
High Arterial Lactate Levels after Hepatic Resection Are Associated with Low Oxygen Delivery and Predict Severe Postoperative Complications

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Anesthetic Management
2.3. Surgical Procedure
2.4. Collected Variables and Definitions
2.5. Study Outcomes
2.6. Statistical Analysis
3. Results
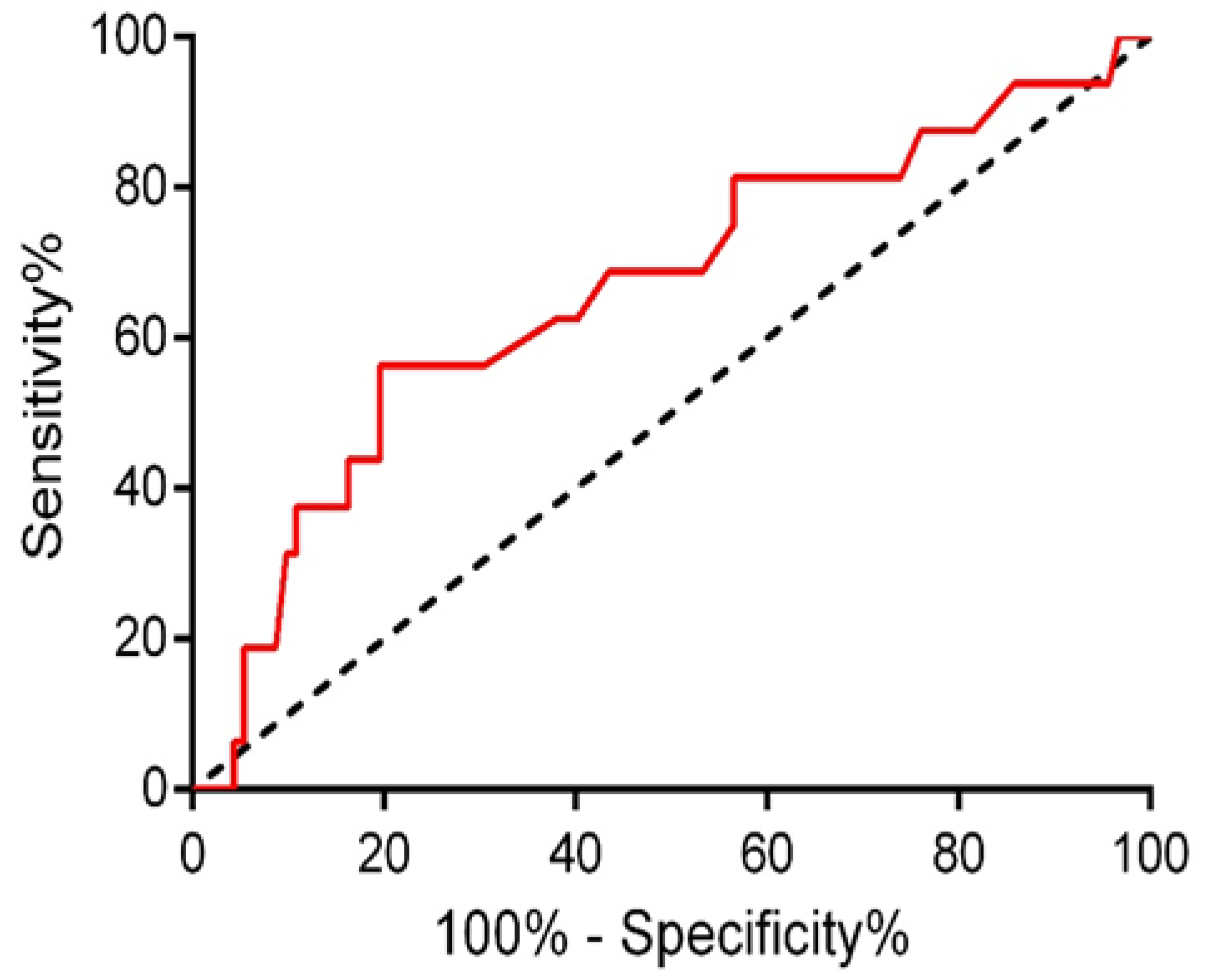
3.1. Lactate Concentration and Risk of Complications
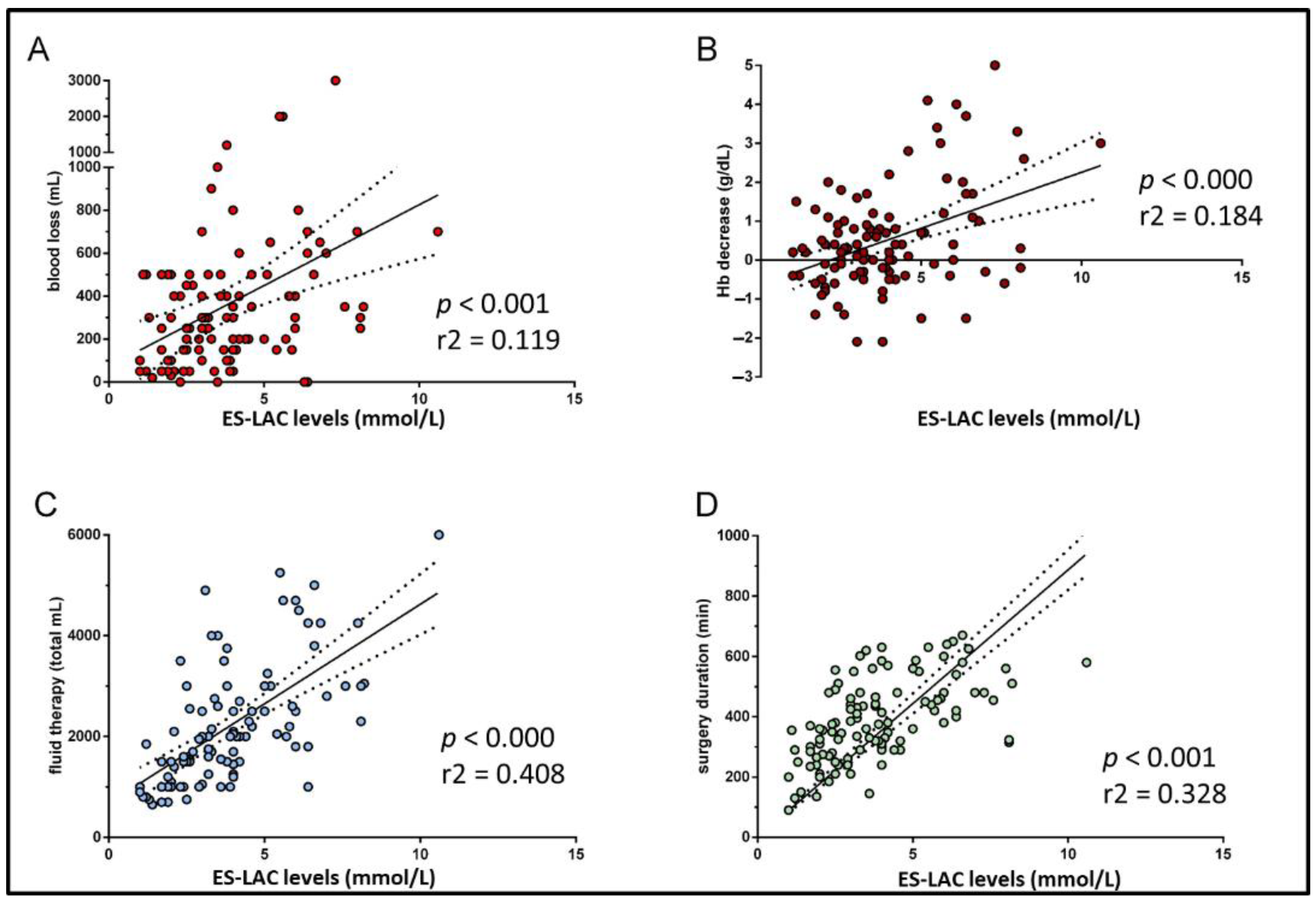
3.2. Clinical Characteristics and Laboratory Parameters Associated with High End-Surgery Arterial Lactate Concentration
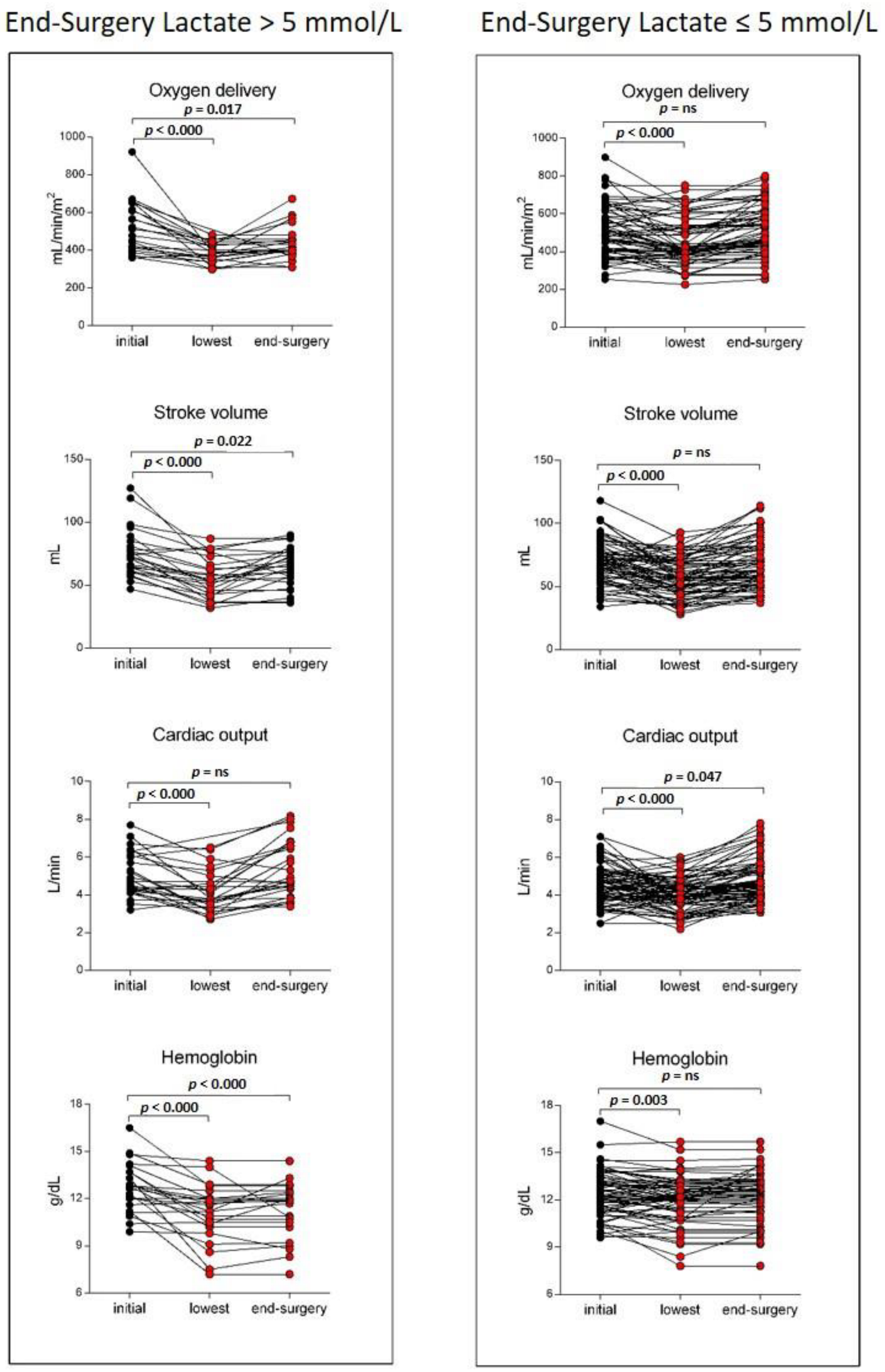
3.3. Determinants for the DO2 Decrease in Patients with High End-Surgery Arterial Lactate Concentration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seheult, J.; Fitzpatrick, G.; Boran, G. Lactic acidosis: An update. Clin. Chem. Lab. Med. 2017, 55, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, I.; Mayumi, T.; Arishima, T.; Takahashi, H.; Shikano, T.; Nakao, A.; Nagino, M.; Nimura, Y.; Takezawa, J. Hyperlactemia can predict the prognosis of liver resection. Shock 2007, 28, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Wiggans, M.G.; Starkie, T.; Shahtahmassebi, G.; Woolley, T.; Birt, D.; Erasmus, P.; Anderson, I.; Bowles, M.J.; Aroori, S.; Stell, D.A. Serum Arterial Lactate Concentration Predicts Mortality and Organ Dysfunction Following Liver Resection. Perioper. Med. 2013, 2, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vibert, E.; Boleslawski, E.; Cosse, C.; Adam, R.; Castaing, D.; Cherqui, D.; Naili, S.; Régimbeau, J.M.; Cunha, A.S.; Truant, S.; et al. Arterial lactate concentration at the end of an elective hepatectomy is an early predictor of the postoperative course and a potential surrogate of intraoperative events. Ann. Surg. 2015, 262, 787–793. [Google Scholar] [CrossRef]
- Meguro, M.; Mizuguchi, T.; Kawamoto, M.; Nishidate, T.; Ishii, M.; Tatsumi, H.; Kimura, Y.; Furuhata, T.; Hirata, K. Highest intraoperative lactate level could predict postoperative infectious complications after hepatectomy, reflecting the Pringle maneuver especially in chronic liver disease. J. Hepatobiliary Pancreat. Sci. 2014, 21, 489–498. [Google Scholar] [CrossRef]
- Lemke, M.; Karanicolas, P.J.; Habashi, R.; Behman, R.; Coburn, N.G.; Hanna, S.S.; Law, C.H.; Hallet, J. Elevated Lactate is Independently Associated with Adverse Outcomes Following Hepatectomy. World J. Surg. 2017, 41, 3180–3188. [Google Scholar] [CrossRef]
