
Baseline Circulating miR-125b Levels Predict a High FIB-4 Index Score in Chronic Hepatitis B Patients after Nucleos(t)ide Analog Treatment

 , , , , , , ,
, , , , , , ,  and
and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Patients
2.3. Laboratory Data
2.4. Extraction of MicroRNAs
2.5. Questionnaire Interview for Patient Profiles
2.6. Statistical Analysis
3. Results
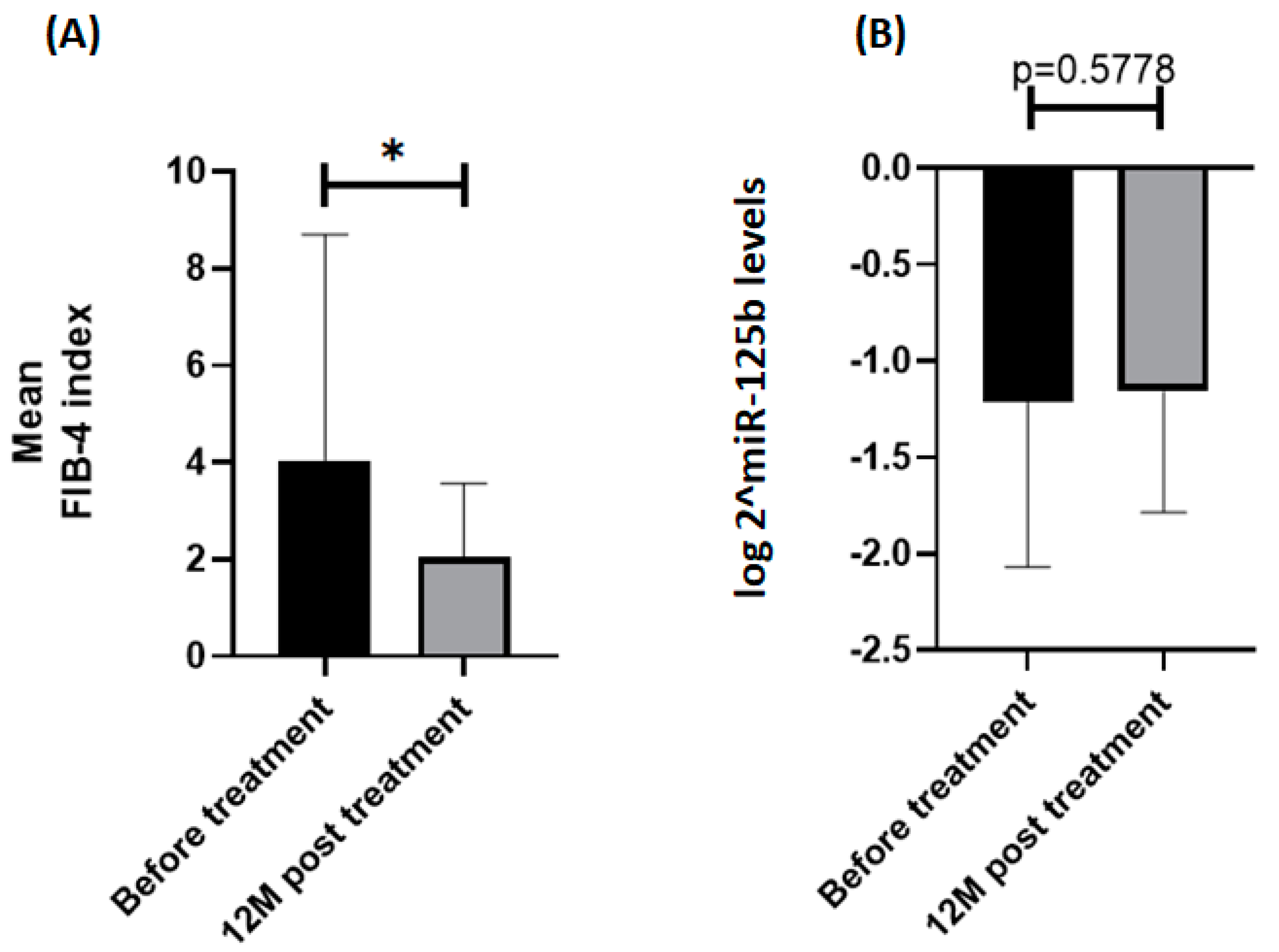
3.1. Characteristics of Patients and Changes in the Parameters
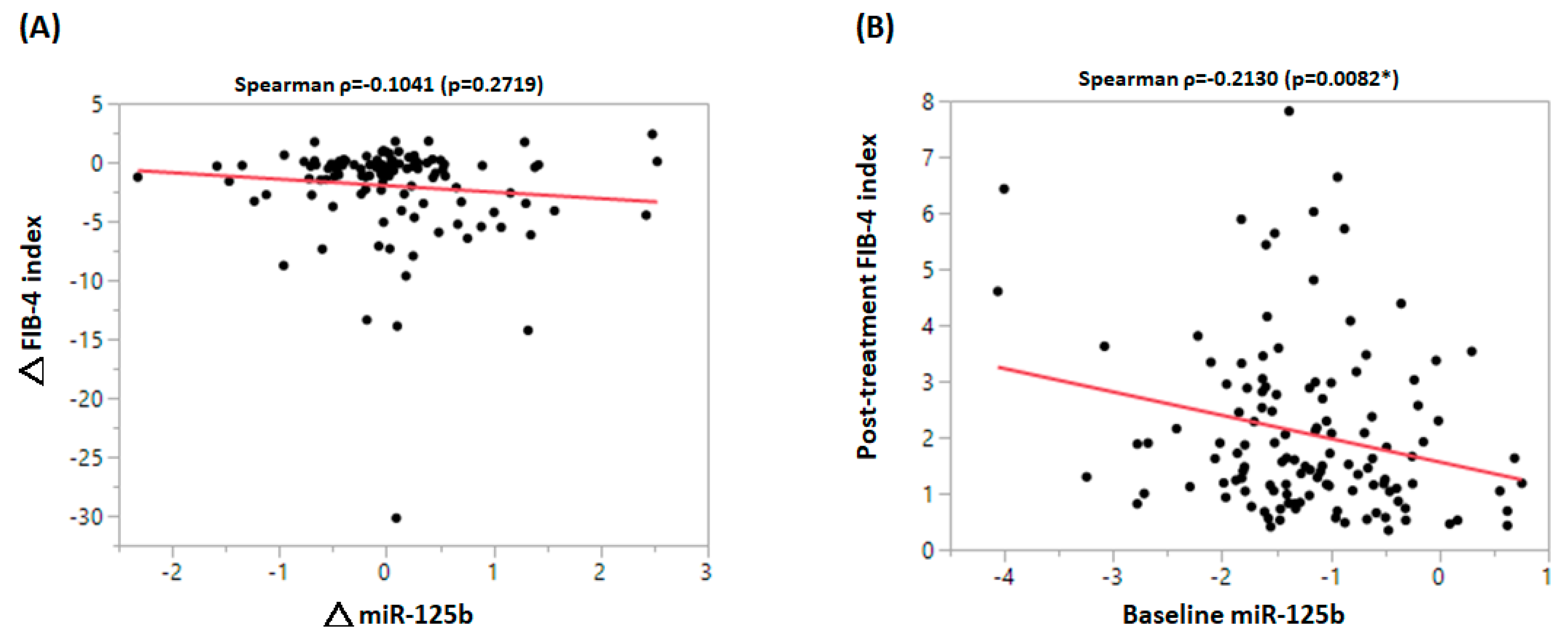
3.2. Baseline and Clinical Parameters Associated with FIB-4 Index after NA Treatment
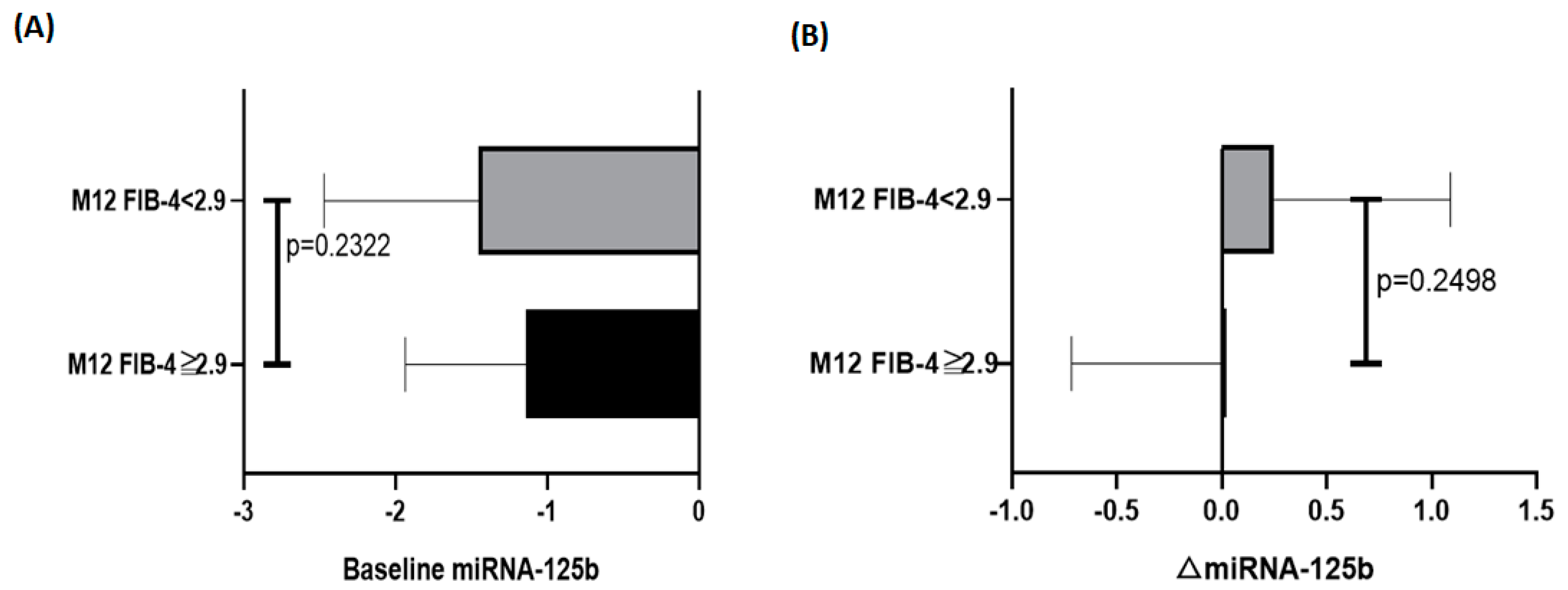
3.3. miR-125b Predicts Liver Fibrosis Stratified by ETV and LAM Response
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- GBD 2019 Hepatitis B Collaborators. Global, regional, and national burden of hepatitis B, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Gastroenterol. Hepatol. 2022, 7, 796–829. [Google Scholar] [CrossRef]
- Fanning, G.C.; Zoulim, F.; Hou, J.; Bertoletti, A. Therapeutic strategies for hepatitis B virus infection: Towards a cure. Nat. Rev. Drug Discov. 2019, 18, 827–844. [Google Scholar] [CrossRef] [PubMed]
- Kanda, T.; Goto, T.; Hirotsu, Y.; Moriyama, M.; Omata, M. Molecular Mechanisms Driving Progression of Liver Cirrhosis towards Hepatocellular Carcinoma in Chronic Hepatitis B and C Infections: A Review. Int. J. Mol. Sci. 2019, 20, 1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.J.; Yang, H.I.; Su, J.; Jen, C.L.; You, S.L.; Lu, S.N.; Huang, G.T.; Iloeje, U.H.; Group, R.-H.S. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA 2006, 295, 65–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gines, P.; Krag, A.; Abraldes, J.G.; Sola, E.; Fabrellas, N.; Kamath, P.S. Liver cirrhosis. Lancet 2021, 398, 1359–1376. [Google Scholar] [CrossRef]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2021, 7, 6. [Google Scholar] [CrossRef]
