

Potential Effects of Non-Surgical Periodontal Therapy on Periodontal Parameters, Inflammatory Markers, and Kidney Function Indicators in Chronic Kidney Disease Patients with Chronic Periodontitis

 , ,
, ,
Abstract
:1. Introduction
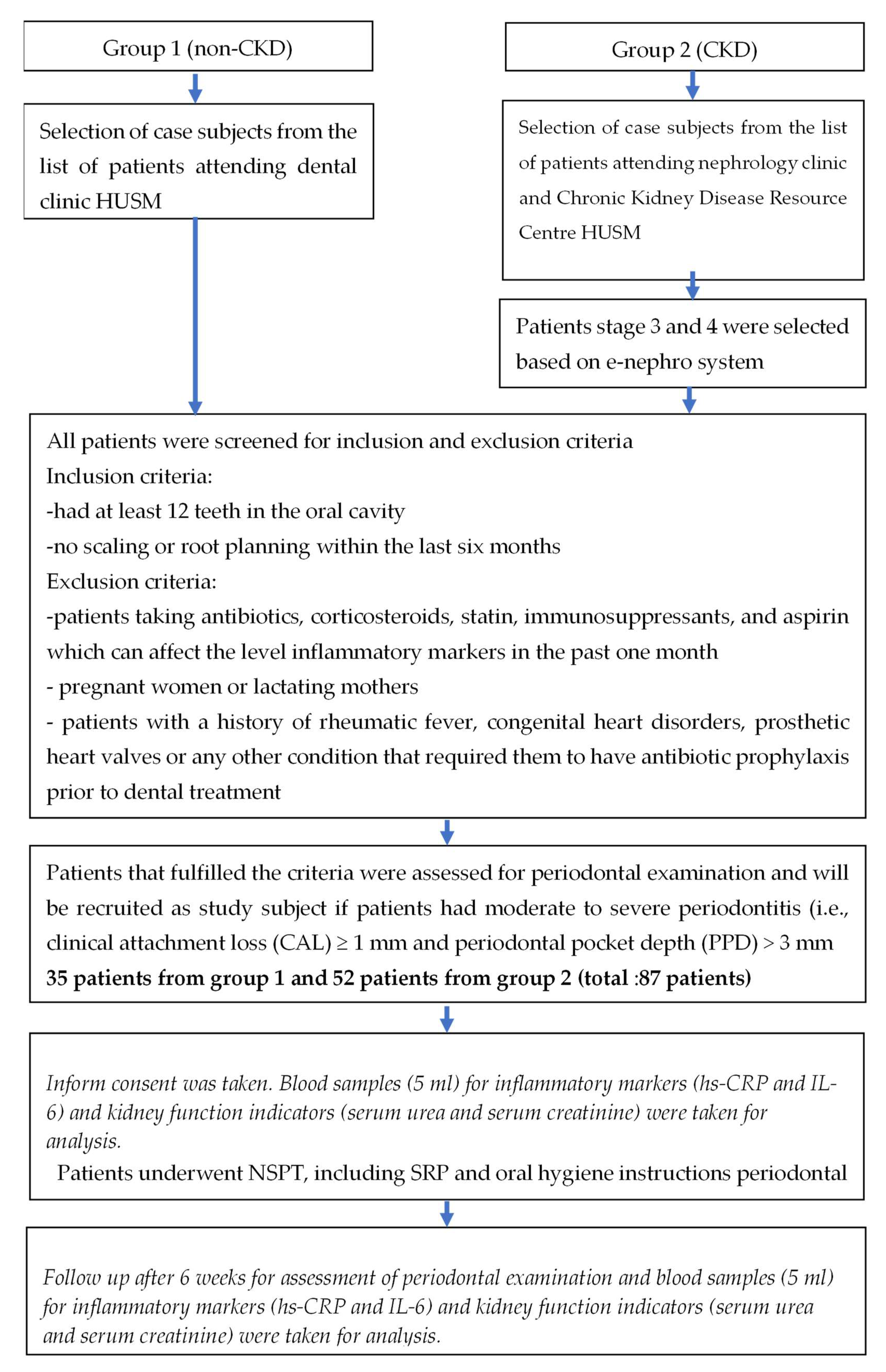
2. Materials and Methods
2.1. Ethical Considerations
2.2. Inclusion and Exclusion Criteria
2.3. Assessment of Clinical Periodontal Parameters
2.4. Collection of Blood Samples
2.5. Provision of NSPT
2.6. Biochemical Assay
2.7. Statistical Analysis
3. Results
3.1. Primary Characteristics of Study Participants
3.2. Clinical Periodontal Parameters
3.3. Inflammatory Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frencken, J.E.; Sharma, P.; Stenhouse, L.; Green, D.; Laverty, D.; Dietrich, T. Global epidemiology of dental caries and severe periodontitis—A comprehensive review. J. Clin. Periodontol. 2017, 44, S94–S105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Prim. 2017, 3, 17038. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.D.A.; Nguyen, T.T.T.; Pham, T.A.V. Periodontal Status in Chronic Kidney Disease Patients. UI Proc. Health Med. 2017, 1, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Clinical, K. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Cengiz, M.I.; Bal, S.; Gökçay, S.; Cengiz, K. Does periodontal disease reflect atherosclerosis in continuous ambulatory peritoneal dialysis patients? J. Periodontol. 2007, 78, 1926–1934. [Google Scholar] [CrossRef]
- Selim, G.; Stojceva-Taneva, O.; Zafirovska, K.; Sikole, A.; Gelev, S.; Dzekova, P.; Stefanovski, K.; Koloska, V.; Polenakovic, M. Inflammation predicts all-cause and cardiovascular mortality in haemodialysis patients. Prilozi 2006, 27, 133–144. [Google Scholar]
- Stenvinkel, P.; Alvestrand, A. Inflammation in end-stage renal disease: Sources, consequences, and therapy. Semin. Dial. 2002, 15, 329–337. [Google Scholar] [CrossRef]
- Fisher, M.A.; Taylor, G.W.; West, B.T.; McCarthy, E.T. Bidirectional relationship between chronic kidney and periodontal disease: A study using structural equation modeling. Kidney Int. 2011, 79, 347–355. [Google Scholar] [CrossRef] [Green Version]
- Wahid, A.; Chaudhry, S.; Ehsan, A.; Butt, S.; Ali Khan, A. Bidirectional Relationship between Chronic Kidney Disease & Periodontal Disease. Pak. J. Med. Sci. 2013, 29, 211–215. [Google Scholar] [PubMed]
- Oyetola, E.O.; Owotade, F.J.; Agbelusi, G.A.; Fatusi, O.A.; Sanusi, A.A. Oral findings in chronic kidney disease: Implications for management in developing countries. BMC Oral Health 2015, 15, 24. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, E.S. Periodontal Infections, Inflammatory Markers in Chronic Kidney Disease. Master’s Thesis, University of Connecticut, Tolland, CT, USA, 2010. [Google Scholar]