- Connolly, C.; Stättner, S.; Niederwieser, T.; Primavesi, F. Systematic review on peri-operative lactate measurements to predict outcomes in patients undergoing liver resection. J Hepatobiliary Pancreat. Sci. 2020, 27, 359–370. [Google Scholar] [CrossRef] [Green Version]
- Niederwieser, T.; Braunwarth, E.; Dasari, B.V.M.; Pufal, K.; Szatmary, P.; Hackl, H.; Haselmann, C.; Connolly, C.; Cardini, B.; Öfner, D.; et al. Early postoperative arterial lactate concentrations to stratify risk of post-hepatectomy liver failure. Br. J. Surg. 2021, 108, 1360–1370. [Google Scholar] [CrossRef]
- Giustiniano, E.; Nisi, F.; Rocchi, L.; Zito, P.C.; Ruggieri, N.; Cimino, M.; Torzilli, G.; Cecconi, M. Perioperative management of complex hepatectomy for colorectal liver metastases: The alliance between the surgeon and the anesthetist. Cancers 2021, 13, 2203. [Google Scholar] [CrossRef]
- Nuzzo, G.; Giuliante, F.; Vellone, M.; De Cosmo, G.; Ardito, F.; Murazio, M.; D’Acapito, F.; Giovannini, I. Pedicle clamping with ischemic preconditioning in liver resection. Liver Transpl. 2004, 10 (Suppl. 1), S53–S57. [Google Scholar] [CrossRef]
- Smyrniotis, V.; Farantos, C.; Kostopanagiotou, G.; Arkadopoulos, N. Vascular Control during Hepatectomy: Review of Methods and Results. World J. Surg. 2005, 29, 1384–1396. [Google Scholar] [CrossRef] [PubMed]
- Pietsch, U.C.; Herrmann, M.L.; Uhlmann, D.; Busch, T.; Hokema, F.; Kaisers, U.X.; Schaffranietz, L. Blood lactate and pyruvate levels in the perioperative period of liver resection with pringle maneuver. Clin. Hemorheol. Microcirc. 2010, 44, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Riediger, C.; Mueller, M.W.; Hapfelmeier, A.; Bachmann, J.; Friess, H.; Kleeff, J. Preoperative Serum Bilirubin and Lactate Levels Predict Postoperative Morbidity and Mortality in Liver Surgery: A Single-Center Evaluation. Scand. J. Surg. 2015, 104, 176–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Merchant, N.B.; Didolkar, M.S. Hepatic Resection Using Intermittent Vascular Inflow Occlusion and Low Central Venous Pressure Anesthesia Improves Morbidity and Mortality. J. Gastrointest. Surg. 2000, 4, s1091–s1255. [Google Scholar] [CrossRef]
- Jones, R.M.; Moulton, C.E.; Hardy, K.J. Central venous pressure and its effect on blood loss during liver resection. Br. J. Surg. 1998, 85, 1058–1060. [Google Scholar] [CrossRef]
