
The Silent Period for Small Fiber Sensory Neuropathy Assessment in a Mixed Cohort of Transthyretin-Mediated Amyloidosis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Neurophysiological Assessment
2.3. Statistics
3. Results
3.1. Demographic Data
3.2. Neurophysiological Assessments
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Russo, M.; Obici, L.; Bartolomei, I.; Cappelli, F.; Luigetti, M.; Fenu, S.; Cavallaro, T.; Chiappini, M.G.; Gemelli, C.; Pradotto, L.G.; et al. ATTRv amyloidosis Italian Registry: Clinical and epidemiological data. Amyloid 2020, 27, 259–265. [Google Scholar] [CrossRef]
- Luigetti, M.; Guglielmino, V.; Antonini, G.; Casali, C.; Ceccanti, M.; Chiappini, M.G.; De Giglio, L.; Di Lazzaro, V.; Di Muzio, A.; Goglia, M.; et al. ATTRv in Lazio-Italy: A High-Prevalence Region in a Non-Endemic Country. Genes 2021, 12, 829. [Google Scholar] [CrossRef]
- He, S.; Tian, Z.; Guan, H.; Li, J.; Fang, Q.; Zhang, S. Clinical characteristics and prognosis of Chinese patients with hereditary transthyretin amyloid cardiomyopathy. Orphanet J. Rare Dis. 2019, 14, 251. [Google Scholar] [CrossRef]
- Pinto, M.V.; Dyck, P.J.B.; Liewluck, T. Neuromuscular amyloidosis: Unmasking the master of disguise. Muscle Nerve 2021, 64, 23–36. [Google Scholar] [CrossRef]
- Reyners, A.K.; Hazenberg, B.P.; Haagsma, E.B.; Tio, R.A.; Reitsma, W.D.; Smit, A.J. The assessment of autonomic function in patients with systemic amyloidosis: Methodological considerations. Amyloid 1998, 5, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Sakashita, N.; Ando, Y.; Obayashi, K.; Terazaki, H.; Yamashita, T.; Takei, M.; Kinjo, M.; Takahashi, K. Familial amyloidotic polyneuropathy (ATTR Ser50Ile): The first autopsy case report. Virchows Arch. 2000, 436, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Papagianni, A.; Ihne, S.; Zeller, D.; Morbach, C.; Üçeyler, N.; Sommer, C. Clinical and apparative investigation of large and small nerve fiber impairment in mixed cohort of ATTR-amyloidosis: Impact on patient management and new insights in wild-type. Amyloid 2022, 29, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Kharoubi, M.; Roche, F.; Bézard, M.; Hupin, D.; Silva, S.; Oghina, S.; Chalard, C.; Zaroui, A.; Galat, A.; Guendouz, S.; et al. Prevalence and prognostic value of autonomic neuropathy assessed by Sudoscan® in transthyretin wild-type cardiac amyloidosis. ESC Heart Fail. 2020, 8, 1656–1665. [Google Scholar] [CrossRef] [PubMed]
- Noordzij, W.; Glaudemans, A.W.J.M.; Slart, R.H.J.A.; Dierckx, R.A.; Hazenberg, B.P.C. Clinical use of differential nuclear medicine modalities in patients with ATTR amyloidosis. Amyloid 2012, 19, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Gimelli, A.; Aimo, A.; Vergaro, G.; Genovesi, D.; Santonato, V.; Kusch, A.; Emdin, M.; Marzullo, P. Cardiac sympathetic denervation in wild-type transthyretin amyloidosis. Amyloid 2020, 27, 237–243. [Google Scholar] [CrossRef]