- Craig, R.G. Interactions between chronic renal disease and periodontal disease. Oral Dis. 2008, 14, 1–7. [Google Scholar] [CrossRef]
- Dioguardi, M.; Caloro, G.A.; Troiano, G.; Giannatempo, G.; Laino, L.; Petruzzi, M.; Lo Muzio, L. Oral manifestations in chronic uremia patients. Ren. Fail. 2016, 38, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Chambrone, L.; Foz, A.M.; Guglielmetti, M.R.; Pannuti, C.M.; Artese, H.P.; Feres, M.; Romito, G.A. Periodontitis and chronic kidney disease: A systematic review of the association of diseases and the effect of periodontal treatment on estimated glomerular filtration rate. J. Clin. Periodontol. 2013, 40, 443–456. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int. Suppl. 2009, 76, S1–S130. [Google Scholar]
- Tanwar, J.; Hungund, S.; Dodani, K. Nonsurgical periodontal therapy: A review. J. Oral Res. Rev. 2016, 8, 39–44. [Google Scholar] [CrossRef]
- Son, A.; Pera, C.; Ueda, P.; Casarin, R.C.V.; Pimentel, S.P.; Cirano, F.R. Clinical effects of supragingival plaque control on uncontrolled type 2 diabetes mellitus subjects with chronic periodontitis. Braz. J. Oral Sci. 2016, 47–51, 1677–3225. [Google Scholar]
- Sanz, I.; Alonso, B.; Carasol, M.; Herrera, D.; Sanz, M. Nonsurgical treatment of periodontitis. J. Evid.-Based Dent. Pract. 2012, 12, 76–86. [Google Scholar] [CrossRef]
- Tonetti, M.S.; D’Aiuto, F.; Nibali, L.; Donald, A.; Storry, C.; Parkar, M.; Suvan, J.; Hingorani, A.D.; Vallance, P.; Deanfield, J. Treatment of periodontitis and endothelial function. N. Engl. J. Med. 2007, 356, 911–920. [Google Scholar] [CrossRef] [Green Version]
- Ritam, S.; Jyoti, R. Effect of periodontal treatment on plasma fibrinogen, serum C-reactive protein and total white blood cell count in periodontitis patients: A prospective interventional trial. Rom. J. Intern. Med. 2013, 51, 45–51. [Google Scholar]
- Mohammed, M.; Jesmin, F.; Kassim, N.K.; Zainuddin, S.L.; Hanafi, M.H.; Kamarudin, M.I.; Ahmad, F.; Sirajudeen, K. Levels of interleukins in patients with chronic kidney disease and periodontitis: A systematic review. J. Int. Oral. Health 2021, 13, 313–318. [Google Scholar]
- Zhang, Q.; Chen, B.; Zhu, D.; Yan, F. Biomarker levels in gingival crevicular fluid of subjects with different periodontal conditions: A cross-sectional study. Arch. Oral Biol. 2016, 72, 92–98. [Google Scholar] [CrossRef]
- Kumar, S.; Shah, S.; Budhiraja, S.; Desai, K.; Shah, C.; Mehta, D. The effect of periodontal treatment on C-reactive protein: A clinical study. J. Nat. Sci. Biol. Med. 2013, 4, 379–382. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Periodontology, O. American Academy of Periodontology Task Force report on the update to the 1999 classification of periodontal diseases and conditions. J. Periodontol. 2015, 86, 835–838. [Google Scholar]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Ribeiro, É.D.P.; Bittencourt, S.; Nociti-Júnior, F.H.; Sallum, E.A.; Sallum, A.W.; Casati, M.Z. The effect of one session of supragingival plaque control on clinical and biochemical parameters of chronic periodontitis. J. Appl. Oral Sci. 2005, 13, 275–279. [Google Scholar] [CrossRef]
