
Biologics and Small Molecule Inhibitors for Treating Hidradenitis Suppurativa: A Systematic Review and Meta-Analysis


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
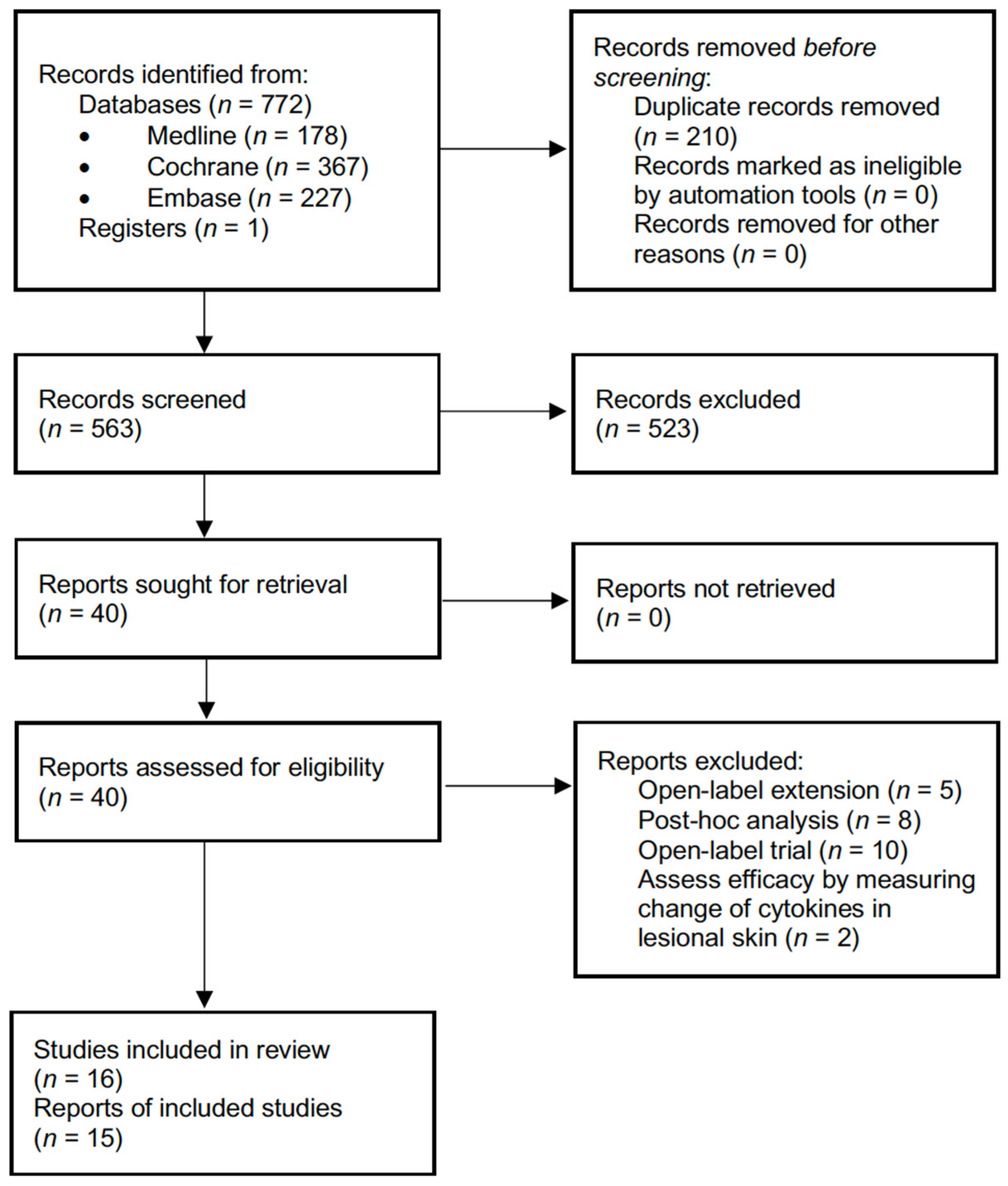
2.1. Literature Search and Study Selection
2.2. Data Extraction and Risk of Bias Evaluation
2.3. Statistical Analysis
3. Results
3.1. Risk of Bias of Included Trials
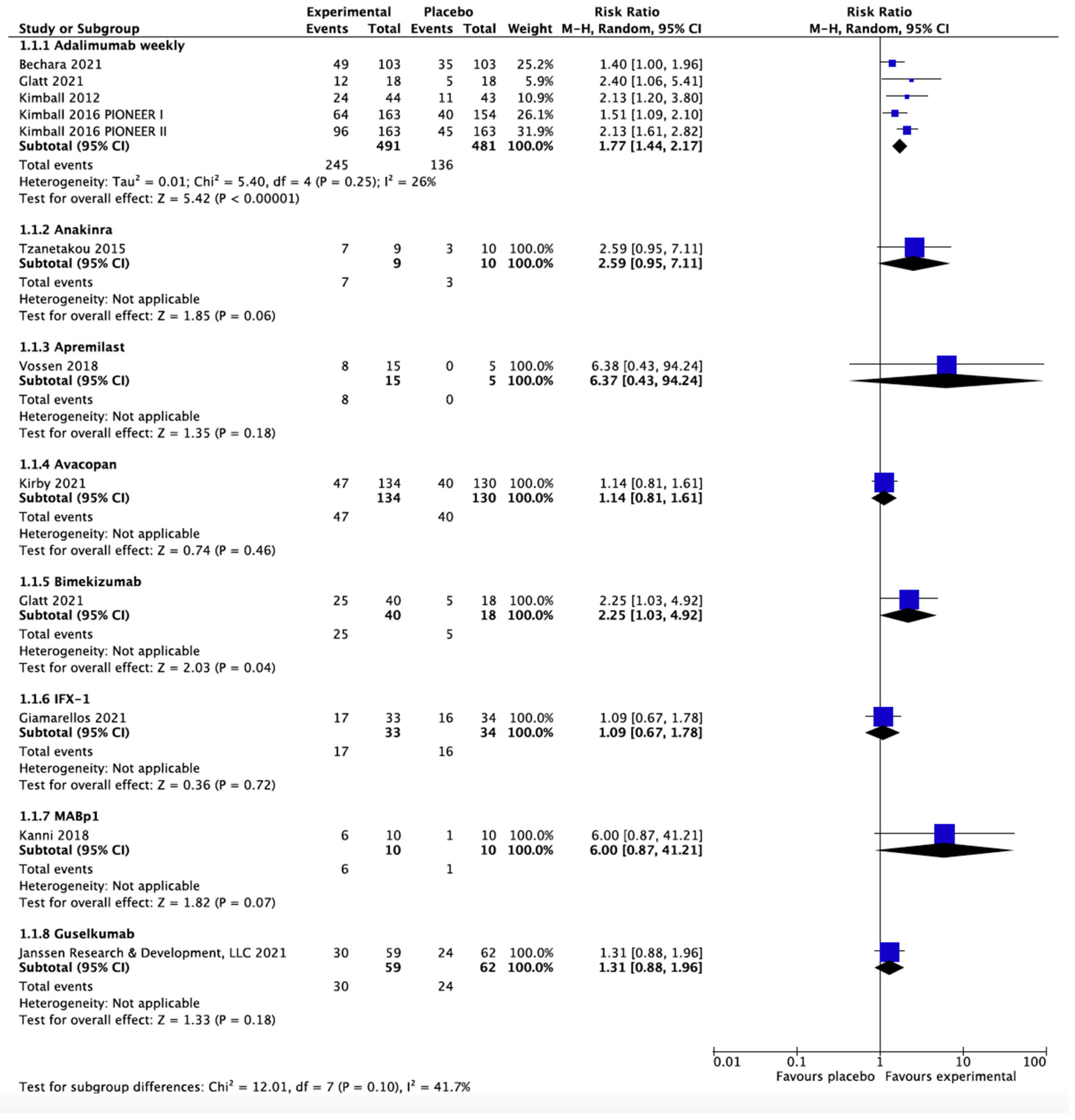
3.2. Hidradenitis Suppurativa Clinical Response at 12 to 16 Weeks
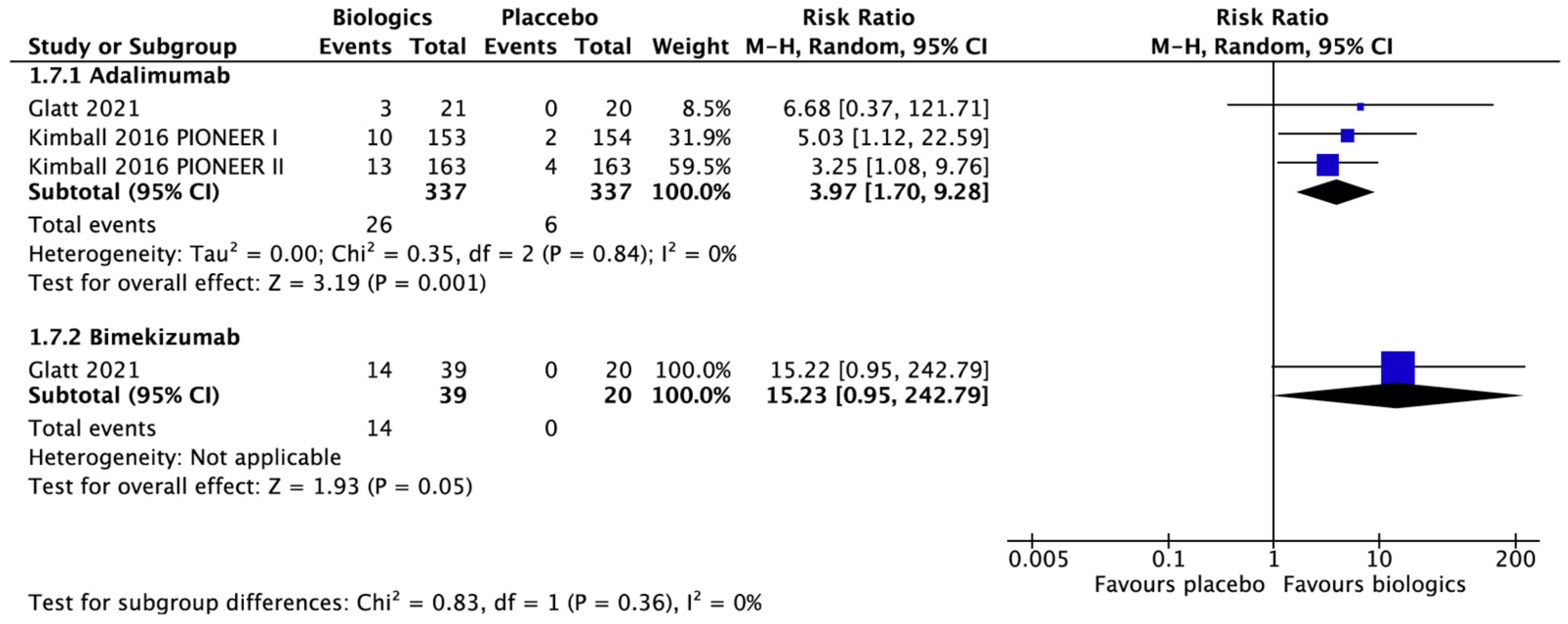
3.3. Serious Adverse Events
3.4. Dermatologic Life Quality Index
3.5. Sartorius Score and Modified Sartorius Score
3.6. Physician Global Assessment and Hidradenitis Suppurativa Physician Global Assessment
3.7. Pain
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kouris, A.; Platsidaki, E.; Christodoulou, C.; Efstathiou, V.; Dessinioti, C.; Tzanetakou, V.; Korkoliakou, P.; Zisimou, C.; Antoniou, C.; Kontochristopoulos, G. Quality of Life and Psychosocial Implications in Patients with Hidradenitis Suppurativa. Dermatology 2016, 232, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.T.; Chi, C.C. Association of hidradenitis suppurativa with inflammatory bowel disease: A systematic review and meta-analysis. JAMA Dermatol. 2019, 155, 1022–1027. [Google Scholar] [CrossRef] [PubMed]
- Dufour, D.N.; Emtestam, L.; Jemec, G.B. Hidradenitis suppurativa: A common and burdensome, yet under-recognised, inflammatory skin disease. Postgrad. Med. J. 2014, 90, 216–221; quiz 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, M.O.; Stergiopoulos, V.; Maes, M.; Kurdyak, P.A.; Lin, P.Y.; Wang, L.J.; Shyu, Y.C.; Firth, J.; Koyanagi, A.; Solmi, M.; et al. Depression and anxiety in adults with hidradenitis suppurativa: A systematic review and meta-analysis. JAMA Dermatol. 2019, 155, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.F.; Huang, Y.H.; Chi, C.C. Concomitant psoriasis and hidradenitis suppurativa responsive to adalimumab therapy: A case series. Indian J. Dermatol. Venereol. Leprol. 2021, 87, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Alatas, E.; Biteker, M.; Alatas, O. Aortic stiffness in hidradenitis suppurativa: A case-control study. Dermatol. Sin. 2021, 39, 182–185. [Google Scholar] [CrossRef]
