
Smaller Cortisol Awakening Responses Are Associated with Greater Visual Dependence in Postural Control

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
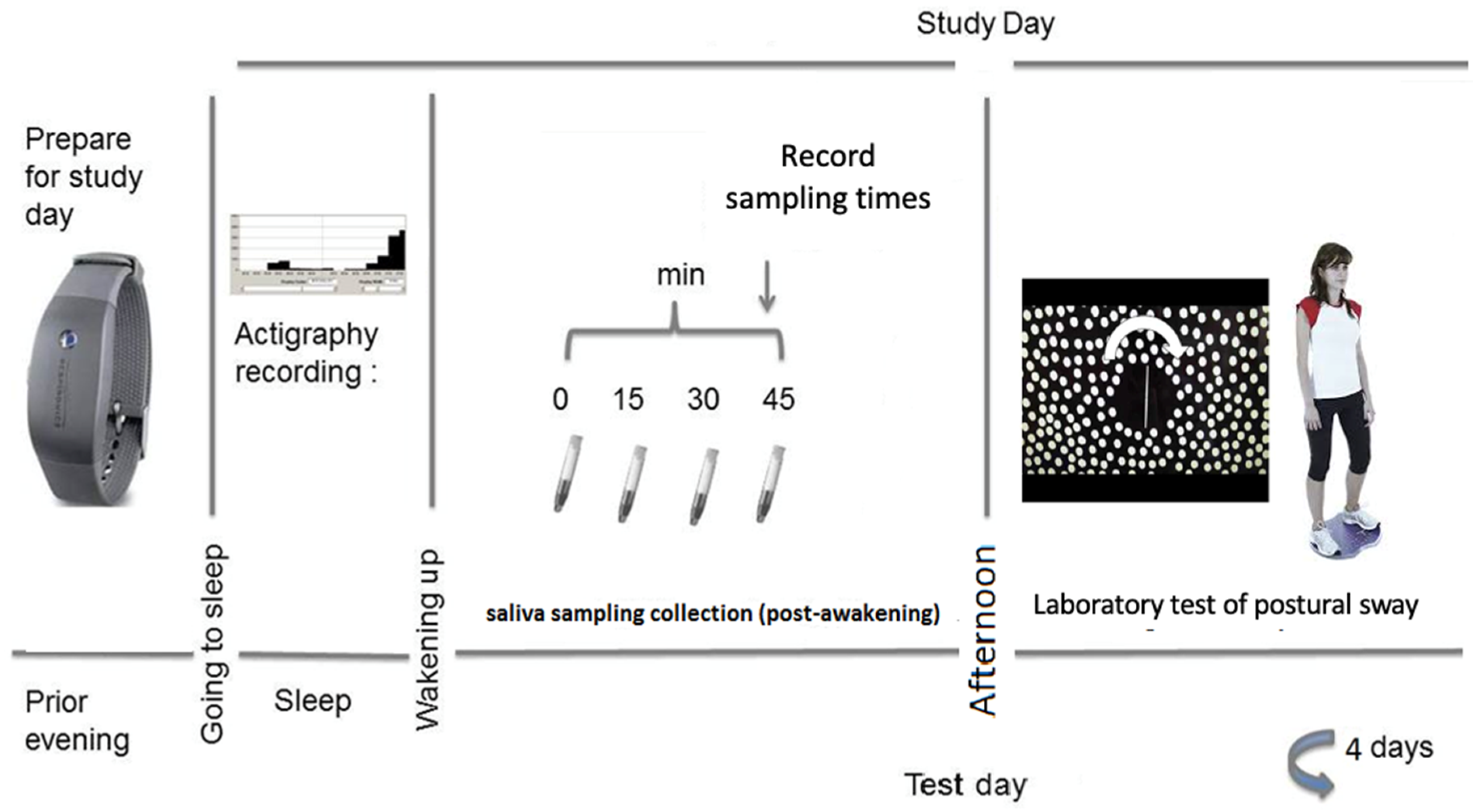
2.2. Design
2.3. Procedure
2.4. Saliva Samples and Electronic Monitoring of the Saliva Sampling Protocol
2.5. Laboratory Testing: Visual Dependence in Postural Sway Assessment
2.6. Cortisol Assessment and Assay
2.7. Treatment of Data and Statistical Analysis
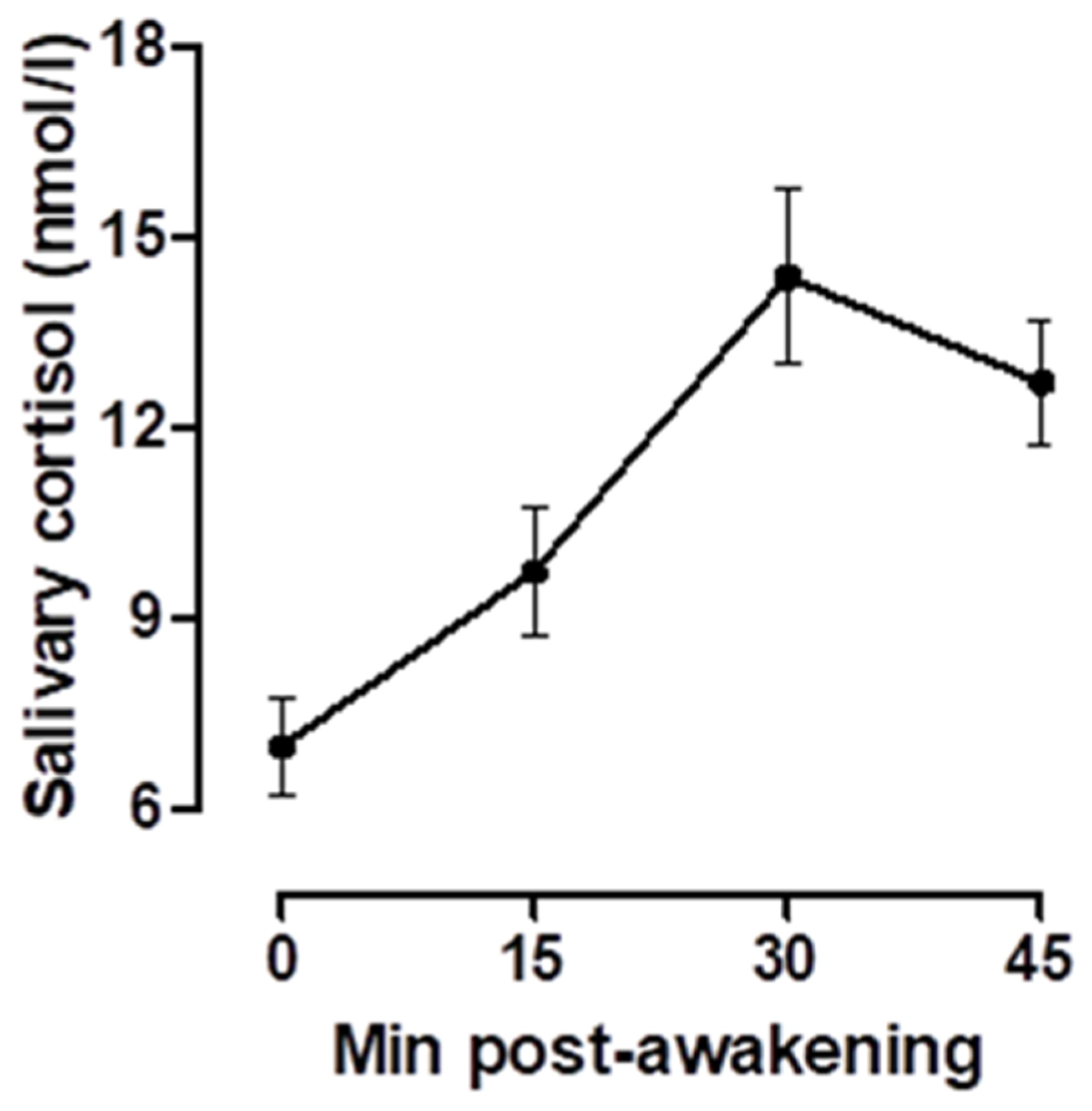
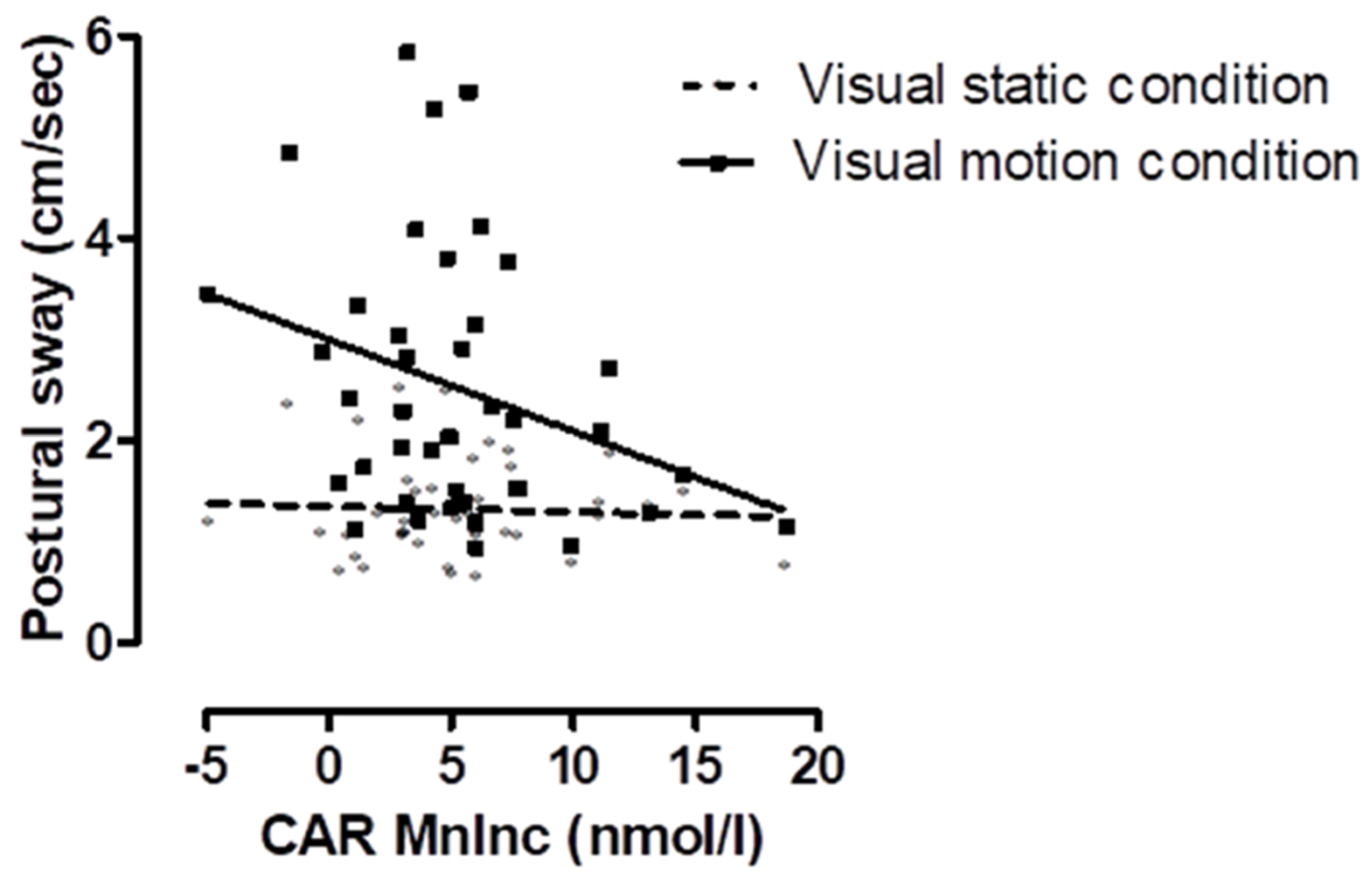
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Asch, S.E.; Witkin, H.A. Studies in Space Orientation: I. Perception of the Upright with Displaced Visual Fields. J. Exp. Psychol. 1948, 38, 325. [Google Scholar] [CrossRef]
- Grace Gaerlan, M.; Alpert, P.T.; Cross, C.; Louis, M.; Kowalski, S. Postural Balance in Young Adults: The Role of Visual, Vestibular and Somatosensory Systems. J. Am. Acad. Nurse Pract. 2012, 24, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Saman, Y.; Arshad, Q.; Dutia, M.; Rea, P. Stress and the Vestibular System. Int. Rev. Neurobiol. 2020, 152, 221–236. [Google Scholar] [CrossRef] [PubMed]
- Micarelli, A.; Viziano, A.; Lanzillotta, A.; Ruscello, B.; D’Ottavio, S.; Alessandrini, M. Visual Dependency and Postural Control on Swing Performance in Golf Players. Eur. J. Sport Sci. 2019, 19, 922–930. [Google Scholar] [CrossRef] [PubMed]
- Redfern, M.S.; Yardley, L.; Bronstein, A.M. Visual Influences on Balance. J. Anxiety Disord. 2001, 15, 81–94. [Google Scholar] [CrossRef]