- Haffajee, A.; Cugini, M.; Dibart, S.; Smith, C.; Kent Jr, R.; Socransky, S. The effect of SRP on the clinical and microbiological parameters of periodontal diseases. J. Clin. Periodontol. 1997, 24, 324–334. [Google Scholar] [CrossRef]
- Graziani, F.; Cei, S.; La Ferla, F.; Vano, M.; Gabriele, M.; Tonetti, M. Effects of non-surgical periodontal therapy on the glomerular filtration rate of the kidney: An exploratory trial. J. Clin. Periodontol. 2010, 37, 638–643. [Google Scholar] [CrossRef]
- Taylor, B.; Tofler, G.; Morel-Kopp, M.C.; Carey, H.; Carter, T.; Elliott, M.; Dailey, C.; Villata, L.; Ward, C.; Woodward, M. The effect of initial treatment of periodontitis on systemic markers of inflammation and cardiovascular risk: A randomized controlled trial. Eur. J. Oral Sci. 2010, 118, 350–356. [Google Scholar] [CrossRef]
- Chakraborty, S.; Tewari, S.; Sharma, R.K.; Narula, S.C. Effect of non-surgical periodontal therapy on serum ferritin levels: An interventional study. J. Periodontol. 2014, 85, 688–696. [Google Scholar] [CrossRef]
- Chang, P.Y.; Chien, L.N.; Lin, Y.F.; Wu, M.S.; Chiu, W.T.; Chiou, H.Y. Risk factors of gender for renal progression in patients with early chronic kidney disease. Medicine 2016, 95, e4203. [Google Scholar] [CrossRef] [PubMed]
- Duru, O.K.; Li, S.; Jurkovitz, C.; Bakris, G.; Brown, W.; Chen, S.C.; Collins, A.; Klag, M.; McCullough, P.A.; McGill, J.; et al. Race and sex differences in hypertension control in CKD: Results from the Kidney Early Evaluation Program (KEEP). Am. J. Kidney Dis. 2008, 51, 192–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komura, H.; Nomura, I.; Kitamura, K.; Kuwasako, K.; Kato, J. Gender difference in relationship between body mass index and development of chronic kidney disease. BMC Res. Notes 2013, 6, 463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.-F.; Yeh, J.-C.; Chiu, Y.-L.; Liou, J.-C.; Hsiung, J.-R.; Tung, T.-H. Periodontal pocket depth, hyperglycemia, and progression of chronic kidney disease: A population-based longitudinal study. Am. J. Med. 2017, 130, 61–69.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, M.A.; Taylor, G.W.; Papapanou, P.N.; Rahman, M.; Debanne, S.M. Clinical and serologic markers of periodontal infection and chronic kidney disease. J. Periodontol. 2008, 79, 1670–1678. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Taylor, G.W.; Nesse, W.; Vissink, A.; Yoshihara, A.; Miyazaki, H. Periodontal disease and decreased kidney function in Japanese elderly. Am. J. Kidney Dis. 2012, 59, 202–209. [Google Scholar] [CrossRef]
