
Hierarchical Cluster Analysis Based on Clinical and Neuropsychological Symptoms Reveals Distinct Subgroups in Fibromyalgia: A Population-Based Cohort Study



Abstract
:1. Introduction
2. Methods
2.1. Study Participants
2.2. Measures
2.3. Health Status Variables
2.4. Neuropsychological Variables
2.5. Statistical Analysis
3. Results
3.1. Participants’ Demographic and Clinical Characteristics
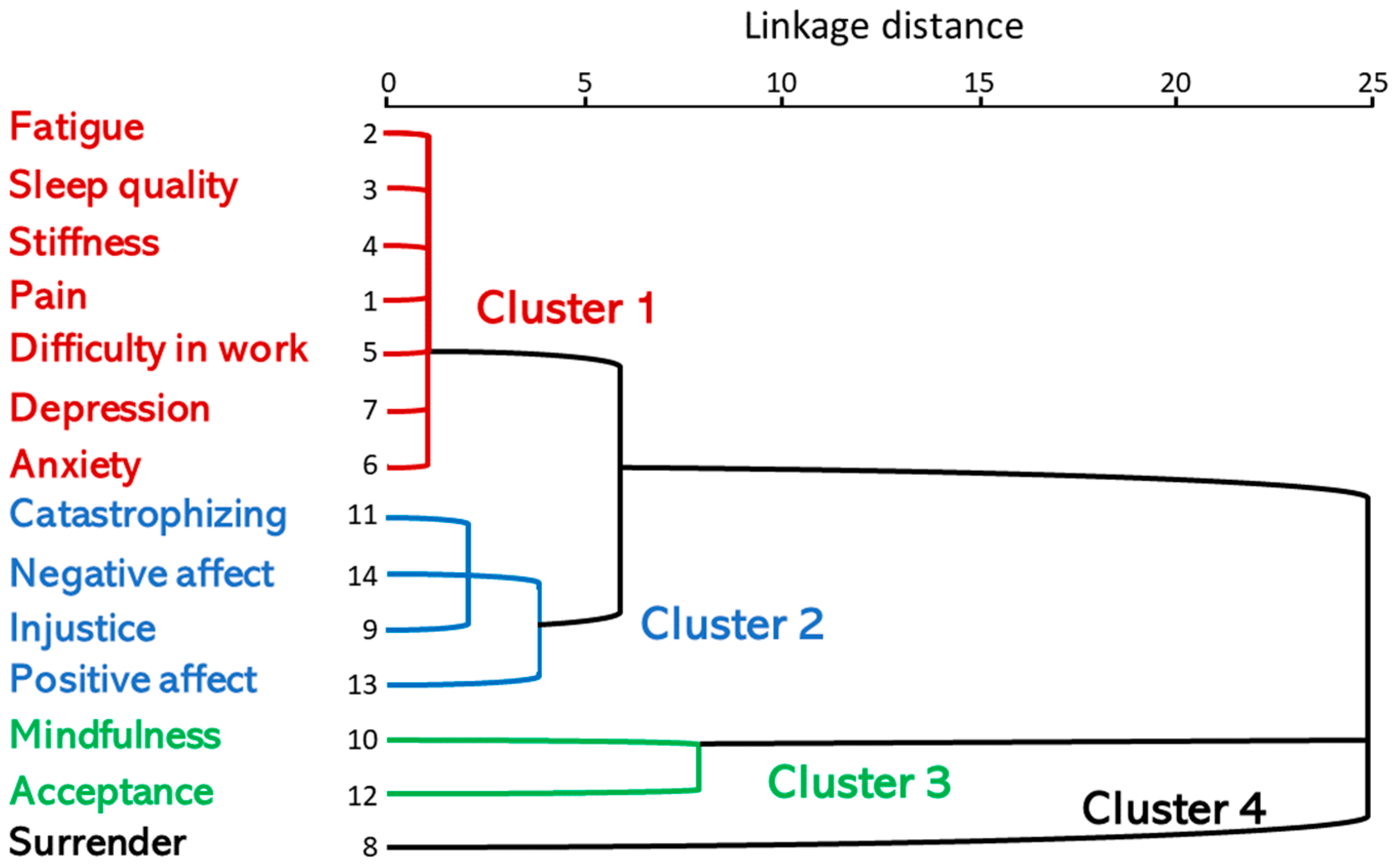
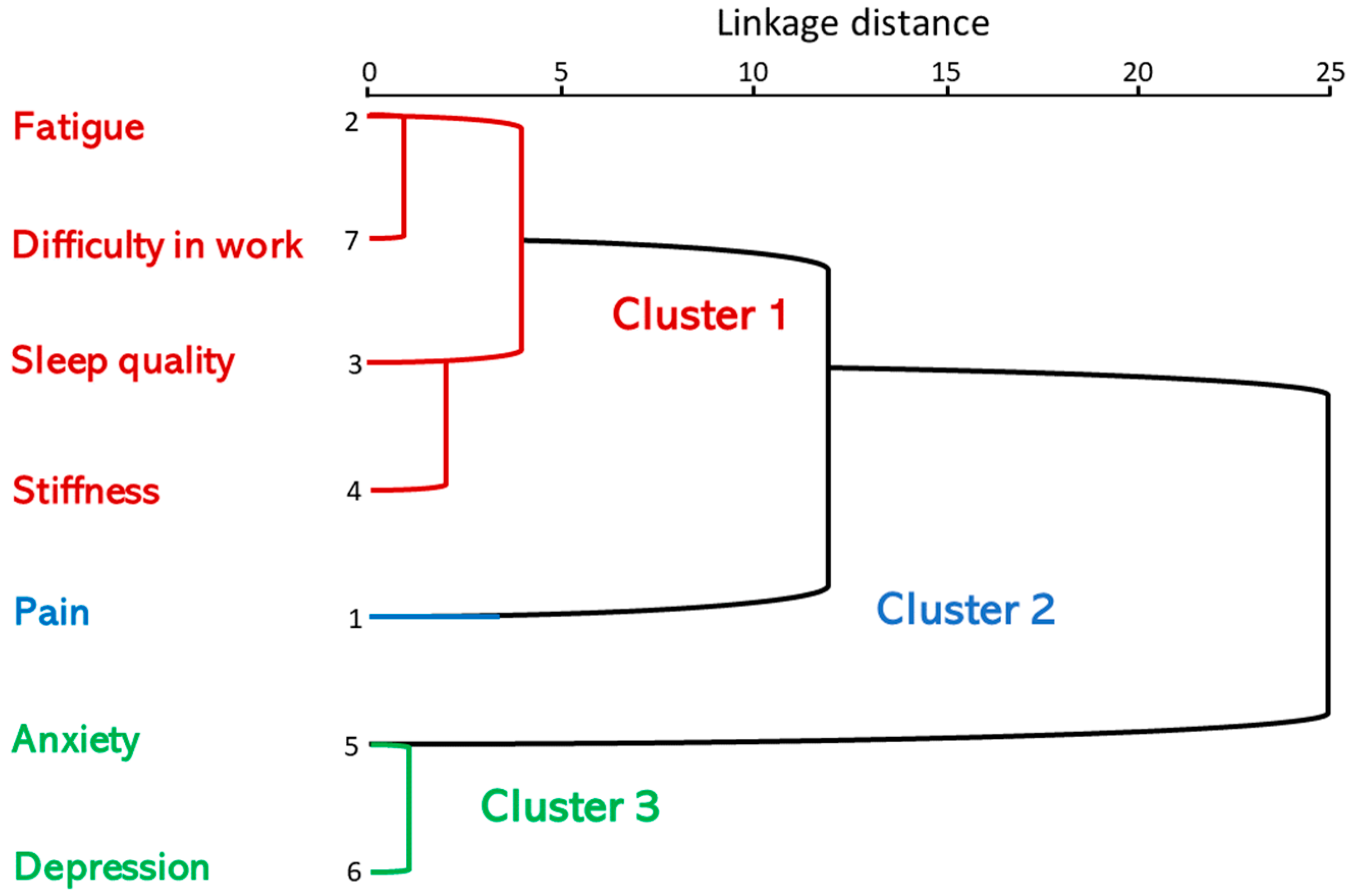
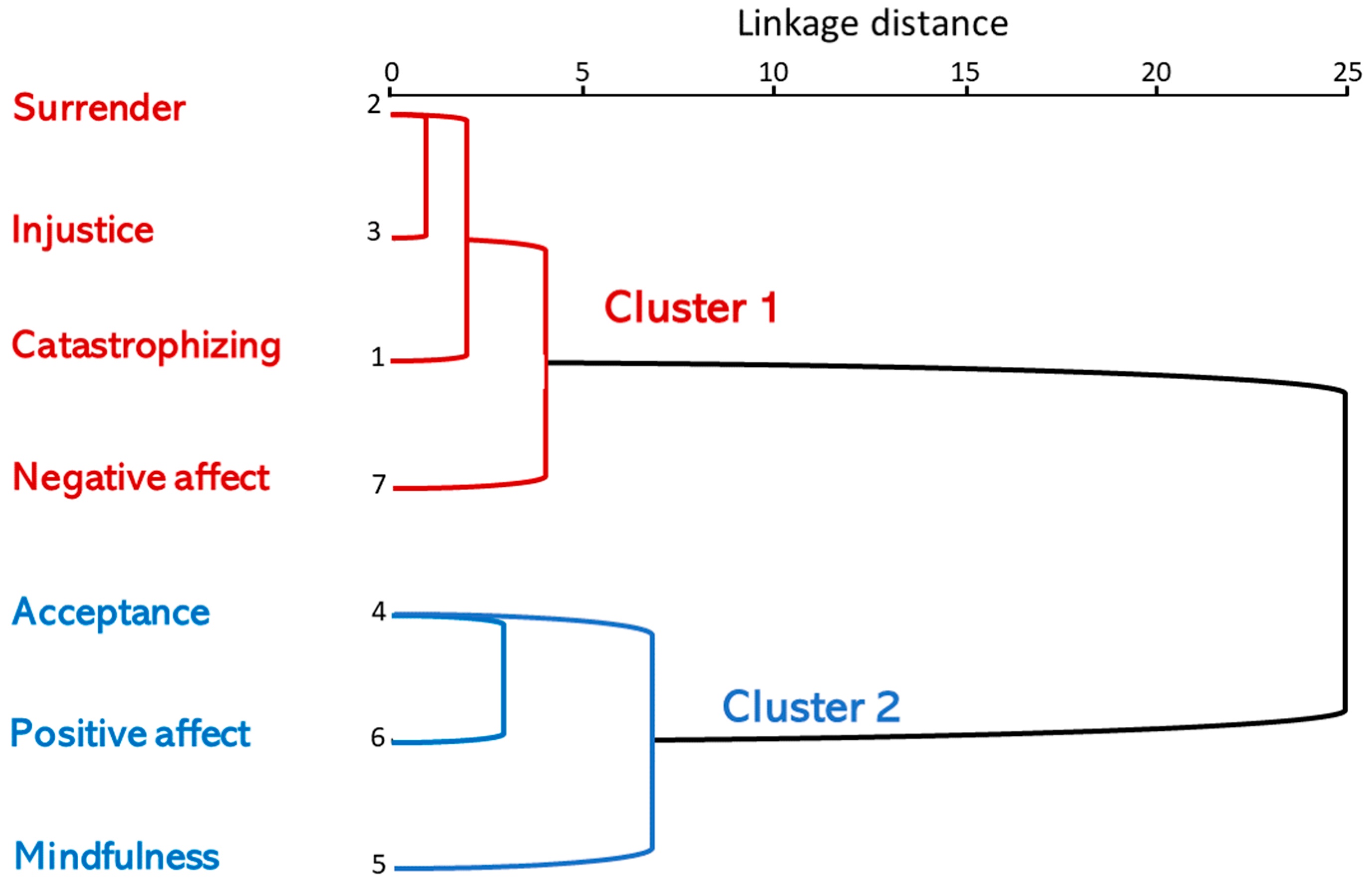
3.2. Cluster Analysis of Clinical and Neuropsychological Parameters
3.3. Combination of Rescaled Distance Clusters
4. Discussion
Study Limitations
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nishishinya, M.B.; Rivera, J.; Alegre, C.; Pereda, C.A. Non pharmacologic and alternative treatments in fibromyalgia. Med. Clin. 2006, 127, 295–299. [Google Scholar] [CrossRef]
- Casanueva, B.; Garcia-Fructuoso, F.; Belenguer, R.; Alegre, C.; Moreno-Muelas, J.V.; Hernandez, J.L.; Pina, T.; Gonzalez-Gay, M.A. The Spanish version of the 2010 American College of Rheumatology Preliminary Diagnostic Criteria for fibromyalgia: Reliability and validity assessment. Clin. Exp. Rheumatol. 2016, 34, S55–S58. [Google Scholar] [PubMed]
- Arnold, L.M. The pathophysiology, diagnosis and treatment of fibromyalgia. Psychiatr. Clin. N. Am. 2010, 33, 375–408. [Google Scholar] [CrossRef] [PubMed]
- Neumann, L.; Berzak, A.; Buskila, D. Measuring health status in Israeli patients with fibromyalgia syndrome and widespread pain and healthy individuals: Utility of the short form 36-item health survey (SF-36). Semin. Arthritis Rheum. 2000, 29, 400–408. [Google Scholar] [CrossRef]
- Sansone, R.A.; Levengood, J.V.; Sellbom, M. Psychological aspects of fibromyalgia: Research vs. clinician impressions. J. Psychosom. Res. 2004, 56, 185–188. [Google Scholar] [CrossRef]
