
Chronic Hepatitis B and Related Liver Diseases Are Associated with Reduced 25-Hydroxy-Vitamin D Levels: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Study Inclusion/Exclusion Criteria as per PICOS
2.3.1. Inclusion Criteria
- Individuals with hepatitis B infection (inactive carriers, chronic hepatitis);
- Adult participants >18 years of age;
- Classified the serum vitamin D concentration as either mean Vitamin D (nmol/L; ng/mL);
- Articles reporting hepatitis B infection with cirrhosis/fibrosis/HCC;
- In the English language;
- Full text available;
- Retrospective studies, cross-sectional, cohort, or randomized controlled trials.
2.3.2. Exclusion Criteria
- We excluded articles that were in a foreign language, or which did not contain the relevant information as per the inclusion criteria;
- Studies including pregnant women and children were not included;
- We also excluded literature reviews, editorial reviews, and systematic reviews;
- Editorials, brief communications, and conference proceedings were also excluded;
- Articles estimating the values of only 1, 25-dihydroxy vitamin D were also excluded.
2.4. Evaluation of the Methodological Quality of the Studies Included
2.5. Data Extraction
2.6. Statistical Analysis
3. Results
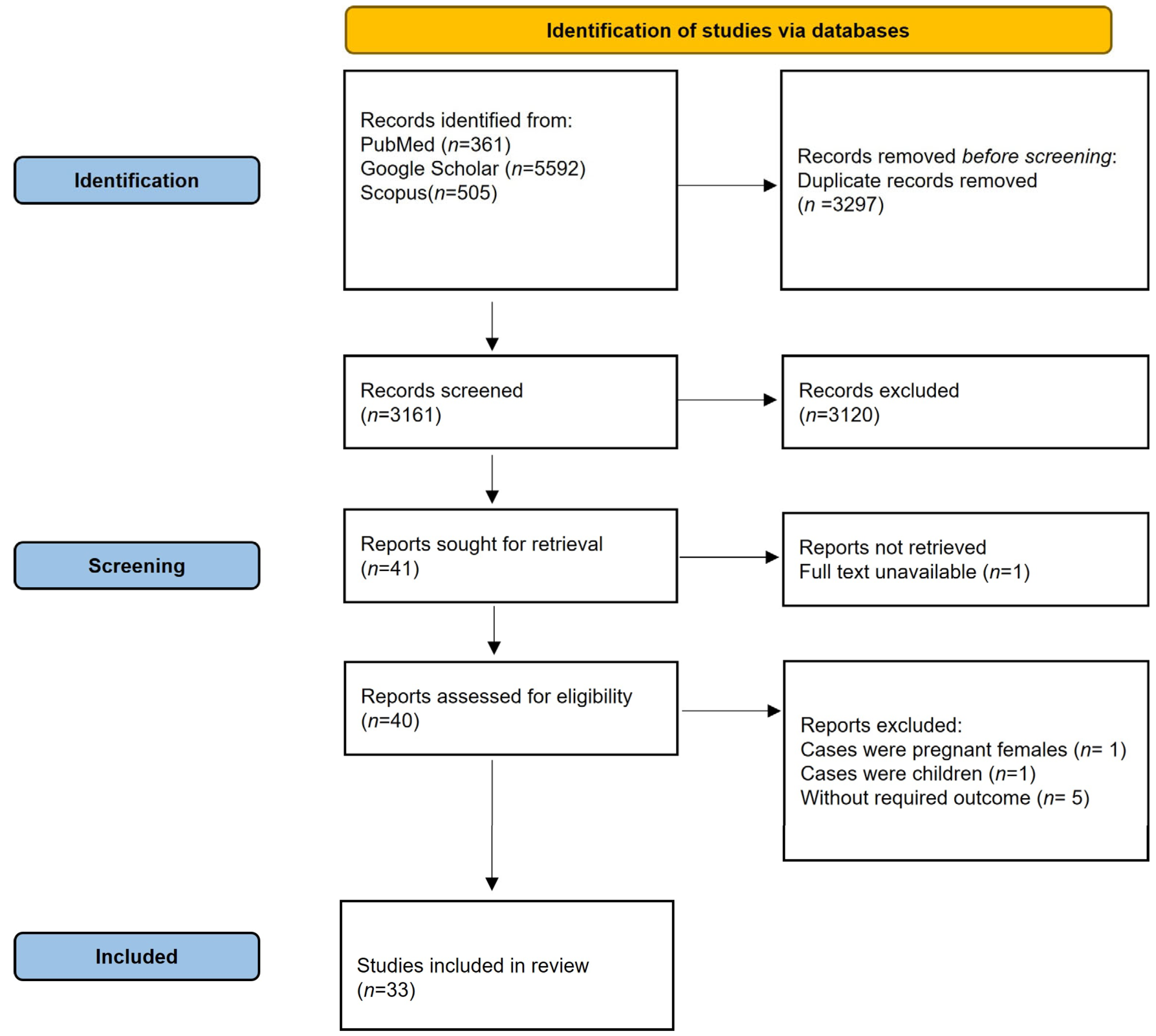
3.1. Search Results and Study Selection
3.2. Study Characteristics and Quality Assessment
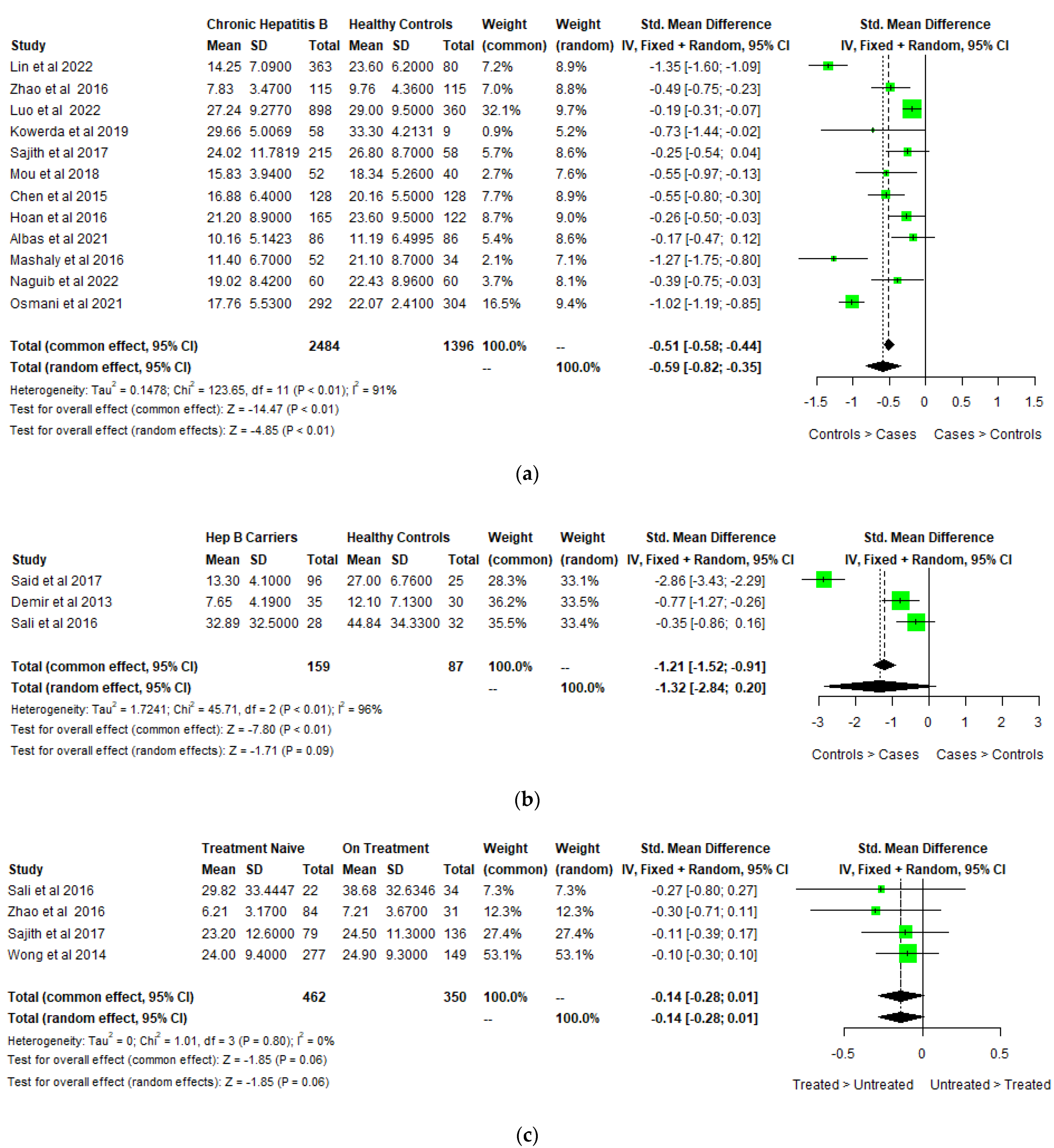
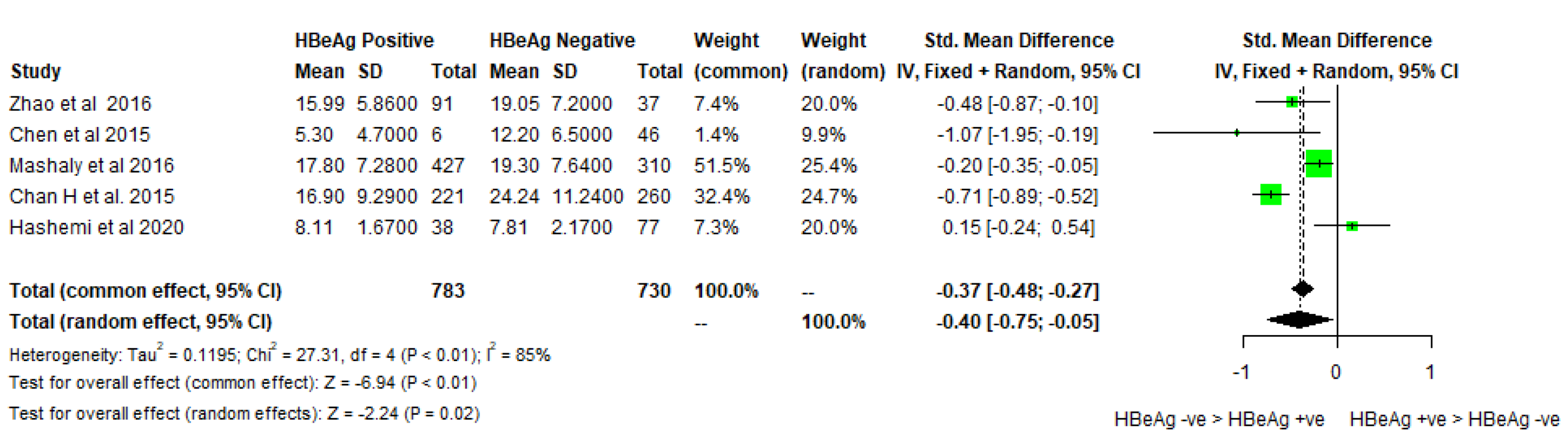
3.3. Pooled Estimates
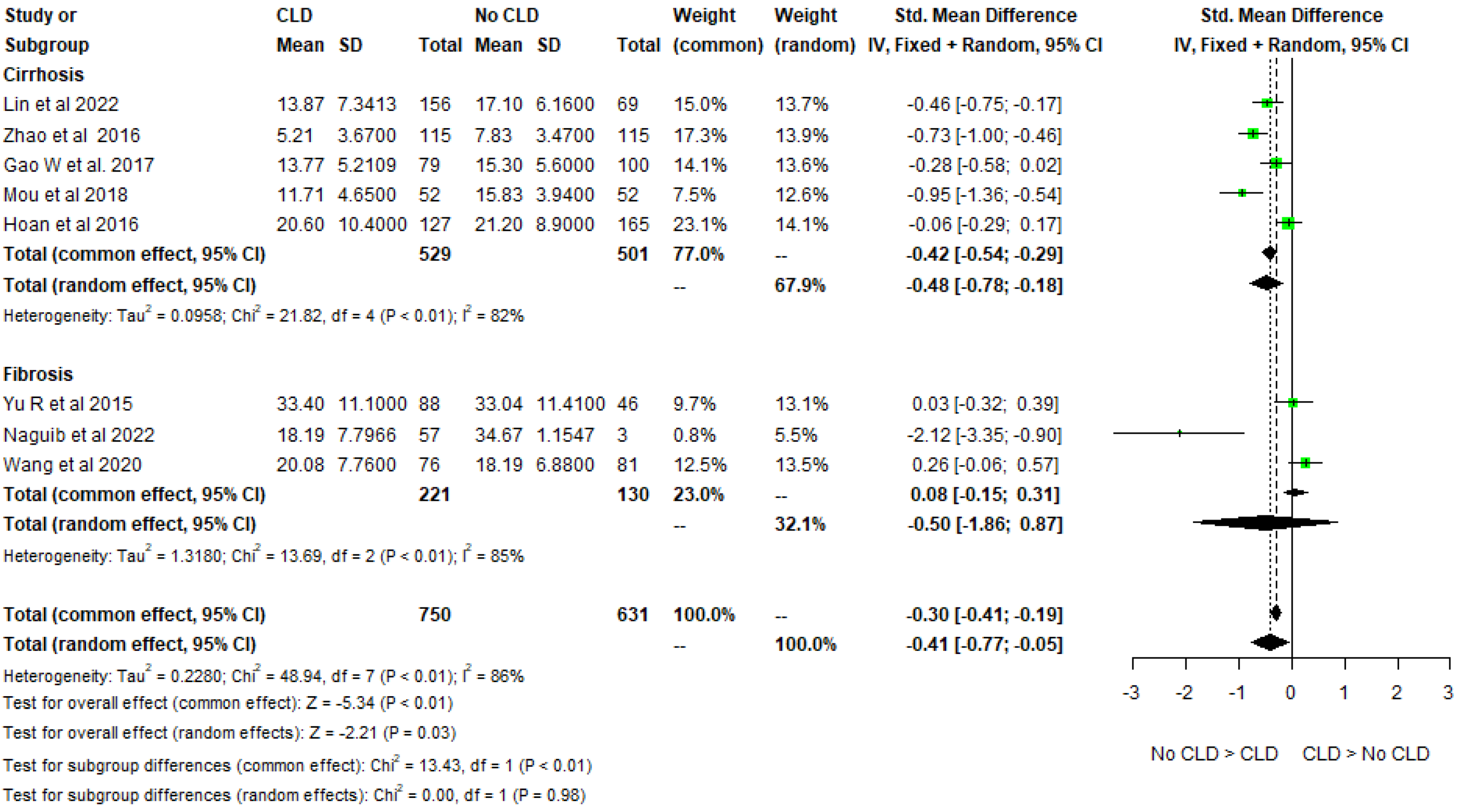
3.4. Meta-Analysis
3.5. Sensitivity Analysis
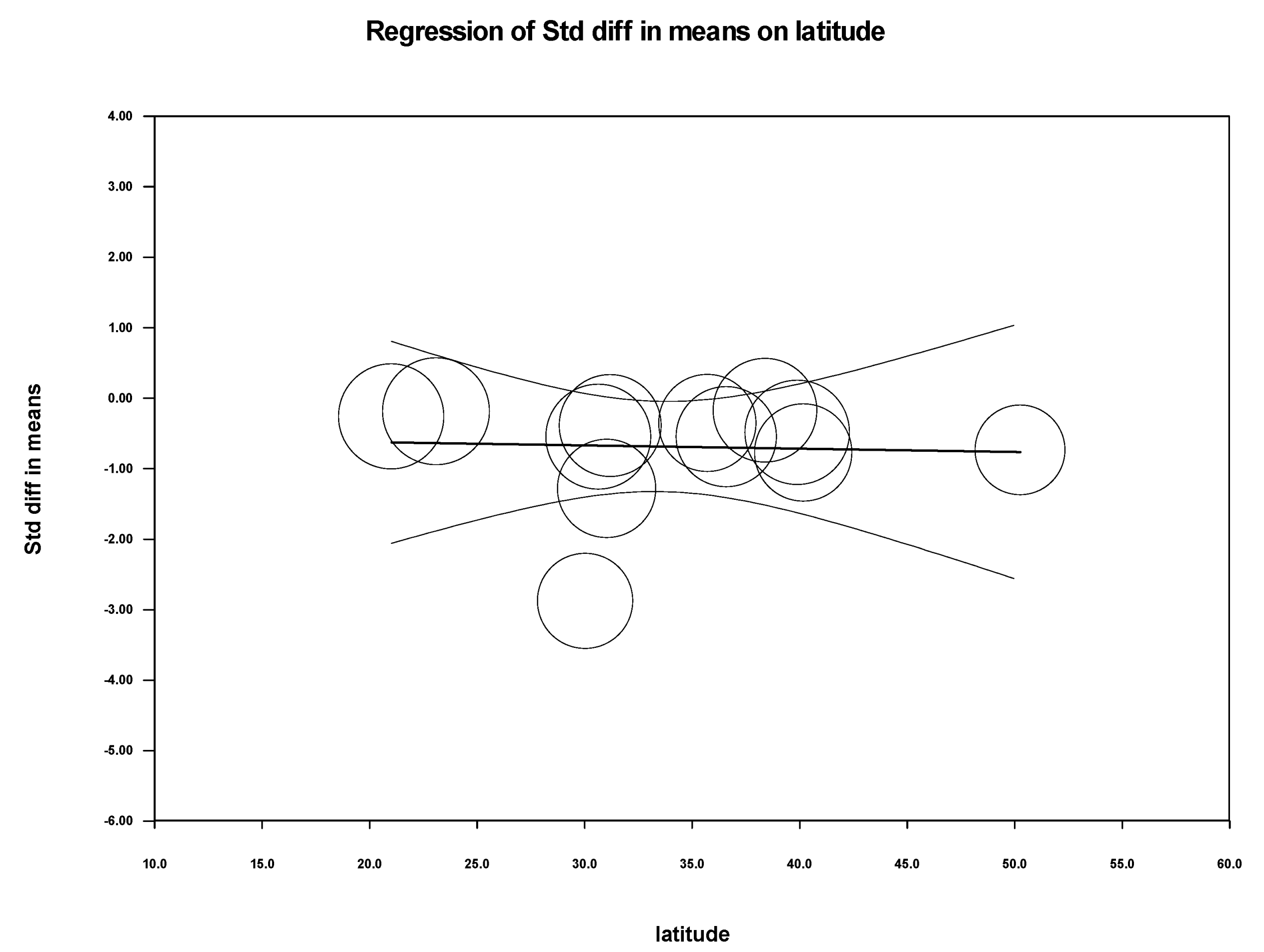
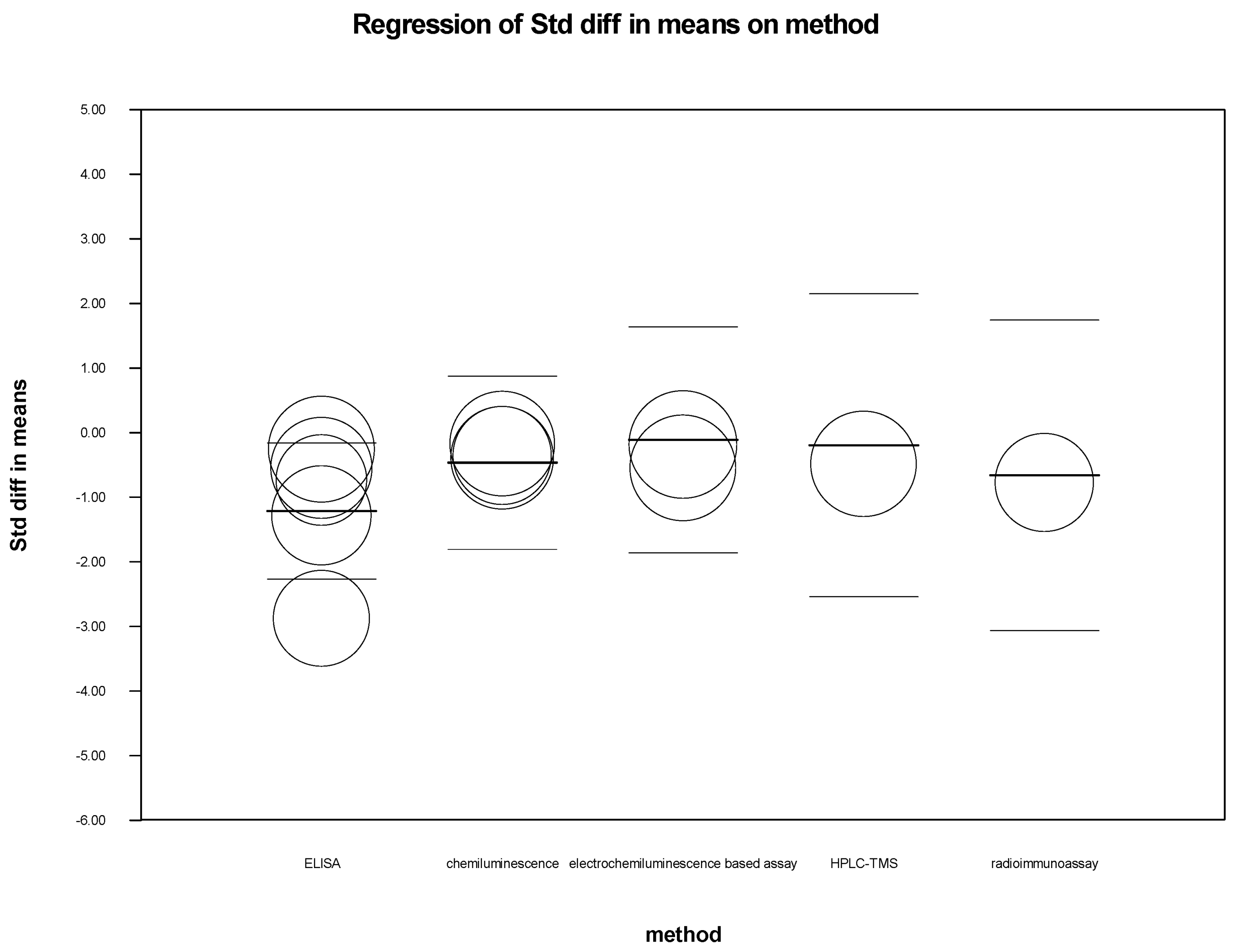
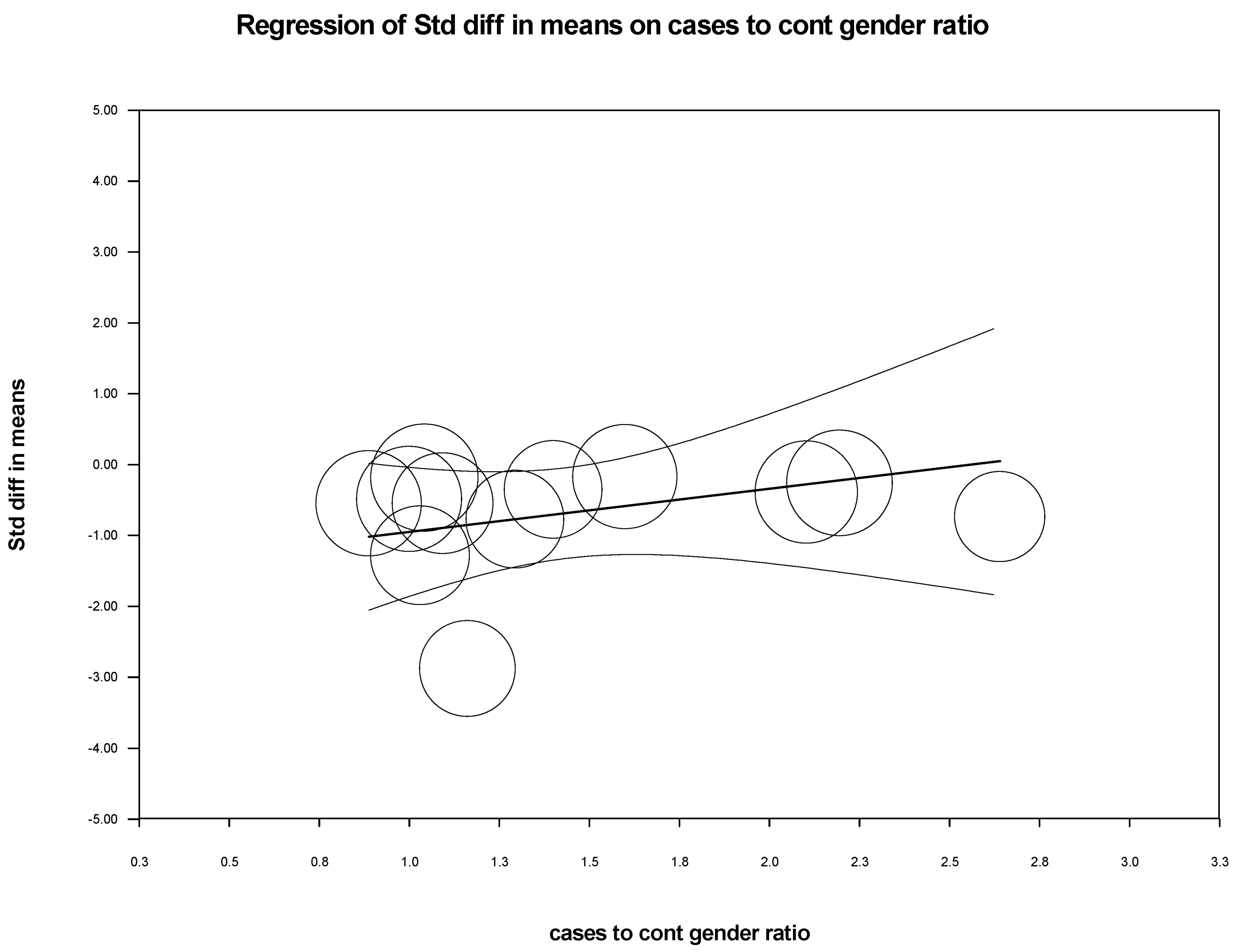
3.6. Meta-Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tang, L.S.Y.; Covert, E.; Wilson, E.; Kottilil, S. Chronic Hepatitis B Infection: A Review. JAMA 2018, 319, 1802–1813. [Google Scholar] [CrossRef]
