
The Cut-off Value of Physical Activity for Undergoing Total Knee Arthroplasty in Patients with Knee Osteoarthritis

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Sample Size
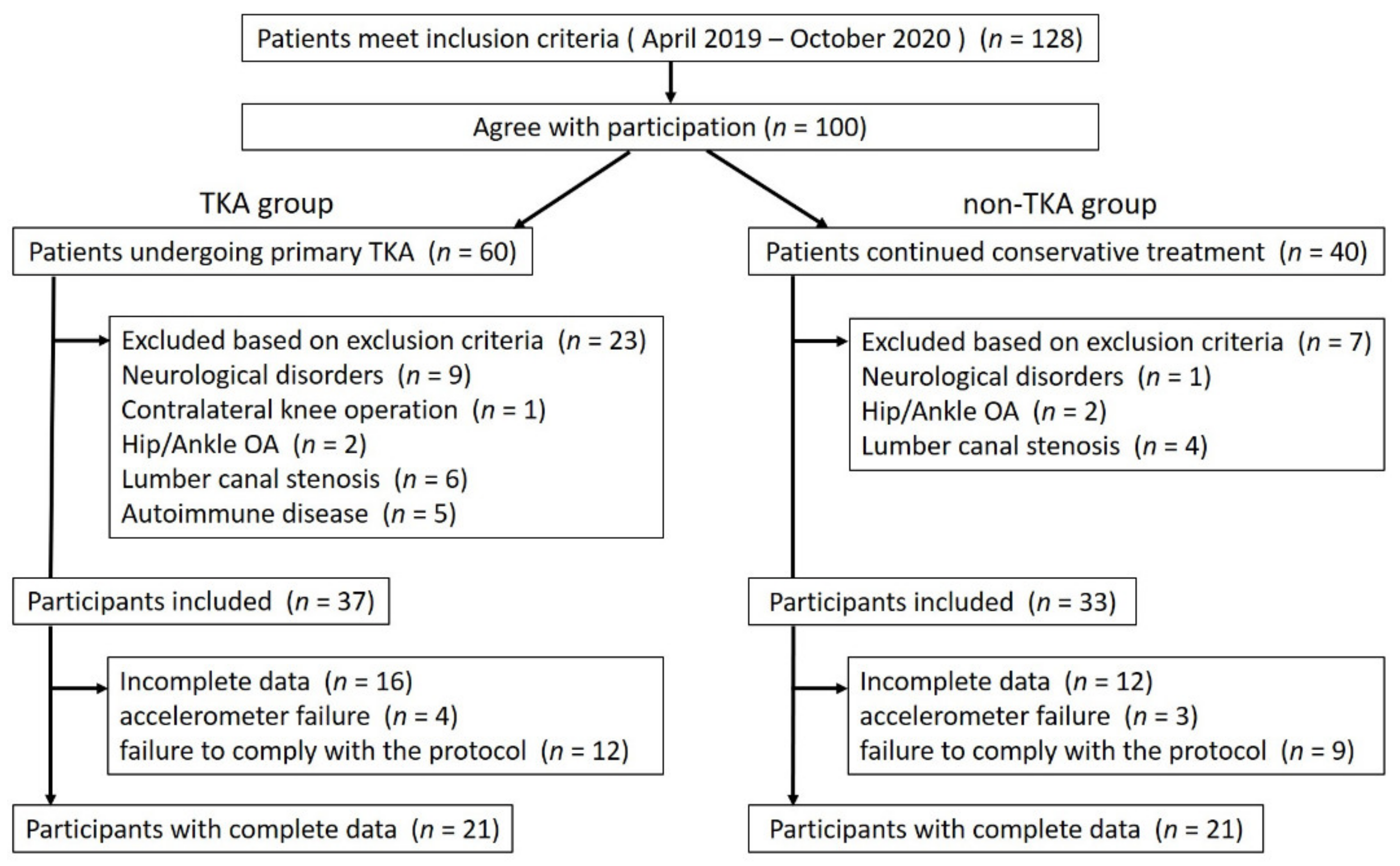
2.3. Enrolment
2.4. Patient Characteristics and Assessment of Disease Severity
2.5. Decision Undergoing TKA
2.6. Measurement of PA
2.7. Allocation
2.8. Statistical Analyses
2.8.1. Comparison of Parameters between the Groups
2.8.2. Cut-off Value Analysis
2.8.3. PA-Related Predictors for Undergoing TKA
3. Results
3.1. Characteristics of the Participants
3.2. Comparison of Variables between the TKA Group and the Non-TKA Group
3.3. Cut-off Value
3.4. Predictors for Undergoing TKA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kloppenburg, M.; Berenbaum, F. Osteoarthritis Year in Review 2019: Epidemiology and Therapy. Osteoarthr. Cartil. 2020, 28, 242–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshimura, N.; Shigeyuki, M.; Oka, H.; Mabuchi, A.; En-Yo, Y.; Yoshida, M.; Saika, A.; Yoshida, H.; Suzuki, T.; Yamamoto, S.; et al. Prevalence of Knee Osteoarthritis, Lumbar Spondylosis, and Osteoporosis in Japanese Men and Women: The Research on Osteoarthritis/Osteoporosis against Disability Study. J. Bone Miner. Metab. 2009, 27, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Michael, J.W.P.; Schlüter-Brust, K.U.; Eysel, P. The Epidemiology, Etiology, Diagnosis, and Treatment of Osteoarthritis of the Knee. Dtsch. Ärzteblatt Int. 2010, 107, 152–162. [Google Scholar] [CrossRef]
- Akazawa, M.; Mimura, W.; Togo, K.; Ebata, N.; Harada, N.; Murano, H.; Abraham, L.; Fujii, K. Patterns of Drug Treatment in Patients with Osteoarthritis and Chronic Low Back Pain in Japan: A Retrospective Database Study. J. Pain Res. 2019, 12, 1631–1648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gademan, M.G.J.; Hofstede, S.N.; Vliet Vlieland, T.P.M.; Nelissen, R.G.H.H.; Marang-van de Mheen, P.J. Indication Criteria for Total Hip or Knee Arthroplasty in Osteoarthritis: A State-of-the-Science Overview. BMC Musculoskelet. Disord. 2016, 17, 463. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, J.; Lange, T.; Günther, K.P.; Kopkow, C.; Rataj, E.; Apfelbacher, C.; Aringer, M.; Böhle, E.; Bork, H.; Dreinhöfer, K.; et al. Indication Criteria for Total Knee Arthroplasty in Patients with Osteoarthritis—A Multi-Perspective Consensus Study. Z. Orthop. Unf. 2017, 155, 539–548. [Google Scholar] [CrossRef]
