
COVID-19 Lockdown Effect on Not Institutionalized Patients with Dementia and Caregivers



Abstract
:1. Introduction
2. Methods
2.1. Neuropsychological Instruments
- Global behavioral symptoms, assessed by the Neuropsychiatric Inventory, NPI [23].
- NPI specific scores, depression, hallucinations and delusions have been registered (Frequency and intensity of symptoms, with the correct score of 4 × 3, considering a maximum score of 12) [23].
- Anxiety, assessed by the Hamilton Anxiety Rating Scale (HAM-A) (score: 0–56; a total score comprised 0–17, estimated mild anxiety; 18–24: mild to moderate anxiety; 25–30: severe anxiety) [24].
- Apathy and abulia, assessed by the Apathy Evaluation Score (AES-C) (clinical examination; score, 18–72; higher scores reflect a higher level of apathy) [25].
- The quality of life, assessed by the Quality of Life in late-stage Dementia Scale (QUALID) [26]; the proxy rating scale consists of 11 items that are rated on a five-point scale. The items are rated by frequency of occurrence, comprising both positive and negative dimensions of concrete and observable mood and performance. Scores are summed to range from 11 to 55. A lower score indicates a higher quality of life.
- 1.
- The caregiver stress was assessed by the Relative Stress Scale, RSS (score 0–60; higher scores reflect more caregiver stress) [27].
- 2.
- 3.
- Anxiety, assessed by the Hamilton Anxiety Rating Scale (HAM-A) (score: 0–56; a total score comprised 0–17, estimated mild anxiety; 18–24: mild to moderate anxiety; 25–30: severe anxiety) [24].
2.2. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guo, Y.R.; Cao, Q.D.; Hong, Z.S.; Tan, Y.Y.; Chen, S.D.; Jin, H.J.; Tan, K.S.; Wang, D.Y.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak—An update on the status. Mil. Med. Res. 2020, 7, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meo, S.A.; Alhowikan, A.M.; Al-Khlaiwi, T.; Meo, I.M.; Halepoto, D.M.; Iqbal, M.; Usmani, A.M.; Hajjar, W.; Ahmed, N. Novel coronavirus 2019-nCoV: Prevalence, biological and clinical characteristics comparison with SARS-CoV and MERS-CoV. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2012–2019. [Google Scholar] [CrossRef]
- Adhikari, S.P.; Meng, S.; Wu, Y.J.; Mao, Y.P.; Ye, R.X.; Wang, Q.Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Li, T.; Barbarino, P.; Gauthier, S.; Brodaty, H.; Molinuevo, J.L.; Xie, H.; Sun, Y.; Yu, E.; Tang, Y.; et al. Dementia care during COVID-19. Lanect 2020, 11, 1190–1191. [Google Scholar] [CrossRef]
- US Centers for Disease Control and Prevention CDC’s Recommendation for the Next 30 Days of Mitigation Strategies for Seattle King, Pierce, and Snohomish Counties Based on Current Situation with Widespread COVID-19 Transmission and Affected Health Care Facilities. 17 March 2020. Available online: https.//www.cdc.gov/coronavirus/2019-ncov/downloads/seattle_community_mitigation.pdf (accessed on 25 May 2020).
- Il Secondo Rapporto Dell’iss Sulla Survey Nazionale Sul Contagio COVID-19 Nelle Strutture Residenziali e Sociosanitarie. Available online: https://www.epicentro.iss.it/ (accessed on 20 May 2020).
- Lai, F.H.; Yan, E.W.; Yu, K.K.; Tsui, W.S.; Chan, D.T.; Yee, B.K. The Protective Impact of Telemedicine on Persons With Dementia and Their Caregivers During the COVID-19 Pandemic. Am. J. Geriatr. Psychiatry 2020, 28, 1175–1184. [Google Scholar] [CrossRef] [PubMed]
- Moretti, R.; Caruso, P.; Storti, B.; Saro, R.; Kassabian, B.; Sala, A.; Giannini, A.; Gazzin, S. Behavior in subcortical vascular dementia with sight pathologies: Visual hallucinations as a consequence of precocious gait imbalance and institutionalization. Neurolog. Sci. 2020. [Google Scholar] [CrossRef]
- Alzheimer’s Disease International. ADI Offers Advice and Support During COVID-19. 17 March 2020. Available online: https://www.alz.co.uk/news/adi-offers-advice-and-support-during-covid-19 (accessed on 18 March 2020).