- Lefaucheur, J.-P.; Wahab, A.; Planté-Bordeneuve, V.; Sène, D.; Ménard-Lefaucheur, I.; Rouie, D.; Tebbal, D.; Salhi, H.; Créange, A.; Zouari, H.; et al. Diagnosis of small fiber neuropathy: A comparative study of five neurophysiological tests. Neurophysiol. Clin. 2015, 45, 445–455. [Google Scholar] [CrossRef]
- Conceição, I.; Costa, J.; Castro, J.; de Carvalho, M. Neurophysiological techniques to detect early small-fiber dysfunction in transthyretin amyloid polyneuropathy. Muscle Nerve 2014, 49, 181–186. [Google Scholar] [CrossRef]
- Bekircan-Kurt, C.E.; Yilmaz, E.; Arslan, D.; Yildiz, F.G.; Dikmetas, Ö.; Ergul-Ulger, Z.; Kocabeyoglu, S.; Irkec, M.; Hekimsoy, V.; Tokgozoglu, L.; et al. The functional and structural evaluation of small fibers in asymptomatic carriers of TTR p.Val50Met (Val30Met) mutation. Neuromuscul. Disord. 2022, 32, 50–56. [Google Scholar] [CrossRef]
- Inghilleri, M.; Cruccu, G.; Argenta, M.; Polidori, L.; Manfredi, M. Silent period in upper limb muscles after noxious cutaneous stimulation in man. Electroencephalogr. Clin. Neurophysiol. 1997, 105, 109–115. [Google Scholar] [CrossRef]
- Floeter, M.K. Cutaneous silent periods. Muscle Nerve 2003, 28, 391–401. [Google Scholar] [CrossRef]
- Kofler, M.; Leis, A.A.; Valls-Solé, J. Cutaneous silent periods-Part 1: Update on physiological mechanisms. Clin. Neurophysiol. 2019, 130, 588–603. [Google Scholar] [CrossRef]
- Kofler, M.; Leis, A.A.; Valls-Solé, J. Cutaneous silent periods-Part 2: Update on pathophysiology and clinical utility. Clin. Neurophysiol. 2019, 130, 604–615. [Google Scholar] [CrossRef]
- Gilio, F.; Bettolo, C.M.; Conte, A.; Iacovelli, E.; Frasca, V.; Serrao, M.; Giacomelli, E.; Gabriele, M.; Prencipe, M.; Inghilleri, M. Influence of the corticospinal tract on the cutaneous silent period: A study in patients with pyramidal syndrome. Neurosci. Lett. 2008, 433, 109–113. [Google Scholar] [CrossRef]
- Leis, A.A. Conduction abnormalities detected by silent period testing. Electroencephalogr. Clin. Neurophysiol. 1994, 93, 444–449. [Google Scholar] [CrossRef]
- Lopergolo, D.; Isak, B.; Gabriele, M.; Onesti, E.; Ceccanti, M.; Capua, G.; Fionda, L.; Biasiotta, A.; Di Stefano, G.; La Cesa, S.; et al. Cutaneous silent period recordings in demyelinating and axonal polyneuropathies. Clin. Neurophysiol. 2015, 126, 1780–1789. [Google Scholar] [CrossRef]
- Koytak, P.K.; Isak, B.; Borucu, D.; Uluc, K.; Tanridag, T.; Us, O. Assessment of symptomatic diabetic patients with normal nerve conduction studies: Utility of cutaneous silent periods and autonomic tests. Muscle Nerve 2011, 43, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Castro, J.; Swash, M.; de Carvalho, M. The cutaneous silent period in motor neuron disease. Clin. Neurophysiol. 2021, 132, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Tekatas, A.; Arican, O.; Guler, S.; Aynacı, O.; Dincer, N. Pruritus: Do Aδ fibers play a role? J. Dermatol. 