- Commissioning Guide: Painful Osteoarthritis of the Knee. Available online: https://www.boa.ac.uk/resources/painful-oa-knee-guide-final--pdf.html (accessed on 25 June 2021).
- Kellgren, J.H.; Lawrence, J.S. Radiological Assessment of Osteo-Arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Allen, K.D.; Coffman, C.J.; Golightly, Y.M.; Stechuchak, K.M.; Keefe, F.J. Daily Pain Variations among Patients with Hand, Hip, and Knee Osteoarthritis. Osteoarthr. Cartil. 2009, 17, 1275–1282. [Google Scholar] [CrossRef] [Green Version]
- Bedson, J.; Croft, P.R. The Discordance between Clinical and Radiographic Knee Osteoarthritis: A Systematic Search and Summary of the Literature. BMC Musculoskelet. Disord. 2008, 9, 116. [Google Scholar] [CrossRef] [Green Version]
- Paterson, D.H.; Warburton, D.E.R. Physical Activity and Functional Limitations in Older Adults: A Systematic Review Related to Canada’s Physical Activity Guidelines. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 38. [Google Scholar] [CrossRef] [Green Version]
- Jordan, K.M.; Arden, N.K.; Doherty, M.; Bannwarth, B.; Bijlsma, J.W.J.; Dieppe, P.; Gunther, K.; Hauselmann, H.; Herrero-Beaumont, G.; Kaklamanis, P.; et al. EULAR Recommendations 2003: An Evidence Based Approach to the Management of Knee Osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann. Rheum. Dis. 2003, 62, 1145–1155. [Google Scholar] [CrossRef]
- Di Sebastiano, K.M.; Chulak-Bozzer, T.; Vanderloo, L.M.; Faulkner, G. Don’t Walk So Close to Me: Physical Distancing and Adult Physical Activity in Canada. Front. Psychol. 2020, 11, 1895. [Google Scholar] [CrossRef]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too Much Sitting: The Population Health Science of Sedentary Behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef]
- Saint-Maurice, P.F.; Troiano, R.P.; Matthews, C.E.; Kraus, W.E. Moderate-to-Vigorous Physical Activity and All-Cause Mortality: Do Bouts Matter? J. Am. Heart Assoc. 2018, 7, e007678. [Google Scholar] [CrossRef] [Green Version]
- Yasunaga, A.; Togo, F.; Watanabe, E.; Park, H.; Shephard, R.J.; Aoyagi, Y. Yearlong Physical Activity and Health-Related Quality of Life in Older Japanese Adults: The Nakanojo Study. J. Aging Phys. Act. 2006, 14, 288–301. [Google Scholar] [CrossRef] [Green Version]
- Physical Activity Guidelines for Americans. 2008. Available online: https://health.gov/sites/default/files/2019-09/paguide.pdf (accessed on 25 June 2021).