- Peng, C.-Y.; Chien, R.-N.; Liaw, Y.-F. Hepatitis B Virus-Related Decompensated Liver Cirrhosis: Benefits of Antiviral Therapy. J. Hepatol. 2012, 57, 442–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binkley, N.; Ramamurthy, R.; Krueger, D. Low Vitamin D Status: Definition, Prevalence, Consequences, and Correction. Endocrinol. Metab. Clin. N. Am. 2010, 39, 287–301, table of contents. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, R.; Maseeh, A. Vitamin D: The “Sunshine” Vitamin. J Pharm. Pharm. 2012, 3, 118–126. [Google Scholar] [CrossRef]
- Ahluwalia, S.; Choudhary, D.; Tyagi, P.; Kumar, V.; Vivekanandan, P. Vitamin D Signaling Inhibits HBV Activity by Directly Targeting the HBV Core Promoter. J. Biol. Chem. 2021, 297, 101233. [Google Scholar] [CrossRef] [PubMed]
- Yin, K.; Agrawal, D.K. Vitamin D and Inflammatory Diseases. J. Inflamm. Res. 2014, 7, 69–87. [Google Scholar] [CrossRef] [Green Version]
- Ratnam, D.; Visvanathan, K. New Concepts in the Immunopathogenesis of Chronic Hepatitis B: The Importance of the Innate Immune Response. Hepatol. Int. 2008, 2, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Kondo, Y.; Ueno, Y.; Shimosegawa, T. Toll-like Receptors Signaling Contributes to Immunopathogenesis of HBV Infection. Gastroenterol. Res. Pract. 2011, 2011, 810939. [Google Scholar] [CrossRef] [Green Version]
- Hoan, N.X.; Khuyen, N.; Binh, M.T.; Giang, D.P.; Van Tong, H.; Hoan, P.Q.; Trung, N.T.; Anh, D.T.; Toan, N.L.; Meyer, C.G.; et al. Association of Vitamin D Deficiency with Hepatitis B Virus—Related Liver Diseases. BMC Infect. Dis. 2016, 16, 507. [Google Scholar] [CrossRef] [Green Version]
- Nimer, A.; Mouch, A. Vitamin D Improves Viral Response in Hepatitis C Genotype 2-3 Naïve Patients. World J. Gastroenterol. 2012, 18, 800–805. [Google Scholar] [CrossRef]
- Farnik, H.; Bojunga, J.; Berger, A.; Allwinn, R.; Waidmann, O.; Kronenberger, B.; Keppler, O.T.; Zeuzem, S.; Sarrazin, C.; Lange, C.M. Low Vitamin D Serum Concentration Is Associated with High Levels of Hepatitis B Virus Replication in Chronically Infected Patients. Hepatology 2013, 58, 1270–1276. [Google Scholar] [CrossRef]