2014, 41, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Stokic, D.S.; Kofler, M.; Stetkarova, I.; Leis, A.A. Exteroceptive suppression of voluntary activity in thenar muscles by cutaneous stimulation: How many trials should be averaged? Clin. Neurol. Neurosurg. 2019, 184, 105452. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.; Ando, Y.; Beirão, J.M.; Coelho, T.; Gertz, M.A.; Gillmore, J.D.; Hawkins, P.N.; Lousada, I.; Suhr, O.B.; Merlini, G. Expert consensus recommendations to improve diagnosis of ATTR amyloidosis with polyneuropathy. J. Neurol. 2021, 268, 2109–2122. [Google Scholar] [CrossRef] [PubMed]
- Ueda, M.; Ando, Y. Recent advances in transthyretin amyloidosis therapy. Transl. Neurodegener. 2014, 3, 19. [Google Scholar] [CrossRef]
- Koike, H.; Nakamura, T.; Hashizume, A.; Nishi, R.; Ikeda, S.; Kawagashira, Y.; Iijima, M.; Katsuno, M.; Sobue, G. Cardiac and peripheral vasomotor autonomic functions in late-onset transthyretin Val30Met familial amyloid polyneuropathy. J. Neurol. 2017, 264, 2293–2302. [Google Scholar] [CrossRef]
- Koike, H.; Tanaka, F.; Hashimoto, R.; Tomita, M.; Kawagashira, Y.; Iijima, M.; Fujitake, J.; Kawanami, T.; Kato, T.; Yamamoto, M.; et al. Natural history of transthyretin Val30Met familial amyloid polyneuropathy: Analysis of late-onset cases from non-endemic areas. J. Neurol. Neurosurg. Psychiatry 2012, 83, 152–158. [Google Scholar] [CrossRef]
- Kholová, I.; Kautzner, J. Current treatment in cardiac amyloidosis. Curr. Treat. Options Cardiovasc. Med. 2006, 8, 468–473. [Google Scholar] [CrossRef]
- Podnar, S.; Vodušek, D.B. Sexual dysfunction in patients with peripheral nervous system lesions. Handb. Clin. Neurol. 2015, 130, 179–202. [Google Scholar] [CrossRef]
- Holmgren, G.; Lundgren, H.-E.; Suhr, O.B. Successful pregnancies and fatherhood in familial amyloidotic polyneuropathy (FAP Val30Met) patients with liver transplantation. Amyloid 2004, 11, 125–129. [Google Scholar] [CrossRef]
- Obayashi, K.; Ando, Y.; Terazaki, H.; Yamashita, S.; Nakagawa, K.; Nakamura, M.; Yamashita, T.; Suga, M.; Ishizaki, T.; Uchino, M.; et al. Effect of sildenafil citrate (Viagra) on erectile dysfunction in a patient with familial amyloidotic polyneuropathy ATTR Val30Met. J. Auton. Nerv. Syst. 2000, 80, 89–92. [Google Scholar] [CrossRef]
- Alves, M.; Conceição, I.; Luis, M.L. Neurophysiological evaluation of sexual dysfunction in familial amyloidotic polyneuropathy--Portuguese type. Acta Neurol. Scand. 1997, 96, 163–166. [Google Scholar] [CrossRef]
- Nakov, R.; Suhr, O.B.; Ianiro, G.; Kupcinskas, J.; Segal, J.P.; Dumitrascu, D.L.; Heinrich, H.; Mikolasevic, I.; Stojkovic-Lalosevic, M.; Barbov, I.; et al. Recommendations for the diagnosis and management of transthyretin amyloidosis with gastrointestinal manifestations. Eur. J. Gastroenterol. Hepatol. 2021, 33, 613–622. [Google Scholar] [CrossRef]
- King, P.; Kates, A.M. Management of Cardiac Symptoms in Amyloidosis. Am. J. Med. 2022, 135 (Suppl. 1), S9–S12. [Google Scholar] [CrossRef]