- Zhang, Z.; Chen, J.; He, Y.; Zhan, X.; Zhao, R.; Huang, Y.; Xu, H.; Zhu, Z.; Liu, Q. miR-125b inhibits hepatitis B virus expression in vitro through targeting of the SCNN1A gene. Arch. Virol. 2014, 159, 3335–3343. [Google Scholar] [CrossRef]
- Sartorius, K.; Makarova, J.; Sartorius, B.; An, P.; Winkler, C.; Chuturgoon, A.; Kramvis, A. The Regulatory Role of MicroRNA in Hepatitis-B Virus-Associated Hepatocellular Carcinoma (HBV-HCC) Pathogenesis. Cells 2019, 8, 1504. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; An, P.; Winkler, C.A.; Yu, Y. Dysregulated microRNAs in Hepatitis B Virus-Related Hepatocellular Carcinoma: Potential as Biomarkers and Therapeutic Targets. Front. Oncol. 2020, 10, 1271. [Google Scholar] [CrossRef]
- Jia, H.Y.; Wang, Y.X.; Yan, W.T.; Li, H.Y.; Tian, Y.Z.; Wang, S.M.; Zhao, H.L. MicroRNA-125b functions as a tumor suppressor in hepatocellular carcinoma cells. Int. J. Mol. Sci. 2012, 13, 8762–8774. [Google Scholar] [CrossRef]
- Zhao, L.; Wang, W. miR-125b suppresses the proliferation of hepatocellular carcinoma cells by targeting Sirtuin7. Int. J. Clin. Exp. Med. 2015, 8, 18469–18475. [Google Scholar] [PubMed]
- Wang, Y.; Wei, Y.; Fan, X.; Zhang, P.; Wang, P.; Cheng, S.; Zhang, J. MicroRNA-125b as a tumor suppressor by targeting MMP11 in breast cancer. Thorac. Cancer 2020, 11, 1613–1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhuri, A.A.; So, A.Y.; Sinha, N.; Gibson, W.S.; Taganov, K.D.; O’Connell, R.M.; Baltimore, D. MicroRNA-125b potentiates macrophage activation. J. Immunol. 2011, 187, 5062–5068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, P.; Dong, M.; Wang, J.; Li, F.; Zhang, J.; Gu, J. Baseline serum miR-125b levels predict virologic response to nucleos(t)ide analogue treatment in patients with HBeAg-positive chronic hepatitis B. Exp. Ther. Med. 2018, 16, 3805–3812. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Zhou, P.; Deng, W.; Wang, J.; Mao, R.; Zhang, Y.; Li, J.; Yu, J.; Yang, F.; Huang, Y.; et al. Serum microRNA-125b correlates with hepatitis B viral replication and liver necroinflammation. Clin. Microbiol. Infect. 2016, 22, 384.e1–384.e10. [Google Scholar] [CrossRef] [Green Version]
- Giray, B.G.; Emekdas, G.; Tezcan, S.; Ulger, M.; Serin, M.S.; Sezgin, O.; Altintas, E.; Tiftik, E.N. Profiles of serum microRNAs; miR-125b-5p and miR223-3p serve as novel biomarkers for HBV-positive hepatocellular carcinoma. Mol. Biol. Rep. 2014, 41, 4513–4519. [Google Scholar] [CrossRef] [PubMed]
- You, K.; Li, S.Y.; Gong, J.; Fang, J.H.; Zhang, C.; Zhang, M.; Yuan, Y.; Yang, J.; Zhuang, S.M. MicroRNA-125b Promotes Hepatic Stellate Cell Activation and Liver Fibrosis by Activating RhoA Signaling. Mol. Ther. Nucleic Acids 2018, 12, 57–66. [Google Scholar] [CrossRef]
- Yeh, M.L.; Huang, C.F.; Huang, C.I.; Holmes, J.A.; Hsieh, M.H.; Tsai, Y.S.; Liang, P.C.; Tsai, P.C.; Hsieh, M.Y.; Lin, Z.Y.; et al. Hepatitis B-related outcomes following direct-acting antiviral therapy in Taiwanese patients with chronic HBV/HCV co-infection. J. Hepatol. 2020, 73, 62–71. [Google Scholar] [CrossRef] [Green Version]
- Jieanu, C.F.; Ungureanu, B.S.; Sandulescu, D.L.; Gheonea, I.A.; Tudorascu, D.R.; Ciurea, M.E.; Purcarea, V.L. Quantification of liver fibrosis in chronic hepatitis B virus infection. J. Med. Life 2015, 8, 285–290. [Google Scholar]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Mark, S.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Shiha, G.; Ibrahim, A.; Helmy, A.; Sarin, S.K.; Omata, M.; Kumar, A.; Bernstien, D.; Maruyama, H.; Saraswat, V.; Chawla, Y.; et al. Asian-Pacific Association for the Study of the Liver (APASL) consensus guidelines on invasive and non-invasive assessment of hepatic fibrosis: A 2016 update. Hepatol. Int. 