- Hu, Y.-C.; Wang, W.-W.; Jiang, W.-Y.; Li, C.-Q.; Guo, J.-C.; Xun, Y.-H. Low Vitamin D Levels Are Associated with High Viral Loads in Patients with Chronic Hepatitis B: A Systematic Review and Meta-Analysis. BMC Gastroenterol. 2019, 19, 84. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Said, E.; Agawy, W.E.; Ahmed, R.; Hassany, M.; Ahmed, A.; Fouad, H.; Baiumy, H. Serum Vitamin D Levels in Treatment-Naïve Chronic Hepatitis B Patients. J. Transl. Intern. Med. 1977, 5, 230–234. [Google Scholar] [CrossRef] [Green Version]
- Demir, C.; Demir, M. Vitamin D Levels in Patients with Chronic Hepatitis B Virus Infection and Naturally Immunized Individuals. Intern. Med. Inside 2013, 4, 2343–6549. [Google Scholar] [CrossRef] [Green Version]
- Sali, S.; Tavakolpour, S.; Farkhondemehr, B. Comparison of Vitamin D Levels in Naive, Treated, and Inactive Carriers with Chronic Hepatitis B Virus. J. Clin. Transl. Hepatol. 2016, 4, 306–309. [Google Scholar] [CrossRef]
- Lin, S.; Wang, W.; Shi, L.; Yang, X.; Chen, Y.; Liu, X.; Li, J.; Ye, F.; An, X.; Zhang, X. Severe Vitamin D Deficiency Is Strongly Associated with Liver Dysfunction and Disease Severity in Hepatitis B Virus Related Cirrhosis and Liver Failure Patients. J. Nutr. Sci. Vitaminol. 2022, 68, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.Y.; Li, J.; Wang, J.H.; Habib, S.; Wei, W.; Sun, S.J.; Strobel, H.W.; Jia, J.D. Vitamin, D. Serum Level Is Associated with Child-Pugh Score and Metabolic Enzyme Imbalances, but Not Viral Load in Chronic Hepatitis B Patients. Medicine 2016, 95, e3926. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Ye, J.; Shao, C.; Lin, Y.; Sun, Y.; Feng, S.; Wang, W.; Zhong, B. Vitamin D Status Presents Different Relationships with Severity in Metabolic-Associated Fatty Liver Disease Patients with or without Hepatitis B Infection. Nutrients 2022, 14, 2114. [Google Scholar] [CrossRef] [PubMed]
- Parfieniuk-Kowerda, A.; Świderska, M.; Rogalska, M.; Maciaszek, M.; Jaroszewicz, J.; Flisiak, R. Chronic Hepatitis B Virus Infection Is Associated with Decreased Serum 25(OH)D Concentration in Non-Cirrhotic Patients. Clin. Exp. Hepatol. 2019, 5, 75–80. [Google Scholar] [CrossRef]
- Sajith, K.G.; Kapoor, N.; Shetty, S.; Goel, A.; Zachariah, U.; Eapen, C.E.; Paul, T.V. Bone Health and Impact of Tenofovir Treatment in Men with Hepatitis-B Related Chronic Liver Disease. J. Clin. Exp. Hepatol. 2018, 8, 23–27. [Google Scholar] [CrossRef]
