
A Salutogenic Perspective on End-of-Life Care among the Indigenous Sámi of Northern Fennoscandia

Abstract
:1. Introduction and Aim
2. Background
3. Methods
3.1. Research Team Investigating Sámi Perspectives on EoL
3.2. Data Collection
3.3. Ethics
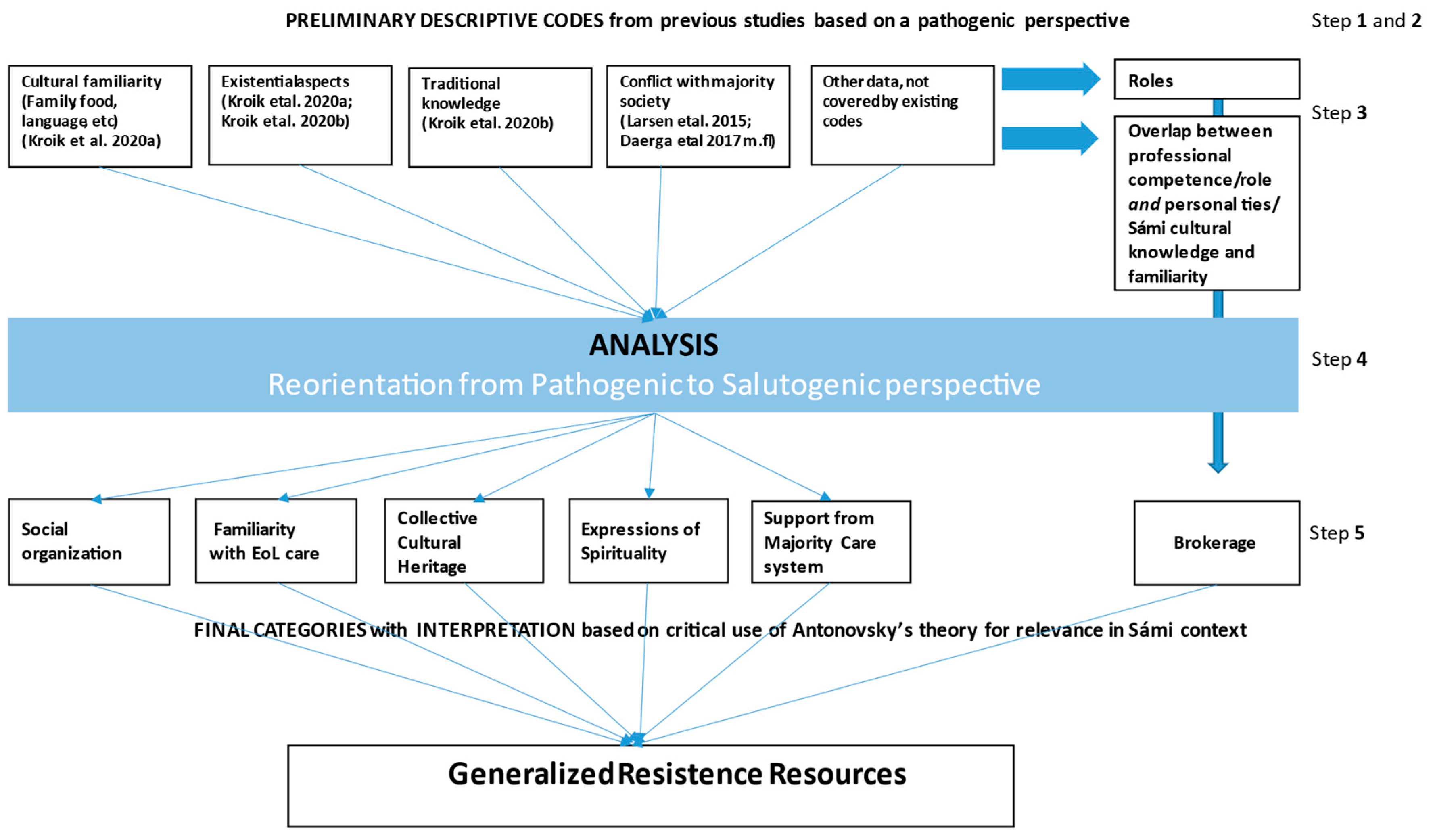
3.4. Data Analysis
4. Findings
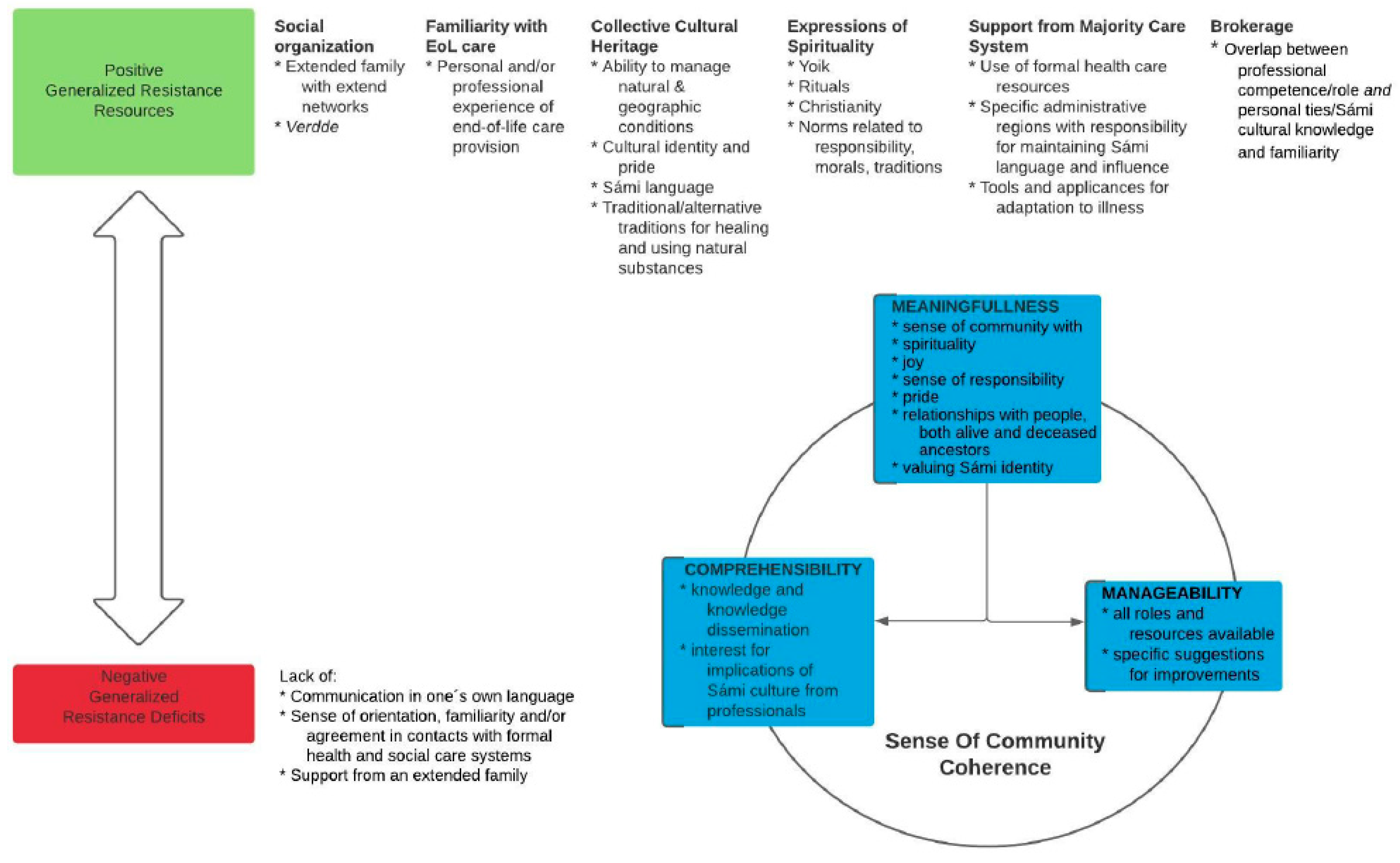
4.1. Generalized Resistance Resources
4.1.1. Social Organization
I’m participating here [at the churchdays] because I think I have…as a member of this clan I have experienced lots of…I have been part of this family system, relation…this care in the end-of-life. There are some...lots of things to think about. Lots of traditions in my area and also in the other Sámi areas. And also dealing with this…subject in my profession.(FGD 3)
4.1.2. Familiarity with End-Of-Life Care
D6: I felt like my workmates were a support during that time.D2: But then you were steering it a bit when you decided what you would need…it was you who was the closest as well, and so it was you who pressed the button when they [staff] should come in.D6: yes, but I…but you know what it was? I’m both an assistant nurse and a relative, and then I could sometimes feel ‘what is what’? But I didn’t feel badly about it. I had to call you know, when I felt like I couldn’t manage, then I called and so another workmate came in.(FGD 4)
Because we were very lost, both mama and me, in the health care system. And these words that are so important, care-planning and …if you…you know what you can get and not get from the health care system when you are in…you know, death’s waiting room, that was very confusing for us. And as Sámi, we are very close to our extended family and it is, it was very confusing because we’re used to doing everything ourselves and then suddenly the health care system tells me “you shouldn’t be the care provider, you should be family, you should brighten up her last phase of life”. And it was really hard to figure out where the line should be drawn. And I realized afterwards that I maybe should have asked for help earlier. As an only child and as a Sámi, it was very…And finally Mama said stop, she said “we reached the limit, it’s no longer dignified for you, as my child, to care for me” And that feeling of being lost in the health care system as a Sámi, in death’s waiting room, I feel that so strongly, that a little book or something is needed.(FGD 4)
4.1.3. Collective Cultural Heritage
And I pushed that ’skåerrie’ [a piece of treated reindeer skin with a recognizable scent] across the table to the two ladies sitting there. And they just went ’mmm, skåerrie, ohhhhh’. So you can see how much it means, things you may think are trivial, but they are memories and they are childhood and they are family and they are just the culture, they are so much…There were three things everyone wanted [refers to the survey]. And these were that when they got older and moved to a care home, they wanted to still have their language with staff that could speak Sámi, and Sámi food, and they wanted to be able to be with other Sámi.(from data collection 2, go-along group discussions)