- Cannesson, M.; Musard, H.; Desebbe, O.; Boucau, C.; Simon, R.; Hénaine, R.; Lehot, J.-J. The ability of stroke volume variations obtained with vigileo/flotrac system to monitor fluid responsiveness in mechanically ventilated patients. Anesth. Analg. 2009, 108, 513–517. [Google Scholar] [CrossRef]
- Lahner, D.; Kabon, B.; Marschalek, C.; Chiari, A.; Pestel, G.; Kaider, A.; Fleischmann, E.; Hetz, H. Evaluation of stroke volume variation obtained by arterial pulse contour analysis to predict fluid responsiveness intraoperatively. Br. J. Anaesth. 2009, 103, 346–351. [Google Scholar] [CrossRef] [Green Version]
- Benes, J.; Chytra, I.; Altmann, P.; Hluchy, M.; Kasal, E.; Svitak, R.; Pradl, R.; Stepan, M. Intraoperative fluid optimization using stroke volume variation in high risk surgical patients: Results of prospective randomized study. Crit. Care 2010, 14, R118. [Google Scholar] [CrossRef] [Green Version]
- Le Manach, Y.; Hofer, C.K.; Lehot, J.J.; Vallet, B.; Goarin, J.P.; Tavernier, B.; Cannesson, M. Can changes in arterial pressure be used to detect changes in cardiac output during volume expansion in the perioperative period? Anesthesiology 2012, 117, 1165–1174. [Google Scholar] [CrossRef] [Green Version]
- Dunki-Jacobs, E.M.; Philips, P.; Scoggins, C.R.; McMasters, K.M.; Martin, R.C.G. Stroke volume variation in hepatic resection: A replacement for standard central venous pressure monitoring. Ann. Surg. Oncol. 2014, 21, 473–478. [Google Scholar] [CrossRef]
- Correa-Gallego, C.; Tan, K.S.; Arslan-Carlon, V.; Gonen, M.; Denis, S.C.; Langdon-Embry, L.; Grant, F.; Kingham, P.T.; DeMatteo, R.P.; Allen, P.J.; et al. Goal-Directed Fluid Therapy Using Stroke Volume Variation for Resuscitation after Low Central Venous Pressure-Assisted Liver Resection: A Randomized Clinical Trial. J. Am. Coll. Surg. 2015, 221, 591–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strasberg, S.M.; Belghiti, J.; Clavien, P.A. Terminology committee of the IHPBA. Terminology of liver anatomy and resections. HPB Surg. 2000, 2, 333–339. [Google Scholar] [CrossRef]
- Giuliante, F.; Nuzzo, G.; Ardito, F.; Vellone, M.; De Cosmo, G.; Giovannini, I. Extraparenchymal Control of Hepatic Veins During Mesohepatectomy. J. Am. Coll. Surg. 2008, 206, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Giuliante, F.; Ardito, F.; Vellone, M.; Ranucci, G.; Federico, B.; Giovannini, I.; Nuzzo, G. Role of the surgeon as a variable in long-term survival after liver resection for colorectal metastases. J. Surg. Oncol. 