1. Introduction
The routine management of localized renal cell cancer (RCC) is radical or partial nephrectomy [
1]. However, it should be emphasized that approximately 20–40% of cases become metastatic during the course of the disease, even given successful initial treatment [
2]. Therefore, determining the key factors that affect postsurgical prognosis would allow early risk-stratification.
Oncological outcomes are routinely estimated based on the TNM classification and pathological features of a tumor [
3]. According to the American Urological Association, the establishment of a prognosis should rely on TNM staging, while localized disease is connected with nearly 90% of cancer-specific survival [
4]. On the other hand, there is a strong recommendation from the European Urological Association (EAU) to focus on more sophisticated tools along with a statement that new models should be compared to already existing tools prior to their introduction into the clinic [
5,
6]. Although it is obviously included in all the models, TNM staging proved to have restricted accuracy if selected as a single prognostic factor [
2]. Additional information has been routinely gathered from pathological examination, i.e., grading or presence of tumor necrosis or sarcomatoid features [
2].
Among other clinical parameters, a prognosis is often assessed using gender [
7] or age [
8]. It is thought that male patients may present with worse prognoses, similar to elderly people [
7,
8]. Interestingly, the observation that comorbidities may have even greater significance is often connected with the fact that urological cancers are diagnosed frequently in the geriatric population [
3]. Consequently, despite curative surgery, other causes of mortality in RCC cases may be of crucial importance.
Among several others, three models have been validated in the literature on localized RCC, i.e., VENUSS (VEnous extension, NUclear grade, Size, Stage) [
9], GRANT (GRade, Age, Nodes and Tumor) [
10] and Leibovich (tumor stage, regional lymph node status, tumor size, nuclear grade and histologic tumor necrosis) [
11]. Although their prognostic accuracies have already been documented, they are not commonly implemented in everyday practice. Furthermore, the EAU does not place one particular tool above the others and leaves the choice up to the clinician.
One can observe a recent growing interest in the novel inflammatory markers that can be easily obtained from preoperative complete blood counts and incorporated into clinical models for prognostic purposes [
12]. Recently, we compared the accuracy of different inflammatory markers in the prognostic assessment of RCC and proved that these clinical parameters may enrich existing models [
13]. However, the common clinicopathological features remained the pillars of risk stratification, as described by other authors [
14].
The aim of the present study was to determine the relevance of comorbidities and selected inflammatory markers to the survival of patients with localized RCC treated by partial and radical nephrectomy in the search for a prognostic model. Here, we focused on a cohort of clear cell RCC patients as a predominant subtype, taking into consideration that the majority of clinical trials enroll these particular patients. The identification of the most efficient model seems to be of greatest importance in terms of both recruiting for future clinical trials and identifying the optimal candidates for adjuvant therapy.
4. Discussion
In the current paper, we revisited the idea of using prognostic models in ccRCC with the incorporation of easily obtainable clinical factors that increase the prognostic properties to be used in a localized setting. Thus, the predictive value of tumor stage, size and grade was exploited, with the inclusion of CCI and novel hematological biomarkers, i.e., either SIRI or SII, depending on the end-point assessed. These features were incorporated into four-feature models, predicting either OS or CSS in localized ccRCC with increased accuracy when compared with three well-recognized models used in non-metastatic disease.
The constant search for an optimal tool to determine the scheme of follow-up after radical treatment, taking into consideration the risk of recurrence and survival, is just one perspective. The schedule includes risk, timing and the site of recurrence, which, in turn, imposes close monitoring in high-risk disease [
9]. In the light of growing evidence on the efficacy of adjuvant treatment, the personalization of therapy using models for localized disease is the other side of the coin [
10]. Clinical tools to assess patients may be even more sought after in order to determine possible high-risk candidates for future adjuvant treatment, e.g., in the paper by Choueiri et al. summarizing the results of the KEYNOTE-564 trial, adjuvant immunotherapy resulted in a remarkable increase in disease-free survival in high-risk patients [
17].
There is no consensus established regarding the optimal risk stratification policy in localized RCC, although a variety of prognostic models are available [
9,
10,
11,
14,
18,
19]. While awaiting results of clinical trials on the role of perioperative systemic therapy, the appropriate selection of candidates may be vital. Taking into consideration the side effects and costs of this approach, validation and application of the risk-based hierarchy will be necessary to optimize and simplify inclusion criteria [
18].
The question that arises is as follows: what is the true value of additional features that are included in the already established prognostic models in the light of ‘overfitting’ phenomenon during model creation? Only after providing the answer can one justify their everyday clinical application [
20]. Furthermore, none of the existing models is routinely recommended based on its approved accuracy [
14,
19]. As a consequence, there is a need for balance between predictive accuracy and simplicity in practice: incorporating additional features may not result in better prognostic value, while it may make the tool too complicated.