- Chui, H. Dementia associated with subcortical ischemic vascular disease. Am. Acad. (AAN) Phila. 2001, 5, 89–101. [Google Scholar]
- Chui, H.C.; Victoroff, J.I.; Margolin, D.; Jagust, W.; Shankle, R.; Katzman, R. Criteria for the diagnosis of ischemic vascular dementia proposed by the state of California Alzheimer’s disease diagnostic and treatment centers. Neurology 1992, 42, 473–480. [Google Scholar] [CrossRef]
- Román, G.C.; Tatemichi, T.K.; Erkinjuntti, T.; Cummings, J.L.; Masdeu, J.C.; Garcia, J.H.; Amaducci, L.; Orgogozo, J.M.; Brun, A.; Hofman, A. Vascular dementia: Diagnostic criteria for research studies. Report of the NINDS-AIREN international workshop. Neurology 1993, 43, 250–260. [Google Scholar] [CrossRef]
- Erkinjuntti, T.; Ketonen, L.; Sulkava, R.; Vuorialho, M.; Palo, J. CT in the differential diagnosis between Alzheimer’s disease and vascular dementia. Acta Neurol. Scand. 1987, 75, 262–270. [Google Scholar] [CrossRef]
- Marshall, G.A.; Shchelchkov, E.; Kaufer, D.I.; Ivanco, L.S.; Bohnen, N.I. White matter hyperintensities and cortical acetylcholinesterase activity in parkinsonian dementia. Acta Neurol. Scand. 2006, 113, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Scheltens, P.; Kittner, B. Preliminary results from an MRI/CT-based database for vascular dementia and Alzheimer’s disease. Ann. N. Y. Acad. Sci. 2000, 903, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Cleutjens, F.A.H.M.; Ponds, R.W.H.M.; Spruit, M.A.; Burgmans, S.; Jacobs, H.I.L.; Gronenchield, H.B.M.; Staals, J.; Franssen, F.M.E.; Dijkstra, J.B.; Vanfleteren, L.E.G.W.; et al. The relationship between cerebral small vessel disease, hippocampal volume and cognitive functioning in patients with COPD: An MRI study. Front. Aging Neurosci. 2017, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Blennow, K.; Wallin, A.; Uhlemann, C.; Gottfries, C.G. White-matter lesions on CT in Alzheimer patients: Relation to clinical symptomatology and vascular factors. Acta Neurol. Scand. 1991, 83, 187–193. [Google Scholar] [CrossRef]
- Wallin, A.; Blennow, K. Pathogenetic basis of vascular dementia. Alzheimer Dis. Assoc. Disord. 1991, 5, 91–102. [Google Scholar] [CrossRef]
- Fazekas, F.; Chawluk, J.B.; Alavi, A.; Hurtig, H.I.; Zimmermann, R.A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. Am. J. Roentgenol. 1987, 149, 351–356. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.H.; Lee, J.H.; Seo, S.W.; Ye, B.S.; Cho, H.; Kim, H.J.; Noh, Y.; Yoon, C.W.; Chin, J.H.; Oh, S.J.; et al. Seoul criteria for PIB(-) subcortical vascular dementia based on clinical and MRI variables. Neurology 2014, 82, 1529–1535. [Google Scholar] [CrossRef]
- Korczyn, A.D.; Vakhapova, V.; Grinberg, L.T. Vascular dementia. J. Neurol. Sci. 2012, 322, 2–10. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.W.; MacFall, J.R.; Payne, M.E. Classification of white matter lesions on magnetic resonance imaging in elderly persons. Biol. Psychiatry 2008, 64, 273–280. [Google Scholar] [CrossRef] [Green Version]
- Cummings, J.L.; Mega, M.; Gray, K.; Rosenberg-Thompson, S.; Carusi, D.A.; Gornbein, J. The neuropsychiatric inventory comprehensive assessment of psychopathology in dementia. Neurology 1994, 44, 2308–2314. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Spchol. 1959, 32, 50–55. [Google Scholar] [CrossRef]