- Jfri, A.; Nassim, D.; O’Brien, E.; Gulliver, W.; Nikolakis, G.; Zouboulis, C.C. Prevalence of Hidradenitis Suppurativa: A Systematic Review and Meta-regression Analysis. JAMA Dermatol. 2021, 157, 924–931. [Google Scholar] [CrossRef]
- Ingram, J.R. The epidemiology of hidradenitis suppurativa. Br. J. Dermatol. 2020, 183, 990–998. [Google Scholar] [CrossRef]
- Chu, C.B.; Li, W.L.; Lin, S.H.; Hsu, C.K.; Yang, C.C.; Tsai, S.J. The influence of gender and smoking on hidradenitis suppurativa: A retrospective study of 161 patients in Taiwan. Dermatol. Sin. 2021, 39, 125–131. [Google Scholar] [CrossRef]
- Del Duca, E.; Morelli, P.; Bennardo, L.; Di Raimondo, C.; Nistico, S.P. Cytokine Pathways and Investigational Target Therapies in Hidradenitis Suppurativa. Int. J. Mol. Sci. 2020, 21, 8436. [Google Scholar] [CrossRef]
- Sabat, R.; Jemec, G.B.E.; Matusiak, L.; Kimball, A.B.; Prens, E.; Wolk, K. Hidradenitis suppurativa. Nat. Rev. Dis. Primers 2020, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Vossen, A.; van der Zee, H.H.; Prens, E.P. Hidradenitis suppurativa: A systematic review integrating inflammatory pathways into a cohesive pathogenic model. Front. Immunol. 2018, 9, 2965. [Google Scholar] [CrossRef] [Green Version]
- Hendricks, A.J.; Hsiao, J.L.; Lowes, M.A.; Shi, V.Y. A comparison of international management guidelines for hidradenitis suppurativa. Dermatology 2021, 237, 81–96. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.; Megna, M.; Timoshchuk, E.A.; Patruno, C.; Balato, N.; Fabbrocini, G.; Monfrecola, G. Hidradenitis suppurativa: From pathogenesis to diagnosis and treatment. Clin. Cosmet. Investig. Dermatol. 2017, 10, 105–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingram, J.R.; Collier, F.; Brown, D.; Burton, T.; Burton, J.; Chin, M.F.; Desai, N.; Goodacre, T.E.E.; Piguet, V.; Pink, A.E.; et al. British Association of Dermatologists guidelines for the management of hidradenitis suppurativa (acne inversa) 2018. Br. J. Dermatol. 2019, 180, 1009–1017. [Google Scholar] [CrossRef] [Green Version]
- Alikhan, A.; Sayed, C.; Alavi, A.; Alhusayen, R.; Brassard, A.; Burkhart, C.; Crowell, K.; Eisen, D.B.; Gottlieb, A.B.; Hamzavi, I.; et al. North American clinical management guidelines for hidradenitis suppurativa: A publication from the United States and Canadian Hidradenitis Suppurativa Foundations: Part II: Topical, intralesional, and systemic medical management. J. Am. Acad. Dermatol. 2019, 81, 91–101. [Google Scholar] [CrossRef] [Green Version]