2017, 11, 1–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, Y.S.; Yeh, M.L.; Tsai, P.C.; Huang, C.I.; Huang, C.F.; Hsieh, M.H.; Liu, T.W.; Lin, Y.H.; Liang, P.C.; Lin, Z.Y.; et al. Clusters of Circulating let-7 Family Tumor Suppressors Are Associated with Clinical Characteristics of Chronic Hepatitis C. Int. J. Mol. Sci. 2020, 21, 4945. [Google Scholar] [CrossRef] [PubMed]
- Parikh, P.; Ryan, J.D.; Tsochatzis, E.A. Fibrosis assessment in patients with chronic hepatitis B virus (HBV) infection. Ann. Transl. Med. 2017, 5, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; He, J.; Li, C.; Benitez, R.; Fu, S.; Marrero, J.; Lubman, D.M. Identification and confirmation of biomarkers using an integrated platform for quantitative analysis of glycoproteins and their glycosylations. J. Proteome Res. 2010, 9, 798–805. [Google Scholar] [CrossRef] [Green Version]
- Li, L.M.; Hu, Z.B.; Zhou, Z.X.; Chen, X.; Liu, F.Y.; Zhang, J.F.; Shen, H.B.; Zhang, C.Y.; Zen, K. Serum microRNA profiles serve as novel biomarkers for HBV infection and diagnosis of HBV-positive hepatocarcinoma. Cancer Res. 2010, 70, 9798–9807. [Google Scholar] [CrossRef] [Green Version]
- Auvinen, E. Diagnostic and Prognostic Value of MicroRNA in Viral Diseases. Mol. Diagn. Ther. 2017, 21, 45–57. [Google Scholar] [CrossRef]
- Chen, S.; Chen, H.; Gao, S.; Qiu, S.; Zhou, H.; Yu, M.; Tu, J. Differential expression of plasma microRNA-125b in hepatitis B virus-related liver diseases and diagnostic potential for hepatitis B virus-induced hepatocellular carcinoma. Hepatol. Res. 2017, 47, 312–320. [Google Scholar] [CrossRef]
- Jin, Y.; Wong, Y.S.; Goh, B.K.P.; Chan, C.Y.; Cheow, P.C.; Chow, P.K.H.; Lim, T.K.H.; Goh, G.B.B.; Krishnamoorthy, T.L.; Kumar, R.; et al. Circulating microRNAs as Potential Diagnostic and Prognostic Biomarkers in Hepatocellular Carcinoma. Sci. Rep. 2019, 9, 10464. [Google Scholar] [CrossRef] [Green Version]
