
The Effect of Scuba Diving on Microleakage of a Class II Composite Restoration: An In-Vitro Study



Abstract
:1. Introduction
2. Material and Methods
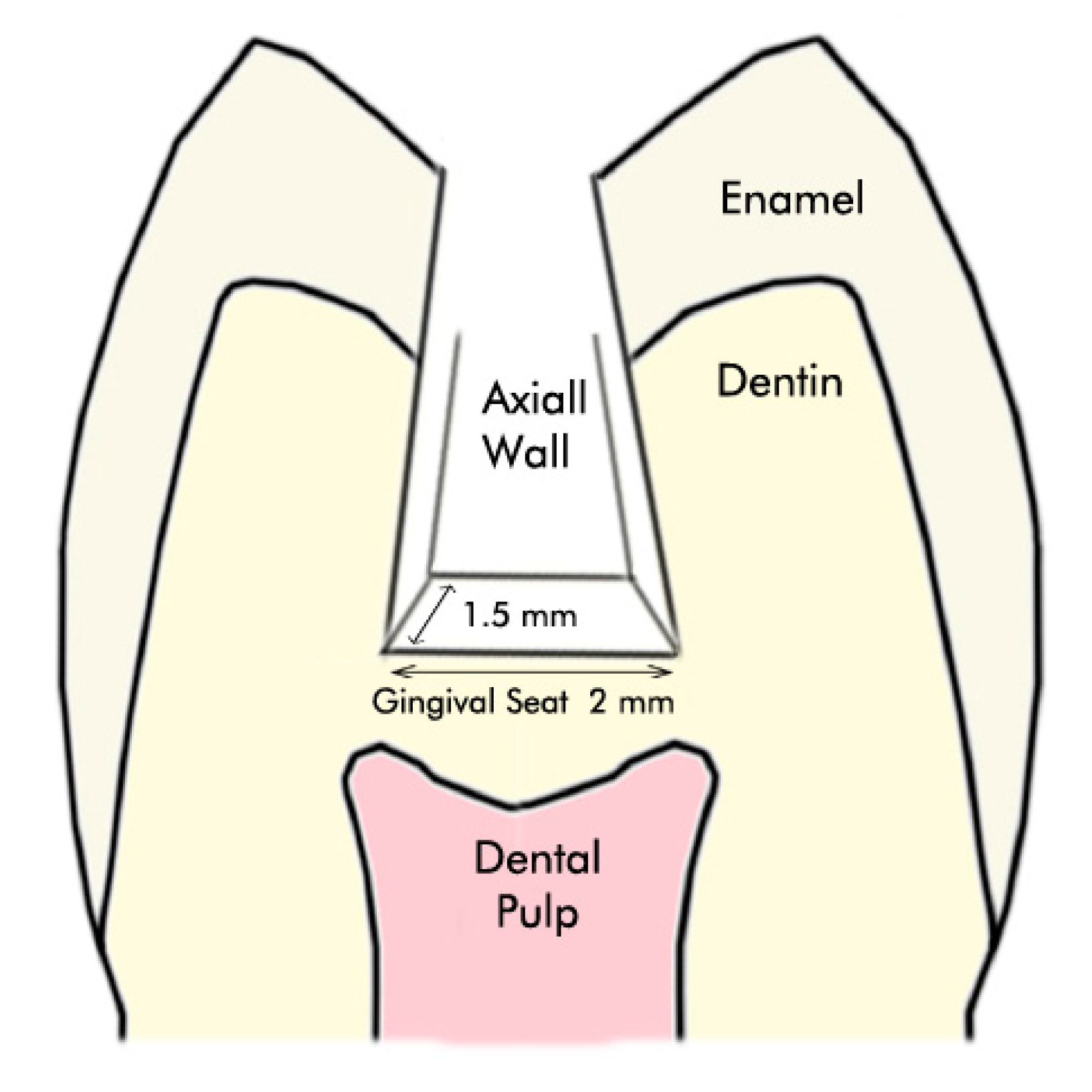
2.1. Tooth Selection and Preparation
2.2. Restorative Procedure
2.3. Thermo Cycling and Scoring Process
2.4. Statistical Analysis
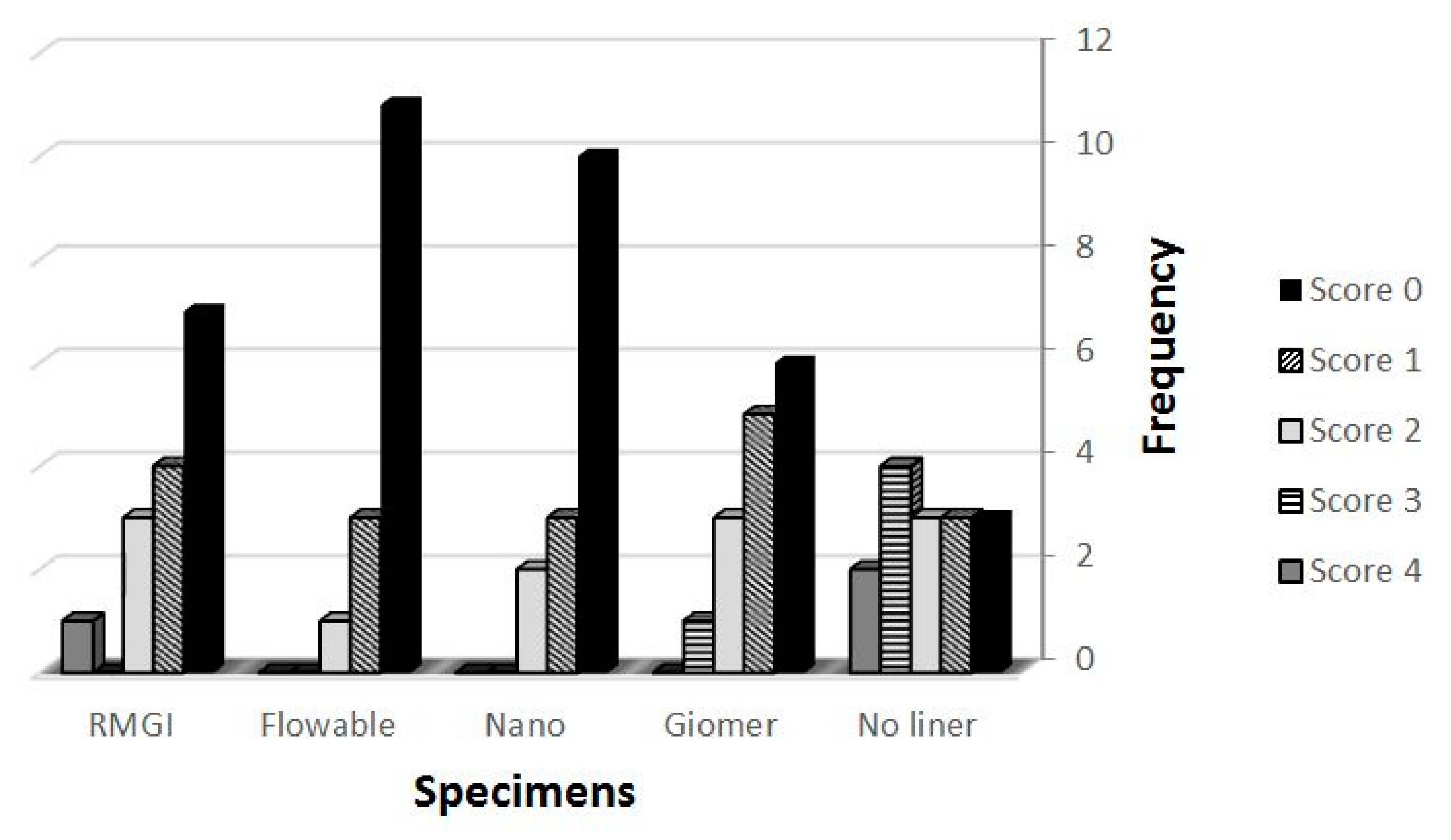
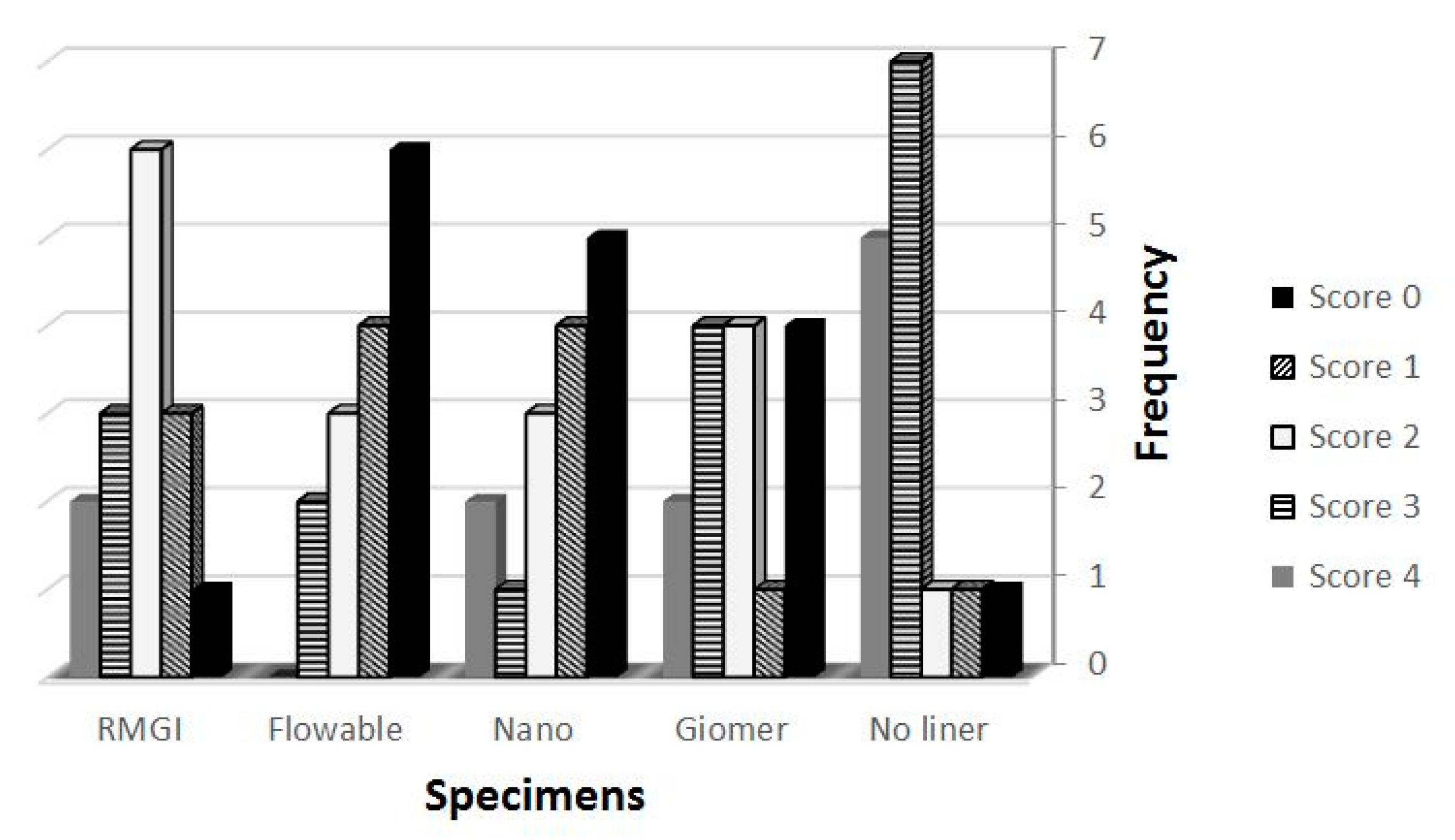
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dimmock, K.; Cummins, T. History of scuba diving tourism. In Scuba Diving Tourism; Routledge: London, UK, 2013; pp. 32–46. [Google Scholar]
- Zadik, Y.; Drucker, S. Diving dentistry: A review of the dental implications of scuba diving. Aust. Dent. J. 2011, 56, 265–271. [Google Scholar] [CrossRef]
- Trimarchi, M.; Bellini, C.; Toma, S.; Bussi, M. Back-and-forth endoscopic septoplasty: Analysis of the technique and outcomes. Int. Forum Allergy Rhinol. 2011, 2, 40–44. [Google Scholar] [CrossRef]
- Gaur, T.K.; Shrivastava, T.V. Barodontalgia: A Clinical Entity. J. Oral Health Community Dent. 2012, 6, 18–20. [Google Scholar] [CrossRef]
- Goethe, M.W.H.G.; Bäter, H.; Laban, C. Barodontalgia and Barotrauma in the Human Teeth: Findings in Navy Divers, Frogmen, and Submariners of the Federal Republic of Germany. Mil. Med. 1989, 154, 491–495. [Google Scholar] [CrossRef] [PubMed]
- Calder, I.M.; Ramsey, J.D. Ondontecrexis—the effects of rapid decompression on restored teeth. J. Dent. 1983, 11, 318–323. [Google Scholar] [CrossRef]
- Shafigh, E.; Fekrazad, R.; Beglou, A. Impact of various pressures on fracture resistance and microleakage of amalgam and composite restorations. Diving Hyperb. Med. J. 2018, 48, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Pamir, T.; Türkün, M. Factors affecting microleakage of a packable resin composite: An in vitro study. Oper. Dent. 2005, 30, 338–345. [Google Scholar] [PubMed]