- Dersh, J.; Polatin, P.B.; Gatchel, R.J. Chronic pain and psychopathology: Research findings and theoretical considerations. Psychosom. Med. 2002, 64, 773–786. [Google Scholar] [CrossRef]
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol. Bull. 2007, 133, 581–624. [Google Scholar] [CrossRef]
- Leadley, R.M.; Armstrong, N.; Lee, Y.C.; Allen, A.; Kleijnen, J. Chronic diseases in the European Union: The prevalence and health cost implications of chronic pain. J. Pain. Palliat. Care Pharmacother. 2012, 26, 310–325. [Google Scholar] [CrossRef]
- Munguia-Izquierdo, D.; Legaz-Arrese, A. Determinants of sleep quality in middle-aged women with fibromyalgia syndrome. J. Sleep. Res. 2012, 21, 73–79. [Google Scholar] [CrossRef]
- Kashikar-Zuck, S.; Lynch, A.M.; Graham, T.B.; Swain, N.F.; Mullen, S.M.; Noll, R.B. Social functioning and peer relationships of adolescents with juvenile fibromyalgia syndrome. Arthritis Rheum. 2007, 57, 474–480. [Google Scholar] [CrossRef]
- Vittori, A.; Cascella, M.; Leonardi, M.; Monaco, F.; Nocerino, D.; Cuomo, A.; Ottaiano, A.; Perri, F.; Mascilini, I.; Francia, E.; et al. VOSviewer-Based Bibliometric Network Analysis for Evaluating Research on Juvenile Primary Fibromyalgia Syndrome (JPFS). Children 2022, 9, 637. [Google Scholar] [CrossRef] [PubMed]
- Carmona, L.; Ballina, J.; Gabriel, R.; Laffon, A.; Group, E.S. The burden of musculoskeletal diseases in the general population of Spain: Results from a national survey. Ann. Rheum. Dis. 2001, 60, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Coles, M.L.; Uziel, Y. Juvenile primary fibromyalgia syndrome: A Review- Treatment and Prognosis. Pediatr. Rheumatol. Online J. 2021, 19, 74. [Google Scholar] [CrossRef]