- Zouboulis, C.C.; Bechara, F.G.; Dickinson-Blok, J.L.; Gulliver, W.; Horvath, B.; Hughes, R.; Kimball, A.B.; Kirby, B.; Martorell, A.; Podda, M.; et al. Hidradenitis suppurativa/acne inversa: A practical framework for treatment optimization—Systematic review and recommendations from the HS ALLIANCE working group. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 19–31. [Google Scholar] [CrossRef]
- Magalhaes, R.F.; Rivitti-Machado, M.C.; Duarte, G.V.; Souto, R.; Nunes, D.H.; Chaves, M.; Hirata, S.H.; Ramos, A.M.C. Consensus on the treatment of hidradenitis suppurativa—Brazilian Society of Dermatology. An. Bras. Dermatol. 2019, 94, 7–19. [Google Scholar] [CrossRef]
- Dastoli, S.; Nistico, S.P.; Morrone, P.; Patruno, C.; Leo, A.; Citraro, R.; Gallelli, L.; Russo, E.; De Sarro, G.; Bennardo, L. Colchicine in Managing Skin Conditions: A Systematic Review. Pharmaceutics 2022, 14, 294. [Google Scholar] [CrossRef]
- Vinkel, C.; Thomsen, S.F. Hidradenitis suppurativa: Causes, features, and current treatments. J. Clin. Aesthet. Dermatol. 2018, 11, 17–23. [Google Scholar]
- Kimball, A.B.; Kerdel, F.; Adams, D.; Mrowietz, U.; Gelfand, J.M.; Gniadecki, R.; Prens, E.P.; Schlessinger, J.; Zouboulis, C.C.; van der Zee, H.H.; et al. Adalimumab for the treatment of moderate to severe Hidradenitis suppurativa: A parallel randomized trial. Ann. Int. Med. 2012, 157, 846–855. [Google Scholar] [CrossRef] [PubMed]
- Grant, A.; Gonzalez, T.; Montgomery, M.O.; Cardenas, V.; Kerdel, F.A. Infliximab therapy for patients with moderate to severe hidradenitis suppurativa: A randomized, double-blind, placebo-controlled crossover trial. J. Am. Acad. Dermatol. 2010, 62, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingram, J.R.; Hadjieconomou, S.; Piguet, V. Development of core outcome sets in hidradenitis suppurativa: Systematic review of outcome measure instruments to inform the process. Br. Dermatol. 2016, 175, 263–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.2; Higgins, J.P., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: Chichester, UK, 2021. [Google Scholar]
- HUMIRA (Adalimumab) Prescribe Information; Abbvie Inc.: North Chicago, IL, USA, 2017.
