
A Survey of Attitudes and Beliefs about Care, Compassion and Communities Networks in Palliative Care. A Preliminary Study for the Development of a Compassionate University

Abstract
:1. Introduction
- Identifying the level of knowledge and sensitivities that professionals and students have regarding the care and attention of people at the end of life.
- Detecting the training needs—according main topics included in the curricular proposals for the training of doctors, nurses and psychologists in Palliative Care-, within the university teaching programs related to the care of people with advanced disease and/or at the end of life.
- Identifying the abilities of professionals and students to perceive values related to compassion and express it in their life environment.
2. Materials and Methods
2.1. Study Design and Population
2.2. Variables and Measures
- Block 1. Sociodemographic and academic characterization: sex, age, household structure, academic relationship with the University.
- Block 2. Level of knowledge and sensitivities of the population about care of people at the end of life.
- Block 3. Training needs of students related to care of people with advanced disease and/or at the end of life. The competencies were classified according to the European Association for Palliative Care (EAPC) curriculum [6] on PC in Universities.
- Block 4. Assessment of Compassion in students and professionals on self-compassion, compassion for others and compassion from others. The validated Gilbert´s scale was used [9].
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Sociodemographic and Academic Characterization of the Study Population
3.2. Level of Knowledge and Sensitivities of the Population about Care of People at the End of Life