- Kawata, N.; Takahashi, H.; Iwane, S.; Inoue, K.; Kojima, M.; Kohno, M.; Tanaka, K.; Mori, H.; Isoda, H.; Oeda, S.; et al. FIB-4 index-based surveillance for advanced liver fibrosis in diabetes patients. Diabetol. Int. 2021, 12, 118–125. [Google Scholar] [CrossRef]
- Li, Y.; Regan, J.; Fajnzylber, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Atyeo, C.; Fischinger, S.; Gillespie, E.; et al. Liver Fibrosis Index FIB-4 Is Associated With Mortality in COVID-19. Hepatol. Commun. 2021, 5, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Vali, Y.; Boursier, J.; Spijker, R.; Anstee, Q.M.; Bossuyt, P.M.; Zafarmand, M.H. Prognostic accuracy of FIB-4, NAFLD fibrosis score and APRI for NAFLD-related events: A systematic review. Liver Int. 2021, 41, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Mallet, V.; Parlati, L.; Vallet-Pichard, A.; Terris, B.; Tsochatzis, E.; Sogni, P.; Pol, S. FIB-4 index to rule-out advanced liver fibrosis in NAFLD patients. Presse Med. 2019, 48, 1484–1488. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Overall | FIB-4 Score ≤ 2.9 | FIB-4 Score > 2.9 (n = 54) | p Value |
|---|---|---|---|---|
| (n = 124) | (n = 70) | |||
| Mean age (years) | 47.95 (11.75) | 43.49 (11.26) | 53.72 (9.76) | <0.0001 * |
| Gender | 0.3810 | |||
| Male | 95 | 52 | 43 | |
| Female | 29 | 18 | 11 | |
| BMI (kg/m2) | 23.99 (3.59) | 24.10 (3.37) | 23.88 (3.87) | 0.7620 |
| BH (cm) | 166.59 (8.02) | 168.23 (7.60) | 164.52 (8.13) | 0.0060 * |
| BW (kg) | 66.75 (12.20) | 68.25 (11.22) | 64.92 (13.18) | 0.0746 |
| HBV DNA > 2000 IU/mL (%) | 76.61 | 70.00 | 85.19 | 0.0476 * |
| HBeAg(+) | 30.89 (38/123) | 31.88 (22/69) | 29.63 (17/54) | 0.7883 |
| Lab data (mean, SD) | ||||
| WBCs (×103/mm3) | 5585.79 (1751.43) | 6072.50 (1753.19) | 4961.32 (1552.85) | 0.0004 * |
| Platelet (×103/mm3) | 170.43 (71.12) | 204.93 (70.29) | 125.70 (41.18) | <0.0001 * |