- Rivera, J.; Alegre, C.; Nishishinya, M.B.; Pereda, C.A. Evidencias terapéuticas en fibromialgia. Reumatol. Clin. 2006, 2 (Suppl. 1), S34–S37. [Google Scholar] [CrossRef]
- Thieme, K.; Turk, D.C.; Flor, H. Comorbid depression and anxiety in fibromyalgia syndrome: Relationship to somatic and psychosocial variables. Psychosom. Med. 2004, 66, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Price, D.D.; Staud, R. Neurobiology of fibromyalgia syndrome. J. Rheumatol. Suppl. 2005, 75, 22–28. [Google Scholar]
- Crofford, L.J. The relationship of fibromyalgia to neuropathic pain syndromes. J. Rheumatol. Suppl. 2005, 75, 41–45. [Google Scholar]
- Giesecke, T.; Williams, D.A.; Harris, R.E.; Cupps, T.R.; Tian, X.; Tian, T.X.; Gracely, R.H.; Clauw, D.J. Subgrouping of fibromyalgia patients on the basis of pressure-pain thresholds and psychological factors. Arthritis Rheum. 2003, 48, 2916–2922. [Google Scholar] [CrossRef]
- Esteve-Vives, J.; Rivera Redondo, J.; Isabel Salvat Salvat, M.; de Gracia Blanco, M.; de Miquel, C.A. Proposal for a consensus version of the Fibromyalgia Impact Questionnaire (FIQ) for the Spanish population. Reumatol. Clin. 2007, 3, 21–24. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Clark, S.R.; Bennett, R.M. The fibromyalgia impact questionnaire: Development and validation. J. Rheumatol. 1991, 18, 728–733. [Google Scholar]
- Herrero, M.J.; Blanch, J.; Peri, J.M.; De Pablo, J.; Pintor, L.; Bulbena, A. A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen. Hosp. Psychiatry 2003, 25, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Rodero, B.; Garcia-Campayo, J.; Casanueva, B.; del Hoyo, Y.L.; Serrano-Blanco, A.; Luciano, J.V. Validation of the Spanish version of the Chronic Pain Acceptance Questionnaire (CPAQ) for the assessment of acceptance in fibromyalgia. Health Qual. Life Outcomes 2010, 8, 37. [Google Scholar] [CrossRef] [PubMed]