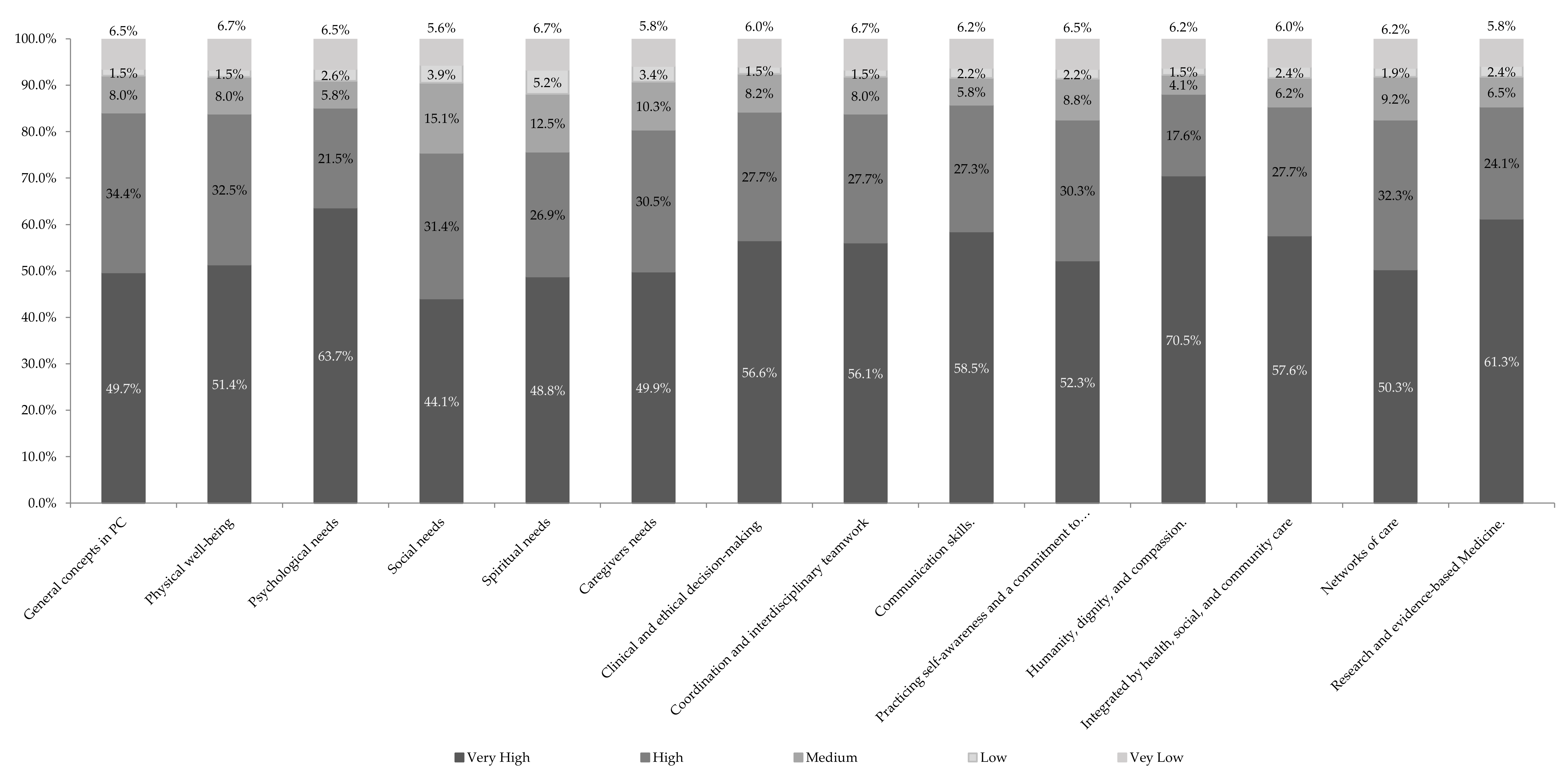
3.3. Students Training Needs Related to Caring of People with Advanced Disease and/or at the End of Life
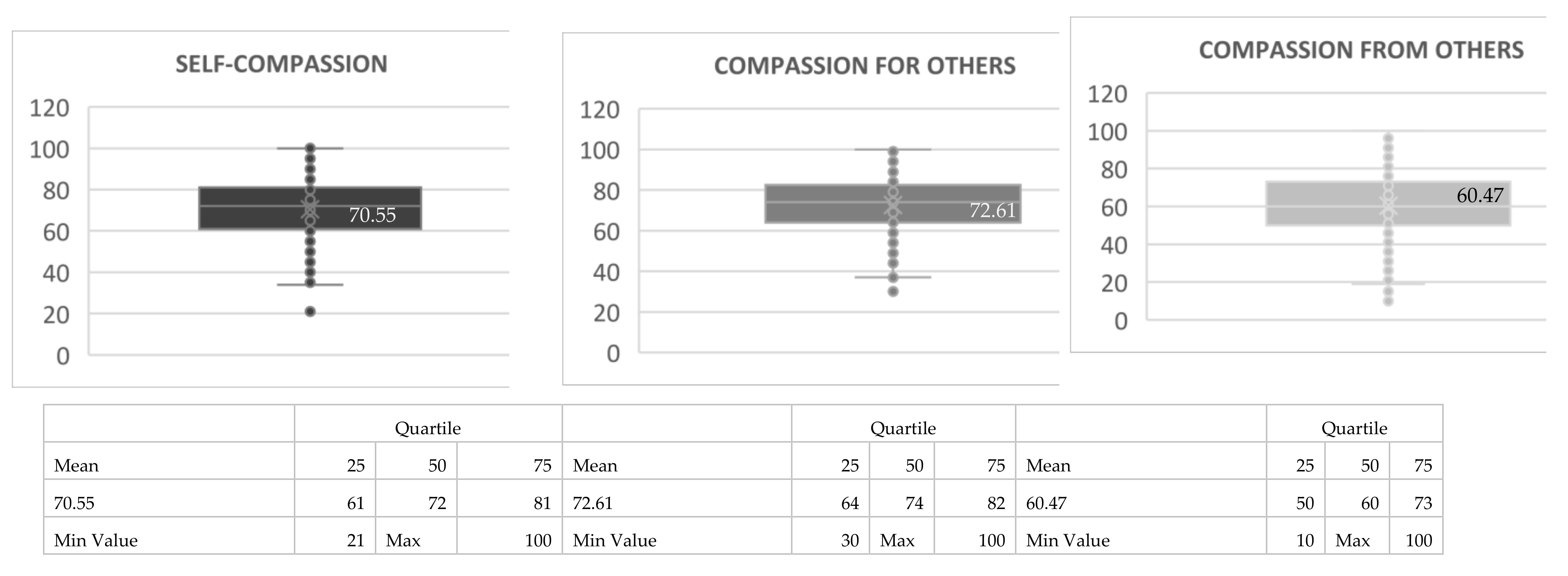
3.4. Self-Compassion, Compassion for Others, Compassion from Others; Gilbert’s Scale
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Block, S.; Billings, J.A. Nurturing humanism through teaching palliative care. Acad. Med. 1998, 73, 763–765. [Google Scholar] [CrossRef] [PubMed]
- Brito, G.; Librada, S. Compassion in palliative care: A review. Curr. Opin. Support. Palliat Care 2018, 12, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Lown, B.; McIntosh, S.; Gaines, M.; McGuinn, K.; Hatem, D.S. Integrating Compassionate, Collaborative Care (the “Triple C”) into health professional eductaion to advance the triple aim of heath care. Acad. Med. 2016, 91, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Abel, J.; Bowra, J.; Walter, T.; Howarth, G. Compassionate community networks: Supporting home dying. BMJ Support. Palliat. Care 2011, 1, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Vindrola-Padros, C.; Mertnoff, R.; Lasmaría, C.; Gomez-Batiste, X. Palliative care education in Latin America: A systematic review of training programs for heathcare professionals. Palliat. Support. Care 2018, 16, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Recommendations of the European Association for Palliative Care (EAPC) for the Development of Undergraduate Curricula in Palliative Medicine to the European Medical Schools; Report of the EAPC Steering Group on Medical Education and Training in Palliative Care. EAPC, 2013. Available online: https://dadun.unav.edu/bitstream/10171/34516/1/Recommendations%20of%20the%20EAPC%20for%20the%20Development%20of%20Undergraduate%20Curricula%20in%20Palliative%20Medicine%20At%20European%20Medical%20Schools.pdf (accessed on 26 July 2021).