- Kimball, A.B.; Okun, M.M.; Williams, D.A.; Gottlieb, A.B.; Papp, K.A.; Zouboulis, C.C.; Armstrong, A.W.; Kerdel, F.; Gold, M.H.; Forman, S.B.; et al. Two phase 3 trials of adalimumab for hidradenitis suppurativa. N. Engl. J. Med. 2016, 375, 422–434. [Google Scholar] [CrossRef] [PubMed]
- Miller, I.; Lynggaard, C.D.; Lophaven, S.; Zachariae, C.; Dufour, D.N.; Jemec, G.B. A double-blind placebo-controlled randomized trial of adalimumab in the treatment of hidradenitis suppurativa. Br. J. Dermatol. 2011, 165, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Glatt, S.; Jemec, G.B.E.; Forman, S.; Sayed, C.; Schmieder, G.; Weisman, J.; Rolleri, R.; Seegobin, S.; Baeten, D.; Ionescu, L.; et al. Efficacy and safety of bimekizumab in moderate to severe hidradenitis suppurativa: A phase 2, double-blind, placebo-controlled randomized clinical trial. JAMA Dermatol. 2021, 157, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- Bechara, F.G.; Podda, M.; Prens, E.P.; Horvath, B.; Giamarellos-Bourboulis, E.J.; Alavi, A.; Szepietowski, J.C.; Kirby, J.; Geng, Z.; Jean, C.; et al. Efficacy and safety of adalimumab in conjunction with surgery in moderate to severe hidradenitis suppurativa: The SHARPS randomized clinical trial. JAMA Surg. 2021, 156, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Tzanetakou, V.; Kanni, T.; Giatrakou, S.; Katoulis, A.; Papadavid, E.; Netea, M.G.; Dinarello, C.A.; van der Meer, J.W.M.; Rigopoulos, D.; Giamarellos-Bourboulis, E.J. Safety and efficacy of anakinra in severe hidradenitis suppurativa: A randomized clinical trial. JAMA Dermatol. 2016, 152, 52–59. [Google Scholar] [CrossRef]
- Vossen, A.; van Doorn, M.B.A.; van der Zee, H.H.; Prens, E.P. Apremilast for moderate hidradenitis suppurativa: Results of a randomized controlled trial. J. Am. Acad. Dermatol. 2019, 80, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Kirby, J.S.; Prens, E.; Jemec, G.; Malathong, V.; Prasad, S.; Schall, T.; Staehr, P.; Investigators, F. LB791 Avacopan, a highly selective small molecule inhibitor of c5a receptor, in patients with hidradenitis suppurativa: Initial results from a randomized, double-blind, placebo-controlled, phase 2 study (aurora). J. Investig. Dermatol. 2021, 141, B19. [Google Scholar] [CrossRef]