2009, 100, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Ardito, F.; Vellone, M.; Barbaro, B.; Grande, G.; Clemente, G.; Giovannini, I.; Federico, B.; Bonomo, L.; Nuzzo, G.; Giuliante, F. Right and extended-right hepatectomies for unilobar colorectal metastases: Impact of portal vein embolization on long-term outcome and liver recurrence. Surgery 2013, 153, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Giuliante, F.; Ardito, F. Minimally invasive liver surgery in a hepato-biliary unit: Learning curve and indications. Updates Surg. 2015, 67, 201–206. [Google Scholar] [CrossRef]
- Kehlet, H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br. J. Anaesth. 1997, 78, 606–617. [Google Scholar] [CrossRef]
- Ardito, F.; Lai, Q.; Rinninella, E.; Mimmo, A.; Vellone, M.; Panettieri, E.; Adducci, E.; Cintoni, M.; Mele, M.C.; Gasbarrini, A.; et al. The impact of personalized nutritional support on postoperative outcome within the enhanced recovery after surgery (ERAS) program for liver resections: Results from the NutriCatt protocol. Updates Surg. 2020, 72, 681–691. [Google Scholar] [CrossRef]
- ASA Physical Status Classification System. Available online: https://www.asahq.org/standards-and-guidelines/asa-physical-status-classification-system (accessed on 20 March 2022).
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Avolio, A.W.; Agnes, S.; Barbarino, R.; Magalini, S.C.; Frongillo, F.; Pagano, L.; Larocca, L.; Pompili, M.; Caira, M.; Sollazzi, L.; et al. Posttransplant lymphoproliferative disorders after liver transplantation: Analysis of early and late cases in a 255 patient series. Transpl. Proc. 2007, 39, 1956–1960. [Google Scholar] [CrossRef]
- Avolio, A.W.; Agnes, S.; Pelosi, G.; Sollazzi, L.; Magalini, S.C.; Gozzo, M.L.; Castagneto, M. Intraoperative trends of oxygen consumption and blood lactate as predictors of primary dysfunction after liver transplantation. Transpl. Proc. 1991, 23, 2263–2265. [Google Scholar]
- Avolio, A.W.; Agnes, S.; Chirico, A.S.; Castagneto, M. Primary dysfunction after liver transplantation: Donor or recipient fault? Transpl. Proc. 1999, 31, 434–436. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients | n = 108 |
|---|---|
| Age, years, median (IQR) | 62.0 (55.0–69.0) |
| Sex, male, No. (%) | 62 (57.4) |
| BMI, kg/m2, median (IQR) | 25.1 (22.1–28.1) |
| ASA classification, No. (%) | |
| 1 | 3 (2.7) |
| 2 | 88 (81.6) |
| 3 | 17 (15.7) |
| Comorbidities, No. (%) | |
| Diabetes mellitus | 9 (8.3) |
| Hypertension | 54 (50) |
| Coronary artery disease | 8 (7.4) |
| COPD | 9 (8.3) |
| Indication for liver resection, No. (%) | |
| Liver metastasis | 69 (63.9) |
