
Korean Nursing Students’ Emotional Response Types to Pandemic: Application of Q-Methodology


Abstract
:1. Introduction
The Rationale for This Research
2. Materials and Methods
2.1. Research Design
2.2. Research Procedure
2.2.1. Q-Population Construction and Q-Sample Selection
2.2.2. P-Sample
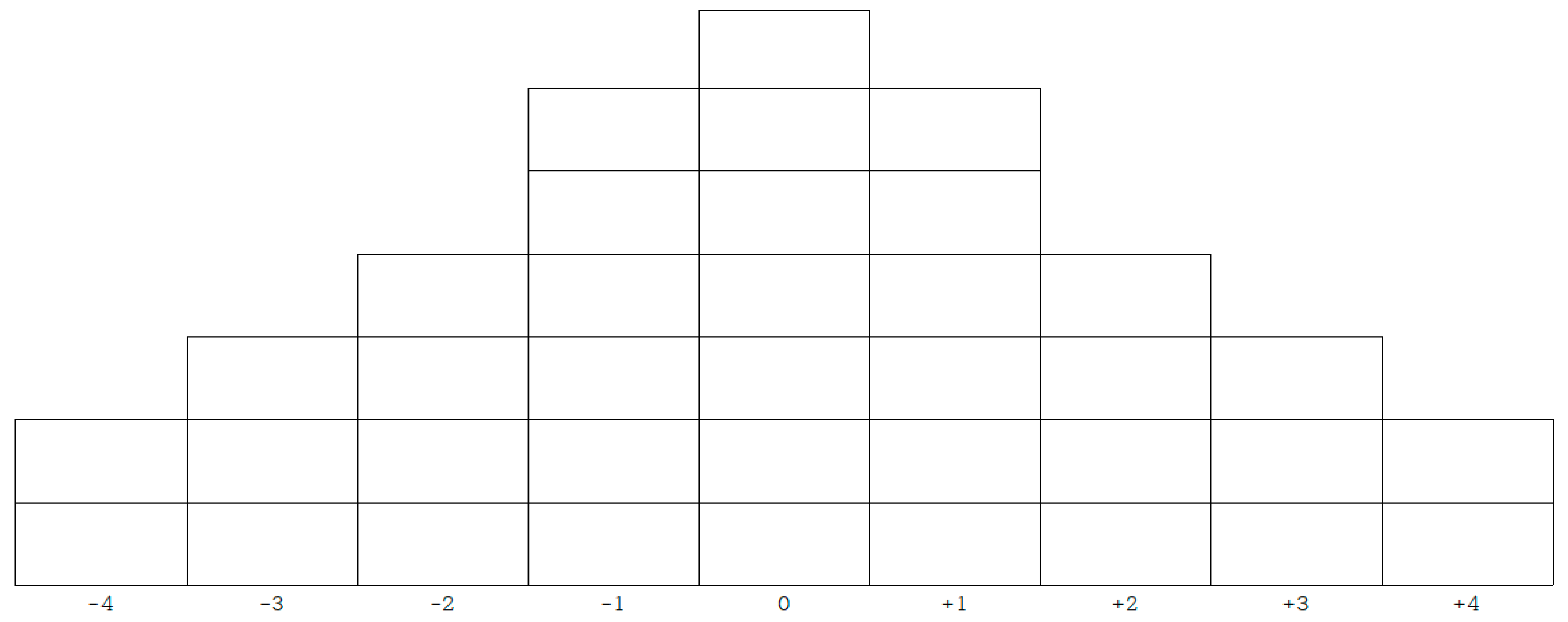
2.2.3. Q-Classification Process and Method
2.3. Ethical Considerations
2.4. Method of Data Analysis
3. Results
3.1. Formation of Q-Types
3.2. Characteristics by Type of Emotional Response
3.2.1. Type 1: Self-Protection
3.2.2. Type 2: Pessimism about the Current Situation
3.2.3. Type 3: Realistic Optimism
3.2.4. Type 4: Developmental-Seeking
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; North, C.S. Mental health and the Covid-19 pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Daniel, J. Education and the COVID-19 pandemic. Prospects 2020, 49, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.; Hwang, E. Effects of academic resilience and interpersonal competence on the happiness of nursing students. Korean Med. Educ. Rev. 2018, 20, 156–163. [Google Scholar]
- Korea Centers for Disease Control and Prevention. COVID-19 Mortality Rate in S. Korea. Available online: http://ncov.mohw.go.kr/en/ (accessed on 16 July 2021).
