nokubi, T.; Maeda, Y.; Hasegawa, Y.; Kokubo, Y.; et al. Factors Influencing the Changes in Masticatory Performance: The Suita Study. JDR Clin. Trans. Res. 2018, 3, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Shiga, H. Masticatory performance of the elderly as seen from differences in occlusal support of residual teeth. J. Prosthodont. Res. 2018, 62, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, Y.; Kuwatsuru, R.; Tsukiyama, Y.; Matsumoto, H.; Oki, K.; Koyano, K. Objective assessment of actual chewing side by measurement of bilateral masseter muscle electromyography. Arch. Oral Biol. 2015, 60, 1756–1762. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical power analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Liang, S.; Zhang, Q.; Witter, D.J.; Wang, Y.; Creugers, N.H. Effects of removable dental prostheses on masticatory performance of subjects with shortened dental arches: A systematic review. J. Dent. 2015, 43, 1185–1194. [Google Scholar] [CrossRef]
- Beyron, H.L. Occlusal changes in adult dentition. J. Am. Dent. Assoc. 1954, 48, 674–686. [Google Scholar] [CrossRef]
- Christensen, L.V.; Radue, J.T. Lateral preference in mastication: Relation to pain. J. Oral Rehabil. 1985, 12, 461–467. [Google Scholar] [CrossRef]
- Pond, L.H.; Barghi, N.; Barnwell, G.M. Occlusion and chewing side preference. J. Prosthet Dent. 1986, 55, 498–500. [Google Scholar] [CrossRef]
- Tay, D.K. Physiognomy in the classification of individuals with a lateral preference in mastication. J. Orofac. Pain. 1994, 8, 61–72. [Google Scholar] [PubMed]
- Nissan, J.; Gross, M.D.; Shifman, A.; Tzadok, L.; Assif, D. Chewing side preference as a type of hemispheric laterality. J. Oral Rehabil. 2004, 5, 412–416. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| KC I n = 44 | KC I D+ n = 22 | KC I D− n = 22 | p-Value | Effect Size (r) | |
|---|---|---|---|---|---|
| Age | 74 (70–77.5) | 75 (71–78) | 73 (67.5–77.25) | 0.95 | 0.09 |
| Gender (male:female | 14:30 | 4:18 | 10:12 | 0.55 | −0.29 |
| The period from delivery of RPD to post measurement (month) | 6 (3–6) | 5 (3–6) | 6 (4–6) | 0.757 | −0.47 |
| Number of posterior occlusal support | 2 (1–3) | 2.5 (1.3–3) | 2 (0–4) | 0.358 | −0.17 |
| Maximum occlusal force (N) | 389.7 (193.8–500.3) | 401.75 (340.2–561.3) | 372.1 (147.95–516.5) | 0.752 | 0.13 |
| Group | Number of Posterior Occlusal Supports (One Side + the Other Side) | Number (Premolar) | Number (Molar) | Number (Patients) | Gender (Male & Female) | Age |
|---|---|---|---|---|---|---|
| D+ | 1 (1 + 0) | 1 | 0 | 6 | 2:4 | 78 (76.25–79) |
| 2 (2 + 0) | 2 | 0 | 5 | 0:5 | 76 (69–77) | |
| 3 (3 + 0) | 2 | 1 | 2 | 1:1 | 76 (75.5–76.5) | |
| 3 (2 + 1) | 3 | 0 | 7 | 1:6 | 72 (63–77) | |
| 4 (3 + 1) | 3 | 1 | 1 | 0:1 | 72 | |
| 5 (3 + 2) | 4 | 1 | 1 | 0:1 | 74 | |
| D− | 0 (0 + 0) | 0 | 0 | 9 | 2:7 | 72 (68–77) |
| 2 (1 + 1) | 2 | 0 | 7 | 2:5 | 74.5 (71.5–77.5) | |
| 4 (2 + 2) | 4 | 0 | 5 | 5:0 | 75 (66.25–77) | |
| 6 (3 + 3) | 4 | 2 | 1 | 1:0 | 64 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinoshita, K.; Ogino, Y.; Oki, K.; Yamasaki, Y.; Tsukiyama, Y.; Ayukawa, Y.; Koyano, K. A Prospective Comparative Study of Mastication Predominance and Masticatory Performance in Kennedy Class I Patients. Healthcare 2021, 9, 660. https://doi.org/10.3390/healthcare9060660
Kinoshita K, Ogino Y, Oki K, Yamasaki Y, Tsukiyama Y, Ayukawa Y, Koyano K. A Prospective Comparative Study of Mastication Predominance and Masticatory Performance in Kennedy Class I Patients. Healthcare. 2021; 9(6):660. https://doi.org/10.3390/healthcare9060660
Chicago/Turabian StyleKinoshita, Kohei, Yoichiro Ogino, Kyosuke Oki, Yo Yamasaki, Yoshihiro Tsukiyama, Yasunori Ayukawa, and Kiyoshi Koyano. 2021. "A Prospective Comparative Study of Mastication Predominance and Masticatory Performance in Kennedy Class I Patients" Healthcare 9, no. 6: 660. https://doi.org/10.3390/healthcare9060660
APA StyleKinoshita, K., Ogino, Y., Oki, K., Yamasaki, Y., Tsukiyama, Y., Ayukawa, Y., & Koyano, K. (2021). A Prospective Comparative Study of Mastication Predominance and Masticatory Performance in Kennedy Class I Patients. Healthcare, 9(6), 660. https://doi.org/10.3390/healthcare9060660