
Anti-PD-1 Monotherapy in Advanced Melanoma—Real-World Data from a 77-Month-Long Retrospective Observational Study


 , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patient Characteristics
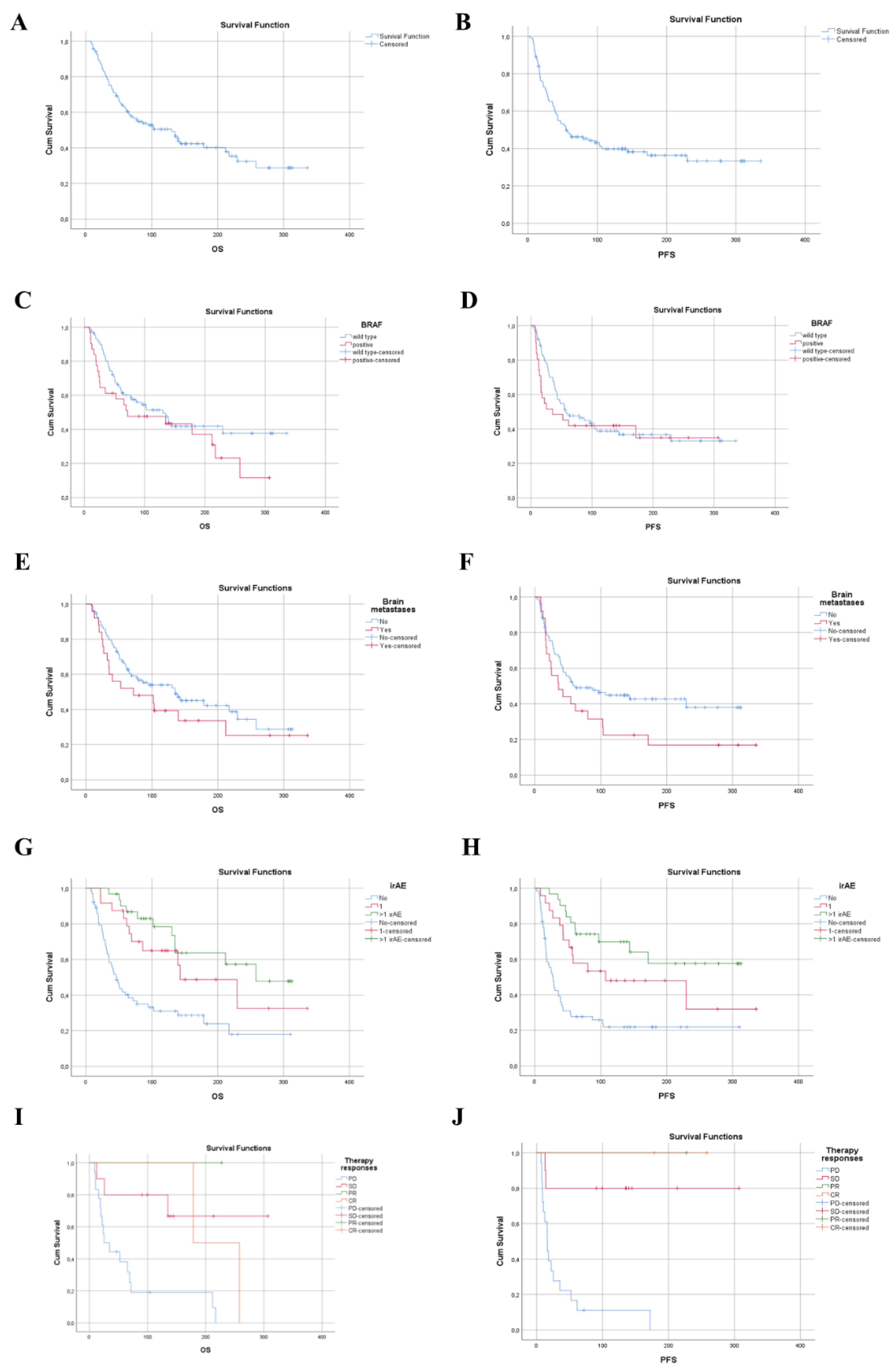
3.2. Efficacy–Survival Data
3.3. Toxicity

{kind=link}
| IrAE | Grade 1–2 N = 37 (31.08%) | Grade 3–4 N = 18 (15.12%) | All Grade N = 55 (46.2%) |
|---|---|---|---|
| Endocrine | 24 (20.16) | 4 (3.36) | 28 (23.52) |
| hypothyroidism | 16 (13.44) | - | 16 (13.44) |
| hyperthyroidism | 2 (1.68) | - | 2 (1.68) |
| hypopituitarism | 6 (5.04) | 4 (3.36) | 10 (8.4) |
| respiratory | 1 (0.84) | 8 (6.72) | 9 (7.56) |
| pneumonitis | 1 (0.84) | 8 (6.72) | 9 (7.56) |
| Gastrointestinal | 9 (7.56) | 14 (11.76) | 23 (19.32) |
| colitis | 5 (4.2) | 11 (9.24) | 16 (13.44) |
| gastritis | 4 (3.36) | 2 (1.68) | 6 (5.04) |
| terminalis ileitis | - | 1 (0.84) | 1 (0.84) |
| Hepato-pancreato-biliary | 25 (21) | 6 (5.04) | 31 (26.04) |
| hepatitis/ALT elevated | 10 (8.4) | 2 (1.68) | 12 (10.08) |
| bilirubin elevated | 6 (5.04) | - | 6 (5.04) |
| pancreatitis | 8 (6.72) | 3 (2.52) | 11 (7.56) |
| hyperlipidemia | 1 (0.84) | 1 (0.84) | 2 (1.68) |
| Musculoskeletal | 9 (7.56) | 2 (1.68) | 11 (7.56) |
| myositis | 5 (4.2) | 2 (1.68) | 7 (5.88) |
| arthritis | 4 (3.36) | - | 4 (3.36) |
| Renal | 5 (4.2) | 4 (3.36) | 9 (7.56) |
| nephritis | 5 (4.2) | 4 (3.36) | 9 (7.56) |
| Skin | 12 (10.04) | 3 (2.52) | 15 (12.6) |
| vitiligo | 5 (4.2) | - | 5 (4.2) |
| dermatitis | 5 (4.2) | 3 (2.52) | 8 (6.72) |
| bullous pemphigoid | 2 (1.68) | - | 2 (1.68) |
| Nervous system | 4 (3.36) | 1 (0.84) | 5 (4.2) |
| polyneuropathy | 4 (3.36) | - | 4 (3.36) |
| encephalitis | - | 1 (0.84) | 1 (0.84) |
| Hematological | 1 (0.84) | 1 (0.84) | |
| pancytopenia | 1 (0.84) | - | 1 (0.84) |
| Ophthalmic | 3 (2.52) | 1 (0.84) | 4 (3.36) |
| bulbitis | - | 1 (0.84) | 1 (0.84) |
| conjunctivitis | 1 (0.84) | - | 1 (0.84) |
| uveitis, iridocyclitis | 2 (1.68) | - | 2 (1.68) |
| Oral cavity/ear | 4 (3.36) | 4 (3.36) | |
| periodontitis | 1 (0.84) | - | 1 (0.84) |
| otitis media, otitis externa, sinusitis, ethmoiditis | 3 (2.52) | - | 3 (2.52) |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Stroyakovskiy, D.; Gogas, H.; Levchenko, E.; de Braud, F.; Larkin, J.; Garbe, C.; Jouary, T.; Hauschild, A.; Grob, J.J.; et al. Combined BRAF and MEK Inhibition versus BRAF Inhibition Alone in Melanoma. N. Engl. J. Med. 2014, 371, 1877–1888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodi, F.S.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1480–1492. [Google Scholar] [CrossRef]