Although it is obviously included in all the models, TNM staging proved to have limited accuracy if selected as a single prognostic factor [
2]. Additional information has been routinely gathered from pathological examination, i.e., grading or presence of tumor necrosis or sarcomatoid features [
2]. Here, we introduced a novel prognostic model developed in the contemporary ccRCC cohort with a stress on both overall and cancer-specific survival using easily approachable features. Firstly, we established significant predictors for CSS in multivariate analysis to be used in a future model. Apart from tumor stage, grade and size, we observed statistical significance for a single hematological marker, i.e., SII. On the other hand, in the multivariate analysis of OS we determined that next to tumor grade and size CCI and SIRI were significant predictors of survival. Berger et al. pinpointed that coexisting chronic diseases remain significant prognostic factors for overall survival after nephrectomy [
21]. Collecting the relevant information and translating it into a validated score may increase the efficacy of perioperative evaluation of the candidates for surgery, as discussed by Charlson et al. [
16]. It seems reasonable then to opt for the incorporation of the Charlson Comorbidity Index into the prognostic tools in the hope of achieving more personalized approaches [
22]. We determined that CCI (>4 vs. ≤4) was a significant predictor in both univariate and multivariate analyses of OS but not CSS. Although a detailed description of patient comorbidities is a routine preoperative work-up to establish both perioperative risk and to define the benefits of invasive treatment, it is rarely taken into consideration, when survival after the nephrectomy is analyzed [
3]. Santos Arrontes et al. found that a significant predictor of OS was not only stage but also CCI (discrimination ≤ 2 and >2) [
23], while Ather et al. observed a feature of >5 CCI to be an independent predictor of OS in cases treated with either radical or partial nephrectomy for RCC [
3]. On the other hand, one should be familiar with another finding i.e., Gettman et al. failed to confirm a similar association between CCI and CSS in a cohort of selected patients with venous tumor thrombus and emphasized the TNM of the primary lesion as of greatest importance [
24]. It seems, however, that OS in RCC is not only tumor-dependent but also patient-dependent, as relevant factors including individuals’ comorbidities, gender and age should be acknowledged. Here, we found that age but not gender was significantly associated with survival in univariate analyses of both endpoints. However, we failed to incorporate it into the further multivariate analyses. It is consistent with the nationwide cohort study (n = 7894 participants) that pinpointed the relationship between survival of patients with RCC and comorbidities (cases with CCIs of 1–2 and ≥3 were found to have increased mortality rates when compared with patients with no defined comorbidity), regardless of age [
25].
Recently, we found that the highest c-indexes were found when including SIRI or, alternatively, SII and NLR in the prognosis of localized RCC [
13]. However, in the present population of ccRCC patients with a longer follow-up, only SIRI and SII reached statistical significance. In a recent paper by Mao et al., elevated SIRI was a better predictor of worse OS and CSS than LMR and hemoglobin [
12]. Then, based on their own results, Lv et al. claimed that enforcing prognostic models with preoperative SIRI results in increased accuracy for RCC with tumor thrombus [
26]. Hu et al. observed that high SII was found in cases with worse OS and CSS in a non-metastatic RCC cohort post-nephrectomy (n = 646) [
27]. Ozbek et al. reported that elevated SII was found in patients with poor OS, but no association was revealed for disease-specific survival, despite the use of different thresholds [
28]. Finally, in a meta-analysis that included 3180 RCC cases, Jin et al. reported that elevated SII was a strong indicator of poor OS (and aggressive disease) but not progression-free survival/disease-free survival or CSS [
29]. These findings may shed some light on the associations of SIRI with OS and SII with CSS.
Interestingly, we failed to confirm associations with uptake of common drugs, including statins. This is consistent with recent papers, including a nationwide case–control study from Denmark (n = 4606 participants) [
30]. Pottegard et al. did not confirm the hypothesis of a chemopreventive effect of long-term statin use on the development of RCC. On the other hand, Berquist reported that statin use resulted in improved CSS and OS [
31].