- Deshpande, K.; Jain, A.; Sharma, R.; Prashar, S.; Jain, R. Diabetes and periodontitis. J. Indian Soc. Periodontol. 2010, 14, 207–212. [Google Scholar] [CrossRef]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontol. 2000 2013, 62, 59–94. [Google Scholar] [CrossRef]
- Badersten, A.; Nilveus, R.; Egelberg, J. Effect of nonsurgical periodontal therapy. J. Clin. Periodontol. 1984, 11, 63–76. [Google Scholar] [CrossRef]
- Umeda, M.; Takeuchi, Y.; Noguchi, K.; Huang, Y.; Koshy, G.; Ishikawa, I. Effects of nonsurgical periodontal therapy on the microbiota. Periodontol. 2000 2004, 36, 98–120. [Google Scholar] [CrossRef] [PubMed]
- Artese, H.P.C.; Sousa, C.O.; Luiz, R.R.; Sansone, C.; Torres, M.C.M. Effect of non-surgical periodontal treatment on chronic kidney disease patients. Braz. Oral Res. 2010, 24, 449–454. [Google Scholar] [CrossRef]
- Fang, F.; Wu, B.; Qu, Q.; Gao, J.; Yan, W.; Huang, X.; Ma, D.; Yue, J.; Chen, T.; Liu, F. The clinical response and systemic effects of non-surgical periodontal therapy in end-stage renal disease patients: A 6-month randomized controlled clinical trial. J. Clin. Periodontol. 2015, 42, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Guo, N.; Lin, G. Effects of nonsurgical periodontal therapy on serum inflammatory factor levels in patients with chronic kidney disease and periodontitis. Biomed. Res.-India 2017, 28, 3899–3902. [Google Scholar]
- Pecoits-Filho, R.; Heimburger, O.; Barany, P.; Suliman, M.; Fehrman-Ekholm, I.; Lindholm, B.; Stenvinkel, P. Associations between circulating inflammatory markers and residual renal function in CRF patients. Am. J. Kidney Dis. 2003, 41, 1212–1218. [Google Scholar] [CrossRef]
- Mihai, S.; Codrici, E.; Popescu, I.D.; Enciu, A.-M.; Albulescu, L.; Necula, L.G.; Mambet, C.; Anton, G.; Tanase, C. Inflammation-Related Mechanisms in Chronic Kidney Disease Prediction, Progression, and Outcome. J. Immunol. Res. 2018, 2018, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrivastava, A.K.; Singh, H.V.; Raizada, A.; Singh, S.K. C-reactive protein, inflammation and coronary heart disease. Egypt. Heart J. 2015, 67, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Yeun, J.Y.; Levine, R.A.; Mantadilok, V.; Kaysen, G.A. C-Reactive protein predicts all-cause and cardiovascular mortality in hemodialysis patients. Am. J. Kidney Dis. 2000, 35, 469–476. [Google Scholar] [CrossRef]
- Ismail, G.; Dumitriu, H.T.; Dumitriu, A.S.; Ismail, F.B. Periodontal disease: A covert source of inflammation in chronic kidney disease patients. Int. J. Nephrol. 2013, 2013, 515796. [Google Scholar] [CrossRef]
- Hussain Bokhari, S.A.; Khan, A.A.; Tatakis, D.N.; Azhar, M.; Hanif, M.; Izhar, M. Non-Surgical Periodontal Therapy Lowers Serum Inflammatory Markers: A Pilot Study. J. Periodontol. 2009, 80, 1574–1580. [Google Scholar] [CrossRef]