- Park, J.H.; Chang, S.J.; Kim, K.S. Correlation between the preventive behaviors on Middle East respiratory syndrome and the knowledge, attitude, and compliance of medically inclined college students. J. Dent. Hyg. Sci. 2017, 17, 341–351. [Google Scholar] [CrossRef] [Green Version]
- Aslan, H.; Pekince, H. Nursing students’ views on the COVID-19 pandemic and their percieved stress levels. Perspect. Psychiatr. Care 2020, 57, 695–701. [Google Scholar] [CrossRef]
- Rafati, F.; Nouhi, E.; Sabzevari, S.; Dehghan-Nayeri, N. Coping strategies of nursing students for dealing with stress in clinical setting: A qualitative study. Electron. Physician 2017, 9, 6120–6128. [Google Scholar] [CrossRef] [Green Version]
- Wong, J.G.; Cheung, E.P.; Cheung, V.; Cheung, C.; Chan, M.T.; Chua, S.E.; McAlonan, G.M.; Tsang, K.W.; Ip, M.S. Psychological responses to the SARS outbreak in healthcare students in Hong Kong. Med. Teach. 2004, 26, 657–659. [Google Scholar] [CrossRef]
- Oh, N.; Hong, N.; Ryu, D.H.; Bae, S.G.; Kam, S.; Kim, K.-Y. Exploring nursing intention, stress, and professionalism in response to infectious disease emergencies: The experience of local public hospital nurses during the 2015 MERS outbreak in South Korea. Asian Nurs. Res. 2017, 11, 230–236. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health and Welfare. Cases in Korea. Available online: http://ncov.mohw.go.kr/bdBoardList_Real.do?brdId=1&brdGubun=11&ncvContSeq=&contSeq=&board_id=&gubun= (accessed on 26 May 2021).
- Watts, S.; Stenner, P. Theory and Q Methodology: From Stephenson to Constructionism. In Doing Q Methodological Research: Theory, Method and Interpretatio; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Kim, H.K. Q methodology: Philosophy, theories, analysis, and application. Seoul Commun. Books 2008, 78–191. [Google Scholar]
- Watts, S.; Stenner, P. Doing Q methodology: Theory, method and interpretation. Qual. Res. Psychol. 2005, 2, 67–91. [Google Scholar] [CrossRef]
- Han, S. Emotional response of civil servants to new public management reform: An application of Q-methodology. Korea Inst. Public Aff. Seoul Natl. Univ. 2010, 48, 25–57. [Google Scholar]
- Sim, J. Triangulation in Public Analysis and Evaluation: Combining Quantitative and Qualitative Methods. Korean J. Policy Anal. Eval. 2019, 29, 143–166. [Google Scholar]
- Kim, J.; Ju, K.; Oh, H.; Yoon, C. Ageism and Types of Subjective Perception of Elderly Persons on the Experience with Healthcare Professionals and Services: Using the Q-Methodology. Korean J. Sociol. 2019, 53, 1–44. [Google Scholar] [CrossRef]
- Min, K.; Kim, J.; Hwang, S.; Jahng, S. Vaiations in Emotion Response Patterning across Genders, Generations, and Personality Types. Korean J. Soc. Personal. Psy. 1998, 12, 119–140. [Google Scholar]
- Ricci, D.M. A Phenomenological Study of the Experience of Learning in Adult Higher Education. Ph.D. Thesis, The University of Wisconsin-Madison, Madison, WI, USA, 2000. [Google Scholar]
- Yin, Q.; Liu, Y.; Chen, A.; Song, X.; Cai, W.; Deng, G.; Dong, W. Risk Perception and Emotion Reaction of Chinese Health Care Workers Varied During COVID-19: A Repeated Cross-Sectional Research. Int. J. Public Health 2021, 66, 15. [Google Scholar]
- Xu, J.; Peng, Z. People at risk of influenza pandemics: The evolution of perception and behavior. PLoS ONE 2015, 10, e0144868. [Google Scholar] [CrossRef] [PubMed]
- Chiaravalloti, N.D.; Amato, M.P.; Brichetto, G.; Chataway, J.; Dalgas, U.; DeLuca, J.; Meza, C.; Moore, N.B.; Feys, P.; Filippi, M. The emotional impact of the COVID-19 pandemic on individuals with progressive multiple sclerosis. J. Neurol. 2021, 268, 1598–1607. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [Green Version]