- Kimball, A.; Prens, E.; Bechara, F.G.; Weisman, J.; Kolbinger, F.; Rozenberg, I.; Jones, J.; Loesche, C.; Jemec, G. Hidradenitis suppurativa responds to a novel anti-il17 antibody (CJM112) in a controlled clinical trial vs. placebo. In Proceedings of the 24th world Congress of Dermatology, Milan, Italy, 11–15 June 2019. [Google Scholar]
- Adams, D.R.; Yankura, J.A.; Fogelberg, A.C.; Anderson, B.E. Treatment of hidradenitis suppurativa with etanercept injection. Arch. Dermatol. 2010, 146, 501–504. [Google Scholar] [CrossRef] [PubMed]
- Janssen, R.; Development, L.L.C. A Study to Evaluate the Efficacy, Safety, and Tolerability of Guselkumab for the Treatment of Participants with Moderate to Severe Hidradenitis Suppurativa (HS). Clinical Trial Registration. 2021. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03628924 (accessed on 19 May 2022).
- Giamarellos-Bourboulis, E.J.; Jemec, G.B.E.; Prens, E.P.; Habel, M.; Szepietowski, J.C.; Van Der Zee, H.H.; Zouboulis, C.C.; Sayed, C.J. Complement Split Product C5a Is Elevated in Moderate and Severe Hidradenitis Suppurativa: Clinical Improvement by Targeted Therapy Coming from the SHINE Study. Available online: https://www.ehsf2021.com/wp-content/uploads/2021/02/EHSF_2021_HP.pdf (accessed on 19 May 2022).
- Alavi, A.; Hamzavi, I.; Brown, K.; Santos, L.L.; Zhu, Z.; Liu, H.; Howell, M.D.; Kirby, J. Janus kinase 1 inhibitor INCB054707 for patients with moderate-to-severe hidradenitis suppurativa: Results from two phase 2 studies. Br. J. Dermatol. 2022, 186, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Kanni, T.; Argyropoulou, M.; Spyridopoulos, T.; Pistiki, A.; Stecher, M.; Dinarello, C.A.; Simard, J.; Giamarellos-Bourboulis, E.J. MABp1 targeting IL-1alpha for moderate to severe hidradenitis suppurativa not eligible for adalimumab: A randomized study. J. Investig. Dermatol. 2018, 138, 795–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingram, J.R.; Woo, P.N.; Chua, S.L.; Ormerod, A.D.; Desai, N.; Kai, A.C.; Hood, K.; Burton, T.; Kerdel, F.; Garner, S.E.; et al. Interventions for hidradenitis suppurativa. Cochrane Database Syst. Rev. 2015, 2015, CD010081. [Google Scholar] [CrossRef]
- Monfrecola, G.; Megna, M. Classification and severity scales. In Hidradenitis Suppurativa: A Diagnostic Atlas, 1st ed.; Micali, G., Ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2017; pp. 39–45. [Google Scholar]