- Pericet-Rodriguez, C.; López-Aguilera, J.; Durán-Torralba, C.; Castillo-Dominguez, J.C.; Ruiz-Ortiz, M.; Perea-Armijo, J.; Delgado-Ortega, M.; Mesa-Rubio, D.; González-Manzanares, R.; Ruiz de Castroviejo, J.; et al. Electrocardiographic features and need for pacemaker in cardiac amyloidosis: Analysis of 58 cases. Med. Clin. 2022, 159, 78–84. [Google Scholar] [CrossRef]
- Alreshq, R.; Tugal, D.; Siddiqi, O.; Ruberg, F. Conduction abnormalities and role of cardiac pacing in cardiac amyloidosis: A systematic review. Pacing Clin. Electrophysiol. 2021, 44, 2092–2099. [Google Scholar] [CrossRef]
- Suarez, G.A.; Opfer-Gehrking, T.L.; Offord, K.P.; Atkinson, E.J.; O’Brien, P.C.; Low, P.A. The Autonomic Symptom Profile: A new instrument to assess autonomic symptoms. Neurology 1999, 52, 523–528. [Google Scholar] [CrossRef]
- Treister, R.; O’Neil, K.; Downs, H.M.; Oaklander, A.L. Validation of the composite autonomic symptom scale 31 (COMPASS-31) in patients with and without small fiber polyneuropathy. Eur. J. Neurol. 2015, 22, 1124–1130. [Google Scholar] [CrossRef]
- Horowitz, S.H. The diagnostic workup of patients with neuropathic pain. Med. Clin. N. Am. 2007, 91, 21–30. [Google Scholar] [CrossRef]
- Gutrecht, J.A. Sympathetic skin response. J. Clin. Neurophysiol. 1994, 11, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Cruccu, G.; Pennisi, E.; Truini, A.; Iannetti, G.D.; Romaniello, A.; Le Pera, D.; De Armas, L.; Leandri, M.; Manfredi, M.; Valeriani, M. Unmyelinated trigeminal pathways as assessed by laser stimuli in humans. Brain 2003, 126, 2246–2256. [Google Scholar] [CrossRef] [PubMed]
- Hüllemann, P.; Shao, Y.Q.; Manthey, G.; Binder, A.; Baron, R. Central habituation and distraction alter C-fibre-mediated laser-evoked potential amplitudes. Eur. J. Pain 2016, 20, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.-P.; Zouari, H.G.; Gorram, F.; Nordine, T.; Damy, T.; Planté-Bordeneuve, V. The value of electrochemical skin conductance measurement using Sudoscan® in the assessment of patients with familial amyloid polyneuropathy. Clin. Neurophysiol. 2018, 129, 1565–1569. [Google Scholar] [CrossRef] [PubMed]
- Castro, J.; Miranda, B.; Castro, I.; de Carvalho, M.; Conceição, I. The diagnostic accuracy of Sudoscan in transthyretin familial amyloid polyneuropathy. Clin. Neurophysiol. 2016, 127, 2222–2227. [Google Scholar] [CrossRef] [PubMed]
- Narasimhaiah, D.; Mahadevan, A. Role of skin punch biopsy in diagnosis of small fiber neuropathy-A review for the neuropathologist. Indian J. Pathol. Microbiol. 2022, 65, S329–S336. [Google Scholar] [CrossRef] [PubMed]
- Leis, A.A.; Ross, M.A.; Emori, T.; Matsue, Y.; Saito, T. The silent period produced by electrical stimulation of mixed peripheral nerves. Muscle Nerve 1991, 14, 1202–1208. [Google Scholar] [CrossRef]
- Ohashi, N.; Kodaira, M.; Morita, H.; Sekijima, Y. Electrophysiological demyelinating features in hereditary ATTR amyloidosis. Amyloid 2019, 26, 15–23. [Google Scholar] [CrossRef]