- Davalos-Batallas, V.; Vargas-Martínez, A.-M.; Bonilla-Sierra, P.; Leon-Larios, F.; Lomas-Campos, M.-d.-l.-M.; Vaca-Gallegos, S.-L.; de Diego-Cordero, R. Compassionate Engagement and Action in the Education for Health Care Professions: A Cross-Sectional Study at an Ecuadorian University. Int. J. Environ. Res. Public Health 2020, 17, 5425. [Google Scholar] [CrossRef] [PubMed]
- Librada, S.; Herrera, E.; Boceta, J.; Vargas, R.M.; Vicuna, M. All with You: A new method for developing compassionate communities and cities at the end of life. Experiences in Spain and Latin-America. Ann. Palliat. Med. 2018, 7, S15–S31. [Google Scholar]
- Gilbert, P.; Catarino, F.; Duarte, C.; Matos, M.; Kolts, R.; Stubbs, J.; Ceresatto, L.; Duarte, J.; Pinto-Gouveia, J.; Basran, J. The development of compassionate engagement and action scales for self and others. J. Compassionate Health Care 2017, 4, 4. [Google Scholar] [CrossRef] [Green Version]
- Colombia. Ministry of Health. Resolution 8430 of 1993. By which the scientific, technical and administrative standards for health research are established. 1993. Available online: https://www.urosario.edu.co/Escuela-Medicina/Investigacion/Documentos-de-interes/Files/resolucion_008430_1993.pdf (accessed on 26 July 2021).
- Statutory Law 1581 of 2012, on the General Regime for the Protection of Personal Data: Article 6.e and article 10.d. Available online: http://www.fundacionmicrofinanzasbbva.org/revistaprogreso/en/international-collection-of-personal-data/ (accessed on 26 July 2021).