- De Vroege, L.; Van Den Broek, A. Results of mental support for health care professionals and mental care during the COVID-19 pandemic. J. Public Health 2021. [Google Scholar] [CrossRef] [PubMed]
- Kim, S. Effects of stigma on self-esteem among individuals with mental illness. Ment. Health Soc. Work 2014, 42, 91–120. [Google Scholar]
- Lee, G.C.; Ahn, J. College Nursing Students’ Experiences of COVID-19 Pandemic. J. Korea Acad.-Ind. Coop. Soc. 2020, 21, 142–152. [Google Scholar]
- Kim, O.S.; Oh, J.H. The convergence study on anxiety, knowledge, infection possibility, preventive possibility and preventive behavior level of MERS in nursing students. J. Korea Converg. Soc. 2016, 7, 59–69. [Google Scholar] [CrossRef] [Green Version]
- Patelarou, A.; Mechili, E.A.; Galanis, P.; Zografakis-Sfakianakis, M.; Konstantinidis, T.; Saliaj, A.; Bucaj, J.; Alushi, E.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I. Nursing students, mental health status during COVID-19 quarantine: Evidence from three European countries. J. Ment. Health 2021, 30, 164–169. [Google Scholar] [CrossRef]
- Reverté-Villarroya, S.; Ortega, L.; Lavedán, A.; Masot, O.; Burjalés-Martí, M.D.; Ballester-Ferrando, D.; Fuentes-Pumarola, C.; Botigué, T. The influence of COVID-19 on the mental health of final-year nursing students: Comparing the situation before and during the pandemic. Int. J. Ment. Health Nurs. 2021, 30, 694–702. [Google Scholar] [CrossRef]
- Vaillant, G.E. Natural history of male psychological health: V. The relation of choice of ego mechanisms of defense to adult adjustment. Arch. Gen. Psychiatry 1976, 33, 535–545. [Google Scholar] [CrossRef]
- Yoon, S.; Ahn, G.; Park, Y. The defense mechanism and coping strategy characteristics of resiliently adaptive female college student. Korean J. Health Psychol. 2008, 13, 961–975. [Google Scholar] [CrossRef]
- Yang, J.; Lee, Y. Pandemic Experience of Infectious Diseases of Nursing Students: Targeting non-confirmed COVID-19. J. Ind. Converg. 2020, 18, 85–98. [Google Scholar]
- Lee, D.; Kim, J.; Kang, H. The emotional distress and fear of contagion related to Middle East Respiratory Syndrome (MERS) on general public in Korea. Korean J. Psychol. Gen. 2016, 35, 355–383. [Google Scholar] [CrossRef]
- Im, S.; Choi, E.-H.; Lee, M.; Hong, N.Y.; Hwang, D.Y.; Choi, Y.B. Adjustment Experiences of Nursing Students in the Face of COVID-19. J. Korean Soc. Sch. Health 2020, 33, 213–221. [Google Scholar]
- Son, S.; Suh, K.H. Relationships between gratitude disposition and psychological well-being: Focus on the mediating effects of interpersonal competence. Korean J. Health Psychol. 2014, 19, 619–663. [Google Scholar]
- Mun, M.; Hwang, S. Impact of Character strengths on major satisfaction and nursing professionalism in nursing students. J. Learn. Cent. Curric. Instr. 2016, 16, 403–418. [Google Scholar]
- Keeling, J.; Templeman, J. An exploratory study: Student nurses’ perceptions of professionalism. Nurse Educ. Pract. 2013, 13, 18–22. [Google Scholar] [CrossRef]
- Lee, N.; Lee, H.-J. South Korean Nurses’ Experiences with Patient Care at a COVID-19-Designated Hospital: Growth after the Frontline Battle against an Infectious Disease Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9015. [Google Scholar] [CrossRef]
- Ji, E.; Lee, H. Type of Perception toward Change of 4th Industrial Revolution and Nursing Education in Nursing Students: Q Methodological Approach. J. Korean Soc. Wellness 2020, 15, 135–148. [Google Scholar] [CrossRef]