- Soler, J.; Tejedor, R.; Feliu-Soler, A.; Pascual, J.C.; Cebolla, A.; Soriano, J.; Alvarez, E.; Perez, V. Psychometric proprieties of Spanish version of Mindful Attention Awareness Scale (MAAS). Actas Esp. Psiquiatr. 2012, 40, 19–26. [Google Scholar] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Garcia Campayo, J.; Rodero, B.; Alda, M.; Sobradiel, N.; Montero, J.; Moreno, S. Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia. Med. Clin. 2008, 131, 487–492. [Google Scholar] [CrossRef]
- Garcia-Campayo, J.; Rodero, B.; del Hoyo, Y.L.; Luciano, J.V.; Alda, M.; Gili, M. Validation of a Spanish language version of the pain self-perception scale in patients with fibromyalgia. BMC Musculoskelet. Disord. 2010, 11, 255. [Google Scholar] [CrossRef]
- Wicksell, R.K.; Renofalt, J.; Olsson, G.L.; Bond, F.W.; Melin, L. Avoidance and cognitive fusion--central components in pain related disability? Development and preliminary validation of the Psychological Inflexibility in Pain Scale (PIPS). Eur. J. Pain. 2008, 12, 491–500. [Google Scholar] [CrossRef]
- Rodero, B.; Luciano, J.V.; Montero-Marin, J.; Casanueva, B.; Palacin, J.C.; Gili, M.; Lopez del Hoyo, Y.; Serrano-Blanco, A.; Garcia-Campayo, J. Perceived injustice in fibromyalgia: Psychometric characteristics of the Injustice Experience Questionnaire and relationship with pain catastrophising and pain acceptance. J. Psychosom. Res. 2012, 73, 86–91. [Google Scholar] [CrossRef]
- Sullivan, M.J.; Adams, H.; Horan, S.; Maher, D.; Boland, D.; Gross, R. The role of perceived injustice in the experience of chronic pain and disability: Scale development and validation. J. Occup. Rehabil. 2008, 18, 249–261. [Google Scholar] [CrossRef]
- Belenguer, R.; Ramos-Casals, M.; Siso, A.; Rivera, J. Classification of fibromyalgia. A systematic review of the literature. Reumatol. Clin. 2009, 5, 55–62. [Google Scholar] [CrossRef]