- Lown, B.A.; Rosen, J.; Marttila, J. An Agenda for Improving Compassionate Care: A Survey Shows About Half of Patients Say Such Care Is Missing. Health Aff. 2011, 30, 1772–1778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinclair, S.; Beamer, K.; Hack, T.F.; McClement, S.; Bouchal, S.R.; Chochinov, H.M.; Hagen, N.A. Sympathy, empathy, and compassion: A grounded theory study of palliative care patients’ understandings, experiences, and preferences. Palliat. Med. 2017, 31, 437–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pastrana, T.; De Lima, L.; Pons, J.J.; Centeno, C. Atlas de Cuidados Paliativos de Latinoamérica; Edición Cartográfica; IAHPC Press: Houston, TX, USA, 2013. [Google Scholar]
- Hui, D.; Nooruddin, Z.; Didwaniya, N.; Dev, R.; De La Cruz, M.; Kim, S.H.; Kwon, J.H.; Hutchins, R.; Liem, C.; Bruera, E. Concepts and definitions for “actively dying”, “end of life”, “terminally ill,“ Terminal care ”, and“ transition of care ”: A systematic review. J. Pain Symptom Manag. 2014, 47, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Fraser, H.C.; Kutner, J.S.; Pfeifer, M.P. Senior Medical Students’ Perceptions of the Adequacy of Education on End-of-Life Issues. J. Palliat. Med. 2001, 4, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Díaz, F.; Redondo, M.J.; Librada, S. Networks of Care at the End of Life people in a palliative care population. In Proceedings of the XI Congress of the Spanish Palliative Care Society, SECPAL, Seville, Spain, 12–14 May 2016. [Google Scholar]
- Librada Flores, S.; Herrera Molina, E.; Díaz Díez, F.; Redondo Moralo, M.J.; Castillo Rodríguez, C.; McLoughlin, K.; Abel, J.; Jadad Garcia, T.; Lucas Díaz, M.Á.; Trabado Lara, I.; et al. REDCUIDA Development and Management of Networks of Care at the End of Life (the REDCUIDA Intervention): Protocol for a Nonrandomized Controlled Trial. JMIR Res. Protoc. 2018, 7, e10515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Librada, S.; Castillo, C.; Trabado, I.; Lucas, M.A. REDCUIDA protocol: Development and Management of Networks of Care at the End of Life. Preliminary results. In Proceedings of the XII Congress of the Spanish Palliative Care Society, Vitoria, Spain, 7–9 June 2018. [Google Scholar]
- Pérez-de la Cruz, S.; García-Luengo, M.V. Comparative study among Spanish students of heatlh sciences degrees: Facing death. Nurs. Health Sci. 2018, 20, 380–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miles, L.; Corr, C.A. Death Cafe. Omega 2017, 75, 151–165. [Google Scholar] [CrossRef] [PubMed]
- Billings, M.; Engelberg, R.; Randall, C.; Block, S.; Sullivan, A.M. Determinants of medical students´perceived preparation to perform end of life care, quality of end of life care education, and attitudes toward end of life care. J. Palliat. Med. 2010, 13, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Borgstrom, E.; Morris, R.; Wood, D.; Cohn, S.; Barclay, S. Learning to care: Medical students’ reported value and evaluation of palliative care teaching involving meeting patients and reflective writing. BMC Med. Educ. 2016, 16, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centeno, C.; Ballesteros, M.; Carrasco, J.M.; Arantzamendi, M. Does palliative care education matter to medical students? The experience of attending an undergraduate course in palliative care. BMJ Support. Palliat. Care 2014, 6, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, S.; Kelly, B.; Powis, D.; Smyth, R.; Lewin, T. The desirable qualities of future doctors—A study of medical student perceptions. Med. Teach. 2013, 35, e1332–e1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | Total Sample N: 465 | % | |||||