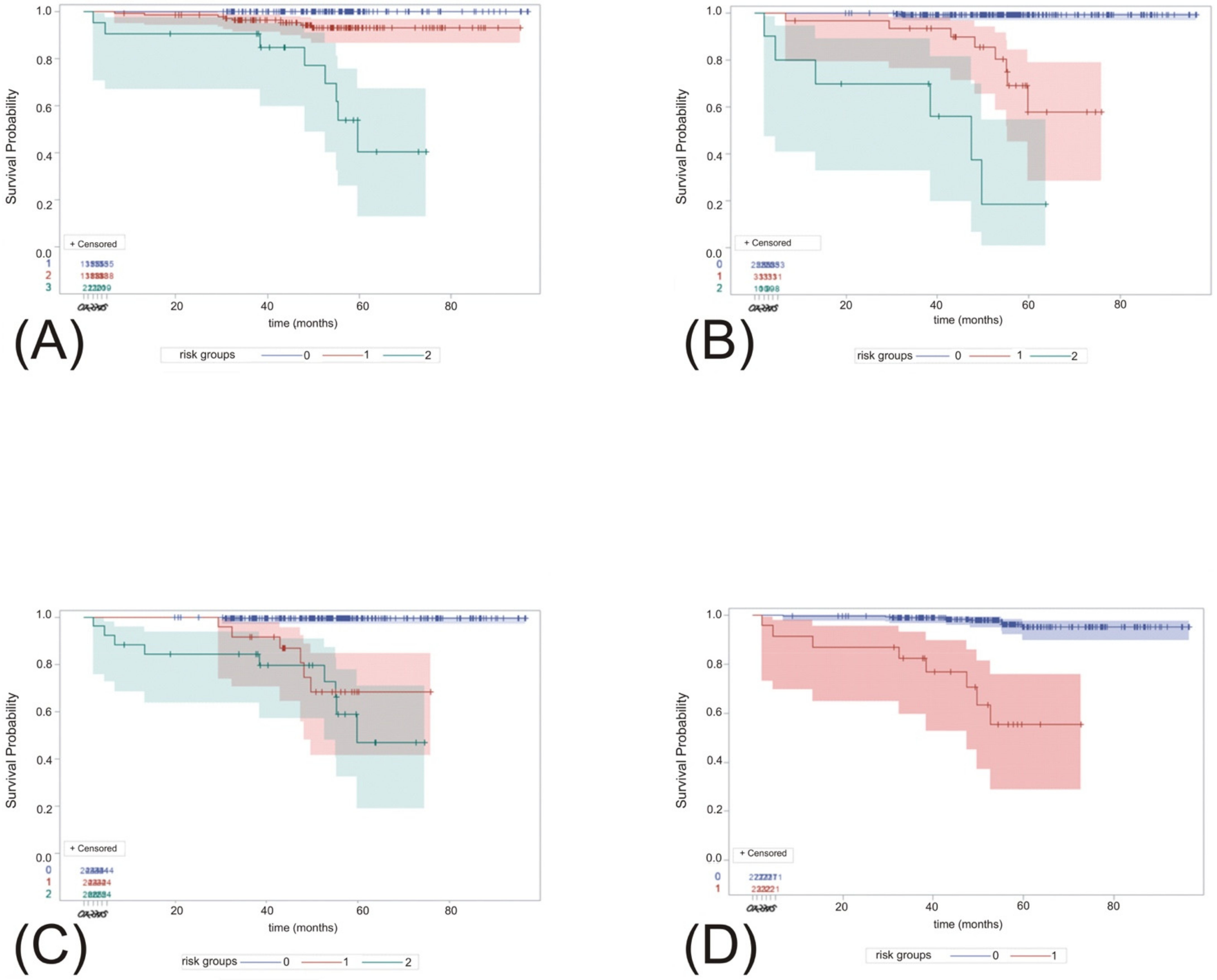
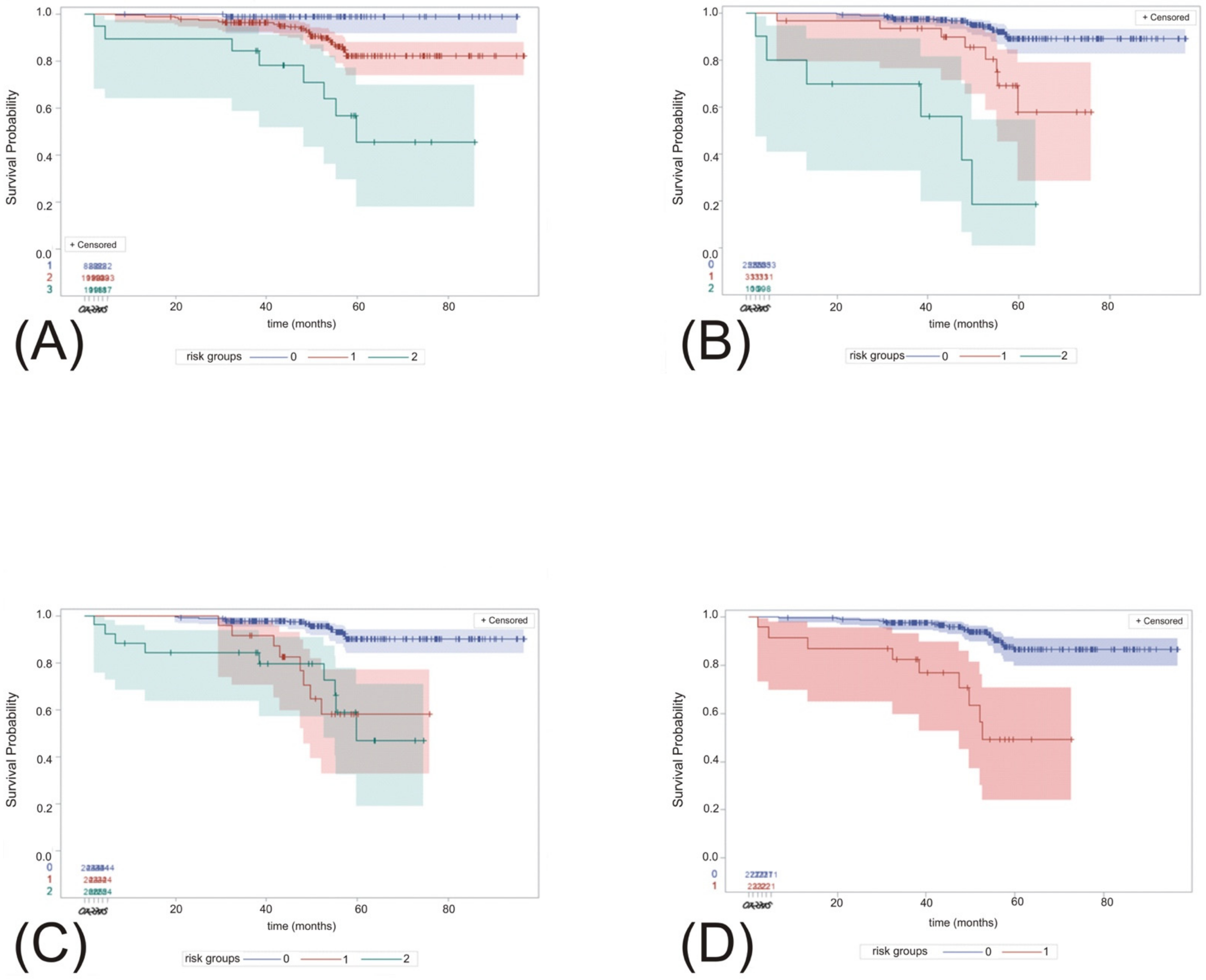
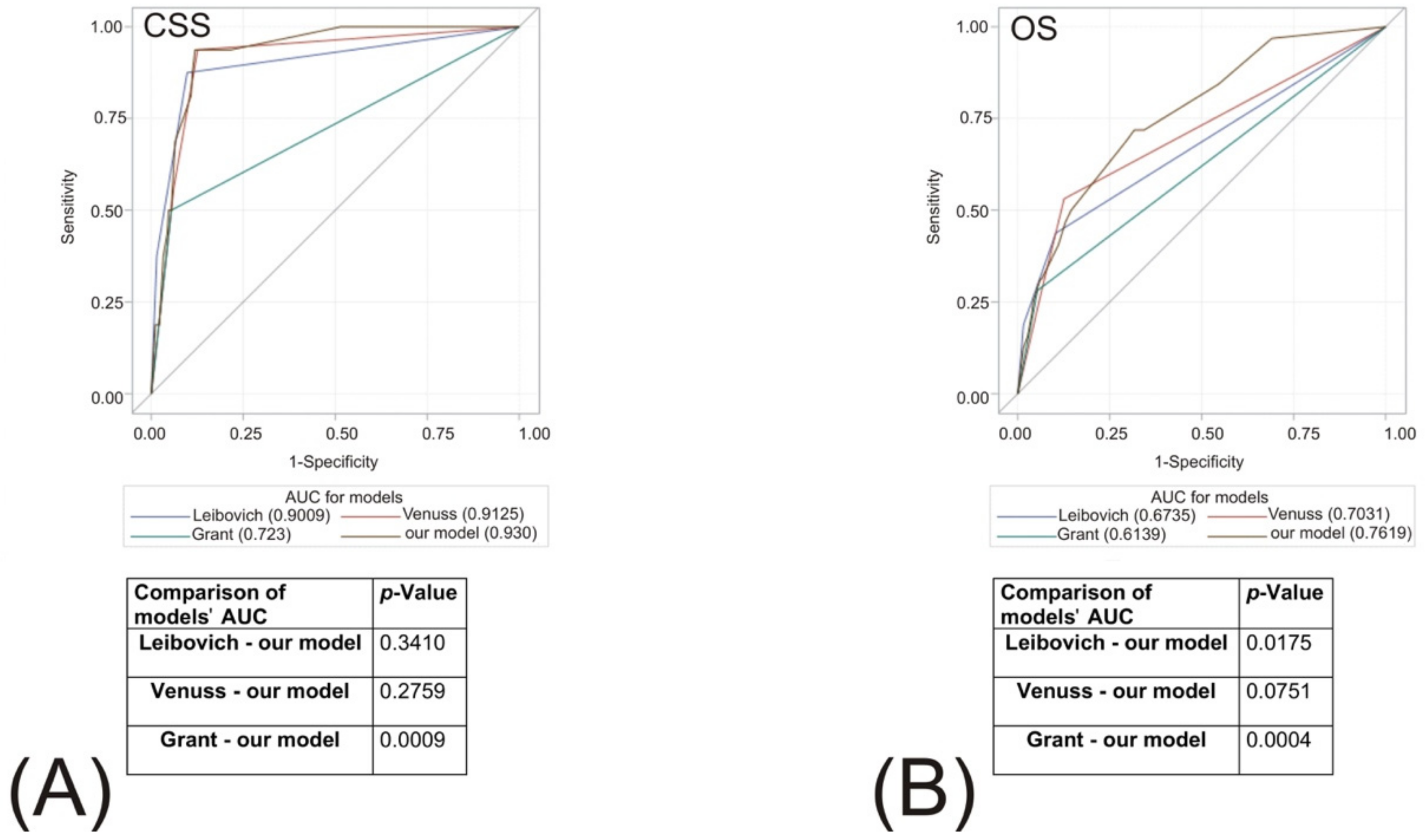
Here, we validated three well-recognized models (VENUSS, GRANT and Leibovich) in our cohort and subsequently proceeded with the preparation of our own predictive tool based on clinicopathological features, including CCI and single inflammatory markers. Clearly, there is no single best model for all the populations of RCC that could be used in the assessment of all outcomes, i.e., OS, CSS and RFS [
5]. In our model, we focused on localized ccRCC cases in the hope that we might determine other features that would have better discriminative properties when compared with TNM staging only. In the light of the multivariate analyses presented above, we described four-feature models for OS and CSS, respectively. Using ROC analyses we found that our model outperformed Leibovich and GRANT with respect to OS prognosis and GRANT with respect to CSS. On the other hand, we confirmed the non-inferiority of our model when compared with VENUSS. Therefore, external validation of the model would allow us to incorporate it into clinical