- Marin, R.S.; Biedrzycki, R.C.; Firinciogiullari, S. Reliability and validity of the apathy evaluation scale. Psych. Res. 1991, 38, 143–162. [Google Scholar] [CrossRef]
- Weiner, M.F.; Martin-Cook, K.; Svetlik, D.A.; Saine, K.; Foster, B.; Fontaine, C.S. The quality of life in late-stage dementia (QUALID) scale. J. Am. Med. Dir. Assoc. 2000, 1, 114–116. [Google Scholar]
- Ulstein, I.; Brrun Wyller, T.; Engedal, K. The relative stress scale, a useful instrument to identify various aspects of caregiver burden in dementia? Int. J. Geriatr. Psych. 2007, 22, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-Second Edition; The Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Ghisi, M.; Flebus, G.B.; Montanaro, A.; Sanavio, E.; Sica, C. Beck Depression Inventory II: Manuale Italiano; Organizzazioni Speciali: Firenze, Italy, 2006. [Google Scholar]
- Dubois, B.; Pillon, B.; Slachevsky, A.; Litvan, I. Frontal Assessment Battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef] [Green Version]
- Apollonio, I.; Leone, M.; Isella, V.; Piamarta, F.; Consoli, T.; Villa, M.L.; Forapani, E.; Russo, A.; Nichelli, P. The Frontal Assessment Battery: Normative values in an Italian population sample. Neurol. Sci. 2005, 26, 108–116. [Google Scholar] [CrossRef]
- Cerejeira, J.; Lagarto, L.; Mukaetova-Ladinska, E.B. Behavioral and psychological symptoms of dementia. Front Neurol. 2012, 3, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srikanth, S.; Nagaraja, A.V.; Ratnavalli, E. Neuropsychiatric symptoms in dementia-frequency, relationship to dementia severity and comparison in Alzheimer’s disease, vascular dementia and frontotemporal dementia. J. Neurol. Sci. 2005, 236, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Matsuoka, T.; Oba, H.; Narumoto, J. Importance of loneliness in behavioral and psychological symptoms of dementia. Int. J. Geriatr. Psychiatry 2021, 36, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Sutin, A.R.; Stephan, Y.; Luchetti, M.; Terracciano, A. Loneliness and Risk of Dementia. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 75, 1414–1422. [Google Scholar] [CrossRef] [PubMed]
- Penninkilampi, R.; Casey, A.N.; Singh, M.F.; Brodaty, H. The Association between Social Engagement, Loneliness, and Risk of Dementia: A Systematic Review and Meta-Analysis. J. Alzheimers Dis. 2018, 66, 1619–1633. [Google Scholar] [CrossRef] [PubMed]
- Ayalon, L. There is nothing new under the sun: Ageism and intergenerational tension in the age of the COVID-19 outbreak. Int. Psychogeriatr. 2020, 32, 1221–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, T.J.; Rabheru, K.; Peisah, C.; Reichman, W.; Ikeda, M. Loneliness and social isolation during the COVID-19 pandemic. Int. Psychogeriatr. 2020, 32, 1217–1220. [Google Scholar] [CrossRef] [PubMed]
- Chase, T.N. Apathy in neuropsychiatric disease: Diagnosis, pathophysiology, and treatment. Neurotox Res. 2011, 19, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, L.N.; Kales, H.C.; Lyketsos, C.G. Nonpharmacologic management of behavioral symptoms in dementia. JAMA 2012, 308, 2020–2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Centre for Health Protection. Guidelines for Centre-Based Services for the Prevention of the Corona Virus Disease (COVID-19). Available online: www.chp.gov.hk/files/pdf/guideline_for_centre_based_services_eng.pdf (accessed on 26 August 2020).