- Garbe, C.; Amaral, T.; Peris, K.; Hauschild, A.; Arenberger, P.; Basset-Seguin, N.; Bastholt, L.; Bataille, V.; del Marmol, V.; Dréno, B.; et al. European consensus-based interdisciplinary guideline for melanoma. Part 2: Treatment-Update 2022. Eur. J. Cancer 2022, 170, 236–255. [Google Scholar] [CrossRef]
- Aroldi, F.; Middleton, M.R. Long-Term Outcomes of Immune Checkpoint Inhibition in Metastatic Melanoma. Am. J. Clin. Dermatol. 2022, 23, 331–338. [Google Scholar] [CrossRef]
- Schachter, J.; Ribas, A.; Long, G.V.; Arance, A.; Grob, J.-J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus ipilimumab for advanced melanoma: Final overall survival results of a multicentre, randomised, open-label phase 3 study (KEYNOTE-006). Lancet 2017, 390, 1853–1862. [Google Scholar] [CrossRef]
- Donia, M.; Kimper-Karl, M.L.; Høyer, K.L.; Bastholt, L.; Schmidt, H.; Svane, I.M. The majority of patients with metastatic melanoma are not represented in pivotal phase III immunotherapy trials. Eur. J. Cancer 2017, 74, 89–95. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Zhou, Z.; Zheng, C.; Liu, Y.; Hao, R.; Ji, X.; Xi, Q.; Shen, J.; Li, Z. Chitosan oligosaccharide regulates AMPK and STAT1 pathways synergistically to mediate PD-L1 expression for cancer chemoimmunotherapy. Carbohydr. Polym. 2021, 277, 118869. [Google Scholar] [CrossRef]
- Xiong, W.; Qi, L.; Jiang, N.; Zhao, Q.; Chen, L.; Jiang, X.; Li, Y.; Zhou, Z.; Shen, J. Metformin Liposome-Mediated PD-L1 Downregulation for Amplifying the Photodynamic Immunotherapy Efficacy. ACS Appl. Mater. Interfaces 2021, 13, 8026–8041. [Google Scholar] [CrossRef]
- Zhou, Z.; Jiang, N.; Chen, J.; Zheng, C.; Guo, Y.; Ye, R.; Qi, R.; Shen, J. Selectively down-regulated PD-L1 by albumin-phenformin nanoparticles mediated mitochondrial dysfunction to stimulate tumor-specific immunological response for enhanced mild-temperature photothermal efficacy. J. Nanobiotechnol. 2021, 19, 375. [Google Scholar] [CrossRef]
- Weber, J.S.; Hodi, F.S.; Wolchok, J.D.; Topalian, S.L.; Schadendorf, D.; Larkin, J.; Sznol, M.; Long, G.; Li, H.; Waxman, I.M.; et al. Safety Profile of Nivolumab Monotherapy: A Pooled Analysis of Patients With Advanced Melanoma. J. Clin. Oncol. 2017, 35, 785–792. [Google Scholar] [CrossRef]
- Bastacky, M.L.; Wang, H.; Fortman, D.; Rahman, Z.; Mascara, G.P.; Brenner, T.; Najjar, Y.G.; Luke, J.J.; Kirkwood, J.M.; Zarour, H.M.; et al. Immune-Related Adverse Events in PD-1 Treated Melanoma and Impact Upon Anti-Tumor Efficacy: A Real World Analysis. Front. Oncol. 2021, 11, 749064. [Google Scholar] [CrossRef] [PubMed]
