
Quantitative Measurement of Spinal Cerebrospinal Fluid by Cascade Artificial Intelligence Models in Patients with Spontaneous Intracranial Hypotension



Abstract
:1. Introduction
2. Materials and Methods
2.1. Enrolled Subjects
2.2. Neuroimaging Acquisition
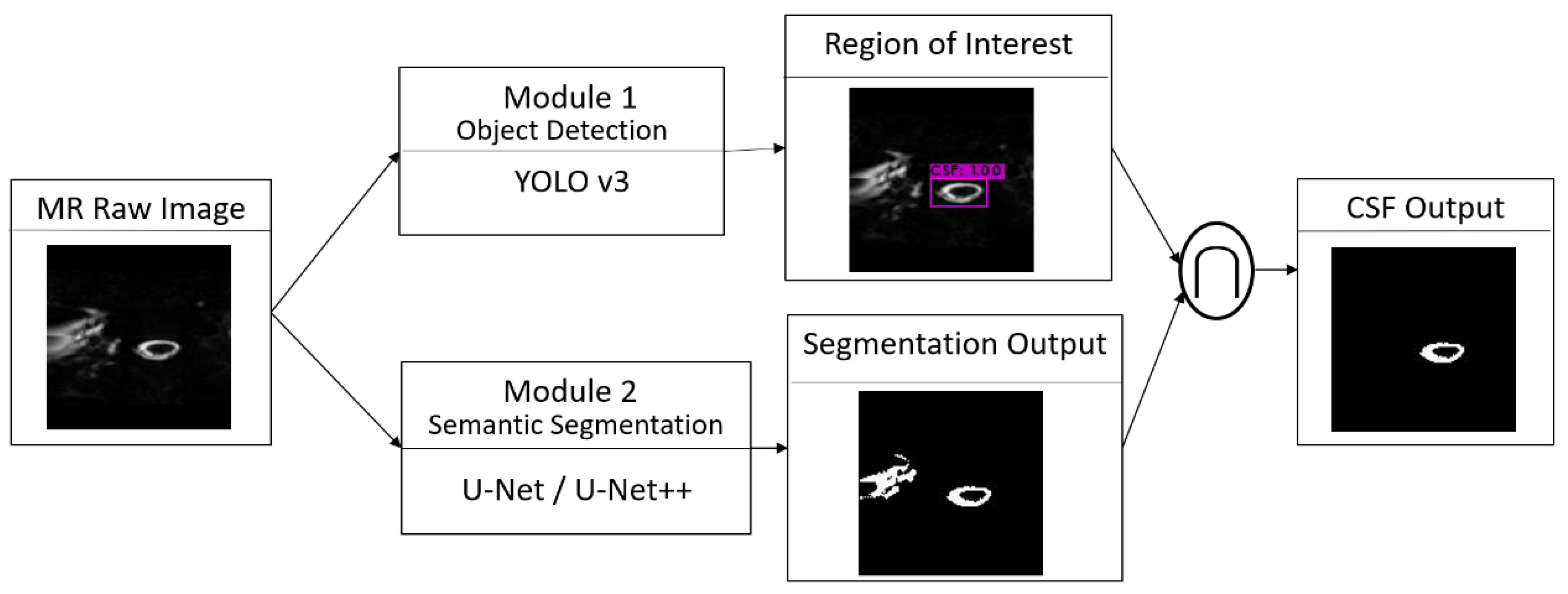
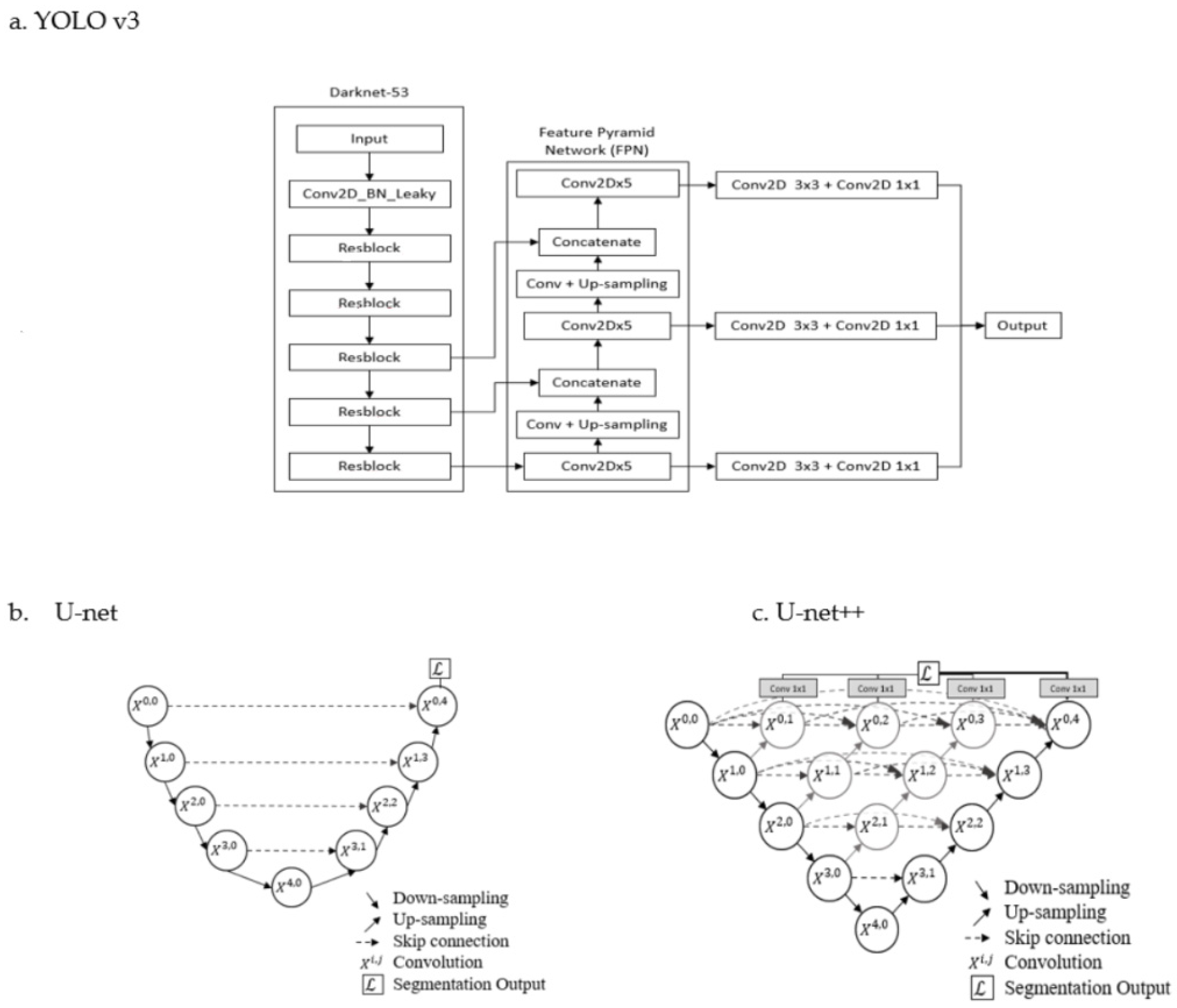
2.3. Object Detection and Semantic Segmentation of Spinal CSF
2.4. Performance Evaluation
2.5. Spinal CSF Quantification in Cohort Study
2.6. Statistical Analysis
3. Results
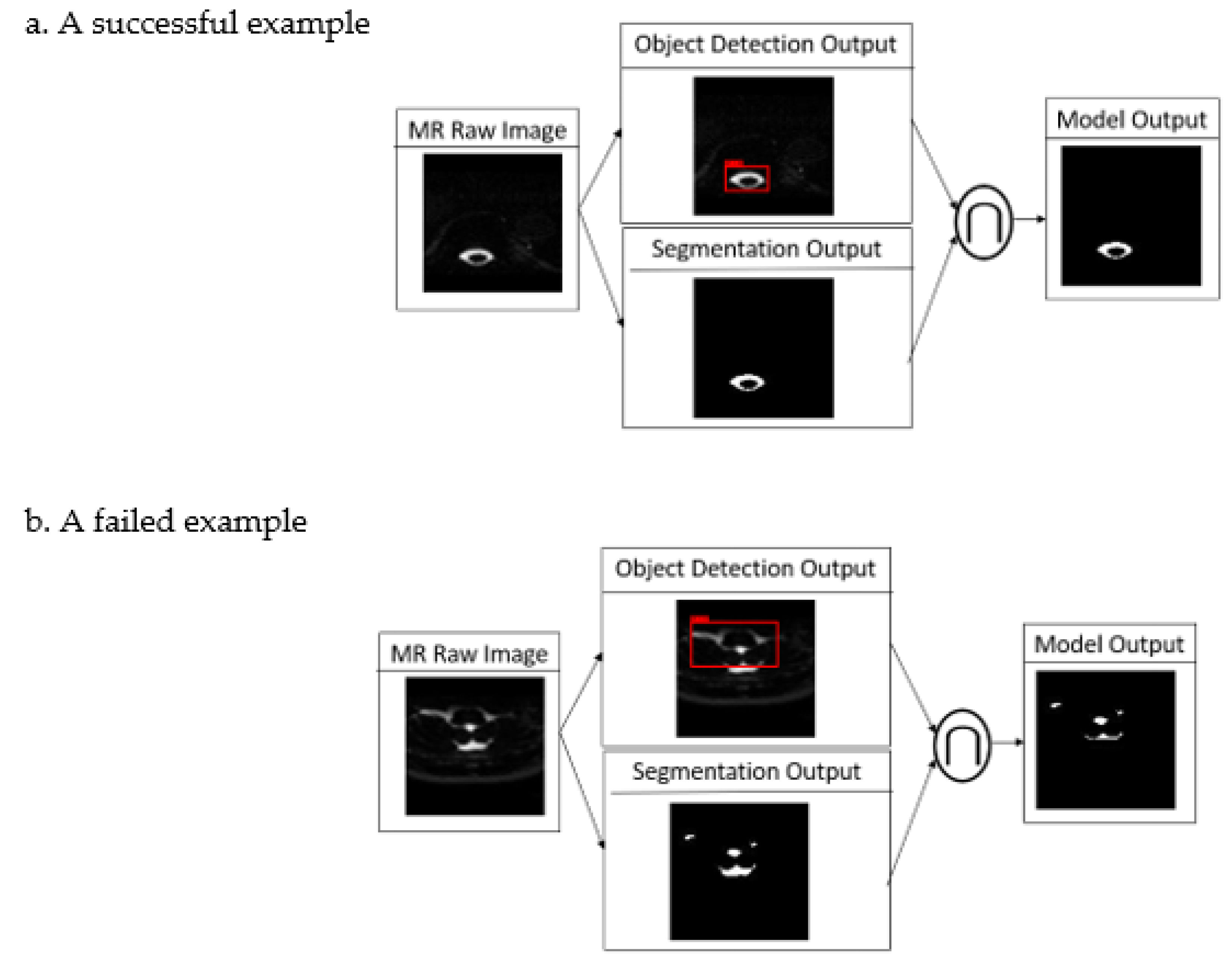
3.1. Object Detection and Semantic Segmentation of Spinal CSF
3.2. Cohort Study
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schievink, W.I.; Maya, M.M.; Louy, C.; Moser, F.G.; Tourje, J. Diagnostic criteria for spontaneous spinal CSF leaks and intracranial hypotension. AJNR Am. J. Neuroradiol. 2008, 29, 853–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013, 33, 629–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, H.M.; Kim, S.J.; Choi, C.G.; Lee, D.H.; Lee, J.H.; Suh, D.C.; Choi, J.W.; Jeong, K.S.; Chung, S.J.; Kim, J.S.; et al. Detection of CSF leak in spinal CSF leak syndrome using MR myelography: Correlation with radioisotope cisternography. AJNR Am. J. Neuroradiol. 