And you know, it’s not possible to carry those feelings across in a second or third language, and so therefore we need to use our mother tongue in such times, that is at a death bed or at the funeral […] as an important part of the process, the healing process or the grieving process.(FGD 1)
And then there’s a lot, you might say alternative medicine, that is not drugs, but how you earlier maybe drank chaga-birch tea and blueberry, that is these things that are around, that have been used for a long time. So this knowledge exists. But it’s very very…hush hush and secretive.(From data collection 3, ACP discussions)
They [the family] called ’govhlar’, what’s it called, kind of healers, shamans, who you believe in, in the Sámi culture and who still remain. And you call them and ask them for help so that they can heal and make it take a turn for the better now […] No one has visited me in person, but it’s about these strong forces that work through the mind.(From data collection 3, ACP discussions)
4.1.4. Expressions of Spirituality
But during the funeral there was yoik and everything. And then these people, her workmates, she said it was fantastic to be at a Sámi funeral. We’re there with koltar [traditional clothing in the national colors of red, blue, yellow and green] and all, it’s not all in black and so, but it was, yes it was so very nice.(FGD 4)
I’m thinking about if I experienced anything […] the animals had such …importance […]. And everyone had their own animal that watched over them and that they were preoccupied with, and then I thought, that this is a Sámi thing. Understanding animals and that way of being observant, it comes from their way of living…(FGD 2)
even though you are related […] there are these moral obligations. There is also a…it’s also dangerous to say no […], yes, it is unheard of, so to speak. You can also bring misfortune over yourself then […] since it is such a very strict norm(FGD 3)
I’ve grown up with X siblings, and if one is sick, we are all sick and everyone wants to contribute […] Father always said ‘it’s important to show your feelings’. And we have cried together and I have a sibling who died in an accident […] I thought when my brother died […] then that it was punishment from God. But then my grandmother said ‘it’s not punishment from God, but we have different trials, because life is a school that can be hard sometimes, and maybe his time had come’. And that has given me strength in my grief process, thinking that […] his time had come. […] it’s a trial but not a punishment. There’s no shame. No sense of shame.(FGD 4)