{kind=link}
| Characteristics | Mean (SD) |
|---|---|
| Age (years) | 75.6 (6.6) |
| Male/female | 102/119 |
| Educational level (yrs school) | 12.1 (2.6) |
| Time of follow-up (months) before 10 March 2020 | 17.4 (3.1) |
| Variables | 10 March | 18 May | 18 July | F Chi2 Value | DF | p Value |
|---|---|---|---|---|---|---|
| NPI (0–144) | 16.3 ± 2.1 | 36.4 ± 5.3 | 30.1 ± 2.3 | 0.91 | 2.77 | 0.01 |
| HAM-A (0–56) | 19.1 ± 2.7 | 39.7 ± 7.1 | 34.6 ± 5.2 | 0.89 | 2.65 | 0.01 |
| AES-C (18–71) | 21.3 ± 3.4 | 31.4 ± 2.5 | 28.3 ± 2.7 | 0.78 | 2.31 | 0.01 |
| QUALID (11–55) | 24.5 ± 2.7 | 35.4 ± 3.7 | 26.1 ± 3.1 | 0.97 | 2.4 | 0.01 |
| NPI Hallucinations (0–12) | 3.5 ± 0.3 | 11.2 ± 0.6 | 7.7 ± 4.1 | 0.76 | 2.36 | 0.01 |
| NPI Delusions (0–12) | 0.9 ± 0.2 | 11.3 ± 0.7 | 8.3 ± 0.6 | 0.67 | 2.17 | 0.01 |
| NPI Depression (0–12) | 9.6 ± 1.1 | 10.9 ± 0.8 | 9.7 ± 0.9 | 0.78 | 2.34 | 0.05 |
| Variables | Low-Medium sVAD (146 pts) Group A | Severe sVAD (75 pts) Group B | F Chi2 Value | DF | p Value |
|---|---|---|---|---|---|
| FAB | 12.3 ± 3.4 | 9.5 ± 2.7 | 0.91 | 2.07 | 0.01 |
| Fazekas Scale | 1.9 ± 1.6 | 2.7 ± 0.1 | 0.98 | 2.65 | 0.01 |
| Variables | 10 March | 18 May | 18 July | F Chi2 Value | DF | p Value |
|---|---|---|---|---|---|---|
| NPI (0–144) | 11.3 ± 1.1 | 31.1 ± 0.3 | 28.4 ± 1.1 | 0.76 | 2.4 | 0.01 |
| HAM-A (0–56) | 17.3 ± 1.2 | 32.3 ± 3.1 | 27.1 ± 3.1 | 0.91 | 2.3 | 0.01 |
| AES-C (18–71) | 18.3 ± 1.2 | 27.1 ± 1.3 | 25.1 ± 1.8 | 0.87 | 2.4 | 0.01 |
| QUALID (11–55) | 21.2 ± 1.4 | 30.1 ± 1.2 | 24.2 ± 1.3 | 0.69 | 2.1 | 0.01 |
| NPI Hallucinations (0–12) | 3.1 ± 0.1 | 8.1 ± 1.1 | 6.9 ± 1.2 | 0.56 | 2.1 | 0.01 |
| NPI Delusions (0–12) | 0.7 ± 0.1 | 7.8 ± 1.2 | 5.3 ± 0.3 | 0.67 | 2.2 | 0.01 |
| NPI Depression (0–12) | 8.1 ± 0.6 | 10.1 ± 0.3 | 8.7 ± 0.4 | 0.89 | 2.1 | 0.05 |