| Sociodemographic characterization | |||||||
| Sex | |||||||
| Male | 121 | 26% | |||||
| Female | 344 | 74% | |||||
| Age group | |||||||
| • 18–39 years | 412 | 88.6% | |||||
| • 40–59 years | 49 | 10.5% | |||||
| • Over 60 years | 4 | 0.9% | |||||
| Mean age | 24 | ||||||
| Standard deviation | 10,003 | ||||||
| Household structure | |||||||
| Couple without children | 347 | 74.6% | |||||
| Married with children | 29 | 6.2% | |||||
| Single with children | 25 | 5.4% | |||||
| Cohabitant without children | 22 | 4.7% | |||||
| Cohabitant with children | 17 | 3.7% | |||||
| Married without children | 14 | 3% | |||||
| Separated with children | 6 | 1.3% | |||||
| Separated without children | 5 | 1.1% | |||||
| Students | |||||||
| Students n = 383 (82.4%) | Total students (%) | (Semester 1/2) | (Semester 3/4) | (Semester 5/6) | (Semester 7/8) | (Semester 9/10) | (Semester 11/12) |
| Medicine Students | 128 (33.4%) | 69 (53.8%) | 24 (18.5%) | 10 (7.6%) | 8 (5.9%) | 9 (6.7%) | 10 (7.6%) |
| Psychology Students | 77 (20.2%) | 51 (65.8%) | 10 (13.2%) | 9 (11.8%) | 7 (9.2%) | 0 (0.0%) | 0 (0.0%) |
| Nursing Students | 167 (43.6%) | 62 (37.1%) | 27 (16.2%) | 58 (34.7%) | 20 (12.0%) | 0 (0.0%) | 0 (0.0%) |
| No specification | 11 (2.8%) | ||||||
| Total | 383 (100%) | 181 (48.8%) | 61 (16.3%) | 77 (20.6%) | 35 (9.3%) | 9 (2.3%) | 10 (2.6%) |
| Teachers | Total Sample | % | |||||
| Professor of the University of Nursing | 16 | 26.2% | |||||
| Professor at the University of Psychology | 15 | 24.6% | |||||
| Professor at the University of Medicine | 21 | 23.0% | |||||
| No job specification | 9 | 14.8% | |||||
| Total Teachers | n = 61 | 13.1% | |||||
| Other professionals at the University | |||||||
| Academic directors | 7 | 33.3% | |||||
| Operational area | 5 | 23.9% | |||||
| Academic support executive and authority area | 4 | 19.0% | |||||
| Administration area | 3 | 14.3% | |||||
| No job specification | 2 | 9.5% | |||||
| Total Other University professionals | n = 21 | 4.5% | |||||
| Knowledge and Sensitivities towards Palliative Care | YES | NO | ||||||||||
| Medicine | Psychology | Nursing | Teachers | Other Professionals | Total | Medicine | Psychology | Nursing | Teachers | Other Professionals | Total | |
| Do you know what palliative care is? (n: 445) | 110 30.3% | 50 13.8% | 139 38.3% | 46 12.7% | 18 5.0% | 363 * 81.6% | 18 4.8% | 27 7.1% | 28 7.4% | 6 1.6% | 3 0.8% | 82 ** 18.4% |
| Who Do You Consider They are Aimed at (n: 442) | Medicine | Psychology | Nursing | Teachers | Other Professionals | Total | ||||||
| - To the entire population (adult and pediatric population) with advanced disease and/or at the end of life | 110 24.9% | 62 14.0% | 150 33.9% | 47 10.6% | 15 3.4% | 384 86.9% | ||||||
| - Only to the adult population with advanced disease and/or at the end of life | 17 3.8% | 13 2.9% | 16 3.6% | 4 0.9% | 2 0.5% | 52 11.8% | ||||||
| - Only to the pediatric population with advanced disease and/or at the end of life | 1 0.2% | 2 0.5% | 1 0.2% | 1 0.2% | 1 0.2% | 6 1.4% | ||||||
| Concepts Associated with Palliative Care (n = 1115 Multiple Responses) | ||||||||||||