- Kang, J.; Bak, A.; Han, S. A Phenomenological Study of the Lifestyle Change Experiences of Undergraduate Due to COVID-19. J. Korean Entertain. Ind. Assoc. 2020, 14, 289–297. [Google Scholar] [CrossRef]
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Type | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Eigenvalues | 10.21 | 4.47 | 2.26 | 1.81 |
| Variance (%) | 8 | 12 | 13 | 6 |
| Cumulative (%) | 8 | 20 | 33 | 39 |
| Type (n) | ID | Gender | Age (Year) | Grade | Personality | Reason for Choosing a Department | Satisfaction with Major Selection | Factor Weight |
|---|---|---|---|---|---|---|---|---|
| 1 (n = 6) | 3 | F | 19 | 2 | Extrovert | Ease of employment | Good | 0.56 |
| 4 | F | 20 | 2 | Mixed | Voluntary | Ordinary | 0.60 * | |
| 13 | M | 21 | 2 | Mixed | Ease of employment | Good | 0.43 | |
| 24 | F | 30 | 3 | Mixed | Voluntary | Ordinary | 0.47 | |
| 33 | F | 18 | 1 | Mixed | Recommendations of others | Ordinary | 0.43 | |
| 46 | F | 20 | 3 | Mixed | Meet college admission scores | Ordinary | 0.52 | |
| 2 (n = 15) | 1 | F | 19 | 2 | Mixed | Ease of employment | Good | 0.68 * |
| 9 | M | 24 | 2 | Introvert | Ease of employment | Ordinary | 0.35 | |
| 15 | F | 20 | 2 | Mixed | Voluntary | Ordinary | 0.58 | |
| 17 | F | 19 | 2 | Mixed | Voluntary | Good | 0.61 | |
| 18 | F | 19 | 2 | Mixed | Ease of employment | Good | 0.60 | |
| 19 | F | 19 | 2 | Extrovert | Ease of employment | Good | 0.60 | |
| 21 | F | 20 | 3 | Mixed | Ease of employment | Ordinary | 0.54 | |
| 22 | F | 20 | 3 | Mixed | Voluntary | Good | 0.34 | |
| 26 | M | 25 | 2 | Mixed | Recommendations of others | Ordinary | 0.45 | |
| 28 | F | 19 | 2 | Introvert | Voluntary | Good | 0.57 | |
| 30 | F | 18 | 1 | Extrovert | Voluntary | Good | 0.52 | |
| 37 | F | 18 | 1 | Extrovert | Voluntary | Ordinary | 0.57 | |
| 38 | F | 18 | 1 | Mixed | Voluntary | Good | 0.45 | |
| 42 | F | 20 | 3 | Introvert | Voluntary | Good | 0.57 | |
| 45 | F | 21 | 3 | Introvert | Voluntary | Ordinary | 0.60 | |
| 3 (n = 12) | 5 | M | 21 | 2 | Introvert | Voluntary | Ordinary | 0.40 |
| 6 | F | 19 | 2 | Extrovert | Voluntary | Good | 0.42 | |
| 8 | M | 20 | 2 | Introvert | Voluntary | Ordinary | 0.65 * | |
| 11 | M | 22 | 2 | Mixed | Ease of employment | Ordinary | 0.38 | |
| 23 | M | 21 | 2 | Extrovert | Voluntary | Good | 0.66 | |
| 25 | F | 30 | 3 | Mixed | Ease of employment | Ordinary | −0.58 | |
| 32 | F | 18 | 1 | Mixed | Ease of employment | Good | 0.63 | |
| 34 | F | 18 | 1 | Extrovert | Voluntary | Ordinary | 0.60 | |
| 36 | F | 19 | 1 | Introvert | Voluntary | Good | 0.53 | |
| 43 | F | 20 | 3 | Introvert | Voluntary | Ordinary | 0.56 | |
| 44 | M | 23 | 3 | Extrovert | Recommendations of others | Ordinary | 0.55 | |
| 47 | F | 20 | 3 | Extrovert | Voluntary | Good | 0.49 | |
| 4 (n = 5) | 10 | M | 22 | 2 | Introvert | Voluntary | Good | 0.46 |
| 14 | M | 23 | 2 | Mixed | Voluntary | Ordinary | −0.35 | |
| 31 | F | 19 | 1 | Mixed | Voluntary | Good | 0.55 | |
| 39 | F | 22 | 4 | Introvert | Voluntary | Ordinary | 0.60 * | |
| 40 | F | 20 | 3 | Mixed | Voluntary | Ordinary | 0.38 |
| No. | Q-Statement | Z−Scores | |||
|---|---|---|---|---|---|
| Type 1 (n = 6) | Type 2 (n = 15) | Type 3 (n = 12) | Type 4 (n = 5) | ||
| 1 | I am suspicious that the people I come into contact with may be infected. | 0.62 | 0.62 | −1.05 | −1.47 |
| 2 | I am afraid that I may spread the infection to others and be stigmatized as a spreader of an infectious disease. | 1.56 | −0.05 | −1.02 | 0.30 |
| 3 | I hope the pandemic will end before I become a nurse. | 1.75 | 1.85 | 1.10 | −0.22 |