| Variables | 10 March | 18 May | 18 July | F Chi2 Value | DF | p Value |
| NPI (0–144) | 24.1 ± 1.6 | 39.1 ± 3.1 | 32.4 ± 1.5 | 0.93 | 2.5 | 0.01 |
| HAM-A (0–56) | 21.3 ± 1.1 | 43.1 ± 2.5 | 37.2 ± 2.3 | 0.88 | 2.4 | 0.01 |
| AES-C (18–71) | 25.1 ± 1.7 | 36.1 ± 1.2 | 32.1 ± 1.5 | 0.98 | 2.4 | 0.01 |
| QUALID (11–55) | 26.1 ± 1.2 | 37.3 ± 2.1 | 29.7 ± 1.2 | 0.79 | 2.3 | 0.01 |
| NPI Hallucinations (0–12) | 4.2 ± 0.6 | 11.5. ± 0.5 | 9.7 ± 2.1 | 0.76 | 2.6 | 0.01 |
| NPI Delusions (0–12) | 1.3 ± 0.3 | 11.6 ± 0.1 | 9.1 ± 0.4 | 0.67 | 2.5 | 0.01 |
| NPI Depression (0–12) | 9.7 ± 0.7 | 11.1 ± 0.8 | 9.4 ± 0.5 | 081 | 2.4 | 0.05 |
| Variables | 10 March Group A | 10 March Group B | F Chi2 Value | DF | p Value |
|---|---|---|---|---|---|
| NPI (0–144) | 11.3 ± 1.1 | 24.1 ± 1.6 | 0.87 | 2.5 | 0.01 |
| HAM-A (0–56) | 17.3 ± 1.2 | 21.3 ± 1.1 | 0.89 | 2.4 | 0.01 |
| AES-C (18–71) | 18.3 ± 1.2 | 25.1 ± 1.7 | 0.91 | 2.4 | 0.01 |
| QUALID (11–55) | 21.2 ± 1.4 | 26.1 ± 1.2 | 0.83 | 2.3 | 0.01 |
| NPI Hallucinations (0–12) | 3.1 ± 0.1 | 4.2 ± 0.6 | 0.87 | 2.6 | 0.057 |
| NPI Delusions (0–12) | 0.7 ± 0.1 | 1.3 ± 0.3 | 0.91 | 2.5 | 0.056 |
| NPI Depression (0–12) | 8.1 ± 0.6 | 9.7 ± 0.7 | 0.87 | 2.4 | 0.05 |
| Variables | 18 May Group A | 18 May Group B | F Chi2 Value | DF | pValue |
| NPI (0–144) | 31.1 ± 0.3 | 39.1 ± 3.1 | 0.78 | 2.5 | 0.05 |
| HAM-A (0–56) | 32.3 ± 3.1 | 43.1 ± 2.5 | 0.93 | 2.4 | 0.01 |
| AES-C (18–71) | 27.1 ± 1.3 | 36.1 ± 1.2 | 0.94 | 2.4 | 0.01 |
| QUALID (11–55) | 30.1 ± 1.2 | 37.3 ± 2.1 | 0.81 | 2.3 | 0.05 |
| NPI Hallucinations (0–12) | 8.1 ± 1.1 | 11.5 ± 0.5 | 0.83 | 2.6 | 0.01 |
| NPI Delusions (0–12) | 7.8 ± 1.2 | 11.6 ± 0.1 | 0.84 | 2.5 | 0.01 |
| NPI Depression (0–12) | 10.1 ± 0.3 | 11.1 ± 0.8 | 0.91 | 2.4 | 0.056 |