- Zavattini, A.; Mancini, M.; Higginson, J.; Foschi, F.; Pasquantonio, G.; Mangani, F. Micro-computed tomography evaluation of microleakage of Class II composite restorations: An in vitro study. Eur. J. Dent. 2018, 12, 369–374. [Google Scholar] [CrossRef] [Green Version]
- Xie, D.; Brantley, W.; Culbertson, B.; Wang, G. Mechanical properties and microstructures of glass-ionomer cements. Dent. Mater. 2000, 16, 129–138. [Google Scholar] [CrossRef]
- Korkmaz, Y.; Ozel, E.; Attar, N. Effect of flowable composite lining on microleakage and internal voids in Class II composite restorations. J Adhes Dent 2007, 9, 189–194. [Google Scholar]
- Karaman, E.; Özgünaltay, G. Polymerization Shrinkage of Different Types of Composite Resins and Microleakage with and without Liner in Class II Cavities. Oper. Dent. 2014, 39, 325–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gowda, V.B.; Murthy, B.V.S.; Hegde, S.; Venkataramanaswamy, S.D.; Pai, V.S.; Krishna, R. Evaluation of Gingival Microleakage in Class II Composite Restorations with Different Lining Techniques: An In Vitro Study. Scientifica 2015, 2015, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Levett, D.Z.H.; Millar, I.L. Bubble trouble: A review of diving physiology and disease. Postgrad. Med. J. 2008, 84, 571–578. [Google Scholar] [CrossRef]
- Darsan, J.; Pai, V.S.; Gowda, V.B.; Krishnakumar, G.; Nadig, R.R. Evaluation of Gingival Microleakage in Deep Class II Closed Sandwich Composite Restoration: An In vitro Study. J. Clin. Diagn. Res. 2018, 12, ZC01–ZC05. [Google Scholar] [CrossRef]
- Von Fraunhofer, J.; Marshall, K.R.; Holman, B.G. The effect of base/liner use on restoration leakage. Gen. Dent. 2006, 54, 106–109. [Google Scholar]