| If you know palliative care (n = 950) | Does not know palliative care (n = 165) | |||||||||||
| - Death | 105 (11.1%) | 22 (13.3%) | ||||||||||
| - State of agony and end of life | 164 (17.3%) | 37 (22.4%) | ||||||||||
| - Decrease in suffering | 276 (29.1%) | 41 (24.8%) | ||||||||||
| - Quality of life | 263 (27.7%) | 38 (23%) | ||||||||||
| - The privilege of caring and being cared for | 138 (14.5%) | 26 (15.8%) | ||||||||||
| - Other concepts | 4 (0.4%) | 1 (0.6) | ||||||||||
| Experiences of Contact with People in Palliative Care | ||||||||||||
| Temporality | Yes = 339 (72.9%) | No = 126 (27.1%) | ||||||||||
| Nowadays | In the last month | In the last year | More than 1 year ago | |||||||||
| 41 (12.1%) | 27 (8.0%) | 97 (28.6%) | 174 (51.3%) | |||||||||
| Relationship | Patient | Grandparent | Uncle | Father mother | Friend | Work partner | Sibling | Spouse/Partner | Other | |||
| 95 (28.9%) | 92 (28.0%) | 52 (15.8%) | 30 (9.1%) | 25 (7.6%) | 7 (2.1%) | 4 (1.2%) | 2 (0.6%) | 22 (6.7%) | ||||
| Received Palliative Care | ||||||||||||
| Usefulness of CP | Yes = 255 (77.3%) | No = 75 (22.7%) | ||||||||||
| Yes and I only considered it useful for the person who was going through this disease process | Yes, and I considered them useful both for the person with the disease, as well as for their family and their entire care network. | Yes and I considered them useful, but only for the family and their care network. | Do not consider them useful | |||||||||
| 36 (145.9%) | 191 (79.3%) | 4 (1.7%) | 10 (4.1) | |||||||||
| Experiences of Caring for Someone at the End of Life | ||||||||||||
| Have cared for a person at the end of life | Yes = 164 (35.3%) | No = 301 (64.7%) | ||||||||||
| Hours of dedication to care Mean of 7 h of dedication | <6 h | 6–11 h | 12–17 h | 18–23 h | 24 h | |||||||
| 41 (51.7%) | 27 (23.1%) | (18.2%) | 97 (1.4%) | (5.6%) | ||||||||
| People involved in care Mean of 8 people involved | <5 people | 5–9 people | 10–14 people | 15–19 people | > 20 people | |||||||
| 55 (41.4%) | 52 (39.1%) | 10 (7.5%) | 5 (3.8%) | 11 (8.3) | ||||||||
| Willingness and Ability to Care | ||||||||||||
| Willingness to take care of a person other than the closest family or circle of friends | Si = 424 (91.2%) | No = 41 (8.8%) | ||||||||||
| You feel able to care for a person with advanced disease | Yes = 236 (50.8%) | No: 229 (49.2%) | ||||||||||
| Care Network (n = 465) | Less Than 5 People | Between 5 and 9 People | Between 10 and 14 People | Between 15 and 19 People | Between 20 and 24 People | More Than 25 People | ||||||
| 313 (67.5%) | 114 (24.6%) | 28 (6.0%) | 2 (0.4%) | 6 (1.3%) | 2 (0.2%) | |||||||
| Talk about death (n = 465) | Yes, Since I Have No Problem and I Talk About it When I Want | Yes, But When It Happens to Me Closely | Sometimes, but with People from my Environment and Professional Profile | Seldom | Never | |||||||
| 208 (44.7%) | 31 (6.7%) | 97 (20.9%) | 114 (24.5%) | 15 (3.2%) | ||||||||
| Training Received in PC | Interest in PC Themes | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medicine n = 119 | Psychology n = 76 | Nursing n = 167 | Academics n = 61 | Total Students n = 383 | ||||||||
| YES | NO | YES | NO | YES | NO | High | Medium | Low | High | Medium | Low | |
| General concepts | 69 (58.0%) | 50 (42.0%) | 36 (47.4%) | 40 (52.6%) | 116 (69.5%) | 51 (30.5%) | 70.5% | 27.9% | 1.6% | 80.9% | 16.7% | 2.3% |