| 4 | Everyday places have changed into places of fear. | −1.11 | −0.44 | −0.88 | 0.18 |
| 5 | Experiencing the pandemic made me afraid of becoming a nurse. | −0.68 | −0.52 | −1.21 | −0.66 |
| 6 | I am concerned that the quality of nursing education will decrease due to the pandemic. | −0.41 | −0.71 | −1.22 | −1.40 |
| 7 | I am depressed that my activities are being restricted due to the pandemic. | −0.45 | 1.44 | −0.14 | −0.86 |
| 8 | I am afraid that I may become infected at school or clinical training sites. | −0.58 | −0.09 | −0.91 | 0.42 |
| 9 | I think I am becoming weary and numb as the pandemic continues. | −0.74 | 0.94 | −0.60 | −0.52 |
| 10 | I experienced physical symptoms due to the pandemic, such as loss of appetite and indigestion. | −2.36 | −2.32 | −1.73 | −0.60 |
| 11 | I am nervous about whether I will be able to cope well with the pandemic after I become a nurse. | −0.85 | 0.47 | −0.17 | −0.16 |
| 12 | I am depressed because I do not know when the pandemic will end. | −0.47 | 0.76 | −0.11 | 0.67 |
| 13 | I feel stifled because my freedom is being suppressed. | −1.02 | 1.30 | −1.01 | 0.34 |
| 14 | As a nursing student, it infuriates me to see people behaving irresponsibly. | −1.16 | 0.58 | 0.44 | −1.30 |
| 15 | I am dissatisfied with the unilateral government and educational policies. | −0.69 | −0.50 | −0.19 | −0.35 |
| 16 | I regret enrolling in the nursing program. | 0.01 | −1.91 | −1.95 | −1.95 |
| 17 | I am worried about being unprepared as a nursing student. | 0.64 | 1.56 | −0.10 | 0.02 |
| 18 | I am afraid that I may not be able to become a nurse or get employed. | −1.09 | −0.73 | −1.68 | 0.70 |
| 19 | My expectations of college life were shattered. | −1.33 | 0.25 | 0.45 | −1.72 |
| 20 | I am confused about whether I am doing well. | −0.75 | 1.10 | 0.48 | 0.96 |
| 21 | I should be concerned with the pandemic as it will be a relevant issue for me as a nurse. | 1.34 | 1.14 | 0.94 | 0.98 |
| 22 | Even in a pandemic, I must do what I want to do. | 0.80 | −0.57 | −0.71 | −1.19 |
| 23 | We will be able to experience personal growth by overcoming the pandemic. | 0.83 | 0.57 | 0.71 | 1.42 |
| 24 | As a nursing student, I actively educate those around me about the importance of infection control. | 0.83 | −0.74 | 0.38 | 0.41 |
| 25 | I wish that infectious disease and disaster management courses were included in the nursing education curriculum. | 0.83 | 0.20 | 0.19 | 0.71 |
| 26 | I feel proud to be a nursing student when I see hard-working nurses. | 1.53 | 1.23 | 1.40 | 0.70 |
| 27 | The pandemic made me realize that I must study harder to become a competent nurse. | 1.26 | 1.11 | 0.60 | 0.67 |
| 28 | Due to the pandemic, I had more time to focus on myself and think about the future. | −0.47 | −1.30 | 0.54 | −0.03 |
| 29 | I feel a sense of accomplishment in completing this stage of education despite difficult circumstances. | 0.49 | −1.00 | 0.77 | 0.02 |
| 30 | It allowed me to think about the nurses’ sense of duty. | 1.36 | 0.31 | 0.59 | 1.38 |
| 31 | By pursuing nursing education, I realized the importance of infection control, and it became a way of life. | 0.55 | −0.12 | 0.99 | 1.10 |
| 32 | As a nursing student, I feel that I should approach information objectively. | 1.06 | −0.56 | −0.14 | −0.48 |
| 33 | I look forward to becoming a nurse and participating in social activities as a professional. | 0.18 | −0.41 | 2.48 | 1.14 |
| 34 | It feels nice to have unexpected spare time. | −0.20 | −1.16 | 1.24 | −2.28 |
| 35 | I think the current pandemic is a learning ground that will help us cope with future crises. | 0.34 | −1.02 | 0.91 | 1.16 |