| AST (U/L) | 227.64 (314.82) | 111.69 (137.87) | 377.94 (405.57) | <0.0001 * |
| ALT (U/L) | 343.16 (435.35) | 215.17 (272.48) | 509.07 (541.77) | 0.0001 * |
| Creatinine (mg/dL) | 0.89 (0.48) | 0.86 (0.24) | 0.92 (0.66) | 0.5363 |
| Bilirubin (mg/dL) | 2.00 (2.57) | 1.37 (1.48) | 2.69 (3.37) | 0.0045 * |
| Albumin (gm/dL) | 4.02 (0.53) | 4.26 (0.36) | 3.72 (0.54) | <0.0001 * |
| HB (g/dL) | 13.95 (1.56) | 14.20 (1.60) | 13.64 (1.46) | 0.0512 |
| Log 2−delta miRNA 125b | −1.21 (0.85) | −1.20 (0.84) | −1.22 (0.88) | 0.8992 |
| Ct values of cel-39 (internal control; mean ± SD) | 27.35 (1.65) | 27.34 (1.74) | 27.36 (1.55) | 0.9673 |
| Comorbidities | (n = 98) | (n = 56) | (n = 42) | |
| Diabetes mellitus (%) | 10.20 | 8.93 | 11.90 | 0.6300 |
| Hypertension (%) | 17.34 | 8.93 | 28.57 | 0.0110 * |
| (n = 122) | (n = 68) | (n = 54) | ||
| Alcohol use (%) | 16.40 | 16.18 | 16.67 | 0.9421 |
| Univariate Analyses | Multivariate Analyses | |||
|---|---|---|---|---|
| Variable | OR (95%CI) | p Value | OR (95%CI) | p Value |
| Age | 1.17 (1.09–1.25) | <0.0001 * | 1.17 (1.09–1.26) | <0.0001 * |
| Gender (male/female) | 0.89 (0.33–2.37) | 0.8188 | ||
| HBV DNA > 2000 IU/mL | 2.11 (0.67–6.69) | 0.2034 | ||
| HBeAg(+) | 0.41 (0.14–1.17) | 0.0963 | ||
| Lab data | ||||
| WBCs | 1.00 (1.00–1.00) | 0.0156 * | 1.00 (1.00–1.00) | 0.1562 |
| Platelet | 0.98 (0.97–0.99) | <0.0001 * | 0.98 (0.96–0.99) | 0.0032 * |
| AST | 1.00 (1.00–1.00) | 0.7116 | ||
| ALT | 1.00 (1.00–1.00) | 0.0496 * | 1.00 (1.00–1.00) | 0.0241 * |
| Creatinine | 0.87 (0.31–2.45) | 0.7900 | ||
| Bilirubin | 1.08 (0.93–1.25) | 0.3138 | ||
| Albumin (gm/dL) | 0.51 (0.23–1.15) | 0.1058 | ||
| HB (g/dL) | 0.77 (0.58–1.01) | 0.0601 | ||
| Log 2−delta pre−miR−125b | 0.65 (0.40–1.08) | 0.0938 | ||
| Δ Log 2−delta miRNA 125b | 0.65 (0.37–1.13) | 0.1270 | ||
| Comorbidities | ||||
| Diabetes mellitus | 1.37 (0.32–5.76) | 0.6699 | ||