Yes, and in the Sámi world, there is a zipper here. You shouldn’t talk about feelings, you shouldn’t…you feel shame if you are sick because then there is something evil you have…sort of…You have maybe…it is a punishment from God. And there is a lot of shame connected to talking about it and opening yourself up.(FGD 4)
4.1.5. Support from Majority Care Systems
If you only knew how stubborn we had to be. Everyone came and said, ‘do you really understand what kind of responsibility you are taking on, the responsibility you have?’ But then I call the community nurse [mentioning her by first name] and so I said…I told about how it was and that we were thinking of bringing Mama home, but that they advised us not to. “Take [mentions mother by name] home, I’ll come and help you” she just said. So my sister went to her [the community nurse] and brought back a load of things to help…(from data collection 2, go-along group discussions)
and there are always some fantastic enthusiasts who work for the Sámi population, the elders, who should be able to have a place in residential care homes, on special units where they feel at home, where staff who applies for those positions, they are able to study Sámi language to be able to meet their needs […]. And then you need some enthusiasts who, along with their maternal and paternal grandparents, get a foot in and have the strength to get the municipalities to… so that this unit…it should be reserved for…it should just be for Sámi.(FGD 2)
...for us Sámi, our own TV and group room, so we can see Ođđasat [Sámi news program] without the laedtieh [non-Sámi] who question ’what’s that you’re watching?’…no, I say, we should have our own […], we can be in the same unit […] but then when we should have our food and such, then we can go and eat in their dining room. But we should have our own…it should be the kind of cooking that we cook, so we can make bovtsen bearkoe [reindeer meat] and we can guelie voessjedh jih maelie laejpie bissedh jih numhtie [cook fish and fry blood bread and all that]…(FGD 2)
4.1.6. Brokerage as a Bridge between Cultures
And then I sang, and so suddenly, the nurse, she happened to be there and suddenly he [the dying Sámi man] lifted one of his hands and so he began…you could even hear it, how he started to hum along, and then she [the nurse] said ‘that’s never happened before’, she said. Yes, but now it happened. It touched something inside him…(from data collection 1, individual interviews)