applications, e.g., in enrollment for clinical trials purposes. Importantly, we discriminated between ≤T2 and ≥T3, high- vs. low-grade tumors and tumor sizes <7 or ≥7 cm, so Tumor characteristics were considered not only through T stage, while no additional pathological assessment was necessary (e.g., sarcomatoid features). The strength of the model may also lie with the incorporation of hematological biomarkers of established accuracy in the prognosis of RCC. Our model is not based on subjective clinical variables such as performance status but on intuitive calculations of CCI. Its validation in terms of predictive accuracy will enable its application in the adjuvant setting for high-risk patients treated with radical surgery to estimate the inclusion criteria for individuals that would gain benefit from systemic treatment. Finally, novel models and risk calculators can find their place in the field of transplantology, both during recipient qualification and the acceptance of organs with small renal lesions frequently found during donor assessment [
32]. Our model may be of special interest to transplant clinicians due to the incorporation of blood count derivatives.
A principal limitation of our model establishment is the retrospective nature of the data from a single tertiary center. However, we focused on records that were complete for all patients and used a single pathological laboratory, a single laboratory for blood-count analyses and a single tool for CCI calculations. Additionally, the TNM classification that we used was based on the 2017 consensus [
15], yet we included pathological grading according to Fuhrman and/or WHO/ISUP when adequate. Moreover, although the sample size was relatively small, we managed to obtain a satisfactory duration of follow-up with a standardized scheme. Our model, similar to other predictive models, is characterized by a significant deterioration in its performance over time. Furthermore, the outcome data were mainly based on intermediate- and low-risk patients. Finally, without external validation, we cannot exclude the possibility of model overfitting because of variable and threshold selections. Therefore, the prospective evaluation of our model in a larger population would enable its clinical application.


 ,
, 
{kind=link}
{kind=link}
{kind=link}