| Hepatocellular carcinoma | 21 (19.4) |
| Cholangiocellular carcinoma | 5 (4.6) |
| Gallbladder cancer | 4 (3.7) |
| Benign disease | 3 (2.8) |
| Intra-hepatic stones | 6 (5.6) |
| Underlying liver disease, No. (%) | |
| Cirrhosis | 9 (8.3) |
| Fibrosis moderate/severe | 19 (17.6) |
| Macrovescicular steatosis >25% | 10 (9.3) |
| Surgery, No. (%) | |
| Laparotomy/Laparoscopy | 94 (87.0)/14 (13.0) |
| Major liver resection | 3.2 (29.6) |
| Minor resection | 57 (52.8) |
| Minor complex resection | 19 (17.6) |
| Overall ischemia time, min, median (IQR) | 57 (28–85) |
| Duration of surgery, min, median (IQR) | 375 (290–480) |
| Postoperative outcome | |
| Length of postoperative stay, days, median (IQR) | 7 (6–11) |
| Clavien–Dindo complications (grade ≥ 3), No. (%) | 16 (14.8) |
| 90-Day postoperative mortality, No. (%) | 1 (0.9) |
| Fluids and transfusions | |
| Fluid administration, mL/kg/h, median (IQR) | 3.9 (3.2–4.8) |
| Total intraoperative fluids, mL, median (IQR) | 2000 (1325–2775) |
| Intraoperative blood loss, mL, median (IQR) | 300 (150–500) |
| RBC transfused patients, No. (%) | 10 (9.3) |
| Intraoperative diuresis, mL/h, median (IQR) | 103 (79–131) |
| Hemodynamic parameters, median (IQR) | |
| Initial arterial lactate, mmol/L | 1.1 (1.0–1.6) |
| End-surgery arterial lactate, mmol/L | 3.6 (2.4–5.1) |
| Initial BE, mmol/L | 4.0 (2.9–5.6) |
| End-surgery BE, mmol/L | 0.8 (−1.1–2.5) |
| Initial pH | 7.49 (7.45–7.52) |
| End-surgery pH | 7.40 (7.36–7.45) |
| Initial blood glucose, mg/dL | 93 (86–106) |
| End-surgery blood glucose, mg/dL | 177 (151–217) |
| Initial Hb, g/dL | 12.6 (11.5–13.4) |
| Lowest Hb, g/dL | 12.0 (10.9–12.9) |
| End-surgery Hb, g/dL | 12.3 (10.9–13.1) |
| Initial heart rate, btm | 65 (59–77) |
| End-surgery heart rate, btm | 76 (67–85) |
| Initial MAP, mmHg | 86 (76–97) |
| Lowest MAP, mmHg | 70 (62–78) |
| End-surgery MAP, mmHg | 77 (69–83) |
| Initial SVV, % | 10.0 (7.8–12.0) |
| Highest SVV, % | 17.0 (13.0–19.0) |
| End-surgery SVV, % | 12.0 (10.0–15.0) |
| Initial CO, L/min | 4.5 (3.9–5.2) |
| Lowest CO, L/min | 3.9 (3.5–4.5) |
| End-surgery CO, L/min | 4.6 (3.9–5.7) |
| Initial DO2, mL/min/m2 | 487 (409–614) |
| Lowest DO2, mL/min/m2 | 413 (361–497) |
| End-surgery DO2, mL/min/m2 | 458 (400–585) |
| Noradrenaline administration, No. (%) | 63 (58.3) |
| >5 mmol/L n = 27 | ≤5 mmol/L n = 81 | p-Value | |
|---|---|---|---|
| Age, years, median (IQR) | 61.0 (57.0–65.0) | 63.0 (54.0–70.5) | 0.563 |
| Sex, male, No. (%) | 17 (63.0) | 45 (55.6) | 0.654 |