2008, 29, 649–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.H.; Chen, J.H.; Chen, H.C.; Chai, J.W.; Chen, P.L.; Chen, C.C. Patterns of cerebrospinal fluid (CSF) distribution in patients with spontaneous intracranial hypotension: Assessed with magnetic resonance myelography. J. Chin. Med. Assoc. 2017, 80, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schievink, W.I. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. JAMA 2006, 295, 2286–2296. [Google Scholar] [CrossRef] [PubMed]
- Mokri, B. Spontaneous intracranial hypotension. Curr. Neurol. Neurosci. Rep. 2001, 1, 109–117. [Google Scholar] [CrossRef]
- Mokri, B. The Monro-Kellie hypothesis: Applications in CSF volume depletion. Neurology 2001, 56, 1746–1748. [Google Scholar] [CrossRef]
- Wu, J.W.; Hseu, S.S.; Fuh, J.L.; Lirng, J.F.; Wang, Y.F.; Chen, W.T.; Chen, S.P.; Wang, S.J. Factors predicting response to the first epidural blood patch in spontaneous intracranial hypotension. Brain 2017, 140, 344–352. [Google Scholar] [CrossRef]
- Chen, H.C.; Chai, J.W.; Wu, C.C.; Chen, P.L.; Teng, C.L. Magnetic resonance imaging predicted the therapeutic response of patients with spinal cerebrospinal fluid leakage undergoing targeted epidural blood patch. Br. J. Radiol. 2022, 95, 20210841. [Google Scholar] [CrossRef]