- Van den Bergh, P.Y.K.; van Doorn, P.A.; Hadden, R.D.M.; Avau, B.; Vankrunkelsven, P.; Allen, J.A.; Attarian, S.; Blomkwist-Markens, P.H.; Cornblath, D.R.; Eftimov, F.; et al. European Academy of Neurology/Peripheral Nerve Society guideline on diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy: Report of a joint Task Force-Second revision. J. Peripher. Nerv. Syst. 2021, 26, 242–268. [Google Scholar] [CrossRef]
- Tozza, S.; Severi, D.; Spina, E.; Iovino, A.; Aruta, F.; Ruggiero, L.; Dubbioso, R.; Iodice, R.; Nolano, M.; Manganelli, F. The neuropathy in hereditary transthyretin amyloidosis: A narrative review. J. Peripher. Nerv. Syst. 2021, 26, 155–159. [Google Scholar] [CrossRef]
- Kiernan, J.A. Vascular permeability in the peripheral autonomic and somatic nervous systems: Controversial aspects and comparisons with the blood-brain barrier. Microsc. Res. Tech. 1996, 35, 122–136. [Google Scholar] [CrossRef]
- Mizisin, A.P.; Weerasuriya, A. Homeostatic regulation of the endoneurial microenvironment during development, aging and in response to trauma, disease and toxic insult. Acta Neuropathol. 2011, 121, 291–312. [Google Scholar] [CrossRef]
- Peterson, C.A.; Murrmann, M.; Steudle, E. Location of the major barriers to water and ion movement in young roots of Zea mays L. Planta 1993, 190, 127–136. [Google Scholar] [CrossRef]
- Sousa, M.M.; Cardoso, I.; Fernandes, R.; Guimarães, A.; Saraiva, M.J. Deposition of transthyretin in early stages of familial amyloidotic polyneuropathy: Evidence for toxicity of nonfibrillar aggregates. Am. J. Pathol. 2001, 159, 1993–2000. [Google Scholar] [CrossRef]
- Sousa, M.M.; Saraiva, M.J. Neurodegeneration in familial amyloid polyneuropathy: From pathology to molecular signaling. Prog. Neurobiol. 2003, 71, 385–400. [Google Scholar] [CrossRef]
- Koike, H.; Misu, K.; Sugiura, M.; Iijima, M.; Mori, K.; Yamamoto, M.; Hattori, N.; Mukai, E.; Ando, Y.; Ikeda, S.; et al. Pathology of early- vs. late-onset TTR Met30 familial amyloid polyneuropathy. Neurology 2004, 63, 129–138. [Google Scholar] [CrossRef]
- Andrés, N.; Poza, J.J.; Martí Massó, J.F. Familial amyloidosis with polyneuropathy type 1 caused by transthyretin mutation Val50Met (Val30Met): 4 cases in a non-endemic area. Neurologia 2018, 33, 583–589. [Google Scholar] [CrossRef]


{kind=link}
| ATTR Patients | Healthy Controls (HCs) | Asymptomatic Carriers (ACs) | p-Value < 0.05 | |
|---|---|---|---|---|
| Age (years) | 72.7 ± 14.1 | 68.2 ± 12.5 | 50.1 ± 15.5 | ATTR vs. HCs (p < 0.001) and ACs (p = 0.002) |
| M/F | 16/5 | 11/9 | 6/12 | ATTR vs. HCs (p = 0.007) and ACs (p = 0.007) |
| ATTR-wt/variant | 16/5 | n.a. | n.a. | |
| Pathologic variants | 2 Phe64Leu 2 Val30Met 1 Val122Ile | n.a. | 3 Phe64Leu 13 Val30Met 2 Val122Ile | |
| Phenotype: Pure cardiologic | 2 | n.a. | n.a. | |
| Pure neurologic | 4 | n.a. | n.a. | |
| Mixed phenotype | 15 | n.a. | n.a. |