- Abdul Razzak, R.; Hussein, W. Postural Visual Dependence in Asymptomatic Type 2 Diabetic Patients without Peripheral Neuropathy during a Postural Challenging Task. J. Diabetes Complicat. 2016, 30, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Furman, J.M.; Jacob, R.G. A Clinical Taxonomy of Dizziness and Anxiety in the Otoneurological Setting. J. Anxiety Disord. 2001, 15, 9–26. [Google Scholar] [CrossRef]
- Balaban, C.D.; Thayer, J.F. Neurological Bases for Balance-Anxiety Links. J. Anxiety Disord. 2001, 15, 53–79. [Google Scholar] [CrossRef]
- Herdman, D.; Norton, S.; Pavlou, M.; Murdin, L.; Moss-Morris, R. Vestibular Deficits and Psychological Factors Correlating to Dizziness Handicap and Symptom Severity. J. Psychosom. Res. 2020, 132, 109969. [Google Scholar] [CrossRef]
- Saman, Y.; Bamiou, D.E.; Gleeson, M.; Dutia, M.B. Interactions between Stress and Vestibular Compensation- A Review. Front. Neurol. 2012, 3, 116. [Google Scholar] [CrossRef] [Green Version]
- Smyth, N.; Hucklebridge, F.; Thorn, L.; Evans, P.; Clow, A. Salivary Cortisol as a Biomarker in Social Science Research. Soc. Personal. Psychol. Compass 2013, 7, 605–625. [Google Scholar] [CrossRef]
- Clow, A.; Hucklebridge, F.; Stalder, T.; Evans, P.; Thorn, L. The Cortisol Awakening Response: More than a Measure of HPA Axis Function. Neurosci. Biobehav. Rev. 2010, 35, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Stalder, T.; Kirschbaum, C.; Kudielka, B.M.; Adam, E.K.; Pruessner, J.C.; Wüst, S.; Dockray, S.; Smyth, N.; Evans, P.; Hellhammer, D.H.; et al. Assessment of the Cortisol Awakening Response: Expert Consensus Guidelines. Psychoneuroendocrinology 2016, 63, 414–432. [Google Scholar] [CrossRef] [PubMed]