| Variables | 18 July Group A | 18 July Group B | F Chi2 Value | DF | pValue |
| NPI (0–144) | 28.4 ± 1.1 | 32.4 ± 1.5 | 0.91 | 2.5 | 0.01 |
| HAM-A (0–56) | 27.1 ± 3.1 | 37.2 ± 2.3 | 0.79 | 2.4 | 0.01 |
| AES-C (18–71) | 25.1 ± 1.8 | 32.1 ± 1.5 | 0.93 | 2.4 | 0.01 |
| QUALID (11–55) | 24.2 ± 1.3 | 29.7 ± 1.2 | 0.87 | 2.3 | 0.01 |
| NPI Hallucinations (0–12) | 6.9 ± 1.2 | 9.7 ± 2.1 | 0.89 | 2.6 | 0.01 |
| NPI Delusions (0–12) | 5.3 ± 0.3 | 9.1 ± 0.4 | 0.82 | 2.5 | 0.01 |
| NPI Depression (0–12) | 8.7 ± 0.4 | 9.4 ± 0.5 | 0.85 | 2.4 | 0.05 |
| Variables | 10 March (p Value) | 18 May (p Value) | 18 July (p Value) | ||
| NPI (0–144) | −12.8 ± 0.5 (p < 0.01) | −8 ± 2.8 (p < 0.01) | −4 ± 0.4 (p < 0.05) | ||
| HAM-A (0–56) | −4 ± 0.1 (p < 0.05) | −10.8 ± 0.6 (p < 0.01) | −10.1 ± 0.8 (p < 0.01) | ||
| AES-C (18–71) | −6.8 ± 0.5 (p < 0.01) | −9 ± 0.1 (p < 0.01) | −7 ± 0.3 (p < 0.01) | ||
| QUALID (11–55) | −4.9 ± 0.2 (p < 0.05) | −7.2 ± 0.9 (p < 0.01) | −5.5 ± 0.1 (p < 0.01) | ||
| NPI Hallucinations (0–12) | −1.1 ± 0.5 (NS) | −3.4 ± 0.6 (p < 0.01) | −2.8 ± 0.9 (p < 0.01) | ||
| NPI Delusions (0–12) | −0.6 ± 0.2 (NS) | −3.8 ± 0.9 (p < 0.01) | −3.8 ± 0.1 (p < 0.01) | ||
| NPI Depression (0–12) | −0.3 ± 0.1 (NS) | 1 ± 0.5 (p < 0.5) | 0.7 ± 0.1 (NS) | ||
| B | p Value | SE | 95% CI | |
|---|---|---|---|---|
| NPI | ||||
| Model 1 | 0.12 | 0.56 | 3.56 | 0.2–0.9 |
| Model 2 | 0.88 | 0.01 | 3.12 | 0.31–1.18 |
| HAM-A | ||||
| Model 1 | 0.37 | 0.47 | 3.43 | 0.2–0.7 |
| Model 2 | 0.72 | 0.01 | 3.17 | 0.21–2.19 |
| AES-C | ||||
| Model 1 | 0.24 | 0.43 | 2.67 | 0.3–2.4 |
| Model 2 | 0.94 | 0.01 | 3.21 | 0.5–2.8 |
| RSS | ||||
| Model 1 | 0.43 | 0.54 | 2.78 | 0.1–4.9 |
| Model 2 | 0.88 | 0.01 | 2.12 | 0.9–2.9 |
| QUALID | ||||
| Model 1 | 0.56 | 0.78 | 2.34 | 0.4–3.4 |
| Model 2 | 0.71 | 0.01 | 2.89 | 0.6–2.8 |