- de Souza, J.B.; Goffaux, P.; Julien, N.; Potvin, S.; Charest, J.; Marchand, S. Fibromyalgia subgroups: Profiling distinct subgroups using the Fibromyalgia Impact Questionnaire. A preliminary study. Rheumatol. Int. 2009, 29, 509–515. [Google Scholar] [CrossRef]
- Muller, W.; Schneider, E.M.; Stratz, T. The classification of fibromyalgia syndrome. Rheumatol. Int. 2007, 27, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Turk, D.C. The potential of treatment matching for subgroups of patients with chronic pain: Lumping versus splitting. Clin. J. Pain. 2005, 21, 44–55; discussion 69–72. [Google Scholar] [CrossRef] [PubMed]
- de Miquel, C.A.; Campayo, J.; Florez, M.T.; Arguelles, J.M.; Tarrio, E.B.; Montoya, M.G.; Martin, A.; Salio, A.M.; Fuentes, J.V.; Alberch, E.A.; et al. Interdisciplinary consensus document for the treatment of fibromyalgia. Actas Esp. Psiquiatr. 2010, 38, 108–120. [Google Scholar] [PubMed]
- Porter-Moffitt, S.; Gatchel, R.J.; Robinson, R.C.; Deschner, M.; Posamentier, M.; Polatin, P.; Lou, L. Biopsychosocial profiles of different pain diagnostic groups. J. Pain. 2006, 7, 308–318. [Google Scholar] [CrossRef]
- Fietta, P.; Fietta, P.; Manganelli, P. Fibromyalgia and psychiatric disorders. Acta Biomed. 2007, 78, 88–95. [Google Scholar]
- Epstein, S.A.; Kay, G.; Clauw, D.; Heaton, R.; Klein, D.; Krupp, L.; Kuck, J.; Leslie, V.; Masur, D.; Wagner, M.; et al. Psychiatric disorders in patients with fibromyalgia. A multicenter investigation. Psychosomatics 1999, 40, 57–63. [Google Scholar] [CrossRef]
- Rawlett, K.E.; Friedmann, E.; Thomas, S.A. Mindfulness based intervention with an attentional comparison group in at risk young adolescents: A pilot randomized controlled trial. Integr. Med. Res. 2019, 8, 101–106. [Google Scholar] [CrossRef]