- Kaisarly, D.; Meierhofer, D.; El Gezawi, M.; Rösch, P.; Kunzelmann, K. Effects of flowable liners on the shrinkage vectors of bulk-fill composites. Clin. Oral Investig. 2021, 25, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Stefanski, S.; Van Dijken, J.W.V. Clinical performance of a nanofilled resin composite with and without an intermediary layer of flowable composite: A 2-year evaluation. Clin. Oral Investig. 2010, 16, 147–153. [Google Scholar] [CrossRef]
- Kwon, Y.; Ferracane, J.; Lee, I.-B. Effect of layering methods, composite type, and flowable liner on the polymerization shrinkage stress of light cured composites. Dent. Mater. 2012, 28, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Ernst, C.-P.; Cortain, G.; Spohn, M.; Rippin, G.; Willershausen, B. Marginal integrity of different resin-based composites for posterior teeth: An in vitro dye-penetration study on eight resin-composite and compomer-/adhesive combinations with a particular look at the additional use of flow-composites. Dent. Mater. 2002, 18, 351–358. [Google Scholar] [CrossRef]
- Braga, R.R.; Hilton, T.J.; Ferracane, J. Contraction stress of flowable composite materials and their efficacy as stress-relieving layers. J. Am. Dent. Assoc. 2003, 134, 721–728. [Google Scholar] [CrossRef]
- Majety, K.K.; Pujar, M. In vitro evaluation of microleakage of class II packable composite resin restorations using flowable composite and resin modified glass ionomers as intermediate layers. J. Conserv. Dent. 2011, 14, 414–417. [Google Scholar] [CrossRef] [Green Version]