| BMI, kg/m2, median (IQR) | 26.9 (24.1–30.8) | 24.6 (21.8–27.8) | 0.032 |
| ASA classification, No. (%) | |||
| 1 2 3 | 0 25 (92.6) 2 (7.4) | 3 (3.7) 63 (77.8) 15 (18.5) | 0.419 |
| Comorbidities, No. (%) | |||
| Diabetes mellitus Hypertension Coronary artery disease COPD | 2 (7.4) 19 (70.4) 0 2 (7.4) | 7 (8.6) 35 (43.2) 8 (9.9) 7 (8.6) | 1.000 0.025 0.197 1.000 |
| Indication for liver resection, No. (%) | |||
| Liver metastasis Hepatocellular carcinoma Cholangiocellular carcinoma Gallbladder cancer Benign disease Intra-hepatic stones | 51 (63.0) 16 (19.8) 4 (4.9) 2 (2.5) 3 (3.7) 5 (6.2) | 18 (66.7) 15 (18.5) 1 (3.7) 2 (7.4) 0 1 (3.7) | 0.728 |
| Underlying liver disease, No. (%) | |||
| Cirrhosis Macrovescicular steatosis >25% | 1 (3.7) 3 (11.1) | 8 (9.9) 7 (8.6) | 0.445 0.708 |
| Surgery, No. (%) | |||
| Laparotomy/Laparoscopy | 26 (96.3)/1(3.7) | 68 (84.0)/13(16.0) | 0.182 |
| Major resection Minor resection Minor complex resection | 9 (33.3) 6 (22.2) 12 (44.4) | 23 (28.4) 51 (63.0) 7 (8.6) | 0.020 |
| RBC postoperative transfused patients, No. (%) | 7 (25.9) | 3 (3.7) | 0.002 |
| Overall ischemia time, min, median (IQR) | 83 (66–139) | 57 (35–82) | 0.001 |
| Duration of surgery, min, median (IQR) | 480 (440–587) | 330 (267–432) | <0.001 |
| Length of stay, days, median (IQR) | 12 (7–17) | 7 (5–9) | 0.001 |
| RBC transfused patients, No. (%) | 8 (29.6) | 9 (11.1) | 0.032 |
| Clavien–Dindo grade ≥3, No. (%) | 9 (33.3) | 7 (8.6) | 0.004 |
| 90-day postoperative mortality, No. (%) | 0 | 1 (0.9) | 1.000 |
| >5 mmol/L n = 27 | ≤5 mmol/L n = 81 | p-Value | |
|---|---|---|---|
| Hemodynamic parameters, median (IQR) | |||
| Initial arterial lactate, mmol/L | 1.2 (1.1–2.0) | 1.1(1.0–1.4) | 0.039 |
| End-surgery lactate level, mmol/L | 6.4 (5.8–7.3) | 3.0 (2.1–3.9) | <0.001 |
| Initial BE, mmol/L | 4.4 (3.6–5.5) | 3.8 (2.9–5.7) | 0.270 |
| End-surgery BE, mmol/L | −1.0 (−4.2–0.6) | 1.5 (−0.7–2.8) | <0.001 |
| Initial pH | 7.48 (7.42–7.51) | 7.49 (7.45–7.52) | 0.614 |
| End-surgery pH | 7.37 (7.35–7.40) | 7.41 (7.38–7.45) | <0.001 |
| Initial blood glucose, mg/dL | 95.0 (86.0–111.0) | 93.0 (85.5–104.0) | 0.408 |
| End-surgery blood glucose, mg/dL | 200.0 (152.0–256.0) | 170.0 (151.0–209.0) | 0.130 |
| Total intraoperative fluids, mL | 3000 (2250–4375) | 1575 (1100–2275) | 0.001 |
| Fluid administration, mL/kg/h | 4.3 (3.8–5.3) | 3.6 (3.0–4.8) | 0.024 |
| Intraoperative blood loss, mL | 500 (250–500) | 200 (100–400) | <0.001 |