- Arheden, A.; Skalenius, J.; Bjursten, S.; Stierner, U.; Ny, L.; Levin, M.; Jespersen, H. Real-world data on PD-1 inhibitor therapy in metastatic melanoma. Acta Oncol. 2019, 58, 962–966. [Google Scholar] [CrossRef]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamid, O.; Robert, C.; Daud, A.; Hodi, F.S.; Hwu, W.J.; Kefford, R.; Wolchok, J.D.; Hersey, P.; Joseph, R.; Weber, J.S.; et al. Five-year survival outcomes for patients with advanced melanoma treated with pembrolizumab in KEYNOTE-001. Ann. Oncol. 2019, 30, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Hamid, O.; Robert, C.; Daud, A.; Carlino, M.S.; Mitchell, T.C.; Hersey, P.; Schachter, J.; Long, G.V.; Hodi, F.S.; Wolchok, J.D.; et al. Long-term outcomes in patients with advanced melanoma who had initial stable disease with pembrolizumab in KEYNOTE-001 and KEYNOTE-006. Eur. J. Cancer 2021, 157, 391–402. [Google Scholar] [CrossRef]
- Robert, C.; Hwu, W.-J.; Hamid, O.; Ribas, A.; Weber, J.S.; Daud, A.I.; Hodi, F.S.; Wolchok, J.D.; Mitchell, T.C.; Hersey, P.; et al. Long-term safety of pembrolizumab monotherapy and relationship with clinical outcome: A landmark analysis in patients with advanced melanoma. Eur. J. Cancer 2020, 144, 182–191. [Google Scholar] [CrossRef]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Di Giacomo, A.M.; Mortier, L.; Rutkowski, P.; Hassel, J.C.; McNeil, C.M.; Kalinka, E.A.; et al. Five-Year Outcomes With Nivolumab in Patients With Wild-Type BRAF Advanced Melanoma. J. Clin. Oncol. 2020, 38, 3937–3946. [Google Scholar] [CrossRef]
- Monestier, S.; Dalle, S.; Mortier, L.; Dutriaux, C.; Dalac-Rat, S.; Meyer, N.; Leccia, M.T.; Mansard, S.; Montaudié, H.; Saiag, P.; et al. Effectiveness and safety of nivolumab in patients with advanced melanoma: A multicenter, observational study. Int. J. Cancer 2021, 148, 2789–2798. [Google Scholar] [CrossRef]
- Tan, X.-L.; Le, A.; Lam, F.C.; Scherrer, E.; Kerr, R.G.; Lau, A.C.; Han, J.; Jiang, R.; Diede, S.J.; Shui, I.M. Current Treatment Approaches and Global Consensus Guidelines for Brain Metastases in Melanoma. Front. Oncol. 2022, 12, 885472. [Google Scholar] [CrossRef]
- Frinton, E.; Tong, D.; Tan, J.; Read, G.; Kumar, V.; Kennedy, S.; Lim, C.; Board, R.E. Metastatic melanoma: Prognostic factors and survival in patients with brain metastases. J. Neuro-Oncol. 2017, 135, 507–512. [Google Scholar] [CrossRef] [Green Version]
- Tawbi, H.A.; Forsyth, P.A.; Algazi, A.; Hamid, O.; Hodi, F.S.; Moschos, S.J.; Khushalani, N.I.; Lewis, K.; Lao, C.D.; Postow, M.A.; et al. Combined Nivolumab and Ipilimumab in Melanoma Metastatic to the Brain. N. Engl. J. Med. 2018, 379, 722–730. [Google Scholar] [CrossRef]