- Mou, H.; Yang, F.; Zhou, J.; Bao, C. Correlation of Liver Function with Intestinal Flora, Vitamin Deficiency and IL-17A in Patients with Liver Cirrhosis. Exp. Ther. Med. 2018, 16, 4082–4088. [Google Scholar] [CrossRef] [Green Version]
- Chen, E.Q.; Bai, L.; Zhou, T.Y.; Fe, M.; Zhang, D.M.; Tang, H. Sustained Suppression of Viral Replication in Improving Vitamin D Serum Concentrations in Patients with Chronic Hepatitis B. Sci. Rep. 2015, 5, 15441. [Google Scholar] [CrossRef] [Green Version]
- Albas, S.; Koc, E.; Nemli, S.; Demirdal, T.; Soyoz, M.; Aksun, S.; Sozmen, M.K.; Avsar, C.; Gurbu, B.C. Vitamin D Levels and Vitamin D Receptor (VDR) Gene Polymorphisms in Inactive Hepatitis B Virus Carriers. Parameters 2021, 30, 393–398. [Google Scholar]
- Mashaly, M.; Sayed, E.E.; Shaker, G.A.; Anwar, R.; Abbas, N.F.; Zakaria, S.; Barakat, E.A.M.E. Occult and Chronic Hepatitis B Infection: Relation of Viral Load to Serum Level of 25 Hydroxy Vitamin D. Int. J. Curr. Microbiol. App. Sci. 2016, 5, 660–669. [Google Scholar] [CrossRef] [Green Version]
- Naguib, R.; Fayed, A.; Abdeen, N.; Naguib, H. Association of Serum 25-Hydroxyvitamin D3 Levels and Insulin Resistance with Viral Load and Degree of Liver Fibrosis in Egyptian Chronic HBV Patients: A Case Control Study. Clin. Exp. Hepatol. 2022, 8, 14–20. [Google Scholar] [CrossRef]
- Osmanï, F.; Ziaee, M. The Importance of Vitamin D Deficiency as a Potential Marker Among Chronic Hepatitis B Patients. Viral Hepat. J. 2021, 27, 74–79. [Google Scholar] [CrossRef]
- Thakur, P.; Cherian, K.E.; Kapoor, N.; Rebekah, G.; Goel, A.; Zachariah, U.; Eapen, C.E.; Thomas, N.; Paul, T.V. Proximal Hip Geometry, Trabecular Bone Score, Bone Mineral Density and Bone Mineral Parameters in Patients With Cryptogenic and Hepatitis B Related Cirrhosis- A Study From the Indian Subcontinent. J. Clin. Densitom. Off. J. Int. Soc. Clin. Densitom. 2022, 25, 97–104. [Google Scholar] [CrossRef]
- Mahamid, M.; Nseir, W.; Abu Elhija, O.; Shteingart, S.; Mahamid, A.; Smamra, M.; Koslowsky, B. Normal Vitamin D Levels Are Associated with Spontaneous Hepatitis B Surface Antigen Seroclearance. World J. Hepatol. 2013, 5, 328–331. [Google Scholar] [CrossRef] [Green Version]