- Verra, M.L.; Angst, F.; Brioschi, R.; Lehmann, S.; Keefe, F.J.; Staal, J.B.; de Bie, R.A.; Aeschlimann, A. Does classification of persons with fibromyalgia into Multidimensional Pain Inventory subgroups detect differences in outcome after a standard chronic pain management program? Pain. Res. Manag. 2009, 14, 445–453. [Google Scholar] [CrossRef]
- Hassett, A.L.; Simonelli, L.E.; Radvanski, D.C.; Buyske, S.; Savage, S.V.; Sigal, L.H. The relationship between affect balance style and clinical outcomes in fibromyalgia. Arthritis Rheum. 2008, 59, 833–840. [Google Scholar] [CrossRef]
- Boersma, K.; Linton, S.J. Screening to identify patients at risk: Profiles of psychological risk factors for early intervention. Clin. J. Pain. 2005, 21, 38–43; discussion 69–72. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhao, Y.; Shone, F.; Li, Z.; Frangi, A.F.; Xie, S.Q.; Zhang, Z.Q. Physics-informed Deep Learning for Musculoskeletal Modelling: Predicting Muscle Forces and Joint Kinematics from Surface EMG. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 31, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Li, Y.; Xiao, W.; Zhang, Z. Online Spatiotemporal Modeling for Robust and Lightweight Device-Free Lo-calization in Nonstationary Environments. IEEE Trans. Ind. Inform. 2023, 19, 8528–8538. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) or Mean ± SD |
|---|---|
| Age (years) | 52.4 ± 8 |
| Gender (F/M) | 241 (96.1)/10 (3.9) |
| Illness duration at diagnosis (years) | 10.2 ± 9.3 |
| Illness duration at inclusion (years) | 18.3 ± 11.1 |
| Current smoking | 70 (27.9) |
| Ex-smoker (≥1 year) | 50 (20) |
| Non-smoker | 131 (52.2) |
| Marital status | |
| Married/living with partner | 185 (73.7) |
| Separated/divorced | 32 (12.8) |
| Single | 23 (9.2) |
