
Elevated Pre- and Postoperative ROTEM™ Clot Lysis Indices Indicate Reduced Clot Retraction and Increased Mortality in Patients Undergoing Liver Transplantation



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Data
2.2. Procedures
2.3. Statistics
3. Results
3.1. Patient Characteristics
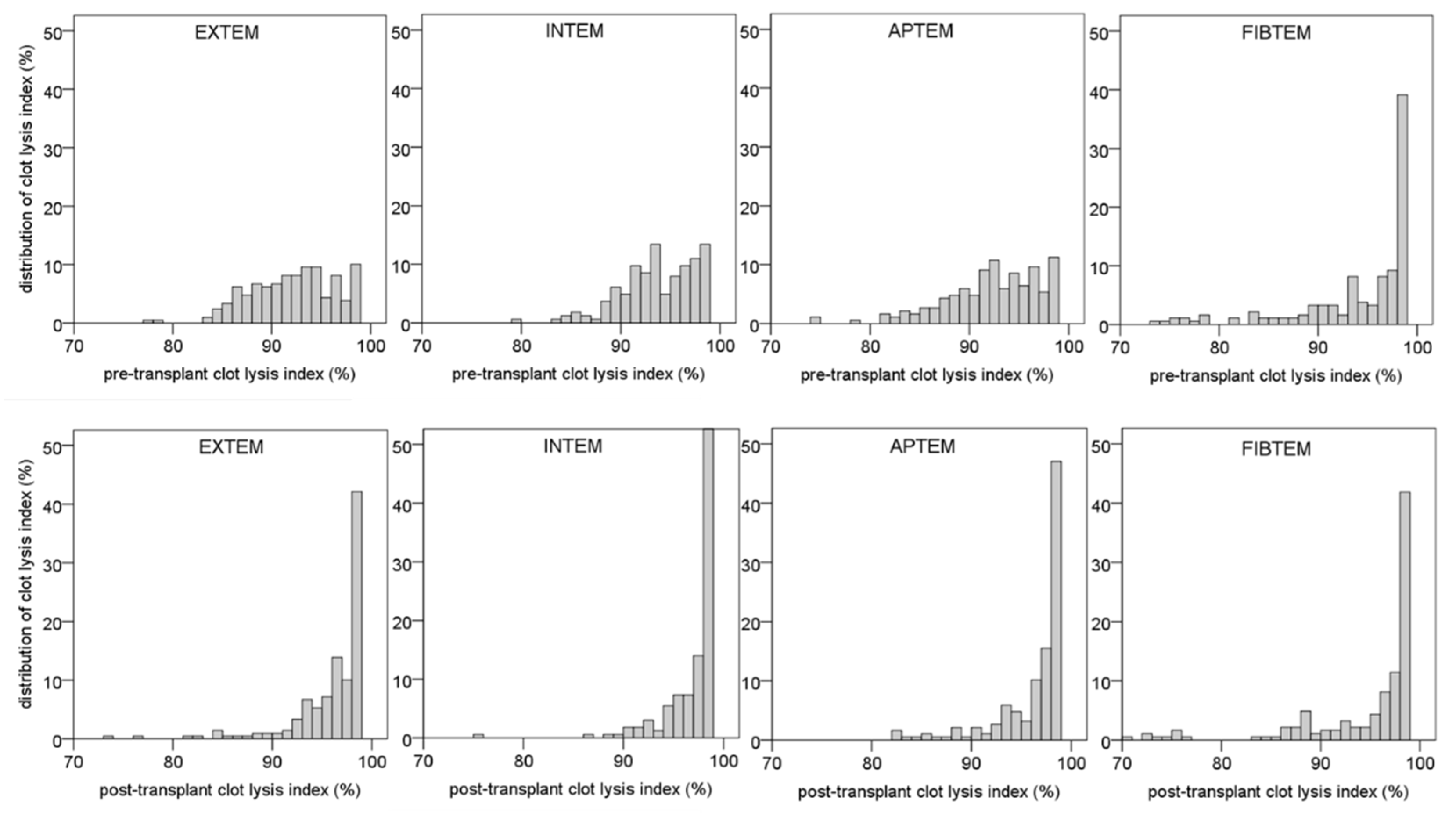
3.2. Distribution of Pre-Transplantation Clot Lysis Index
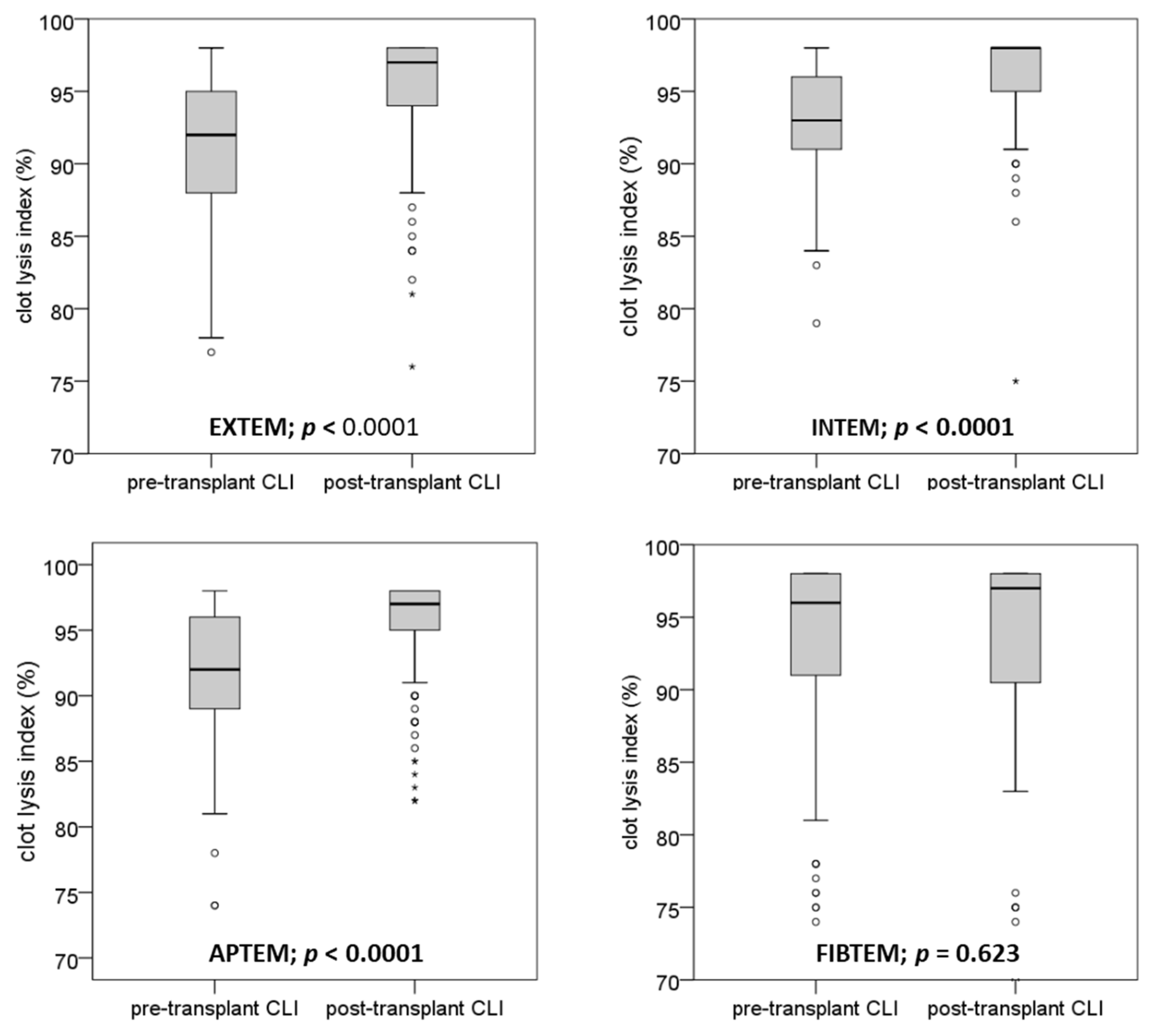
3.3. Distribution of Post-Transplantation Clot Lysis Index
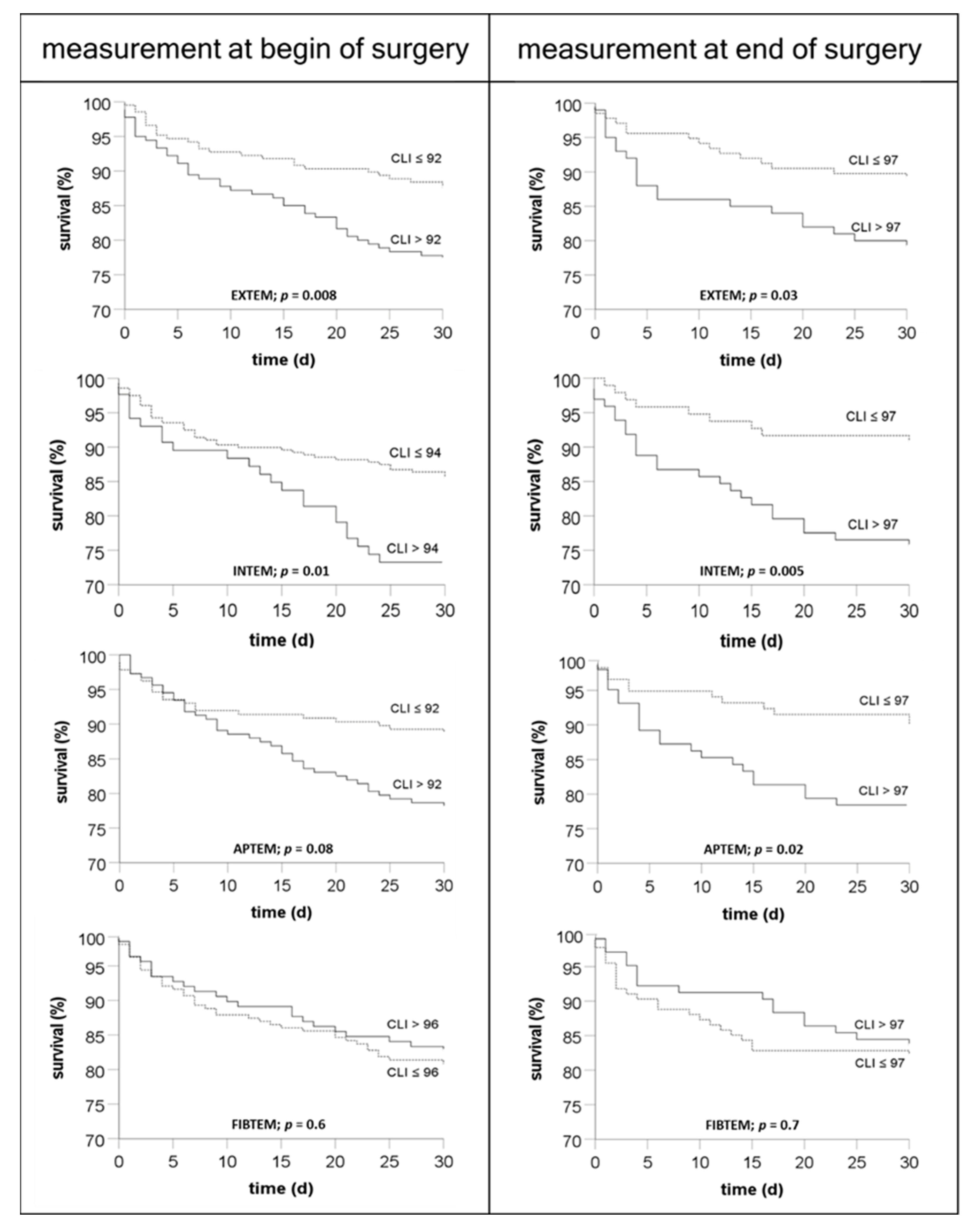
3.4. Association of Clot Lysis Index at the Beginning and the End of Transplantation with Mortality
3.5. Correlation of Pre-Transplantation Clot Lysis Index with Other Laboratory Findings
3.6. Correlation of the Post-Transplant Clot Lysis Index with Blood Products
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Biancofiore, G.; Blasi, A.; De Boer, M.T.; Franchini, M.; Hartmann, M.; Lisman, T.; Liumbruno, G.M.; Porte, R.J.; Saner, F.; Senzolo, M.; et al. Perioperative hemostatic management in the cirrhotic patient: A position paper on behalf of the Liver Intensive Care Group of Europe (LICAGE). Minerva Anestesiol. 2019, 85, 782–798. [Google Scholar] [CrossRef] [PubMed]
- Bezinover, D.; Dirkmann, D.; Findlay, J.; Guta, C.; Hartmann, M.; Nicolau-Raducu, R.; Mukhtar, A.M.; Moguilevitch, M.; Pivalizza, E.; Rosenfeld, D.; et al. Perioperative Coagulation Management in Liver Transplant Recipients. Transplantation 2018, 102, 578–592. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, M.; Szalai, C.; Saner, F.H. Hemostasis in liver transplantation: Pathophysiology, monitoring, and treatment. World J. Gastroenterol. 2016, 22, 1541–1550. [Google Scholar] [CrossRef] [PubMed]