- Bonnefont, X. Circadian Timekeeping and Multiple Timescale Neuroendocrine Rhythms. J. Neuroendocrinol. 2010, 22, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Menet, J.S.; Rosbash, M. When Brain Clocks Lose Track of Time: Cause or Consequence of Neuropsychiatric Disorders. Curr. Opin. Neurobiol. 2011, 21, 849–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clow, A.; Smyth, N. Salivary Cortisol as a Non-Invasive Window on the Brain. Int. Rev. Neurobiol. 2020, 150, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Smyth, N.; Thorn, L.; Hucklebridge, F.; Clow, A.; Evans, P. Assessment of the Cortisol Awakening Response: Real-Time Analysis and Curvilinear Effects of Sample Timing Inaccuracy. Psychoneuroendocrinology 2016, 74, 380–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clow, A.; Law, R.; Evans, P.; Vallence, A.-M.; Hodyl, N.A.; Goldsworthy, M.R.; Rothwell, J.R.; Ridding, M.C. Day Differences in the Cortisol Awakening Response Predict Day Differences in Synaptic Plasticity in the Brain. Stress 2014, 17, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Boyne, K.; Sherry, D.D.; Gallagher, P.R.; Olsen, M.; Brooks, L.J. Accuracy of Computer Algorithms and the Human Eye in Scoring Actigraphy. Sleep Breath. 2013, 17, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Cousins, S.; Cutfield, N.J.; Kaski, D.; Palla, A.; Seemungal, B.M.; Golding, J.F.; Staab, J.P.; Bronstein, A.M. Visual Dependency and Dizziness after Vestibular Neuritis. PLoS ONE 2014, 9, e105426. [Google Scholar] [CrossRef] [Green Version]