- Long, G.V.; Atkinson, V.; Lo, S.; Sandhu, S.; Guminski, A.D.; Brown, M.P.; Wilmott, J.S.; Edwards, J.; Gonzalez, M.; Scolyer, R.A.; et al. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: A multicentre randomised phase 2 study. Lancet Oncol. 2018, 19, 672–681. [Google Scholar] [CrossRef]
- Roger, A.; Finet, A.; Boru, B.; Beauchet, A.; Mazeron, J.-J.; Otzmeguine, Y.; Blom, A.; Longvert, C.; De Maleissye, M.-F.; Fort, M.; et al. Efficacy of combined hypo-fractionated radiotherapy and anti-PD-1 monotherapy in difficult-to-treat advanced melanoma patients. OncoImmunology 2018, 7, e1442166. [Google Scholar] [CrossRef]
- Umeda, Y.; Yoshikawa, S.; Kiniwa, Y.; Maekawa, T.; Yamasaki, O.; Isei, T.; Matsushita, S.; Nomura, M.; Nakai, Y.; Fukushima, S.; et al. Real-world efficacy of anti-PD-1 antibody or combined anti-PD-1 plus anti-CTLA-4 antibodies, with or without radiotherapy, in advanced mucosal melanoma patients: A retrospective, multicenter study. Eur. J. Cancer 2021, 157, 361–372. [Google Scholar] [CrossRef]
- Funck-Brentano, E.; Baghad, B.; Fort, M.; Aouidad, I.; Roger, A.; Beauchet, A.; Otmezguine, Y.; Blom, A.; Longvert, C.; Boru, B.; et al. Efficacy of late concurrent hypofractionated radiotherapy in advanced melanoma patients failing anti-PD-1 monotherapy. Int. J. Cancer 2020, 147, 1707–1714. [Google Scholar] [CrossRef]
- Suo, A.; Chan, Y.; Beaulieu, C.; Kong, S.; Cheung, W.Y.; Monzon, J.G.; Smylie, M.; Walker, J.; Morris, D.; Cheng, T. Anti-PD1-Induced Immune-Related Adverse Events and Survival Outcomes in Advanced Melanoma. Oncologist 2020, 25, 438–446. [Google Scholar] [CrossRef] [Green Version]

| Median (IQR) or N (%) | ||||
|---|---|---|---|---|
| Total Sample * (N = 119) | Non-Responders * (N = 98) | Responders * (N = 20) | p-Value ** | |
| Age (years) | 69.0 (57.0–75.0) | 68.5 (57.0–75.0) | 68.5 (53.5–79.25) | 0.622 |
| ≥70 years | 62 (52.1) | 52 (83.9) | 10 (16.1) | 0.811 |
| <70 years | 57 (47.9) | 46 (80.7) | 10 (17.5) | |
| Gender | ||||
| Male | 68 (57.1) | 54 (79.4) | 13 (19.1) | 0.466 |
| Female | 51 (42.9) | 44 (86.3) | 7 (13.7) | |
| Received doses | 14.0 (7.0–32.0) | 12.0 (6.0–26.0) | 24.0 (17.5–44.5) | 0.002 |
| Duration of treatment (weeks) | 45.1 (17.3–112.1) | 37.6 (16.1–92.3) | 118.0 (56.0–192.4) | <0.001 |
| Primary tumor | ||||
| Occult | 21 (17.6) | 16 (76.2) | 5 (23.8) | 0.670 |
| Superficial spreading melanoma (SSM) | 23 (19.3) | 21 (91.3) | 2 (8.7) | |
| Nodular melanoma (NM) | 33 (27.7) | 28 (84.8) | 5 (15.2) | |
| Acral lentiginous (ALM) | 15 (12.6) | 13 (86.7) | 2 (13.3) | |
| Lentigo maligna melanoma (LMM) | 2 (1.7) | 2 (100.0) | - | |