- Vilela, E.M.; Bastos, J.A.; Fernandes, N.; Ferreira, A.P.; Chaoubah, A.; Bastos, M.G. Treatment of chronic periodontitis decreases serum prohepcidin levels in patients with chronic kidney disease. Clinics 2011, 66, 657–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamazaki, K.; Honda, T.; Oda, T.; Ueki-Maruyama, K.; Nakajima, T.; Yoshie, H.; Seymour, G.J. Effect of periodontal treatment on the C-reactive protein and proinflammatory cytokine levels in Japanese periodontitis patients. J. Periodontal Res. 2005, 40, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Ide, M.; Jagdev, D.; Coward, P.Y.; Crook, M.; Barclay, G.R.; Wilson, R.F. The short-term effects of treatment of chronic periodontitis on circulating levels of endotoxin, C-reactive protein, tumor necrosis factor-alpha, and interleukin-6. J. Periodontol. 2004, 75, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Piconi, S.; Trabattoni, D.; Luraghi, C.; Perilli, E.; Borelli, M.; Pacei, M.; Rizzardini, G.; Lattuada, A.; Bray, D.H.; Catalano, M. Treatment of periodontal disease results in improvements in endothelial dysfunction and reduction of the carotid intima-media thickness. FASEB J. 2009, 23, 1196–1204. [Google Scholar] [CrossRef] [PubMed]
- Cobb, C.M. Microbes, inflammation, scaling and root planing, and the periodontal condition. Am. Dent. Hyg. Assoc. 2008, 82, 4–9. [Google Scholar]


{kind=link}
| Study Groups | Significance | ||
|---|---|---|---|
| Demographic Features | Non-CKD Group n (%) (n = 33) | CKD Group n (%) (n = 33) | p-Value |
| Age (years) (mean ± SD) | 49.18 ± 8.58 | 55.96 ± 11.26 | 0.1 |
| Gender | |||
| Male Female | 16 (24.2) 17 (25.8) | 27 (40.9) 6 (9.1) | 0.004 |
| Ethnicity | |||
| Malay Chinese | 28 (42.4) 5 (7.6) | 31 (47) 2 (3) | 0.4 |
| Marital status | |||
| Married Single | 28 (42.4) 5 (7.6) | 27 (40.9) 6 (9.1) | 0.7 |
| Mean number of teeth present | 24.36 ± 3.89 | 19.51 ± 6.23 | < 0.001 |
| Smoking | |||
| Non-smokers Ex-smokers Active smokers | 22 (33.3) 7 (10.6) 4 (6.1) | 25 (37.9) 6 (9.1) 2 (3.0) | 0.7 |
| CKD staging | |||
| Stage-III Stage-IV | - - | 12 (36.4) 21 (63.6) | |
| Medical illness | |||
| Diabetes mellitus Hypertension Ischemic heart disease Other medical illnesses No medical illness | 1 9 - - 23 | 19 23 6 5 - | |
| Periodontal Parameters | Baseline | Six Weeks Follow-Up | p-Value |
|---|---|---|---|
| PPD (mm) | ptime * group = 0.002 ptime < 0.001 pgroup = 0.9 | ||
| Non-CKD | 4.76 ± 0.52 | 2.97 ± 0.74 * | |
| CKD | 5.02 ± 0.50 † | 2.74 ± 0.50 * | |
| p-value | 0.046 | 0.15 | |
CAL (mm) | ptime * group = 0.02 ptime < 0.001 pgroup = 0.1 | ||
| Non-CKD | 4.79 ± 0.53 | 3.20 ± 0.152 * | |
| CKD | 5.34 ± 1.06 † | 3.27 ± 0.152 * | |
| p-value | 0.01 | 0.77 | |
| GBI (%) | ptime * group = 0.9 ptime < 0.001 pgroup = 0.3 | ||