| Rights, Policies | 42 (35.3%) | 77 (64.7%) | 36 (47.4%) | 40 (52.6%) | 108 (64.7%) | 59 (35.3%) | 55.7% | 36.1% | 8.2% | 70.5% | 25.6% | 3.9% |
| Oncological PC | 28 (23.5%) | 91 (76.5%) | 9 (11.8%) | 67 (88.2%) | 84 (50.3%) | 83 (49.7%) | 54.1% | 31.1% | 14.8% | 77.5% | 17.5% | 5.0% |
| Non-Oncological PCs | 29 (24.4%) | 90 (75.6%) | 12 (15.8%) | 64 (84.2%) | 89 (53.3%) | 78 (46.7%) | 59.0% | 32.8% | 8.2% | 75.2% | 20.6% | 4.2% |
| Pediatric PC | 19 (16.0%) | 100 (84.0%) | 9 (11.8%) | 67 (88.2%) | 35 (21.0%) | 132 (79.0%) | 55.7% | 29.5% | 14.8% | 80.4% | 15.4% | 4.2% |
| Needs people end of life | 47 (39.5%) | 72 (60.5%) | 26 (34.2%) | 50 (65.8%) | 104 (62.3%) | 63 (37.7%) | 62.3% | 32.8% | 4.9% | 80.2% | 15.9% | 3.9% |
| Physical symptoms | 34 (28.6%) | 85 (71.4%) | 12 (15.8%) | 64 (84.2%) | 105 (62.9%) | 62 (37.1%) | 62.3% | 27.9% | 9.8% | 83.8% | 12.3% | 3.9% |
| Nursing care | 21 (17.6%) | 98 (82.4%) | 10 (13.2%) | 66 (86.8%) | 126 (75.4%) | 41 (24.6%) | 42.6% | 27.9% | 29.5% | 66.3% | 26.1% | 7.6% |
| End of life emergencies | 20 (16.8%) | 99 (83.2%) | 6 (7.9%) | 70 (92.1%) | 67 (40.1%) | 100 (59.9%) | 50.8% | 31.1% | 18.0% | 80.7% | 14.1% | 5.2% |
| Last days | 24 (20.2%) | 95 (79.8%) | 9 (11.8%) | 67 (88.2%) | 88 (52.7%) | 79 (47.3%) | 62.3% | 29.5% | 8.2% | 76.2% | 18.3% | 5.5% |
| Death and mourning | 41 (34.5%) | 78 (65.5%) | 26 (34.2%) | 50 (65.8%) | 109 (65.3%) | 58 (34.7%) | 70.5% | 27.9% | 1.6% | 79.9% | 14.1% | 6.0% |
| Psychological aspects, communication | 39 (32.8%) | 80 (67.2%) | 21 (27.6%) | 55 (72.4%) | 107 (64.1%) | 60 (35.9%) | 72.1% | 26.2% | 1.6% | 79.9% | 15.4% | 4.7% |
| Social aspects | 30 (25.2%) | 89 (74.8%) | 16 (21.1%) | 60 (78.9%) | 100 (59.9%) | 67 (40.1%) | 62.3% | 34.4% | 3.3% | 72.3% | 22.5% | 5.2% |
| Cultural and spiritual aspects | 29 (24.4%) | 90 (75.6%) | 16 (21.1%) | 60 (78.9%) | 95 (56.9%) | 72 (43.1%) | 66.9% | 27.3% | 5.8% | 67.6% | 26.6% | 5.7% |
| Community aspects and networks | 33 (27.7%) | 86 (72.3%) | 14 (18.4%) | 62 (81.6%) | 102 (61.1%) | 65 (38.9%) | 63.9% | 32.8% | 3.3% | 70.5% | 23.5% | 6.0% |
| Social awareness | 36 (30.3%) | 83 (69.7%) | 20 (26.3%) | 56 (73.7%) | 86 (51.5%) | 81 (48.5%) | 60.7% | 36.1% | 3.3% | 70.2% | 24.5% | 5.2% |
| Volunteer programs | 31 (26.1%) | 88 (73.9%) | 11 (14.5%) | 65 (85.5%) | 55 (32.9%) | 112 (67.1%) | 52.5% | 39.3% | 8.2% | 74.2% | 19.1% | 6.8% |
| Integrated care | 30 (25.2%) | 89 (74.8%) | 8 (10.5%) | 68 (89.5%) | 73 (43.7%) | 94 (56.3%) | 60.7% | 34.4% | 4.9% | 69.5% | 24.5% | 6.0% |
| Tools to care | 28 (23.5%) | 91 (76.5%) | 11 (14.5%) | 65 (85.5%) | 97 (58.1%) | 70 (41.9%) | 70.5% | 24.6% | 4.9% | 79.4% | 15.7% | 5.0% |
| Compassionate, active listening, emotional | 48 (40.3%) | 71 (59.7%) | 20 (26.3%) | 56 (73.7%) | 106 (63.5%) | 61 (36.5%) | 75.4% | 23.0% | 1.6% | 84.3% | 11.0% | 4.7% |
| Investigation and evaluation | 17 (14.3%) | 102 (85.7%) | 12 (15.8%) | 64 (84.2%) | 79 (47.3%) | 88 (52.7%) | 62.3% | 29.5% | 8.2% | 77.5% | 17.2% | 5.2% |
| Management and organization | 17 (14.3%) | 102 (85.7%) | 5 (6.6%) | 71 (93.4%) | 76 (45.5%) | 91 (54.5%) | 50.8% | 41.0% | 8.2% | 71.3% | 22.5% | 6.3% |
| Networks and Compassionate Communities | 20 (16.8%) | 99 (83.2%) | 8 (10.5%) | 68 (89.5%) | 67 (40.1%) | 100 (59.9%) | 55.7% | 41.0% | 3.3% | 71.8% | 23.0% | 5.2% |
| Public politics | 19 (16.0%) | 100 (84.0%) | 7 (9.2%) | 69 (90.8%) | 79 (47.3%) | 88 (52.7%) | 59.0% | 34.4% | 6.6% | 67.9% | 25.3% | 6.8% |