| Hypertension | 1.91 (0.62–5.88) | 0.2596 | ||
| Alcohol use | 0.86 (0.80–0.26) | 0.8019 | ||
| Univariate Analyses | Multivariate Analyses | |||
|---|---|---|---|---|
| Variable | OR (95%CI) | p Value | OR (95%CI) | p Value |
| Age | 1.14 (1.05–1.25) | 0.0033 * | 1.17 (1.04–1.32) | 0.0078 * |
| Gender (male/female) | 1.27 (0.30–5.42) | 0.7442 | ||
| HBV DNA > 2000 IU/mL | 1.76 (0.33–9.32) | 0.5036 | ||
| HBeAg(+) | 0.19 (0.02–1.65) | 0.1332 | ||
| Lab data | ||||
| WBCs | 1.00 (1.00–1.00) | 0.2872 | ||
| Platelet | 0.98 (0.97–0.99) | 0.0109 * | 0.99 (0.98–1.00) | 0.1522 |
| AST | 1.00 (1.00–1.00) | 0.6767 | ||
| ALT | 1.00 (1.00–1.00) | 0.2354 | ||
| Creatinine | 0.89 (0.32–2.44) | 0.8213 | ||
| Bilirubin | 1.06 (0.90–0.12) | 0.4909 | ||
| Albumin (gm/dL) | 0.42 (0.13–1.31) | 0.1362 | ||
| HB (g/dL) | 0.66 (0.42–1.03) | 0.0718 | ||
| Log 2−delta pre−miR−125b | 0.52 (0.25–1.06) | 0.0727 | ||
| Δ Log 2−delta miRNA 125b | 0.34 (0.13–0.88) | 0.0268 * | 0.22 (0.06–0.75) | 0.0157 * |
| Comorbidities | ||||
| Diabetes mellitus | 1.38 (0.30–6.36) | 0.6756 | ||
| Hypertension | 2.00 (0.48–8.30) | 0.3400 | ||
| Alcohol use | 1.27 (0.33–4.95) | 0.7314 | ||
| Univariate Analyses | Multivariate Analyses | |||
|---|---|---|---|---|
| Variable | OR (95%CI) | p Value | OR (95%CI) | p Value |
| Age | 1.18 (1.06–1.32) | 0.0030 * | 1.22 (1.06–1.41) | 0.0068 * |
| Gender (male/female) | 0.22 (0.04–1.05) | 0.0579 | ||
| HBV DNA > 2000 IU/mL | 1.22 (0.22–6.84) | 0.8222 | ||
| HBeAg(+) | 0.82 (0.17–3.86) | 0.8030 | ||
| Lab data | ||||
| WBCs | 1.00 (1.00–1.00) | 0.0503 | ||
| Platelet | 0.97 (0.95–0.99) | 0.0094* | 0.95 (0.90–1.00) | 0.0314 * |
| AST | 1.00 (1.00–1.00) | 0.9120 | ||
| ALT | 1.00 (1.00–1.00) | 0.1204 | ||
| Creatinine | 0.59 (0.03–13.72) | 0.7413 | ||
| Bilirubin | 1.17 (0.82–0.12) | 0.3856 | ||
| Albumin (gm/dL) | 0.48 (0.12–1.93) | 0.3026 | ||