- Van der Zee, H.H.; Laman, J.D.; de Ruiter, L.; Dik, W.A.; Prens, E.P. Adalimumab (antitumour necrosis factor-alpha) treatment of hidradenitis suppurativa ameliorates skin inflammation: An in situ and ex vivo study. Br. J. Dermatol. 2012, 166, 298–305. [Google Scholar] [CrossRef]
- Van der Zee, H.H.; de Ruiter, L.; van den Broecke, D.G.; Dik, W.A.; Laman, J.D.; Prens, E.P. Elevated levels of tumour necrosis factor (TNF)-alpha, interleukin (IL)-1beta and IL-10 in hidradenitis suppurativa skin: A rationale for targeting TNF-alpha and IL-1beta. Br. J. Dermatol. 2011, 164, 1292–1298. [Google Scholar] [CrossRef]
- Kelly, G.; Hughes, R.; McGarry, T.; van den Born, M.; Adamzik, K.; Fitzgerald, R.; Lawlor, C.; Tobin, A.M.; Sweeney, C.M.; Kirby, B. Dysregulated cytokine expression in lesional and nonlesional skin in hidradenitis suppurativa. Br. J. Dermatol. 2015, 173, 1431–1439. [Google Scholar] [CrossRef]
- Vossen, A.; van der Zee, H.H.; Davelaar, N.; Mus, A.M.C.; van Doorn, M.B.A.; Prens, E.P. Apremilast for moderate hidradenitis suppurativa: No significant change in lesional skin inflammatory biomarkers. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 761–765. [Google Scholar] [CrossRef]
- Lowe, M.M.; Naik, H.B.; Clancy, S.; Pauli, M.; Smith, K.M.; Bi, Y.; Dunstan, R.; Gudjonsson, J.E.; Paul, M.; Harris, H.; et al. Immunopathogenesis of hidradenitis suppurativa and response to anti-TNF-alpha therapy. JCI Insight 2020, 5, e139932. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Shear, N.H.; Piguet, V.; Bamimore, M.A. Efficacy of non-surgical monotherapies for hidradenitis suppurativa: A systematic review and network meta-analyses of randomized trials. J. Dermatol. Treat. 2022, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Jemec, G.B.; Wendelboe, P. Topical clindamycin versus systemic tetracycline in the treatment of hidradenitis suppurativa. J. Am. Acad. Dermatol. 1998, 39, 971–974. [Google Scholar] [CrossRef]
- Grimstad, O.; Kvammen, B.O.; Swartling, C. Botulinum Toxin Type B for Hidradenitis Suppurativa: A Randomised, Double-Blind, Placebo-Controlled Pilot Study. Am. J. Clin. Dermatol. 2020, 21, 741–748. [Google Scholar] [CrossRef]