And most people don’t have the energy and the knowledge that they have [in the formal health care system]. So that’s why it’s so important that someone in the church and in the health care system knows what’s important to Sámi, and asks about it, isn’t it? And it is…that we know too little, really both the church and health care and all those places. That’s why it’s so important, what you see here [in this research].(FGD 3)
4.2. Generalized Resistance Deficits
I was thinking, horrors of horrors is one of…if there is a Sámi who doesn’t have a strong family who can stop, then you are …abandoned to a system that has it’s bureaus and doesn’t have time or space or possibility or the desire to let the family go in and be involved. And the people of the church even have [refers to internal lack of understanding for Sámi culture and needs even within the church]. Because we wanted the family to ride with the casket but ‘no that’s not what we usually do’…(FGD 3)
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kroik, L.; Lindqvist, O.; Stoor, K.; Tishelman, C. The past is present: Death systems among the Indigenous Sámi in Northern Scandinavia today. Mortality 2020, 25, 470–489. [Google Scholar] [CrossRef] [Green Version]
- Kroik, L.; Stoor, K.; Edin-Liljegren, A.; Tishelman, C. Using narrative analysis to explore traditional Sámi knowledge through storytelling about End-of-Life. Health Place 2020, 65, 102424. [Google Scholar] [CrossRef]
- Kroik, L.; Eneslätt, M.; Tishelman, C.; Stoor, K.; Edin-Liljegren, A. Values and Preferences for Future End-of-Life Care among the Indigenous Sámi. DiVA 2021, diva2:1542796. [Google Scholar]
- Kelley; Prince, H.; Nadin, S.; Brazil, K.; Crow, M.; Hanson, G.; Maki, L.; Monture, L.; Mushquash, C.J.; O’Brien, V.; et al. Developing palliative care programs in Indigenous communities using participatory action research: a Canadian application of the public health approach to palliative care. Ann. Palliat. Med. 2018, 7, S52–S72. [Google Scholar] [CrossRef] [Green Version]
- Caxaj, C.S.; Schill, K.; Janke, R. Priorities and challenges for a palliative approach to care for rural indigenous populations: A scoping review. Health Soc. Care Community 2018, 26, e329–e336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wängberg, H.Å. Samerätt och samiskt språk: slutbetänkande. In Statens Offentliga Utredningar; Allmänna förl.: Stockholm, Sweden, 1990; ISSN 0375-250X. [Google Scholar]
- Sametinget. Samerna i Sverige. Available online: https://www.sametinget.se/samer (accessed on 17 June 2021).
- Hassler; Johansson, R.; Sjolander, P.; Gronberg, H.; Damber, L. Causes of death in the Sami population of Sweden, 1961–2000. Int. J. Epidemiol. 2005, 34, 623–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sametinget. Statistik Rennäring. Available online: https://www.sametinget.se/renstatistik (accessed on 17 June 2021).
- Ingold, T. Hunters, Pastoralists and Ranchers: Reindeer Economies and Their Transformations; Cambridge U.P.: Cambridge, UK, 1980. [Google Scholar]