| desmoplastic melanoma (DM) | 2 (1.7) | 2 (100.0) | - | |
| Not classified | 23 (19.3) | 16 (69.6) | 6 (26.1) | |
| T | 0.082 | |||
| ptx or no primary tumor | 35 (29.4) | 25 (71.4) | 10 (28.6) | |
| pT1a | 3 (2.5) | 3 (100.0) | - | |
| pT2a | 6 (5.0) | 6 (100.0) | - | |
| pT2b | 5 (4.2) | 5 (100.0) | - | |
| pT3a | 9 (7.6) | 8 (88.9) | 1 (11.1) | |
| pT3b | 16 (13.4) | 16 (100.0) | - | |
| pT4a | 9 (7.6) | 9 (100.0) | - | |
| pT4b | 36 (30.3) | 26 (72.2) | 9 (25.0) | |
| TIL | ||||
| Brisk | 15 (12.6) | 12 (80.0) | 3 (20.0) | 0.316 |
| Non-brisk | 12 (10.1) | 7 (58.3) | 4 (33.3) | |
| Absent | 18 (15.1) | 16 (88.9) | 2 (11.1) | |
| Unknown | 74 (62.2) | 63 (85.1) | 11 (14.9) | |
| N | 0.158 | |||
| No | 57 (47.9) | 51 (89.5) | 6 (30.0) | |
| Yes | 58 (48.7) | 44 (75.9) | 13 (65.0) | |
| Unknown | 4 (3.4) | 3 (75.0) | 1 (5.0) | |
| M AJCC 8th edition | 0.136 | |||
| M0 | 1 (0.8) | 1 (100.0) | - | |
| M1a | 22 (18.5) | 19 (86.4) | 3 (13.6) | |
| M1b | 15 (12.6) | 13 (86.7) | 2 (13.3) | |
| M1c | 56 (47.04) | 41 (73.2) | 14 (25.0) | |
| M1d | 25 (21.0) | 24 (96.0) | 1 (4.0) | |
| Disease stage | ||||
| III | 1 (0.8) | 1 (100.0) | - | 1.000 |
| IV | 118 (99.2) | 97 (82.2) | 20 (16.9) | |
| Treatment NE = 1 | ||||
| Nivolumab | 52 (43.7) | 45 (86.5) | 6 (11.5) | 0.220 |
| Pembrolizumab | 66 (55.5) | 52 (78.8) | 14 (21.2) | |
| Line of treatment | ||||
| First | 81 (68.1) | 66 (81.5) | 14 (17.3) | 1.000 |
| Second + third | 38 (31.9) | 32 (84.2) | 6 (15.8) | |
| Reason for treatment cessation | ||||
| Did not stop | 36 (30.3) | 24 (66.7) | 11 (30.6) | <0.001 |
| AE | 13 (10.9) | 9 (69.2) | 4 (30.8) | |
| PD | 49 (41.2) | 48 (98.0) | 1 (2.0) | |
| Exit | 19 (16.0) | 17 (89.5) | 2 (10.5) | |
| CR | 2 (1.7) | - | 2 (100.0) | |
| IrAE | ||||
| No | 64 (53.8) | 56 (87.5) | 7 (10.9) | 0.058 |
| IrAE = 1 | 24 (20.2) | 16 (66.7) | 8 (33.3) | |
| IrAE > 1 | 31 (26.1) | 26 (83.9) | 5 (16.1) | |
| IrAE toxicity | ||||
| No irAE | 66 (55.5) | 58 (87.9) | 7 (10.6) | |
| G1-2 | 37 (31.1) | 28 (75.7) | 9 (15.4) | 0.126 |
| G3-4 | 16 (13.4) | 12 (75.0) | 4 (25.0) | |
| Brain metastases | ||||
| No | 94 (79.0) | 74 (78.7) | 19 (20.2) | 0.070 |
| Yes | 25 (21.0) | 24 (96.0) | 1 (4.0) | |
| Lactate dehydrogenase (LDH) | ||||
| Normal LDH | 110 (92.4) | 90 (81.8) | 19 (17.3) | 0.706 |
| Elevated LDH | 9 (7.6) | 8 (88.9) | 1 (11.1) | |
| BRAF | ||||
| Wild type | 88 (73.9) | 70 (79.5) | 17 (19.3) | 0.272 |
| Positive | 31 (26.1) | 28 (90.3) | 3 (9.7) | |
| Total sample (N = 31) | Non-responders (N = 28) | Responders (N = 3) | ||
| BRAF mutation genotype | ||||