- Cousins, S.; Kaski, D.; Cutfield, N.; Arshad, Q.; Ahmad, H.; Gresty, M.A.; Seemungal, B.M.; Golding, J.; Bronstein, A.M. Predictors of Clinical Recovery from Vestibular Neuritis: A Prospective Study. Ann. Clin. Transl. Neurol. 2017, 4, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Coco, M.; Fiore, A.S.; Perciavalle, V.; Maci, T.; Petralia, M.C.; Perciavalle, V. Stress Exposure and Postural Control in Young Females. Mol. Med. Rep. 2015. [Google Scholar] [CrossRef] [Green Version]
- Coco, M.; Buscemi, A.; Pennisi, E.; Cavallari, P.; Papotto, G.; Papotto, G.M.F.; Perciavalle, V.; Di Corrado, D.; Perciavalle, V. Postural Control and Stress Exposure in Young Men: Changes in Cortisol Awakening Response and Blood Lactate. Int. J. Environ. Res. Public Health 2020, 17, 7222. [Google Scholar] [CrossRef]
- Smyth, N.; Flynn, M.; Rajcani, J.; Hucklebridge, M.F.; Thorn, L.; Wood, C.; Golding, J.; Evans, P.; Clow, A. Attenuated Cortisol Reactivity to Psychosocial Stress Is Associated with Greater Visual Dependency in Postural Control. Psychoneuroendocrinology 2019, 104, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.; O’Connor, D.B.; Schaefer, A.; Talbot, D.; Hendrickx, H. The Cortisol Awakening Response: Associations with Trait Anxiety and Stress Reactivity. Pers. Individ. Dif. 2011, 51, 123–127. [Google Scholar] [CrossRef]
- Joseph, J.J.; Golden, S.H. Cortisol Dysregulation: The Bidirectional Link between Stress, Depression, and Type 2 Diabetes Mellitus. Ann. N. Y. Acad. Sci. 2017, 1391, 20. [Google Scholar] [CrossRef] [PubMed]