- FAO. Understanding Mobile Pastoralism Key to Prevent Conflict. Available online: http://www.fao.org/pastoralist-knowledge-hub/news/detail/en/c/449730/ (accessed on 22 January 2021).
- Lag (2009:724) om Nationella Minoriteter och Minoritetsspråk. Available online: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/lag-2009724-om-nationella-minoriteter-och_sfs-2009-724 (accessed on 17 June 2021).
- Larsen, L.S.; Normann, H.K.; Hamran, T. Collaboration between Sami and non-Sami formal and family caregivers in rural municipalities. Ethn. Racial Stud. 2015, 39, 821–839. [Google Scholar] [CrossRef] [Green Version]
- Daerga; Sjolander, P.; Jacobsson, L.; Edin-Liljegren, A. The confidence in health care and social services in northern Sweden—A comparison between reindeer-herding Sami and the non-Sami majority population. Scand. J. Public Health 2012, 40, 516–522. [Google Scholar] [CrossRef]
- Bernardes, C.M.; Diaz, A.; Valery, P.C.; Sabesan, S.; Baxi, S.; Aoun, S.; Thompson, S.C.; Lashbrook, M.; Garvey, G. Unmet supportive care needs among Indigenous cancer patients across Australia. Rural Remote Health 2019, 19, 4660. [Google Scholar] [CrossRef] [PubMed]
- Shahid, S.; Taylor, E.V.; Cheetham, S.; Woods, J.A.; Aoun, S.M.; Thompson, S.C. Key features of palliative care service delivery to Indigenous peoples in Australia, New Zealand, Canada and the United States: A comprehensive review. BMC Palliat. Care 2018, 17, 72. [Google Scholar] [CrossRef] [PubMed]
- Waran, E.; O’Connor, N.; Zubair, M.Y.; May, P. ‘Finishing up’ on country: Challenges and compromises. Intern. Med. J. 2016, 46, 1108–1111. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.A.; Groot, G.; Carr, T. Decisions on cancer care by Indigenous peoples in Alberta and Saskatchewan: A narrative analysis. Rural Remote Health 2020, 20, 5610. [Google Scholar] [CrossRef] [PubMed]
- Hansen, K.L. Ethnic discrimination and health: the relationship between experienced ethnic discrimination and multiple health domains in Norway’s rural Sami population. Int. J. Circumpolar Health 2015, 74, 25125. [Google Scholar] [CrossRef] [PubMed]
- Nystad, T.; Melhus, M.; Lund, E. Sami speakers are less satisfied with general practitioners’ services. Int. J. Circumpolar Health 2008, 67, 116–123. [Google Scholar] [CrossRef]
- Blix, B.H.; Hamran, T. “They take care of their own”: Healthcare professionals’ constructions of Sami persons with dementia and their families’ reluctance to seek and accept help through attributions to multiple contexts. Int. J. Circumpolar Health 2017, 76. [Google Scholar] [CrossRef]
- Blix, B.H. Helse- og Omsorgstjenester til den Samiske Befolkningen i Norge. Available online: https://core.ac.uk/download/pdf/335076695.pdf (accessed on 17 June 2021).