| Initial Hb, g/dL | 12.8 (11.9–13.7) | 12.4 (11.4–13.4) | 0.458 |
| Lowest Hb, g/dL | 11.2 (10.2–12.0) | 12.1 (11.2–13.0) | 0.002 |
| End-surgery Hb, g/dL | 11.8 (10.0–12.4) | 12.6 (11.4–13.2) | 0.003 |
| Initial heart rate, btm | 67 (61–77) | 65 (59–76) | 0.575 |
| End-surgery heart rate, btm | 82 (76–90) | 74 (64–83) | 0.010 |
| Initial MAP, mmHg | 87 (76–105) | 86 (76–95) | 0.202 |
| Lowest MAP, mmHg | 66 (60–76) | 71 (64–80) | 0.142 |
| End-surgery MAP, mmHg | 75 (69–81) | 77 (68–86) | 0.421 |
| Initial SVV, % | 10 (7–12) | 11 (8–12) | 0.355 |
| Highest SVV, % | 18 (14–20) | 16 (12–19) | 0.184 |
| End-surgery SVV, % | 14 (11–16) | 12 (10–15) | 0.214 |
| Initial SV, mL | 72 (61–83) | 70 (56–77) | 0.286 |
| Lowest SV, mL | 53 (42–64) | 55 (44–68) | 0.592 |
| End-surgery SV, mL | 65 (54–76) | 64 (52–82) | 0.633 |
| Initial CO, L/min | 4.7 (4.2–6.1) | 4.4 (3.8–5.1) | 0.064 |
| Lowest CO, L/min | 3.8 (3.3–5.0) | 3.9 (3.5–4.5) | 0.951 |
| End-surgery CO, L/min | 4.7 (4.3–6.6) | 4.4 (3.8–5.3) | 0.064 |
| Initial DO2, mL/min/m2 | 494 (409–624) | 487 (407–599) | 0.762 |
| Lowest DO2, mL/min/m2 | 383 (338–432) | 417 (375–532) | 0.014 |
| End-surgery DO2, mL/min/m2 | 410 (387–464) | 488 (418–608) | 0.008 |
| Noradrenaline administration No. (%) | 17 (63%) | 28 (34.6%) | 0.013 |
| >5 mmol/L n = 27 | ≤5 mmol/L n = 81 | p-Value | |
|---|---|---|---|
| Clavien–Dindo complications grade, No. (%) | |||
| Grade I Type of complications, No. | 1 (3.7) Increase in serum creatinine (1) | 1 (1.2) Pleural effusion (1) | 0.439 |
| Grade II Type of complications, No. | 9 (33.3) bile leak (1), anemia (7), coagulopathy (1), fever (3), abdominal collection (2), lymphatic fistula (1), pleural effusion (2), mild liver failure (2) | 17 (21.0) bile leak (7), anemia (2) fever (6), abdominal collection (3), lymphatic fistula (1), pleural effusion (2), bowel obstruction (1), mild liver failure (1) | 0.203 |
| Grade IIIa Type of complications, No. | 7 (25.9) pleural effusion (1) abdominal collection (4), bile leak (2), sepsis (1), liver failure (1), nefrostomy (1) | 3 (3.7) pleural effusion (1), abdominal collection (2), bile leak (1), ascites (1) | 0.002 |
| Grade IIIb Type of complications, No. | 1 (3.7) abdominal collection (1), pleural effusion (1) | 1 (1.2) abdominal collection (1) | 0.439 |
| Grade IVa Type of complications, No. | 1 (3.7) dialysis (1) | 2 (2.5) respiratory failure (1) gastric ulcer hemorrhage (1) | 1.000 |
| Grade IVb | 0 | 0 | |
| Grade V Type of complications, No. | 0 | 1 (1.2) Liver failure (1) | |