- Nemoto, Y.; Suzuki, K. Prevention of Dementia Onset with Targeting at Physical Activity and Social Participation Among Japanese Community-Dwelling Older Adults. Arch. Phys. Health Sports Med. 2018, 1, 39–43. [Google Scholar]
- Matsunaga, Y.; Fujita, K.; Ide, S.; Tabuchi, Y.; Mawatari, M. Improved Levels of Physical Activity in Patients over 75 Years Following Total Knee Arthroplasty. J. Orthop. Surg. 2019, 27, 2309499019873363. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Bull. World Health Organ. 2007, 85, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software “EZR” for Medical Statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandrekar, J.N. Receiver Operating Characteristic Curve in Diagnostic Test Assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alghadir, A.H.; Anwer, S.; Iqbal, A.; Iqbal, Z.A. Test-Retest Reliability, Validity, and Minimum Detectable Change of Visual Analog, Numerical Rating, and Verbal Rating Scales for Measurement of Osteoarthritic Knee Pain. J. Pain Res. 2018, 11, 851–856. [Google Scholar] [CrossRef] [Green Version]
- Schneider, P.L.; Crouter, S.E.; Lukajic, O.; Bassett, D.R. Accuracy and Reliability of 10 Pedometers for Measuring Steps over a 400-m Walk. Med. Sci. Sports Exerc. 2003, 35, 1779–1784. [Google Scholar] [CrossRef]
- Sliepen, M.; Brandes, M.; Rosenbaum, D. Current Physical Activity Monitors in Hip and Knee Osteoarthritis: A Review. In Arthritis Care and Research; John Wiley and Sons Inc.: Hoboken, NJ, USA, 2017; pp. 1460–1466. [Google Scholar] [CrossRef] [Green Version]
- Aoyagi, Y.; Park, H.; Park, S.; Shephard, R.J. Habitual Physical Activity and Health-Related Quality of Life in Older Adults: Interactions between the Amount and Intensity of Activity (the Nakanojo Study). Qual. Life Res. 2010, 19, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Kumahara, H.; Schutz, Y.; Ayabe, M.; Yoshioka, M.; Yoshitake, Y.; Shindo, M.; Ishii, K.; Tanaka, H. The Use of Uniaxial Accelerometry for the Assessment of Physical-Activity-Related Energy Expenditure: A Validation Study against Whole-Body Indirect Calorimetry. Br. J. Nutr. 2004, 91, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Beckers, L.W.M.E.; Smeets, R.J.E.M. Methodological and Interpretive Concerns about Beemster et al.’s Article “The Interpretation of Change Score of the Pain Disability Index after Vocational Rehabilitation Is Baseline Dependent”: A Letter to the Editor. Health Qual. Life Outcomes 2020, 18, 301. [Google Scholar] [CrossRef] [PubMed]
- Turk, D.C.; Dworkin, R.H.; Allen, R.R.; Bellamy, N.; Brandenburg, N.; Carr, D.B.; Cleeland, C.; Dionne, R.; Farrar, J.T.; Galer, B.S.; et al. Core Outcome Domains for Chronic Pain Clinical Trials: IMMPACT Recommendations. Pain 2003, 106, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, H.; Ikemoto, T.; Honjo, H.; Akao, M.; Tsujimoto, T.; Ushida, T. One-Year Results of Voluntary-Based Supervised Exercise or Treatment at Orthopedic Clinic for Radiographic Severe Knee Osteoarthritis. J. Phys. Ther. Sci. 2016, 28, 906–910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandes, M.; Ringling, M.; Winter, C.; Hillmann, A.; Rosenbaum, D. Changes in Physical Activity and Health-Related Quality of Life During the First Year After Total Knee Arthroplasty. Arthritis Care Res. 2011, 63, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Pua, Y.H.; Seah, F.J.T.; Clark, R.A.; Lian-Li Poon, C.; Tan, J.W.M.; Chong, H.C. Factors Associated with Gait Speed Recovery after Total Knee Arthroplasty: A Longitudinal Study. Semin. Arthritis Rheum. 2017, 46, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Lützner, C.; Kirschner, S.; Lützner, J. Patient Activity After TKA Depends on Patient-Specific Parameters. Clin. Orthop. Relat. Res. 2014, 472, 3933–3940. [Google Scholar] [CrossRef] [Green Version]