| ATTR Patients | Healthy Controls (HCs) | Asymptomatic Carriers (ACs) | p-Value < 0.05 | |
|---|---|---|---|---|
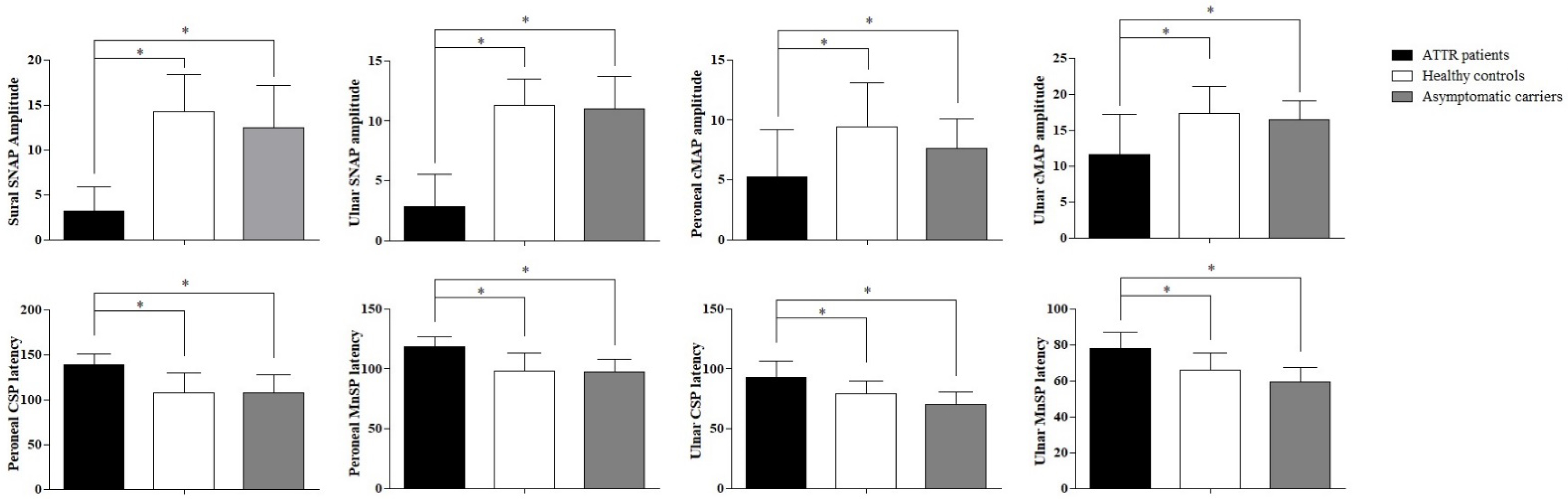
| Sural SNAP amplitude (μV) | 3.15 ± 2.7 | 14.3 ± 4.1 | 12.5 ± 4.7 | ATTR vs. HCs (p < 0.001) and ACs (p < 0.001) |
| Ulnar SNAP amplitude (μV) | 2.8 ± 2.7 | 11.3 ± 2.2 | 11.0 ± 2.7 | ATTR vs. HCs (p < 0.001) and ACs (p < 0.001) |
| Peroneal | ||||
| cMAP amplitude (mV) | 5.2 ± 4.0 | 9.4 ± 3.7 | 7.6 ± 2.5 | ATTR vs. HCs (p = 0.026) and ACs (p = 0.037) |
| cMAP latency (ms) | 3.5 ± 0.27 | 3.7 ± 0.3 | 3.5 ± 0.29 | |
| F-wave latency (ms) | 49.6 ± 7.7 | 48.2 ± 4.8 | 47.5 ± 3.3 | |
| CSP latency (ms) | 138.2 ± 12.3 | 108.1 ± 21.7 | 107.7 ± 19.5 | ATTR vs. HCs (p = 0.006) and ACs (p = 0.019) |
| CSP duration (ms) | 43.5 ± 8.4 | 56.9 ± 17.9 | 68.5 ± 27.5 | |
| MnSP latency (ms) | 119.2 ± 8.0 | 98.1 ± 15.0 | 97.6 ± 10.1 | ATTR vs. HCs (p = 0.005) and ACs (p = 0.028) |
| MnSP duration (ms) | 53.4 ± 23.8 | 63.6 ± 11.9 | 67.2 ± 19.0 | |
| Ulnar | ||||
| cMAP amplitude (mV) | 11.6 ± 5.6 | 17.3 ± 3.8 | 16.4 ± 2.7 | ATTR vs. HCs (p = 0.003) and ACs (p = 0.042) |
| cMAP latency (ms) | 2.0 ± 0.17 | 2.1 ± 0.14 | 2.1 ± 0.12 | |
| F-wave latency (ms) | 28.8 ± 9.6 | 27.7 ± 2.6 | 27.0 ± 2.4 | |
| CSP latency (ms) | 92.9 ± 13.1 | 78.9 ± 11.0 | 70.5 ± 10.2 | ATTR vs. HCs (p = 0.008) and ACs (p = 0.002) |
| CSP duration (ms) | 51.2 ± 23.5 | 54.2 ± 13.4 | 53.9 ± 23.5 | |
| MnSP latency (ms) | 77.6 ± 9.1 | 66.0 ± 9.3 | 59.2 ± 7.9 | ATTR vs. HCs (p = 0.007) and ACs (p = 0.002) |
| MnSP duration (ms) | 56.2 ± 14.1 | 54.8 ± 16.0 | 63.4 ± 35.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cambieri, C.; Libonati, L.; Moret, F.; Tartaglia, G.; Garibaldi, M.; Chimenti, C.; Inghilleri, M.; Ceccanti, M. The Silent Period for Small Fiber Sensory Neuropathy Assessment in a Mixed Cohort of Transthyretin-Mediated Amyloidosis. Biomedicines 2022, 10, 2073. https://doi.org/10.3390/biomedicines10092073
Cambieri C, Libonati L, Moret F, Tartaglia G, Garibaldi M, Chimenti C, Inghilleri M, Ceccanti M. The Silent Period for Small Fiber Sensory Neuropathy Assessment in a Mixed Cohort of Transthyretin-Mediated Amyloidosis. Biomedicines. 2022; 10(9):2073. https://doi.org/10.3390/biomedicines10092073
Chicago/Turabian StyleCambieri, Chiara, Laura Libonati, Federica Moret, Giorgio Tartaglia, Matteo Garibaldi, Cristina Chimenti, Maurizio Inghilleri, and Marco Ceccanti. 2022. "The Silent Period for Small Fiber Sensory Neuropathy Assessment in a Mixed Cohort of Transthyretin-Mediated Amyloidosis" Biomedicines 10, no. 9: 2073. https://doi.org/10.3390/biomedicines10092073
APA StyleCambieri, C., Libonati, L., Moret, F., Tartaglia, G., Garibaldi, M., Chimenti, C., Inghilleri, M., & Ceccanti, M. (2022). The Silent Period for Small Fiber Sensory Neuropathy Assessment in a Mixed Cohort of Transthyretin-Mediated Amyloidosis. Biomedicines, 10(9), 2073. https://doi.org/10.3390/biomedicines10092073