| Non-CKD | 52.78 ± 22.33 | 19.68 ±13.38 * | |
| CKD | 56.12 ± 19.01 | 23.30 ± 5.81 * | |
| p-value | 0.515 | 0.171 | |
| PS (%) | ptime * group = 0.6 ptime < 0.001 pgroup = 0.3 | ||
| Non-CKD | 63.61 ± 18.41 | 23.49 ± 14.17 * | |
| CKD | 61.53 ± 20.78 | 19.27 ± 8.16 * | |
| p-value | 0.688 | 0.143 |
| Variables | Baseline | Six Weeks Follow-Up | p-Value |
|---|---|---|---|
| hs-CRP (mg/L) | ptime * group = 0.2 ptime < 0.001 pgroup = 0.02 | ||
| Non-CKD | 1.71 ± 1.64 | 0.82 ± 0.71 * | |
| CKD | 3.07 ± 2.37 † | 1.50 ± 1.38 * | |
| p-value | 0.03 | 0.041 | |
| IL-6 (pg/mL) | ptime * group = 0.3 ptime = 0.001 pgroup = 0.002 | ||
| Non-CKD | 2.54 ± 1.09 | 1.89 ± 0.63 * | |
| CKD | 4.11 ± 2.84 † | 2.93 ± 1.47 * | |
| p-value | 0.013 | 0.002 | |
| Serum urea (mmol/L) | ptime * group = 0.9 ptime = 0.8 pgroup < 0.001 | ||
| Non-CKD | 4.15 ± 1.23 | 4.04 ± 1.15 | |
| CKD | 12.57 ± 4.84 † | 12.30 ± 5.35 | |
| p-value | < 0.001 | < 0.001 | |
| eGFR (mL/min/1.73 m2) | ptime * group = 0.6 ptime = 0.1 pgroup < 0.001 | ||
| Non-CKD | 89.60 ± 21.33 | 92.21 ± 18.30 | |
| CKD | 25.96 ± 10.56 † | 27.18 ± 12.17 | |
| p-value | < 0.001 | < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaudhry, A.; Kassim, N.K.; Zainuddin, S.L.A.; Taib, H.; Ibrahim, H.A.; Ahmad, B.; Hanafi, M.H.; Adnan, A.S. Potential Effects of Non-Surgical Periodontal Therapy on Periodontal Parameters, Inflammatory Markers, and Kidney Function Indicators in Chronic Kidney Disease Patients with Chronic Periodontitis. Biomedicines 2022, 10, 2752. https://doi.org/10.3390/biomedicines10112752
Chaudhry A, Kassim NK, Zainuddin SLA, Taib H, Ibrahim HA, Ahmad B, Hanafi MH, Adnan AS. Potential Effects of Non-Surgical Periodontal Therapy on Periodontal Parameters, Inflammatory Markers, and Kidney Function Indicators in Chronic Kidney Disease Patients with Chronic Periodontitis. Biomedicines. 2022; 10(11):2752. https://doi.org/10.3390/biomedicines10112752
Chicago/Turabian StyleChaudhry, Ahmed, Nur Karyatee Kassim, Siti Lailatul Akmar Zainuddin, Haslina Taib, Hanim Afzan Ibrahim, Basaruddin Ahmad, Muhammad Hafiz Hanafi, and Azreen Syazril Adnan. 2022. "Potential Effects of Non-Surgical Periodontal Therapy on Periodontal Parameters, Inflammatory Markers, and Kidney Function Indicators in Chronic Kidney Disease Patients with Chronic Periodontitis" Biomedicines 10, no. 11: 2752. https://doi.org/10.3390/biomedicines10112752
APA StyleChaudhry, A., Kassim, N. K., Zainuddin, S. L. A., Taib, H., Ibrahim, H. A., Ahmad, B., Hanafi, M. H., & Adnan, A. S. (2022). Potential Effects of Non-Surgical Periodontal Therapy on Periodontal Parameters, Inflammatory Markers, and Kidney Function Indicators in Chronic Kidney Disease Patients with Chronic Periodontitis. Biomedicines, 10(11), 2752. https://doi.org/10.3390/biomedicines10112752