| V600E | 22 (71.0) | 20 (90.9) | 2 (9.1) | 1.000 |
| V600K | 8 (25.8) | 7 (87.5) | 1 (12.5) | |
| V600 others | 1 (3.2) | 1 (100.0) | - | |
| Total Sample (N = 25) | Non-Responders (SD + PD) (N = 24) | Responders (CR + PR) (N = 1) | ||
|---|---|---|---|---|
| Brain metastases—Treatment | ||||
| Stereotaxy | 13 (52.0) | 12 (50.0) | 1 (100.0) | 0.916 |
| WBRT | 7 (28.0) | 7 (29.2) | - | |
| Both | 3 (12.0) | 3 (12.5) | - | |
| No treatment | 1 (4.0) | 1 (4.2) | - | |
| Operation | 1 (4.0) | 1 (4.2) | - |
| All Patients | BRAF Positive | BRAF Wild Type | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Responses | Total (N = 119) | First-Line Treatment (N = 81) | ≥Second- Line Treatment (N = 38) | Total N = 31 | First-Line Treatment (N = 7) | ≥Second-Line Treatment (N = 24) | Total (N = 88) | First-Line Treatment (N = 74) | ≥Second-Line Treatment (N = 14) |
| CR | 8 (6.72%) | 3 (3.7%) | 5 (13.15%) | 2 (6.45%) | 0 | 2 (8.33%) | 6 (6.81%) | 3 (4.05%) | 3 (21.42%) |
| PR | 12 (10.08%) | 11 (13.5%) | 1 (2.63%) | 1 (3.22%) | 0 | 1 (4.16%) | 11 (12.5%) | 11 (14.86%) | 0 |
| SD | 42 (35.28%) | 28 (34.56%) | 14 (36.84%) | 10 (32.2%) | 1 (14.28%) | 9 (37.5%) | 32 (36.36%) | 27 (36.48%) | 5 (35.71%) |
| PD | 56 (47.04%) | 38 (46.9%) | 18 (47.36%) | 18 (58.06%) | 6 (85.71%) | 12 (50%) | 38 (43.18%) | 32 (43.24%) | 6 (42.85%) |
| NE | 1 (0.84%) | 1 (1.23%) | 0 | 0 | 0 | 0 | 1 (1.13%) | 1 (1.35%) | 0 |
| DCR * | 52.08% | 51.76% | 52.62% | 41.87% | 14.28% | 49.99% | 55.67% | 55.39% | 35.71% |
| ORR ** | 16.8% | 17.2% | 15.78% | 9.67% | 14.28% | 12.49% | 19.31% | 18.91% | 21.42% |
| N | Median OS (Weeks) | LCI | UCI | p-Values (Log-Rank) | Median PFS (Weeks) | LCI | UCI | p-Values (Log-Rank) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| All patients (median) | 119 | 130.29 | 81.02 | 179.57 | - | 54.86 | 19.75 | 89.97 | - | |
| Age (years) | <70 | 62 | 135.14 | 81.05 | 189.23 | 0.324 | 54.57 | 1.75 | 107.40 | 0.982 |
| ≥70 | 57 | 86.00 | 8.31 | 163.69 | 54.86 | 17.97 | 91.75 | |||
| Gender | Male | 68 | 139.43 | 58.53 | 220.33 | 0.304 | 97.14 | 14.38 | 179.90 | 0.139 |
| Female | 51 | 77.29 | 36.17 | 118.42 | 46.86 | 27.59 | 66.13 | |||
| T | ptx or occult primary tumor | 35 | 229.430 | 86.48 | 372.38 | 0.020 | 143.86 | 0.00 | 293.85 | 0.003 |
| pT1a | 3 | 86.00 | 22.68 | 149.33 | 43.14 | 36.29 | 49.99 | |||
| pT2a | 6 | 24.00 | 16.80 | 31.20 | 13.86 | 7.34 | 20.38 | |||
| pT2b | 5 | 142.86 | - | - | 30.57 | 0.00 | 69.82 | |||
| pT3a | 9 | - | - | - | 54.00 | 48.57 | 59.44 | |||
| pT3b | 16 | 48.43 | 0.00 | 145.11 | 35.71 | 19.76 | 51.66 | |||
| pT4a | 9 | - | - | - | 80.43 | 0.00 | 190.64 | |||