- Simurda, T.; Casini, A.; Stasko, J.; Hudecek, J.; Skornova, I.; Vilar, R.; Neerman-Arbez, M.; Kubisz, P. Perioperative management of a severe congenital hypofibrinogenemia with thrombotic phenotype. Thromb. Res. 2020, 188, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Simurda, T.; Asselta, R.; Zolkova, J.; Brunclikova, M.; Dobrotova, M.; Kolkova, Z.; Loderer, D.; Skornova, I.; Hudecek, J.; Lasabova, Z.; et al. Congenital Afibrinogenemia and Hypofibrinogenemia: Laboratory and Genetic Testing in Rare Bleeding Disorders with Life-Threatening Clinical Manifestations and Challenging Management. Diagnostics 2021, 11, 2140. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, M.; Craciun, B.; Paul, A.; Brenner, T.; Saner, F.H. Pre-Liver Transplant ROTEM™ Clot Lysis Index Is Associated with 30-Day Mortality, But Is Not a Measure for Fibrinolysis. J. Clin. Med. 2020, 9, 3298. [Google Scholar] [CrossRef] [PubMed]
- Nicolau-Raducu, R.; Beduschi, T.; Vianna, R.; Diez, C.; Sleem, M.; Singh, B.P.; Vasileiou, G.; Raveh, Y. Fibrinolysis Shutdown Is Associated with Thrombotic and Hemorrhagic Complications and Poorer Outcomes After Liver Transplantation. Liver Transpl. 2019, 25, 380–387. [Google Scholar] [CrossRef]
- Adamzik, M.; Langemeier, T.; Frey, U.H.; Görlinger, K.; Saner, F.; Eggebrecht, H.; Peters, J.; Hartmann, M. Comparison of thrombelastometry with simplified acute physiology score II and sequential organ failure assessment scores for the prediction of 30-day survival: A cohort study. Shock 2011, 35, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, F.C.F.; Manolov, V.; Morgenstern, J.; Fleming, T.; Heitmeier, S.; Uhle, F.; Al-Saeedi, M.; Hackert, T.; Bruckner, T.; Schöchl, H.; et al. Acute fibrinolysis shutdown occurs early in septic shock and is associated with increased morbidity and mortality: Results of an observational pilot study. Ann. Intensive Care 2019, 9, 19. [Google Scholar] [CrossRef] [PubMed]
- Moore, H.B.; Moore, E.E.; Liras, I.N.; Gonzalez, E.; Harvin, J.A.; Holcomb, J.B.; Sauaia, A.; Cotton, B.A. Acute Fibrinolysis Shutdown after Injury Occurs Frequently and Increases Mortality: A Multicenter Evaluation of 2,540 Severely Injured Patients. J. Am. Coll. Surg. 2016, 222, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Moore, H.B.; Moore, E.E.; Neal, M.D.; Sheppard, F.R.; Kornblith, L.Z.; Draxler, D.F.; Walsh, M.; Medcalf, R.L.; Cohen, M.J.; Cotton, B.A.; et al. Fibrinolysis Shutdown in Trauma: Historical Review and Clinical Implications. Anesth. Analg. 2019, 129, 762–773. [Google Scholar] [CrossRef]
- Nelson, J.T.; Coleman, J.R.; Carmichael, H.; Mauffrey, C.; Vintimilla, D.R.; Samuels, J.M.; Sauaia, A.; Moore, E.E. High Rate of Fibrinolytic Shutdown and Venous Thromboembolism in Patients with Severe Pelvic Fracture. J. Surg. Res. 2020, 246, 182–189. [Google Scholar] [CrossRef]
- Madoiwa, S.; Nunomiya, S.; Ono, T.; Shintani, Y.; Ohmori, T.; Mimuro, J.; Sakata, Y. Plasminogen activator inhibitor 1 promotes a poor prognosis in sepsis-induced disseminated intravascular coagulation. Int. J. Hematol. 