- Fernandez-Vozmediano, J.M.; Armario-Hita, J.C. Infliximab for the treatment of hidradenitis suppurativa. Dermatology 2007, 215, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Garnock-Jones, K.P.; Keam, S.J. Adalimumab: A review in hidradenitis suppurativa. Am. J. Clin. Dermatol. 2016, 17, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Savage, K.T.; Flood, K.S.; Porter, M.L.; Kimball, A.B. TNF-alpha inhibitors in the treatment of hidradenitis suppurativa. Ther. Adv. Chronic Dis. 2019, 10, 2040622319851640. [Google Scholar] [CrossRef]
- Hong, D.S.; Hui, D.; Bruera, E.; Janku, F.; Naing, A.; Falchook, G.S.; Piha-Paul, S.; Wheler, J.J.; Fu, S.; Tsimberidou, A.M.; et al. MABp1, a first-in-class true human antibody targeting interleukin-1alpha in refractory cancers: An open-label, phase 1 dose-escalation and expansion study. Lancet Oncol. 2014, 15, 656–666. [Google Scholar] [CrossRef]
- Crowley, J.; Thaci, D.; Joly, P.; Peris, K.; Papp, K.A.; Goncalves, J.; Day, R.M.; Chen, R.; Shah, K.; Ferrandiz, C.; et al. Long-term safety and tolerability of apremilast in patients with psoriasis: Pooled safety analysis for ≥156 weeks from 2 phase 3, randomized, controlled trials (ESTEEM 1 and 2). J. Am. Acad. Dermatol. 2017, 77, 310–317.e1. [Google Scholar] [CrossRef] [Green Version]
- Schiff, M.H.; DiVittorio, G.; Tesser, J.; Fleischmann, R.; Schechtman, J.; Hartman, S.; Liu, T.; Solinger, A.M. The safety of anakinra in high-risk patients with active rheumatoid arthritis: Six-month observations of patients with comorbid conditions. Arthritis Rheum 2004, 50, 1752–1760. [Google Scholar] [CrossRef]
- Reich, K.; Papp, K.A.; Blauvelt, A.; Langley, R.G.; Armstrong, A.; Warren, R.B.; Gordon, K.B.; Merola, J.F.; Okubo, Y.; Madden, C.; et al. Bimekizumab versus ustekinumab for the treatment of moderate to severe plaque psoriasis (BE VIVID): Efficacy and safety from a 52-week, multicentre, double-blind, active comparator and placebo controlled phase 3 trial. Lancet 2021, 397, 487–498. [Google Scholar] [CrossRef]
- Kaul, M.; Jarvis, P.; Rozenberg, I.; Kolbinger, F.; Di Padova, F.; Calonder, C.; Espie, P.; Rondeau, J.M.; Cebe, R.; Huber, T.; et al. First-in-human study demonstrating the safety and clinical efficacy of novel anti-IL-17A monoclonal antibody CJM112 in moderate to severe plaque psoriasis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Vlaar, A.P.J.; de Bruin, S.; Busch, M.; Timmermans, S.A.M.E.G.; van Zeggeren, I.E.; Koning, R.; Ter Horst, L.; Bulle, E.B.; van Baarle, F.E.H.P.; van de Poll, M.C.G.; et al. Anti-C5a antibody IFX-1 (vilobelimab) treatment versus best supportive care for patients with severe COVID-19 (PANAMO): An exploratory, open-label, phase 2 randomised controlled trial. Lancet Rheumatol. 2020, 2, e764–e773. [Google Scholar] [CrossRef]