- Kasraei, S.; Azarsina, M.; Majidi, S. In Vitro Comparison of Microleakage of Posterior Resin Composites With and Without Liner Using Two-Step Etch-and-Rinse and Self-etch Dentin Adhesive Systems. Oper. Dent. 2011, 36, 213–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.-G.; Hirano, S. Setting Shrinkage and Hygroscopic Expansion of Resin-modified Glass-ionomer in Experimental Cylindrical Cavities. Dent. Mater. J. 1999, 18, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Gualdi, A.; Cambiaso-Daniel, J.; Gatti, J.; Wurzer, P.; Sljivich, M.; Scherer, S.S.; Pietramaggiori, G.; Bertossi, D.; Botti, C.; Botti, G. Double Triangular Cartilage Excision Otoplasty. Plast. Reconstr. Surg. 2018, 141, 348e–356e. [Google Scholar] [CrossRef]
- El Halim, S.A.; Zaki, D. Comparative Evaluation of Microleakage Among Three Different Glass Ionomer Types. Oper. Dent. 2011, 36, 36–42. [Google Scholar] [CrossRef]
- Ab Malik, N.; Lin, S.L.; Abd Rahman, N.; Jamaludin, M. Effect of Liners on Microleakage in Class Ii Composite Restoration. Sains Malays. 2014, 42, 45–51. [Google Scholar] [CrossRef]
- Atas, O.; Celenk, S.; Aras, A. Microleakage of novel glass ionomer restoration in cavities prepared by Er,Cr: YSGG laser: An in-vitro study. J. Int. Oral Health 2020, 12, 378–384. [Google Scholar] [CrossRef]
- Sunico, M.C.; Shinkai, K.; Katoh, Y. Two-year clinical performance of occlusal and cervical giomer restorations. Oper. Dent. 2005, 30, 282–289. [Google Scholar] [PubMed]
- Fard, E.S.; Monfaredi, K. Optimization of the running speed of ant colony algorithm with address-based hardware method. J. Telecommun. Electron. Comput. Eng. 2015, 7, 1–4. [Google Scholar]
- Safai, P.; Farzaneh, B.; Fekrazad, R. The effects of pressure in vitro on three methods of root canal obturation. Diving Hyperb. Med. J. 2019, 49, 16–20. [Google Scholar] [CrossRef]
- Polizzi, E.; Tetè, G. Manual vs Mechanical Oral Hygiene Procedures: Has the Role of the Dental Hygienist in Phase 2 Post-lockdown Really Changed? Oral Health Prev. Dent. 2020, 18, 1031–1037. [Google Scholar] [PubMed]