- Chen, H.C.; Chen, P.L.; Tsai, Y.H.; Chen, C.H.; Chen, C.C.; Chai, J.W. Quantitative Measurement of CSF in Patients with Spontaneous Intracranial Hypotension. AJNR Am. J. Neuroradiol. 2017, 38, 1061–1067. [Google Scholar] [CrossRef] [Green Version]
- Krizhevsky A, Sutskever I, Hinton GE, Image net classification with deep convolutional neural networks. Adv. Neural Inf. Process Syst. 2012, 5, 1106–1114. [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Medical Image Computing and Computer-Assisted Intervention–MICCAI 2015; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar] [CrossRef]
- Siddique, N.; Paheding, S.; Elkin, C.P.; Devabhaktuni, V. U-net and its variants for medical image segmentation: A review of theory and applications. IEEE Access 2021, 9, 82031–82057. [Google Scholar] [CrossRef]
- Paugam, F.; Lefeuvre, J.; Perone, C.S.; Gros, C.; Reich, D.S.; Sati, P.; Cohen-Adad, J. Open-source pipeline for multi-class segmentation of the spinal cord with deep learning. Magn. Reason. Imaging 2019, 64, 21–27. [Google Scholar] [CrossRef] [PubMed]
- AskariHemmat, M.H.; Honari, S.; Rouhier, L.; Perone, C.S.; Cohen-Adad, J.; Savaria, Y.; David, J.P. U-net fixed-point quantization for medical image segmentation. In Large-Scale Annotation of Biomedical Data and Expert Label Synthesis and Hardware Aware Learning for Medical Imaging and Computer Assisted Intervention; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2019; Volume 11851. [Google Scholar] [CrossRef] [Green Version]
- Redmon, J.; Divvala, S.; Girshick, R.; Farhadi, A. You only look once: Unified, real-time object detection. arXiv 2015. [Google Scholar] [CrossRef] [Green Version]
- Lo, C.M.; Hung, P.H.; Lin, D.T. Rapid Assessment of Acute Ischemic Stroke by Computed Tomography Using Deep Convolutional Neural Networks. J. Digit. Imaging 2021, 34, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Siddiquee, M.M.R.; Tajbakhsh, N.; Liang, J. UNet++: Redesigning Skip Connections to Exploit Multiscale Features in Image Segmentation. IEEE Trans. Med. Imaging 2020, 39, 1856–1867. [Google Scholar] [CrossRef] [Green Version]
- Redmon, K.; Farhadi, A. YOLOv3: An Incremental Improvement. arXiv 2018. Available online: https://arxiv.org/abs/1804.02767v1 (accessed on 5 August 2022).