| 36 | It was nice to spend more time with my family due to the pandemic. | −1.09 | −0.92 | 1.02 | 0.63 |
| 37 | I think my competence as a professional nurse will increase as a result of experiencing new methods of teaching and learning. | −0.54 | −0.37 | −0.42 | 1.26 |
| Type | No. | Q Statements | Z-Score | Average | Difference |
|---|---|---|---|---|---|
| 1 | 2 | I am afraid that I may spread the infection to others and be stigmatized as a spreader of an infectious disease. | 1.56 | 0.20 | 1.36 |
| 32 | As a nursing student, I feel that I should approach information objectively. | 1.06 | −0.03 | 1.09 | |
| 22 | Even in a pandemic, I must do what I want to do. | 0.80 | −0.42 | 1.22 | |
| 16 | I regret enrolling in the nursing program. | 0.01 | −1.45 | 1.46 | |
| 20 | I am confused about whether I am doing well. | −0.75 | 0.45 | 1.20 | |
| 2 | 17 | I am worried about being unprepared as a nursing student. | 1.56 | 0.53 | 1.03 |
| 7 | I am depressed that my activities are being restricted due to the pandemic. | 1.44 | 0.00 | 1.44 | |
| 13 | I feel stifled because my freedom is being suppressed. | 1.30 | −0.10 | 1.40 | |
| 9 | I think I am becoming weary and numb as the pandemic continues. | 0.94 | −0.23 | 1.17 | |
| 31 | By pursuing nursing education, I realized the importance of infection control, and it became a way of life. | −0.12 | 0.63 | 0.75 | |
| 24 | As a nursing student, I actively educate those around me about the importance of infection control. | −0.74 | 0.22 | 0.96 | |
| 29 | I feel a sense of accomplishment for completing this stage of education despite difficult circumstances. | −1.00 | 0.07 | 1.07 | |
| 35 | I think the current pandemic is a learning ground that will help us cope with future crises. | −1.02 | 0.35 | 1.37 | |
| 34 | It feels nice to have unexpected spare time. | −1.16 | −0.60 | 0.56 | |
| 28 | Due to the pandemic, I had more time to focus on myself and think about the future. | −1.30 | −0.32 | 0.98 | |
| 3 | 33 | I look forward to becoming a nurse and participating in social activities as a professional. | 2.48 | 0.85 | 1.63 |
| 34 | It feels nice to have unexpected spare time. | 1.24 | −0.60 | 1.84 | |
| 2 | I am afraid that I may become a spreader of an infectious disease and be stigmatized as one. | −1.02 | 0.20 | 1.22 | |
| 4 | 37 | I think my competence as a professional nurse will increase as a result of experiencing new methods of teaching and learning. | 1.26 | −0.02 | 1.28 |
| 3 | I hope the pandemic will end before I become a nurse. | −0.22 | 1.12 | 1.34 | |
| 10 | I experienced physical symptoms due to the pandemic, such as loss of appetite and indigestion. | −0.60 | −1.75 | 1.15 | |
| 34 | It feels nice to have unexpected spare time. | −2.28 | −0.60 | 1.68 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seong, M. Korean Nursing Students’ Emotional Response Types to Pandemic: Application of Q-Methodology. Healthcare 2021, 9, 1080. https://doi.org/10.3390/healthcare9081080
Seong M. Korean Nursing Students’ Emotional Response Types to Pandemic: Application of Q-Methodology. Healthcare. 2021; 9(8):1080. https://doi.org/10.3390/healthcare9081080
Chicago/Turabian StyleSeong, Mihyeon. 2021. "Korean Nursing Students’ Emotional Response Types to Pandemic: Application of Q-Methodology" Healthcare 9, no. 8: 1080. https://doi.org/10.3390/healthcare9081080
APA StyleSeong, M. (2021). Korean Nursing Students’ Emotional Response Types to Pandemic: Application of Q-Methodology. Healthcare, 9(8), 1080. https://doi.org/10.3390/healthcare9081080