| Pts with complications grade III-V | 9/27 (33.3) | 7/81 (8.6) | 0.004 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| OR [95% CI] | p-Value | OR [95% CI] | p-Value | |
| Age | 0.99 (0.95–1.03) | 0.621 | ||
| BMI | 1.03 (1.00–1.06) | 0.510 | ||
| Hypertension | 3.12 (1.23–7.96) | 0.017 | ||
| Overall ischemia time | 1.02 (1.01–1.03) | 0.001 | ||
| Duration of surgery | 1.01 (1.01–1.02) | <0.001 | 1.011 [1.005–1.018] | 0.001 |
| Noradrenaline administration | 3.22 (1.30–7.96) | 0.011 | ||
| RBC transfused patients | 9.10 (2.16–36.37) | 0.003 | ||
| Initial arterial lactate | 2.42 (1.11–5.26) | 0.026 | ||
| End-surgery BE | 0.61 (0.48–0.76) | <0.001 | ||
| Blood loss | 1.00 (1.00–1.00) | 0.004 | ||
| Total fluid administration | 1.00 (1.00–1.00) | <0.001 | ||
| Lowest Hb | 0.83 (0.66–1.05) | 0.126 | ||
| End-surgery Hb | 0.67 (0.51–0.88) | 0.004 | ||
| Lowest DO2 | 0.99 (0.99–0.99) | 0.011 | 0.989 [0.979–0.999] | 0.028 |
| End-surgery DO2 | 0.99 (0.99–1.00) | 0.206 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaspari, R.; Teofili, L.; Ardito, F.; Adducci, E.; Vellone, M.; Mele, C.; Orlando, N.; Iacobucci, T.; Antonelli, M.; Giuliante, F. High Arterial Lactate Levels after Hepatic Resection Are Associated with Low Oxygen Delivery and Predict Severe Postoperative Complications. Biomedicines 2022, 10, 1108. https://doi.org/10.3390/biomedicines10051108
Gaspari R, Teofili L, Ardito F, Adducci E, Vellone M, Mele C, Orlando N, Iacobucci T, Antonelli M, Giuliante F. High Arterial Lactate Levels after Hepatic Resection Are Associated with Low Oxygen Delivery and Predict Severe Postoperative Complications. Biomedicines. 2022; 10(5):1108. https://doi.org/10.3390/biomedicines10051108
Chicago/Turabian StyleGaspari, Rita, Luciana Teofili, Francesco Ardito, Enrica Adducci, Maria Vellone, Caterina Mele, Nicoletta Orlando, Tiziana Iacobucci, Massimo Antonelli, and Felice Giuliante. 2022. "High Arterial Lactate Levels after Hepatic Resection Are Associated with Low Oxygen Delivery and Predict Severe Postoperative Complications" Biomedicines 10, no. 5: 1108. https://doi.org/10.3390/biomedicines10051108
APA StyleGaspari, R., Teofili, L., Ardito, F., Adducci, E., Vellone, M., Mele, C., Orlando, N., Iacobucci, T., Antonelli, M., & Giuliante, F. (2022). High Arterial Lactate Levels after Hepatic Resection Are Associated with Low Oxygen Delivery and Predict Severe Postoperative Complications. Biomedicines, 10(5), 1108. https://doi.org/10.3390/biomedicines10051108