- Yu, R.; Tan, D.; Ning, Q.; Niu, J.; Bai, X.; Chen, S.; Cheng, J.; Yu, Y.; Wang, H.; Xu, M.; et al. Association of Baseline Vitamin D Level with Genetic Determinants and Virologic Response in Patients with Chronic Hepatitis B. Hepatol. Res. Off. J. Jpn. Soc. Hepatol. 2018, 48, E213–E221. [Google Scholar] [CrossRef] [Green Version]
- Yu, R.; Sun, J.; Zheng, Z.; Chen, J.; Fan, R.; Liang, X.; Zhu, Y.; Liu, Y.; Shen, S.; Hou, J. Association between Vitamin D Level and Viral Load or Fibrosis Stage in Chronic Hepatitis B Patients from Southern China. J. Gastroenterol. Hepatol. 2015, 30, 566–574. [Google Scholar] [CrossRef]
- Chan, H.L.; Elkhashab, M.; Trinh, H.; Tak, W.Y.; Ma, X.; Chuang, W.L.; Kim, Y.J.; Martins, E.B.; Lin, L.; Dinh, P.; et al. Association of Baseline Vitamin D Levels with Clinical Parameters and Treatment Outcomes in Chronic Hepatitis B. J. Hepatol. 2015, 63, 1086–1092. [Google Scholar] [CrossRef]
- Gao, W.; Wang, R.; Wang, X.; Wu, H.; Wang, Y.; Lu, X.; Li, L.; Zheng, J.; Li, W. Vitamin D Serum Levels and Receptor Genetic Polymorphisms Are Associated with Hepatitis B Virus and HIV Infections and IFN-λ Levels. Biomark. Med. 2017, 11, 733–740. [Google Scholar] [CrossRef]
- Osmani, F.; Azarkar, G. Fitting Logistic Regression Models to Assess Vitamin D Deficiency with Clinical Parameters in Chronic Hepatitis B Patients. Infect. Dis. Model. 2021, 6, 612–617. [Google Scholar] [CrossRef]
- Ko, B.J.; Kim, Y.S.; Kim, S.G.; Park, J.H.; Lee, S.H.; Jeong, S.W.; Jang, J.Y.; Kim, H.S.; Kim, B.S.; Kim, S.M.; et al. Relationship between 25-Hydroxyvitamin D Levels and Liver Fibrosis as Assessed by Transient Elastography in Patients with Chronic Liver Disease. Gut Liver 2016, 10, 818–825. [Google Scholar] [CrossRef] [Green Version]
- Ko, W.S.; Yang, Y.P.; Shen, F.P.; Wu, M.C.; Shih, C.J.; Lu, M.C.; Yan, Y.H.; Chiou, Y.L. The Study of Correlation Between Serum Vitamin D(3) Concentrations and HBV DNA Levels and Immune Response in Chronic Hepatitis Patients. Nutrients 2020, 12, 1114. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.L.; Chan, H.L.; Chan, H.Y.; Tse, C.H.; Chim, A.M.; Lo, A.O.; Wong, V.W. Adverse Effects of Vitamin D Deficiency on Outcomes of Patients with Chronic Hepatitis B. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2015, 13, 783–790.e1. [Google Scholar] [CrossRef] [PubMed]