2006, 84, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, M.; Walde, C.; Dirkmann, D.; Saner, F.H. Safety of coagulation factor concentrates guided by ROTEM™-analyses in liver transplantation: Results from 372 procedures. BMC Anesthesiol. 2019, 19, 97. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.A.; McNeil, J.; Abuelkasem, E. Clot Retraction: Lost in Interpretation? Anesth. Analg. 2019, 128, e53–e54. [Google Scholar] [CrossRef] [PubMed]
- Jansen, E.E.; Hartmann, M. Clot Retraction: Cellular Mechanisms and Inhibitors. Meas. Methods Clin. Implications. Biomed. 2021, 9, 1064. [Google Scholar] [CrossRef]
- Jansen, E.E.; Braun, A.; Jansen, P.; Hartmann, M. Platelet-Therapeutics to Improve Tissue Regeneration and Wound Healing-Physiological Background and Methods of Preparation. Biomedicines 2021, 9, 869. [Google Scholar] [CrossRef] [PubMed]
- Simm, V.; Dirkmann, D.; Peters, J.; Hartmann, M. Whole blood impedance aggregometry findings in experimental endotoxinemia. Crit. Care 2013, 17, 427. [Google Scholar] [CrossRef] [PubMed]
- Adamzik, M.; Görlinger, K.; Peters, J.; Hartmann, M. Whole blood impedance aggregometry as a biomarker for the diagnosis and prognosis of severe sepsis. Crit. Care. 2012, 16, R204. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease Leading to LTX | Cases | Percentage |
|---|---|---|
| alcohol | 38 | 20.3 |
| cholestatic diseases | 24 | 12.8 |
| hepatocellular carcinoma | 32 | 17.1 |
| hepatitis | 23 | 12.3 |
| re-transplant | 14 | 7.5 |
| inherited diseases | 13 | 7.0 |
| non-alcoholic steatohepatitis | 12 | 6.4 |
| acute liver failure | 11 | 5.9 |
| autoimmune diseases | 7 | 3.7 |