- Duggleby, W.; Kuchera, S.; MacLeod, R.; Holyoke, P.; Scott, T.; Holtslander, L.; Letendre, A.; Moeke-Maxwell, T.; Burhansstipanov, L.; Chambers, T. Indigenous people’s experiences at the end of life. Palliat. Supportive Care 2015, 13, 1721–1733. [Google Scholar] [CrossRef]
- Daerga, L. Att Leva I Två Världar: Hälsoaspekter Bland Renskötande Samer. Ph.D. Thesis, Umeå Universitet, Umeå, Sweden, 2017. [Google Scholar]
- Ness, T.M.; Soderberg, S.; Hellzen, O. ‘Contradictions in having care providers with a South Sami background who speak South Sami’: older South Sami People in Sweden’s expectations of home nursing care. Scand. J. Caring Sci. 2020, 34, 436–445. [Google Scholar] [CrossRef]
- Kastenbaum, R.; Moreman, C.M. Death, Society, and Human Experience, 12nd ed.; Routledge: New York, NY, USA, 2018. [Google Scholar]
- Hsieh, H.-F.; Shannon, S. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Ward, D.J.; Furber, C.; Tierney, S.; Swallow, V. Using Framework Analysis in nursing research: a worked example. J. Adv. Nurs. 2013, 69, 2423–2431. [Google Scholar] [CrossRef]
- Mittelmark, M.B.; Sagy, S.; Eriksson, M.; Bauer, G.F.; Pelikan, J.M.; Lindström, B.; Espnes, G.A. The Handbook of Salutogenesis, 1st ed.; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar] [CrossRef] [Green Version]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well, 1st ed.; Jossey-Bass: San Francisco, CA, USA, 1987. [Google Scholar]
- Idan, O.; Eriksson, M.; Al-Yagon, M. The Salutogenic Model: The Role of Generalized Resistance Resources. In The Handbook of Salutogenesis; Sagy, M.B.M.S., Pelikan, M.E.G.F.B.J.M., Espnes, B.L.G.A., Eds.; Springer: Cham, Switzerland, 2017; pp. 62–65. [Google Scholar]
- Peled, D.; Sagy, S.; Braun-Lewensohn, O. Community perceptions as a coping resource among adolescents living under rockets fire: A salutogenic approach. J. Community Posit. Pract. 2012, 4, 681–702. [Google Scholar]
- Abrahamsson, A.; Lindmark, U.; Gerdner, A. Sense of coherence of reindeer herders and other Samis in comparison to other Swedish citizens. Int. J. Circumpolar Health 2013, 72, 20633. [Google Scholar] [CrossRef]
- Hassler, S.; Eklund, L. Sense of coherence and self-reported health among Roma people in Sweden—A pilot study. Int. J. Circumpolar Health 2012, 71, 18438. [Google Scholar] [CrossRef]
- Alex, L. Resilience among old Sami women. Ageing Soc. 2016, 36, 1738–1756. [Google Scholar] [CrossRef]
- Nordin, Å. Relationer i ett Samiskt Samhälle: En Studie av Skötesrensystemet i Gällivare Socken under Första Hälften av 1900-talet; Umeå University: Umeå, Sweden, 2002. [Google Scholar]
- Stoor, K. Juoiganmuitalusat-Jojkberättelser: En Studie av Jojkens Narrativa Egenskaper. Ph.D. Thesis, Umeå Universitet, Umeå, Sweden, 31 August 2007. [Google Scholar]