| HB (g/dL) | 0.74 (0.46–1.19) | 0.2139 | ||
| Log 2−delta pre-miR-125b | 0.82 (0.34–1.97) | 0.6508 | ||
| Δ Log 2−delta miRNA 125b | 1.10 (0.45–2.71) | 0.8338 | ||
| Comorbidities | ||||
| Diabetes mellitus | 1.10 (0.30–6.36) | 0.9945 | ||
| Hypertension | 0.90 (0.08–9.97) | 0.9316 | ||
| Alcohol use | 1.50 (0.33–4.95) | 0.9980 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, J.-Y.; Tsai, Y.-S.; Li, C.-C.; Yeh, M.-L.; Huang, C.-I.; Huang, C.-F.; Hsu, J.-N.; Hsieh, M.-H.; Chen, Y.-C.; Liu, T.-W.; et al. Baseline Circulating miR-125b Levels Predict a High FIB-4 Index Score in Chronic Hepatitis B Patients after Nucleos(t)ide Analog Treatment. Biomedicines 2022, 10, 2824. https://doi.org/10.3390/biomedicines10112824
Wu J-Y, Tsai Y-S, Li C-C, Yeh M-L, Huang C-I, Huang C-F, Hsu J-N, Hsieh M-H, Chen Y-C, Liu T-W, et al. Baseline Circulating miR-125b Levels Predict a High FIB-4 Index Score in Chronic Hepatitis B Patients after Nucleos(t)ide Analog Treatment. Biomedicines. 2022; 10(11):2824. https://doi.org/10.3390/biomedicines10112824
Chicago/Turabian StyleWu, Jyun-Yi, Yi-Shan Tsai, Chia-Chen Li, Ming-Lun Yeh, Ching-I Huang, Chung-Feng Huang, Jia-Ning Hsu, Meng-Hsuan Hsieh, Yo-Chia Chen, Ta-Wei Liu, and et al. 2022. "Baseline Circulating miR-125b Levels Predict a High FIB-4 Index Score in Chronic Hepatitis B Patients after Nucleos(t)ide Analog Treatment" Biomedicines 10, no. 11: 2824. https://doi.org/10.3390/biomedicines10112824
APA StyleWu, J. -Y., Tsai, Y. -S., Li, C. -C., Yeh, M. -L., Huang, C. -I., Huang, C. -F., Hsu, J. -N., Hsieh, M. -H., Chen, Y. -C., Liu, T. -W., Lin, Y. -H., Liang, P. -C., Lin, Z. -Y., Chuang, W. -L., Yu, M. -L., & Dai, C. -Y. (2022). Baseline Circulating miR-125b Levels Predict a High FIB-4 Index Score in Chronic Hepatitis B Patients after Nucleos(t)ide Analog Treatment. Biomedicines, 10(11), 2824. https://doi.org/10.3390/biomedicines10112824