- Berkan-Kawińska, A.; Koślińska-Berkan, E.; Piekarska, A. The Prevalence and Severity of 25-(OH)-Vitamin D Insufficiency in HCV Infected and in HBV Infected Patients: A Prospective Study. Clin. Exp. Hepatol. 2015, 1, 5–11. [Google Scholar] [CrossRef]
- Hashemi, S.J.; Parsi, A.; Hajiani, E.; Masjedizadeh, A.; Shayesteh, A. Relationship Between 25-HydroxyVitamin D Level and Liver Stiffness in Patients with Chronic Hepatitis B Using Transient Elastography. Hepat. Mon. 2020, 20, e100891. [Google Scholar] [CrossRef]
- Karim, A.; Memon, S.H.; Ahmed, J.; Soomro, A.K.; Manan, A. Prevalence Of Vitamin-D Deficiency Among The Patients Of Hbv And Hcv Relatedchronic Liver Disease. J. Peoples Univ. Med. Health Sci. 2021, 11, 67–72. [Google Scholar] [CrossRef]
- Kumar, D.; Khan, M.U.; Kashif, S.M.; Shaikh, M.A.; Nawaz, Z.; Shaikh, U. Association of Vitamin D Deficiency with Hepatitis B and C Virus Infection. J. Pharm. Res. Int. 2021, 33, 10–14. [Google Scholar] [CrossRef]
- Motor, S.; Koksaldi-Motor, V.; Dokuyucu, R.; Ustun, I.; Evirgen, O.; Yilmaz, N.; Onlen, Y.; Gokce, C. Investigation of Vitamin D Levels in Patients with Inactive Hepatitis B Virus Carrier. Acta Med. Mediterr. 2014, 30, 793–796. [Google Scholar]
- Schiefke, I.; Fach, A.; Wiedmann, M.; Aretin, A.-V.; Schenker, E.; Borte, G.; Wiese, M.; Moessner, J. Reduced Bone Mineral Density and Altered Bone Turnover Markers in Patients with Non-Cirrhotic Chronic Hepatitis B or C Infection. World J. Gastroenterol. 2005, 11, 1843–1847. [Google Scholar] [CrossRef]
- Wang, C.-C.; Tzeng, I.-S.; Su, W.-C.; Li, C.-H.; Lin, H.H.; Yang, C.-C.; Kao, J.-H. The Association of Vitamin D with Hepatitis B Virus Replication: Bystander Rather than Offender. J. Med. Assoc. 2020, 119, 1634–1641. [Google Scholar] [CrossRef]
- WHO Hepatitis B Factsheet. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 25 October 2022).