| TIL | Unknown | 74 | 86.00 | 42.27 | 129.73 | 0.381 | 42.71 | 26.02 | 59.40 | 0.285 |
| Brisk | 15 | 229.43 | 9.08 | 449.78 | 229.43 | 0.00 | 502.56 | |||
| Non-brisk | 12 | 142.86 | 15.73 | 269.99 | 80.43 | - | - | |||
| Absent | 18 | - | - | - | 97.14 | - | - | |||
| N | No | 57 | 139.43 | 36.68 | 242.18 | 0.289 | 87.57 | 33.31 | 141.83 | 0.179 |
| Yes | 58 | 103.14 | 22.90 | 183.38 | 43.00 | 22.75 | 63.26 | |||
| Unknown | 4 | 32.14 | 27.24 | 37.04 | 17.29 | 5.11 | 29.47 | |||
| M AJCC 8th edition | M0 | 1 | 61.71 | - | - | 0.109 | 27.14 | - | - | 0.085 |
| M1a | 22 | 57.00 | 16.54 | 97.47 | 37.86 | 21.45 | 54.27 | |||
| M1b | 15 | - | - | - | - | - | - | |||
| M1c | 56 | 178.57 | 86.87 | 270.27 | 107.43 | 0.00 | 228.49 | |||
| M1d | 25 | 52.57 | 0.00 | 134.24 | 35.29 | 13.53 | 57.05 | |||
| Line of treatment | First | 81 | 94.14 | 33.01 | 155.27 | 0.596 | 46.86 | 30.03 | 63.69 | 0.175 |
| Second + third | 38 | 178.57 | 20.51 | 336.63 | 172.00 | 0.00 | 382.17 | |||
| Treatment NA = 1 | Nivolumab | 52 | 86.00 | 19.33 | 152.68 | 0.358 | 43.14 | 23.74 | 62.54 | 0.606 |
| Pembrolizumab | 66 | 139.71 | 67.66 | 211.76 | 61.43 | 4.67 | 118.19 | |||
| irAE | No | 64 | 46.43 | 34.53 | 58.33 | <0.001 | 27.86 | 19.92 | 35.80 | <0.001 |
| IrAE = 1 | 24 | 142.86 | 52.49 | 233.23 | 107.43 | 0.00 | 245.26 | |||
| >1 IrAE | 31 | 258.00 | - | - | - | - | - | |||
| BRAF | Wild-type | 88 | 130.29 | 80.80 | 179.78 | 0.161 | 58.14 | 19.19 | 97.09 | 0.462 |
| Positive | 31 | 71.71 | 0.00 | 172.50 | 35.29 | 0.00 | 82.81 | |||
| Brain metastases | No | 94 | 135.14 | 57.31 | 212.97 | 0.259 | 61.00 | 4.44 | 117.56 | 0.063 |
| Yes | 25 | 71.71 | 0.00 | 169.70 | 36.00 | 7.57 | 64.43 | |||
| Response of the treatments | PD + SD | 98 | 71.71 | 40.01 | 103.42 | <0.001 | 42.14 | 31.64 | 52.64 | <0.001 |
| CR + PR | 20 | - | - | - | - | - | - | |||
| Received radiation therapy | No | 86 | 86.00 | 21.93 | 150.07 | 0.010 | 43.14 | 22.36 | 63.92 | 0.326 |
| Yes | 33 | - | - | - | 80.43 | 25.14 | 135.72 | |||
| BRAF-wild type (n = 88) | ||||||||||
| Line of treatment | First | 74 | 103.14 | 41.07 | 165.21 | 0.392 | 57.00 | 19.62 | 94.38 | 0.218 |
| Second + third | 14 | 229.43 | 43.62 | 415.25 | 229.43 | - | - | |||
| BRAF V600 mutation (n = 31) | ||||||||||
| Line of treatment | First | 7 | 69.14 | 0.00 | 159.09 | 0.312 | 12.29 | 6.77 | 17.81 | 0.022 |
| Second + third | 24 | 71.71 | 0.00 | 222.94 | 61.43 | 0.00 | 225.52 | |||
| Survival | Progression-Free Survival | |||
|---|---|---|---|---|
| HR for Death (OS) (95% CI) | p-Value | HR for Progression-Free (PFS) (95% CI) | p-Value | |