- Lawal, M.O. Tomato detection based on modified YOLOv3 framework. Sci. Rep. 2021, 1447, 1–11. [Google Scholar] [CrossRef]
- Fan, K.J. Applications of U-Net to Cerebrospinal Fluid Segmentation in Magnetic Resonance Imaging. Mater’s Thesis, National Yunlin University of Science and Technology, Douliu City, Taiwan. 2019. Available online: https://hdl.handle.net/11296/yy99k8 (accessed on 1 May 2022).
- Jaeger, P.F.; Kohl, S.A.A.; Bickelhaupt, S.; Isensee, F.; Kuder, T.A.; Schlemmer, H.P.; Maier-Hein, K.H. Retina U-net: Embarrassingly simple exploitation segmentation supervision for medical object detection. arXiv 2019. [Google Scholar] [CrossRef]
- Ku, S.Y. Applications of 3D Context Retina U-net to Cerebrospinal Fluid Segmentation and Quantification in Magnetic Resonance Imaging. Master’s Thesis, National Yunlin University of Science and Technology, Douliu City, Taiwan, 2020. Available online: https://hdl.handle.net/11296/762zzz (accessed on 1 May 2022).
- Huang, H.X.; Tang, X.D.; Wen, F.; Jin, X. Small object detection method with shallow feature fusion network for chip surface defect detection. Sci. Rep. 2022, 12, 3914. [Google Scholar] [CrossRef]
- Lee, R.R.; Abraham, R.A.; Quinn, C.B. Dynamic physiologic changes in lumbar CSF volume quantitatively measured by three-dimensional fast spin-echo MRI. Spine 2001, 26, 1172–1178. [Google Scholar] [CrossRef]
- Higuchi, H.; Adachi, Y.; Kazama, T. The influence of lumbosacral cerebrospinal fluid volume on extent and duration of hyperbaric bupivacaine spinal anesthesia: A comparison between seated and lateral decubitus injection positions. Anesth. Analg. 2005, 101, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.M.; Chen, H.C.; Chen, C.C.; Chang, Y.C.; Wu, Y.Y.; Chen, W.H.; Sung, C.C.; Chai, J.W.; Lee, S.K. Comparison of Multispectral Image-Processing Methods for Brain Tissue Classification in BrainWeb Synthetic Data and Real MR Images. Biomed. Res. Int. 2021, 2021, 9820145. [Google Scholar] [CrossRef] [PubMed]
- Alperin, N.; Bagci, A.M.; Lee, S.H.; Lam, B.L. Automated Quantitation of Spinal CSF Volume and Measurement of Craniospinal CSF Redistribution following Lumbar Withdrawal in Idiopathic Intracranial Hypertension. AJNR Am. J. Neuroradiol. 2016, 37, 1957–1963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebret, A.; Hodel, J.; Rahmouni, A.; Decq, P.; Petit, E. Cerebrospinal fluid volume analysis for hydrocephalus diagnosis and clinical research. Comput. Med. Imaging Graph. 2013, 37, 224–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edsbagge, M.; Starck, G.; Zetterberg, H.; Ziegelitz, D.; Wikkelso, C. Spinal cerebrospinal fluid volume in healthy elderly individuals. Clin. Anat. 2011, 24, 733–740. [Google Scholar] [CrossRef]
- Hogan, Q.H.; Prost, R.; Kulier, A.; Taylor, M.L.; Liu, S.; Mark, L. Magnetic resonance imaging of cerebrospinal fluid volume and the influence of body habitus and abdominal pressure. Anesthesiology 1996, 84, 1341–1349. [Google Scholar] [CrossRef]