- Finkelmeier, F.; Kronenberger, B.; Zeuzem, S.; Piiper, A.; Waidmann, O. Low 25-Hydroxyvitamin D Levels Are Associated with Infections and Mortality in Patients with Cirrhosis. PLoS ONE 2015, 10, e0132119. [Google Scholar] [CrossRef]
- He, L.-J.; Zhang, H.-P.; Li, H.-J.; Wang, J.; Chang, D.-D. Effect of Serum Vitamin D Levels on Cellular Immunity and Antiviral Effects in Chronic Hepatitis B Patients. Clin. Lab. 2016, 62, 1933–1939. [Google Scholar] [CrossRef]
- Malham, M.; Peter Jørgensen, S.; Lauridsen, A.L.; Ott, P.; Glerup, H.; Dahlerup, J.F. The Effect of a Single Oral Megadose of Vitamin D Provided as Either Ergocalciferol (D2) or Cholecalciferol (D3) in Alcoholic Liver Cirrhosis. Eur. J. Gastroenterol. Hepatol. 2012, 24, 172–178. [Google Scholar] [CrossRef]
- Lee, P.-C.; Yang, Y.-Y.; Lee, W.-P.; Lee, K.-C.; Hsieh, Y.-C.; Lee, T.-Y.; Lin, H.-C. Comparative Portal Hypotensive Effects as Propranolol of Vitamin D3 Treatment by Decreasing Intrahepatic Resistance in Cirrhotic Rats. J. Gastroenterol. Hepatol. 2015, 30, 628–637. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sr. No. | Key Words | Databases | ||
|---|---|---|---|---|
| PubMed | Google Scholar | Scopus | ||
| 1 | “Calcitriol” and “Hepatitis B” | 44 | 998 | 132 |
| 2 | “Cholecalciferol” and “Hepatitis B” | 6 | 999 | 8 |
| 3 | “Vitamin D” and “Hepatitis B” | 192 | 998 | 200 |
| 4 | “Calcitriol” and “HBV” | 26 | 996 | 32 |
| 5 | “Cholecalciferol” and “HBV” | 2 | 606 | 3 |
| 6 | “Vitamin D” and “HBV” | 91 | 995 | 130 |
| Author & Year | Country | Study Design | Number of Cases | CHB State | Number of Healthy Controls | Vitamin D Estimation Method | Vitamin D in Patients (Mean ± SD) (ng/mL) | Vitamin D in Controls (Mean ± SD) (ng/mL) | Quality Score |
|---|---|---|---|---|---|---|---|---|---|
| Said et al. 2017 [18] | Egypt | retrospective case control | 96 | Inactive carriers | 25 | ELISA | 13.3 ± 4.1 | 27 ± 6.76 | 17 |
| Demir et al. 2013 [19] | Turkey | cross-sectional | 35 | Inactive carriers | 30 | radioimmunoassay | 7.65 ± 4.19 | 12.1 ± 7.13 | 18 |
| Sali et al. 2016 [20] | Iran | retrospective case control | 28 | Inactive carriers | 32 | chemiluminescence | 32.89 ± 32.5 | 44.84 ± 34.33 | 13 |
| Lin et al. 2022 [21] | China | retrospective case control | 363 | CHB | 80 | electrochemiluminescence based assay | 14.25 ± 7.09 | 23.6 ± 6.2 | 22 |
| Zhao et al. 2016 [22] | China | retrospective case control | 115 | CHB | 115 | HPLC-TMS | 7.83 ± 3.47 | 9.76 ± 4.36 | 21 |
| Luo et al. 2022 [23] | China | cross-sectional | 898 | CHB & MAFLD with CHB | 360 | electrochemiluminescence based assay | 27.2371 ± 9.277 | 29 ± 9.5 | 20 |
| Kowerda et al. 2019 [24] | Poland | retrospective case control | 58 | CHB | 9 | ELISA | 29.6646 ± 5.0069 | 33.2984 ± 4.2131 | 15 |
| Sajith et al. 2017 [25] | India | retrospective case control | 215 | CHB | 58 | chemiluminescence | 24.0223 ± 11.7819 | 26.8 ± 8.7 | 16 |
| Mou et al. 2018 [26] | China | retrospective case control | 52 | CHB | 40 | ELISA | 15.83 ± 3.94 | 18.34 ± 5.26 | 16 |
| Chen et al. 2015 [27] | China | cohort | 128 | CHB | 128 | electrochemiluminescence based assay | 16.88 ± 6.4 | 20.16 ± 5.5 | 22 |
| Hoan et al. 2016 [9] | Vietnam | cross-sectional | 165 | CHB | 122 | ELISA | 21.2 ± 8.9 | 23.6 ± 9.5 | 17 |
| Albas et al. 2021 [28] | Turkey | cross-sectional | 86 | CHB | 86 | chemiluminescence | 10.16 ± 5.1423 | 11.1895 ± 6.4995 | 16 |
| Mashaly et al. 2016 [29] | Egypt | cross-sectional | 52 | CHB | 34 | ELISA | 11.4 ± 6.7 | 21.1 ± 8.7 | 19 |
| Naguib et al. 2022 [30] | Egypt | retrospective case control | 60 | CHB | 60 | chemiluminescence | 19.02 ± 8.42 | 22.43 ± 8.96 | 14 |
| Osmani et al. 2021b [31] | Iran | retrospective case control | 292 | CHB | 304 | electrochemiluminescence based assay | 17.76 ± 5.53 | 22.07 ± 2.41 | 20 |
| Thakur et al. 2021 [32] | India | cross-sectional | 30 | Hep B Cirrhosis | 30 | electrochemiluminescence based assay | 25.4 ± 11 | 30.4 ± 8.6 | 16 |
| Mahamid et al. 2013 [33] | Israel | cross-sectional | 53 | HBsAg seroclearance | - | NA | 28.0283 ± 8.0753 | - | 16 |
| Yu R et al. 2018 [34] | China | RCT | 560 | CHB | - | electrochemiluminescence based assay | 29.64 ± 11.29 | - | 15 |
| Yu R et al. 2015 [35] | China | cross-sectional | 242 | CHB | - | electrochemiluminescence based assay | 33.9 ± 10.67 | - | 16 |
| Chan H et al. 2015 [36] | RCT | 737 | CHB | - | chemiluminescence | 18.4 ± 7.46 | - | 16 | |
| Gao W et al. 2017 [37] | China | cross-sectional | 100 | CHB | - | NA | 15.3 ± 5.6 | - | 16 |
| Farnik et al. 2013 [11] | Germany | retrospective case control | 203 | CHB | - | radioimmunoassay | 14.4 ± 7.9 | - | 16 |
| Osmani et al. 2021a [38] | Iran | cross-sectional | 292 | CHB | - | electrochemiluminescence based assay | 18.4 ± 3.5 | - | 16 |