- Miura, Y.; Fukumoto, Y.; Miura, T.; Shimada, K.; Asakura, M.; Kadokami, T.; Ando, S.I.; Miyata, S.; Sakata, Y.; Daida, H.; et al. Impact of Physical Activity on Cardiovascular Events in Patients with Chronic Heart Failure—A Multicenter Prospective Cohort Study. Circ. J. 2013, 77, 2963–2972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, L.J.D.; Azevedo, M.R.; Matsudo, S.; Lopes, G.S. Association between Levels of Physical Activity and Use of Medication among Older Women Associação Entre Nível de Atividade Física e Uso de Medicamentos Entre Mulheres Idosas. Cad. Saude Publica 2012, 28, 463–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suarez-Almazor, M.E.; Richardson, M.; Kroll, T.L.; Sharf, B.F. A Qualitative Analysis of Decision-Making for Total Knee Replacement in Patients with Osteoarthritis. J. Clin. Rheumatol. 2010, 16, 158–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | TKA (n = 21) | non-TKA (n = 21) | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (IQR) | p-Value S–W Test # | Mean ± SD | Median (IQR) | p-Value S–W Test # | Non-Adjusted | Adjusted | ||
| Epidemiologic | Age (years) | 75.86 ± 5.52 | 75 (71, 79) | 0.442 | 74.24 ± 6.38 | 74 (70, 78) | 0.872 | 0.384 | — |
| Sex (m:f) | 6:15 | — | 3:18 | — | 0.259 | — | |||
| BMI (kg/m2) | 25.28 ± 4.85 | 23.74 (21.63, 26.92) | 0.002 ** | 25.30 ± 2.88 | 25.0 (23.3, 26.4) | 0.154 | 0.435 | — | |
| KL grade (II:III:IV) | 1:2:18 | — | 5:10:6 | — | 0.001 ** | — | |||
| PA | Step (step/day) | 3681.42 ± 1437.10 | 3614.71 (2906.71, 4631.00) | 0.513 | 5109.37 ± 2449.51 | 4331.00 (3678.57, 5855.86) | 0.109 | 0.028 * | 0.537 |
| LPA (min/day) | 39.86 ± 15.93 | 36.42 (29.06, 48.77) | 0.540 | 47.86 ± 23.83 | 45.19 (30.37, 59.11) | 0.275 | 0.208 | 0.698 | |
| MVPA (min/day) | 2.47 ± 2.32 | 1.53 (0.66, 4.24) | 0.005 ** | 8.39 ± 7.64 | 7.04 (1.78, 12.51) | 0.014 * | 0.002 ** | 0.012 * | |
| Independent Variable | β | Odds Ratio | p-Value | 95% CI |
|---|---|---|---|---|
| KL grade | 1.38 | 3.97 | 0.049 * | 1.01–15.66 |
| Knee pain | 1.01 | 2.75 | 0.019 * | 1.18–6.42 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okamoto, T.; Ikemoto, T.; Miyagawa, H.; Ishida, T.; Akao, M.; Takata, T.; Kobayakawa, K.; Yamanashi, Y.; Inoue, M.; Nakaso, Y.; et al. The Cut-off Value of Physical Activity for Undergoing Total Knee Arthroplasty in Patients with Knee Osteoarthritis. Healthcare 2021, 9, 1063. https://doi.org/10.3390/healthcare9081063
Okamoto T, Ikemoto T, Miyagawa H, Ishida T, Akao M, Takata T, Kobayakawa K, Yamanashi Y, Inoue M, Nakaso Y, et al. The Cut-off Value of Physical Activity for Undergoing Total Knee Arthroplasty in Patients with Knee Osteoarthritis. Healthcare. 2021; 9(8):1063. https://doi.org/10.3390/healthcare9081063
Chicago/Turabian StyleOkamoto, Takuya, Tatsunori Ikemoto, Hirofumi Miyagawa, Tomohiro Ishida, Machiko Akao, Takuya Takata, Kyosuke Kobayakawa, Yuki Yamanashi, Masayuki Inoue, Yuichiro Nakaso, and et al. 2021. "The Cut-off Value of Physical Activity for Undergoing Total Knee Arthroplasty in Patients with Knee Osteoarthritis" Healthcare 9, no. 8: 1063. https://doi.org/10.3390/healthcare9081063
APA StyleOkamoto, T., Ikemoto, T., Miyagawa, H., Ishida, T., Akao, M., Takata, T., Kobayakawa, K., Yamanashi, Y., Inoue, M., Nakaso, Y., Ushida, T., & Deie, M. (2021). The Cut-off Value of Physical Activity for Undergoing Total Knee Arthroplasty in Patients with Knee Osteoarthritis. Healthcare, 9(8), 1063. https://doi.org/10.3390/healthcare9081063