- Horsburgh, M.E.; Ferguson, A.L. Salutogenesis: Origins of helath and sense of coherence. In Handbook of Stress, Coping, and Health: Implications for Nursing Research, Theory, and Practice, 2nd ed.; Rice, V.H., Ed.; Sage Publications: Thousand Oaks, CA, USA, 2012; pp. 180–198. [Google Scholar]
- Idan, O.; Eriksson, M.; Al-Yagon, M. The salutogenic model: The role of generalized resistance resources. In The Handbook of Salutogenesis; Springer: Cham, Switzerland, 2017; pp. 57–69. [Google Scholar]
- Tishelman, C. Några kritiska reflektioner över vårt okritiska bruk av mätinstrument: Exemplet Känsla av Sammanhang frågeformulär. Vård i Norden 1996, 16, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A.; Sagy, S. Confronting developmental tasks in the retirement transition. Gerontologist 1990, 30, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Mehus, G.; Bongo, B.A.; Engnes, J.I.; Moffitt, P.M. Exploring why and how encounters with the Norwegian health-care system can be considered culturally unsafe by North Sami-speaking patients and relatives: A qualitative study based on 11 interviews. Int. J. Circumpolar Health 2019, 78, 1612703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devik, S.A.; Olsen, R.M. Trygghet uten særomsorg? Tidsskr. Omsorgsforskning 2020, 6, 70–86. [Google Scholar] [CrossRef]
- Evans, N.; Meñaca, A.; Koffman, J.; Harding, R.; Higginson, I.J.; Pool, R.; Gysels, M. Cultural Competence in End-of-Life Care: Terms, Definitions, and Conceptual Models from the British Literature. J. Palliat. Med. 2012, 15, 812–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foronda, C.; Baptiste, D.-L.; Reinholdt, M.M.; Ousman, K. Cultural Humility: A Concept Analysis. J. Transcult. Nurs. 2016, 27, 210–217. [Google Scholar] [CrossRef]
- Schill, K.; Caxaj, S. Cultural safety strategies for rural Indigenous palliative care: A scoping review. BMC Palliat. Care 2019, 18, 21. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kroik, L.; Tishelman, C.; Stoor, K.; Edin-Liljegren, A. A Salutogenic Perspective on End-of-Life Care among the Indigenous Sámi of Northern Fennoscandia. Healthcare 2021, 9, 766. https://doi.org/10.3390/healthcare9060766
Kroik L, Tishelman C, Stoor K, Edin-Liljegren A. A Salutogenic Perspective on End-of-Life Care among the Indigenous Sámi of Northern Fennoscandia. Healthcare. 2021; 9(6):766. https://doi.org/10.3390/healthcare9060766
Chicago/Turabian StyleKroik, Lena, Carol Tishelman, Krister Stoor, and Anette Edin-Liljegren. 2021. "A Salutogenic Perspective on End-of-Life Care among the Indigenous Sámi of Northern Fennoscandia" Healthcare 9, no. 6: 766. https://doi.org/10.3390/healthcare9060766
APA StyleKroik, L., Tishelman, C., Stoor, K., & Edin-Liljegren, A. (2021). A Salutogenic Perspective on End-of-Life Care among the Indigenous Sámi of Northern Fennoscandia. Healthcare, 9(6), 766. https://doi.org/10.3390/healthcare9060766