- Persiani, M.; Piras, A.; Squatrito, S.; Raffi, M. Laterality of Stance during Optic Flow Stimulation in Male and Female Young Adults. Biomed Res. Int. 2015, 2015, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Model A | Model B | |||
|---|---|---|---|---|
| Co-Efficient | SE | Co-Efficient | SE | |
| Intercept | 0.068 | 0.161 | 0.095 | 0.164 |
| Visual stimulus condition (static vs. motion) | 0.598 * | 0.053 | 0.599 * | 0.048 |
| MnInc | −0.130 | 0.114 | ||
| Visual stimulus condition * MnInc | −0.204 * | 0.057 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smyth, N.; Milani, M.; Thorn, L.; Flynn, M.; Golding, J.F.; Evans, P.; Clow, A. Smaller Cortisol Awakening Responses Are Associated with Greater Visual Dependence in Postural Control. Healthcare 2021, 9, 723. https://doi.org/10.3390/healthcare9060723
Smyth N, Milani M, Thorn L, Flynn M, Golding JF, Evans P, Clow A. Smaller Cortisol Awakening Responses Are Associated with Greater Visual Dependence in Postural Control. Healthcare. 2021; 9(6):723. https://doi.org/10.3390/healthcare9060723
Chicago/Turabian StyleSmyth, Nina, Monica Milani, Lisa Thorn, Maria Flynn, John F. Golding, Phil Evans, and Angela Clow. 2021. "Smaller Cortisol Awakening Responses Are Associated with Greater Visual Dependence in Postural Control" Healthcare 9, no. 6: 723. https://doi.org/10.3390/healthcare9060723
APA StyleSmyth, N., Milani, M., Thorn, L., Flynn, M., Golding, J. F., Evans, P., & Clow, A. (2021). Smaller Cortisol Awakening Responses Are Associated with Greater Visual Dependence in Postural Control. Healthcare, 9(6), 723. https://doi.org/10.3390/healthcare9060723