| biliary atresia | 5 | 2.7 |
| intoxication | 3 | 1.6 |
| tumor | 3 | 1.6 |
| cryptogenic | 2 | 1.1 |
| ROTEM | EXTEM | INTEM | FIBTEM | APTEM |
|---|---|---|---|---|
| CT | 0.133 | 0.089 | 0.02 | 0.005 |
| Alpha | 0.153 * | 0.082 | 0.03 | −0.022 |
| CFT | −0.073 | −0.235 * | 0.148 | −0.011 |
| MCF | −0.202 * | −0.246 * | 0.151 | −0.049 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hartmann, M.; Lorenz, B.; Brenner, T.; Saner, F.H. Elevated Pre- and Postoperative ROTEM™ Clot Lysis Indices Indicate Reduced Clot Retraction and Increased Mortality in Patients Undergoing Liver Transplantation. Biomedicines 2022, 10, 1975. https://doi.org/10.3390/biomedicines10081975
Hartmann M, Lorenz B, Brenner T, Saner FH. Elevated Pre- and Postoperative ROTEM™ Clot Lysis Indices Indicate Reduced Clot Retraction and Increased Mortality in Patients Undergoing Liver Transplantation. Biomedicines. 2022; 10(8):1975. https://doi.org/10.3390/biomedicines10081975
Chicago/Turabian StyleHartmann, Matthias, Benedikt Lorenz, Thorsten Brenner, and Fuat H. Saner. 2022. "Elevated Pre- and Postoperative ROTEM™ Clot Lysis Indices Indicate Reduced Clot Retraction and Increased Mortality in Patients Undergoing Liver Transplantation" Biomedicines 10, no. 8: 1975. https://doi.org/10.3390/biomedicines10081975
APA StyleHartmann, M., Lorenz, B., Brenner, T., & Saner, F. H. (2022). Elevated Pre- and Postoperative ROTEM™ Clot Lysis Indices Indicate Reduced Clot Retraction and Increased Mortality in Patients Undergoing Liver Transplantation. Biomedicines, 10(8), 1975. https://doi.org/10.3390/biomedicines10081975