- Sullivan, J.T.; Grouper, S.; Walker, M.T.; Parrish, T.B.; McCarthy, R.J.; Wong, C.A. Lumbosacral cerebrospinal fluid volume in humans using three-dimensional magnetic resonance imaging. Anesth. Analg. 2006, 103, 1306–1310. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Training and Validation Dataset | Test Dataset | Cohort Study | ||
|---|---|---|---|---|---|
| Patients | HVs | Patients | HVs | Patients | |
| No. | 7 | 6 | 6 | 6 | 13 |
| Age (mean ± SD) | 45.14 ± 9.70 | 38.00 ± 9.70 | 41.17 ± 8.75 | 36.33 ± 6.09 | 43.57 ± 12.12 |
| Age range (years) | 30–61 | 30–57 | 30–53 | 29–46 | 22–61 |
| Male | 2 | 1 | 4 | 1 | 2 |
| Female | 5 | 5 | 2 | 5 | 11 |
| Algorithms | Mean of IoU | SD of IoU |
|---|---|---|
| Cascade Models—Integration of Object Detection Module and Semantic Segmentation Module | ||
| 1. U-net++ and YOLO v3 (YOLO v3 ∩ U-net++) | 0.9374 | 0.0159 |
| 2. U-net and YOLO v3 (YOLO v3 ∩ U-net) | 0.9373 | 0.0158 |
| Non-cascade Models—Semantic Segmentation Module Only | ||
| 1. U-net++ | 0.9102 | 0.0774 |
| 2. U-net | 0.9077 | 0.0799 |
| Algorithms | Mean | SD | 95% Confidence Int. | DoF | Sig. Level | Results | |
|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||||
| Cascade Models vs. Non-cascade Models | |||||||
| YOLO v3 U-net (IoU1) vs. U-net (IoU2) | 0.0303 | 0.0834 | 0.0288 | 0.0317 | 12,209 | 0.000 | Accept H1: IoU1 > IoU2 |
| YOLO v3 U-net++ (IoU1) vs. U-net++ (IoU2) | 0.0276 | 0.0811 | 0.0262 | 0.0291 | 12,209 | 0.000 | Accept H1: IoU1 > IoU2 |
| Comparison of Algorithms in Non-cascade Models | |||||||
| U-net++ (IoU1) vs. U-net (IoU2) | 0.0028 | 0.0351 | 0.0021 | 0.0034 | 12,209 | 0.000 | Accept H1: IoU1 > IoU2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, J.; Chai, J.-W.; Chen, P.-L.; Ding, Y.-W.; Chen, H.-C. Quantitative Measurement of Spinal Cerebrospinal Fluid by Cascade Artificial Intelligence Models in Patients with Spontaneous Intracranial Hypotension. Biomedicines 2022, 10, 2049. https://doi.org/10.3390/biomedicines10082049
Fu J, Chai J-W, Chen P-L, Ding Y-W, Chen H-C. Quantitative Measurement of Spinal Cerebrospinal Fluid by Cascade Artificial Intelligence Models in Patients with Spontaneous Intracranial Hypotension. Biomedicines. 2022; 10(8):2049. https://doi.org/10.3390/biomedicines10082049
Chicago/Turabian StyleFu, Jachih, Jyh-Wen Chai, Po-Lin Chen, Yu-Wen Ding, and Hung-Chieh Chen. 2022. "Quantitative Measurement of Spinal Cerebrospinal Fluid by Cascade Artificial Intelligence Models in Patients with Spontaneous Intracranial Hypotension" Biomedicines 10, no. 8: 2049. https://doi.org/10.3390/biomedicines10082049
APA StyleFu, J., Chai, J. -W., Chen, P. -L., Ding, Y. -W., & Chen, H. -C. (2022). Quantitative Measurement of Spinal Cerebrospinal Fluid by Cascade Artificial Intelligence Models in Patients with Spontaneous Intracranial Hypotension. Biomedicines, 10(8), 2049. https://doi.org/10.3390/biomedicines10082049