| Age group/70 years+ | 1.66 (0.96–2.88) | 0.072 | 1.12 (0.67–1.86) | 0.675 |
| Gender/female | 1.16 (0.69–1.96) | 0.570 | 1.23 (0.74–2.02) | 0.423 |
| Line of treatment/advanced setting | 1.04 (0.53–2.06) | 0.906 | 0.50 (0.24–1.03) | 0.060 |
| IrAE | 0.000 | 0.000 | ||
| IrAE = 1 | 0.31 (0.14–0.65) | 0.002 | 0.31 (0.15–0.62) | 0.001 |
| IrAE > 1 | 0.21 (0.10–0.44) | 0.000 | 0.17 (0.08–0.35) | 0.000 |
| M | 0.119 | 0.501 | ||
| M/M1a | 0.38 (0.04–3.27) | 0.375 | 0.34 (0.04–2.91) | 0.325 |
| M/M1b | 0.10 (0.01–1.08) | 0.058 | 0.16 (0.02–1.63) | 0.123 |
| M/M1c | 0.26 (0.03–2.26) | 0.221 | 0.27 (0.03–2.33) | 0.232 |
| M/M1d | 0.41 (0.02–8.94) | 0.567 | 0.21 (0.01–4.35) | 0.312 |
| BRAF/positive | 1.96 (1.02–3.77) | 0.044 | 2.68 (1.26–5.72) | 0.011 |
| Brain metastases/yes | 0.84 (0.09–7.73) | 0.880 | 1.62 (0.18–14.25) | 0.666 |
| Therapy responses/CR + PR | 0.14 (0.05–0.43) | 0.001 | 0.09 (0.03–0.30) | 0.000 |
| Grade of irAE | 0.154 | 0.105 | ||
| Grade of irAE/G1-G2 | 0.26 (0.05–1.40) | 0.116 | 0.32 (0.06–1.72) | 0.184 |
| Grade of irAE/G3-G4 | 0.14 (0.02–1.03) | 0.053 | 0.11 (0.01–0.89) | 0.038 |
| Received radiation therapy/yes | 0.48 (0.24–0.98) | 0.043 | 0.85 (0.47–1.51) | 0.573 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuzmanovszki, D.; Kiss, N.; Tóth, B.; Kerner, T.; Tóth, V.; Szakonyi, J.; Lőrincz, K.; Hársing, J.; Imrédi, E.; Pfund, A.; et al. Anti-PD-1 Monotherapy in Advanced Melanoma—Real-World Data from a 77-Month-Long Retrospective Observational Study. Biomedicines 2022, 10, 1737. https://doi.org/10.3390/biomedicines10071737
Kuzmanovszki D, Kiss N, Tóth B, Kerner T, Tóth V, Szakonyi J, Lőrincz K, Hársing J, Imrédi E, Pfund A, et al. Anti-PD-1 Monotherapy in Advanced Melanoma—Real-World Data from a 77-Month-Long Retrospective Observational Study. Biomedicines. 2022; 10(7):1737. https://doi.org/10.3390/biomedicines10071737
Chicago/Turabian StyleKuzmanovszki, Daniella, Norbert Kiss, Béla Tóth, Tünde Kerner, Veronika Tóth, József Szakonyi, Kende Lőrincz, Judit Hársing, Eleonóra Imrédi, Alexa Pfund, and et al. 2022. "Anti-PD-1 Monotherapy in Advanced Melanoma—Real-World Data from a 77-Month-Long Retrospective Observational Study" Biomedicines 10, no. 7: 1737. https://doi.org/10.3390/biomedicines10071737
APA StyleKuzmanovszki, D., Kiss, N., Tóth, B., Kerner, T., Tóth, V., Szakonyi, J., Lőrincz, K., Hársing, J., Imrédi, E., Pfund, A., Szabó, Á., Brodszky, V., Rencz, F., & Holló, P. (2022). Anti-PD-1 Monotherapy in Advanced Melanoma—Real-World Data from a 77-Month-Long Retrospective Observational Study. Biomedicines, 10(7), 1737. https://doi.org/10.3390/biomedicines10071737