| Rights of care | 38 (31.9%) | 81 (68.1%) | 16 (21.1%) | 60 (78.9%) | 103 (61.7%) | 64 (38.3%) | 68.9% | 29.5% | 1.6% | 80.7% | 14.1% | 5.2% |
| Sex | Self-Compassion | Compassion for Others | Compassion from Others | ||||||
| Mean | Eng | Act | Mean | Eng | Act | Mean | Eng | Act | |
| Male | 73.04 | 41.75 | 31.28 | 73 | 42.74 | 30.25 | 61.30 | 35.57 | 25.73 |
| Female | 69.67 | 39.91 | 29.75 | 72.47 | 42.03 | 30.44 | 60.18 | 34.71 | 25.46 |
| SELF-COMPASSION | COMPASSION FOR OTHER | COMPASSION FROM OTHERS | |||||||
| t = −0.356 | t = −0.612 | ||||||||
| p-value = 0.722 | p-value = 0.541 | ||||||||
| Age | Self-Compassion | Compassion for Others | Compassion from Others | ||||||
| Mean | Eng | Act | Mean | Eng | Act | Mean | Eng | Act | |
| 18–39 years | 70.32 | 40.19 | 30.13 | 72.29 | 41.98 | 30.30 | 60.46 | 34.86 | 25.59 |
| 40–59 years | 71.71 | 41.69 | 30.02 | 74.53 | 43.81 | 30.71 | 59.83 | 35.12 | 24.71 |
| > 60 years | 79.75 | 45.5 | 34.25 | 81.75 | 46.25 | 35.5 | 69.75 | 40 | 29.75 |
| SELF-COMPASSION | COMPASSION FOR OTHER | COMPASSION FROM OTHERS | |||||||
| F = 1.012 | F = 2.138 | F = 1.331 | |||||||
| p-value = 0.039 * | p-value = 0.119 | p-value = 0.265 | |||||||
| Self-Compassion | Compassion for Others | Compassion from Others | |||||||
| Mean | Engagement | Action | Mean | Engagement | Action | Mean | Engagement | Action | |
| Academics | 73.77 | 43.14 | 30.62 | 72.93 | 43.09 | 29.83 | 59.01 | 34.42 | 24.59 |
| Medicine Student | 69.03 | 39.23 | 29.79 | 72.36 | 42.10 | 30.25 | 59.95 | 34.04 | 25.91 |
| Psychology Student | 71.59 | 40.23 | 31.35 | 74.94 | 43.42 | 31.52 | 58.89 | 33.98 | 24.90 |
| Nursing Student | 69.41 | 39.86 | 29.55 | 71.29 | 41.08 | 30.20 | 61.82 | 35.92 | 25.89 |
| Self-Compassion | Compassion for Other | Compassion from Others | |||||||
| F = 3.327 | F = 1.423 | F = 0.607 | |||||||
| p-value = 0.364 * | p-value = 0.242 | p-value = 0.545 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Librada Flores, S.; Roa Trujillo, S.H.; Torrejano Gonzálex, N.; García Buitrago, M.d.P.; Lucas Díaz, M.Á. A Survey of Attitudes and Beliefs about Care, Compassion and Communities Networks in Palliative Care. A Preliminary Study for the Development of a Compassionate University. Healthcare 2021, 9, 946. https://doi.org/10.3390/healthcare9080946
Librada Flores S, Roa Trujillo SH, Torrejano Gonzálex N, García Buitrago MdP, Lucas Díaz MÁ. A Survey of Attitudes and Beliefs about Care, Compassion and Communities Networks in Palliative Care. A Preliminary Study for the Development of a Compassionate University. Healthcare. 2021; 9(8):946. https://doi.org/10.3390/healthcare9080946
Chicago/Turabian StyleLibrada Flores, Silvia, Sonia Herminia Roa Trujillo, Nurlian Torrejano Gonzálex, María del Pilar García Buitrago, and Miguel Ángel Lucas Díaz. 2021. "A Survey of Attitudes and Beliefs about Care, Compassion and Communities Networks in Palliative Care. A Preliminary Study for the Development of a Compassionate University" Healthcare 9, no. 8: 946. https://doi.org/10.3390/healthcare9080946
APA StyleLibrada Flores, S., Roa Trujillo, S. H., Torrejano Gonzálex, N., García Buitrago, M. d. P., & Lucas Díaz, M. Á. (2021). A Survey of Attitudes and Beliefs about Care, Compassion and Communities Networks in Palliative Care. A Preliminary Study for the Development of a Compassionate University. Healthcare, 9(8), 946. https://doi.org/10.3390/healthcare9080946