| Ko et al. 2016 [39] | Korea | cross-sectional | 207 | CHB | - | isotope-dilution liquid chromatography-tandem mass spectrometry. | 13.4717 ± 7.1565 | - | 16 |
| Ko et al. 2020 [40] | Taiwan | cross-sectional | 60 | CHB | - | chemiluminescence | 20.9 ± 5.6 | - | 16 |
| Wong et al. 2014 [41] | China | cohort | 426 | CHB | - | electrochemiluminescence based assay | 24.3 ± 9.4 | - | 16 |
| Berkan-Kawinska et al. 2015 [42] | Poland | cross-sectional | 35 | CHB | - | chemiluminescence | 17.6 ± - | - | 15 |
| Hashemi et al. 2020 [43] | Iran | cross-sectional | 281 | CHB | - | ELISA | 23.69 ± 11.26 | - | 15 |
| Karim et al. 2021 [44] | Pakistan | cross-sectional | 108 | CHB | - | chemiluminescence | 25.23 ± - | - | 10 |
| Kumar et al. 2021 [45] | Pakistan | cross-sectional | 93 | CHB | - | NA | 24.31 ± - | - | 10 |
| Motor et al. 2014 [46] | Turkey | cross-sectional | 81 | Inactive carriers | - | chemiluminescence | 52.764 ± 20.03 | - | 13 |
| Schiefke et al. 2005 [47] | Germany | cross-sectional | 13 | CHB | - | biochemistry assay | 31.2354 ± 13.3896 | - | 13 |
| Wang et al. 2020 [48] | Taiwan | RCT | 196 | CHB | - | chemiluminescence | 19.8 ± 7.4 | - | 21 |
| Covariate | Coefficient | Standard Error | 95% Lower | 95% Upper | Z-Value | 2-Sided p-Value | Set |
|---|---|---|---|---|---|---|---|
| Cases vs. Controls | |||||||
| Intercept | −1.9311 | 1.0683 | −4.025 | 0.1628 | −1.81 | 0.0707 | |
| Latitude | −0.0047 | 0.0273 | −0.0581 | 0.0488 | −0.17 | 0.8635 | |
| Chemiluminescence Method | 0.7477 | 0.4402 | −0.1152 | 1.6105 | 1.7 | 0.0894 | Q = 6.03, df = 4, p = 0.1971 |
| Electrochemiluminescence Method | 1.1013 | 0.5598 | 0.004 | 2.1985 | 1.97 | 0.0492 | |
| HPLC-TMS Method | 1.0181 | 0.7092 | −0.3718 | 2.4081 | 1.44 | 0.1511 | |
| Radioimmunoassay Method | 0.5537 | 0.7118 | −0.8414 | 1.9488 | 0.78 | 0.4366 | |
| Cases to Controls Gender Ratio | 0.6102 | 0.3962 | −0.1663 | 1.3867 | 1.54 | 0.1235 | |
| All Cases | |||||||
| Intercept | 53.1721 | 29.3444 | −4.3418 | 110.686 | 1.81 | 0.07 | |
| Chemiluminescence Method | −3.2579 | 10.6526 | −24.1366 | 17.6208 | −0.31 | 0.7597 | Q = 13.91, df = 6, p = 0.0306 |
| Electrochemiluminescence Method | −9.2847 | 11.8277 | −32.4666 | 13.8971 | −0.78 | 0.4325 | |
| ELISA Method | −13.5263 | 10.6162 | −34.3337 | 7.2811 | −1.27 | 0.2026 | |
| HPLC-TMS Method | −19.5501 | 12.7232 | −44.4871 | 5.3868 | −1.54 | 0.1244 | |
| Isotope-dilution Liquid Chromatography-tandem Mass Spectrometry Method | −15.438 | 12.1771 | −39.3047 | 8.4288 | −1.27 | 0.2049 | |
| Radioimmunoassay Method | −27.7252 | 11.4111 | −50.0906 | −5.3598 | −2.43 | 0.0151 | |
| Latitude | 0.2235 | 0.2937 | −0.3521 | 0.7991 | 0.76 | 0.4466 | |
| Age | −0.6979 | 0.4296 | −1.5398 | 0.1441 | −1.62 | 0.1043 | |
| Male female ratio | 0.3166 | 2.1212 | −3.8409 | 4.474 | 0.15 | 0.8814 | |
| All Controls | |||||||
| Intercept | −71.6418 | 82.2164 | −232.783 | 89.4993 | −0.87 | 0.3835 | |
| Latitude | 0.9468 | 0.8782 | −0.7744 | 2.668 | 1.08 | 0.281 | |
| Electrochemiluminescence Method | −9.1972 | 16.0905 | −40.734 | 22.3395 | −0.57 | 0.5676 | Q = 3.09, df = 4, p = 0.5421 |
| ELISA Method | −2.4554 | 8.7522 | −19.6094 | 14.6985 | −0.28 | 0.7791 | |
| HPLC-TMS Method | −60.6786 | 43.2949 | −145.535 | 24.1777 | −1.4 | 0.1611 | |
| Radioimmunoassay Method | −8.1006 | 15.618 | −38.7113 | 22.5101 | −0.52 | 0.604 | |
| Male female ratio | 14.047 | 13.5259 | −12.4632 | 40.5572 | 1.04 | 0.299 | |
| Age | 1.0935 | 1.0572 | −0.9785 | 3.1655 | 1.03 | 0.3009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banerjee, A.; Athalye, S.; Khargekar, N.; Shingade, P.; Madkaikar, M. Chronic Hepatitis B and Related Liver Diseases Are Associated with Reduced 25-Hydroxy-Vitamin D Levels: A Systematic Review and Meta-Analysis. Biomedicines 2023, 11, 135. https://doi.org/10.3390/biomedicines11010135
Banerjee A, Athalye S, Khargekar N, Shingade P, Madkaikar M. Chronic Hepatitis B and Related Liver Diseases Are Associated with Reduced 25-Hydroxy-Vitamin D Levels: A Systematic Review and Meta-Analysis. Biomedicines. 2023; 11(1):135. https://doi.org/10.3390/biomedicines11010135
Chicago/Turabian StyleBanerjee, Anindita, Shreyasi Athalye, Naveen Khargekar, Poonam Shingade, and Manisha Madkaikar. 2023. "Chronic Hepatitis B and Related Liver Diseases Are Associated with Reduced 25-Hydroxy-Vitamin D Levels: A Systematic Review and Meta-Analysis" Biomedicines 11, no. 1: 135. https://doi.org/10.3390/biomedicines11010135
APA StyleBanerjee, A., Athalye, S., Khargekar, N., Shingade, P., & Madkaikar, M. (2023). Chronic Hepatitis B and Related Liver Diseases Are Associated with Reduced 25-Hydroxy-Vitamin D Levels: A Systematic Review and Meta-Analysis. Biomedicines, 11(1), 135. https://doi.org/10.3390/biomedicines11010135