- Mandelli, F.; Gherlone, E.; Gastaldi, G.; Ferrari, M. Evaluation of the accuracy of extraoral laboratory scanners with a single-tooth abutment model: A 3D analysis. J. Prosthodont. Res. 2017, 61, 363–370. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Liner | Environment (Subgroup) | Score (Mean) | p-Value |
|---|---|---|---|
| No Liner | Scuba Diving (A1) | 12.30 | 0.039 |
| Ambient Pressure (B1) | 18.70 | ||
| GIOMER | Scuba Diving (A2) | 12.43 | 0.049 |
| Ambient Pressure (B2) | 18.57 | ||
| Nano-Ionomer | Scuba Diving (A3) | 12.47 | 0.043 |
| Ambient Pressure (B3) | 18.53 | ||
| Flowable Composite | Scuba Diving (A4) | 12.57 | 0.042 |
| Ambient Pressure (B4) | 18.43 | ||
| Resin Modified- Glass Ionomer | Scuba Diving (A5) | 11.23 | 0.006 |
| Ambient Pressure (B5) | 19.77 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shahnavazi, M.; Salari, B.; Fekrazad, R. The Effect of Scuba Diving on Microleakage of a Class II Composite Restoration: An In-Vitro Study. Healthcare 2021, 9, 768. https://doi.org/10.3390/healthcare9060768
Shahnavazi M, Salari B, Fekrazad R. The Effect of Scuba Diving on Microleakage of a Class II Composite Restoration: An In-Vitro Study. Healthcare. 2021; 9(6):768. https://doi.org/10.3390/healthcare9060768
Chicago/Turabian StyleShahnavazi, Maryam, Behzad Salari, and Reza Fekrazad. 2021. "The Effect of Scuba Diving on Microleakage of a Class II Composite Restoration: An In-Vitro Study" Healthcare 9, no. 6: 768. https://doi.org/10.3390/healthcare9060768
APA StyleShahnavazi, M., Salari, B., & Fekrazad, R. (2021). The Effect of Scuba Diving on Microleakage of a Class II Composite Restoration: An In-Vitro Study. Healthcare, 9(6), 768. https://doi.org/10.3390/healthcare9060768