- Osman, M.; Cohen Tervaert, J.W.; Pagnoux, C. Avacopan for the treatment of ANCA-associated vasculitis. Expert Rev. Clin. Immunol. 2021, 17, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Gulliver, W.P. Update on clinical trials in hidradenitis suppurativa. Exp. Dermatol. 2021, 30, 67–68. [Google Scholar] [CrossRef]
- Frew, J.W.; Navrazhina, K.; Grand, D.; Sullivan-Whalen, M.; Gilleaudeau, P.; Garcet, S.; Ungar, J.; Krueger, J.G. The effect of subcutaneous brodalumab on clinical disease activity in hidradenitis suppurativa: An open-label cohort study. J. Am. Acad. Dermatol. 2020, 83, 1341–1348. [Google Scholar] [CrossRef] [PubMed]
- Casseres, R.G.; Prussick, L.; Zancanaro, P.; Rothstein, B.; Joshipura, D.; Saraiya, A.; Turkowski, Y.; Au, S.C.; Alomran, A.; Abdat, R.; et al. Secukinumab in the treatment of moderate to severe hidradenitis suppurativa: Results of an open-label trial. J. Am. Acad. Dermatol. 2020, 82, 1524–1526. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-H.; Huang, I.-H.; Tai, C.-C.; Chi, C.-C. Biologics and Small Molecule Inhibitors for Treating Hidradenitis Suppurativa: A Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 1303. https://doi.org/10.3390/biomedicines10061303
Huang C-H, Huang I-H, Tai C-C, Chi C-C. Biologics and Small Molecule Inhibitors for Treating Hidradenitis Suppurativa: A Systematic Review and Meta-Analysis. Biomedicines. 2022; 10(6):1303. https://doi.org/10.3390/biomedicines10061303
Chicago/Turabian StyleHuang, Chun-Hsien, I-Hsin Huang, Cheng-Chen Tai, and Ching-Chi Chi. 2022. "Biologics and Small Molecule Inhibitors for Treating Hidradenitis Suppurativa: A Systematic Review and Meta-Analysis" Biomedicines 10, no. 6: 1303. https://doi.org/10.3390/biomedicines10061303
APA StyleHuang, C. -H., Huang, I. -H., Tai, C. -C., & Chi, C. -C. (2022). Biologics and Small Molecule Inhibitors for Treating Hidradenitis Suppurativa: A Systematic Review and Meta-Analysis. Biomedicines, 10(6), 1303. https://doi.org/10.3390/biomedicines10061303