| Drugs | 10 March 2020 | 18 May 2020 | 18 June 2020 | |||
|---|---|---|---|---|---|---|
| Group A | Group B | Group A | Group B | Group A | Group B | |
| Benzodiazepines | 44 (30%) | 13 (17%) | 59 (41%) | 32 (43%) | 59 (41%) | 32 (43%) |
| Typ. Neurolep. | 19 (13%) | 19 (25%) | 27 (16%) | 22 (30%) | 27 (16%) | 22 (30%) |
| Atyp. Neurolep. | 16 (11%) | 36 (48%) | 30 (21%) | 38 (51%) | 30 (21%) | 38 (51%) |
| Two drugs together | 0 | 7 (9%) | 28 (19%) | 37 (49%) | 14 (10%) | 11 (15%) |
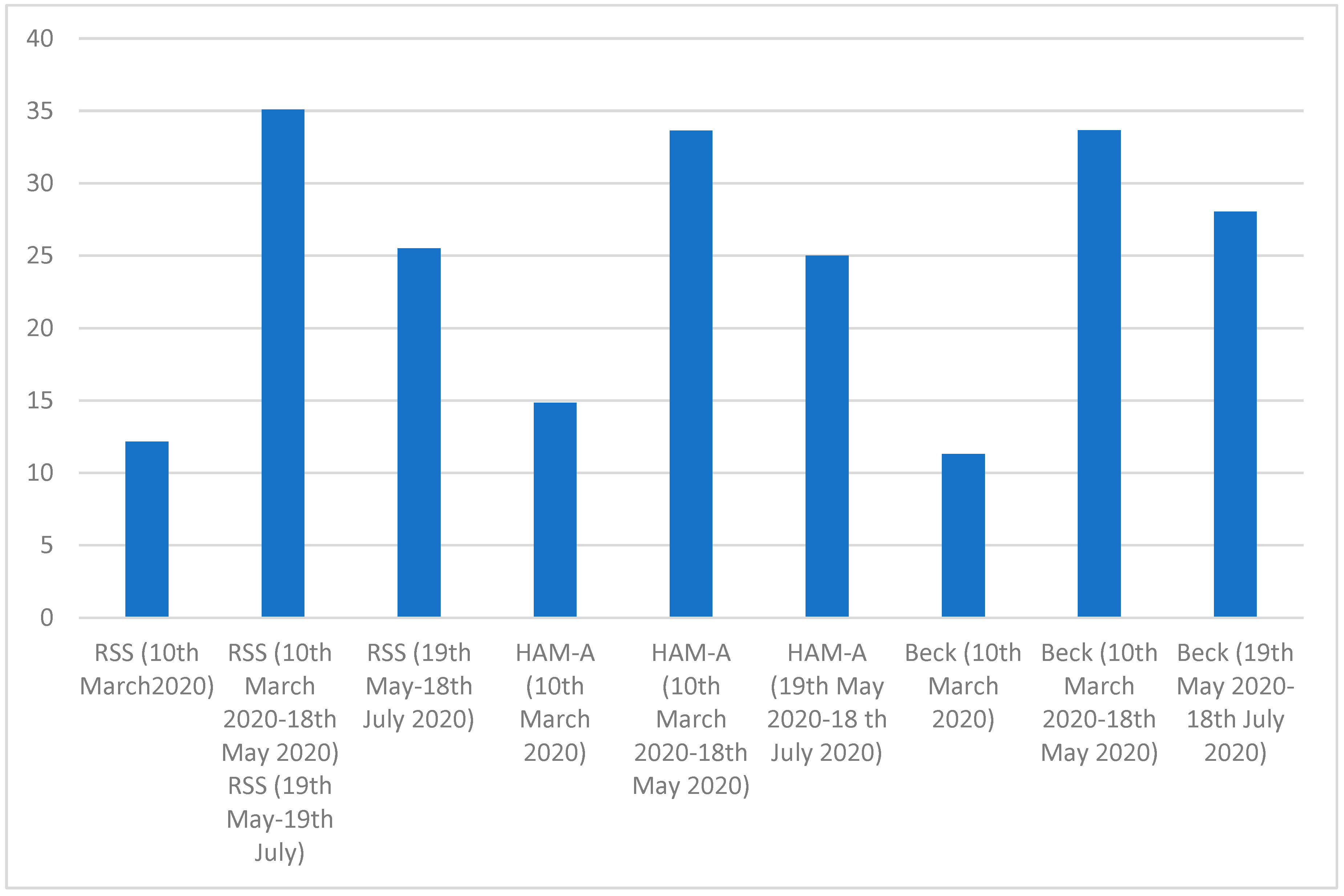
| Variables | 10 March | 18 May | 18 July | F Chi2 Value | DF | p Value |
|---|---|---|---|---|---|---|
| RSS (0–66) | 12.15 ± 1.1 | 35.1 ± 1.3 | 25.5 ± 1.9 | 0.98 | 2.77 | 0.01 |
| HAM-A (0–56) | 14.9 ± 2.3 | 33.7 ± 2.1 | 25.1 ± 3.2 | 0.82 | 2.61 | 0.01 |
| Beck | 11.3 ± 1.2 | 33.7 ± 1.4 | 28.1 ± 1.3 | 0.67 | 2.56 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moretti, R.; Caruso, P.; Giuffré, M.; Tiribelli, C. COVID-19 Lockdown Effect on Not Institutionalized Patients with Dementia and Caregivers. Healthcare 2021, 9, 893. https://doi.org/10.3390/healthcare9070893
Moretti R, Caruso P, Giuffré M, Tiribelli C. COVID-19 Lockdown Effect on Not Institutionalized Patients with Dementia and Caregivers. Healthcare. 2021; 9(7):893. https://doi.org/10.3390/healthcare9070893
Chicago/Turabian StyleMoretti, Rita, Paola Caruso, Mauro Giuffré, and Claudio Tiribelli. 2021. "COVID-19 Lockdown Effect on Not Institutionalized Patients with Dementia and Caregivers" Healthcare 9, no. 7: 893. https://doi.org/10.3390/healthcare9070893
APA StyleMoretti, R., Caruso, P., Giuffré, M., & Tiribelli, C. (2021). COVID-19 Lockdown Effect on Not Institutionalized Patients with Dementia and Caregivers. Healthcare, 9(7), 893. https://doi.org/10.3390/healthcare9070893