| Widower | 11 (4.3) |
| Place of residence | |
| Zaragoza | 221 (88.1) |
| Huesca | 20 (7.9) |
| Teruel | 10 (3.9) |
| Living arrangements | |
| Living with partner/spouse and children | 119 (47.4) |
| Living with partner/spouse | 80 (31.8) |
| Living alone | 28 (11.2) |
| Living with other family | 10 (3.9) |
| Others | 14 (5.6) |
| Education | |
| Finished primary school | 116 (46.2) |
| Finished secondary school | 95 (37.8) |
| University graduate | 32 (12.8) |
| No qualifications | 8 (3.2) |
| Employment | |
| Employed | 63 (25.1) |
| Disabled | 53 (21.1) |
| Unemployed | 38 (15.1) |
| Retired | 34 (13.5) |
| Homemaker | 32 (12.7) |
| Sick leave | 31 (12.3) |
| Comorbid health conditions | |
| Chronic neck pain | 238 (94.8) |
| Low back pain | 230 (91.6) |
| Dry eyes | 223 (88.8) |
| Anxiety/Depression | 175 (69.7) |
| Cephalea/Migraine | 193 (76.9) |
| Intestinal bowel syndrome | 187 (74.5) |
| Menopause | 169 (67.3) |
| Osteoarthritis | 153 (60.9) |
| Rheumatoid arthritis | 61 (24.3) |
| Stage | Cluster * 1 | Cluster * 2 | Coefficients | Cluster ** 1 | Cluster ** 2 | Next Stage |
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 886.000 | 0 | 0 | 3 |
| 2 | 1 | 5 | 972.250 | 0 | 0 | 4 |
| 3 | 2 | 4 | 1058.000 | 1 | 0 | 4 |
| 4 | 1 | 2 | 1560.958 | 2 | 3 | 5 |
| 5 | 1 | 7 | 4534.450 | 4 | 0 | 6 |
| 6 | 1 | 6 | 7649.042 | 5 | 0 | 10 |
| 7 | 11 | 14 | 31,097.000 | 0 | 0 | 8 |
| 8 | 9 | 11 | 36,317.500 | 0 | 7 | 9 |
| 9 | 9 | 13 | 77,097.667 | 8 | 0 | 10 |
| 10 | 1 | 9 | 108,588.036 | 6 | 9 | 12 |
| 11 | 10 | 12 | 151,021.000 | 0 | 0 | 12 |
| 12 | 1 | 10 | 513,915.114 | 10 | 11 | 13 |
| 13 | 1 | 8 | 526,653.865 | 12 | 0 | 0 |
| Variables | Pain | Fatigue | Sleep | Stiffness | Anxiety | Depression | Difficulty at Work |
|---|---|---|---|---|---|---|---|
| Pain | 0.0000 | 206.240 | 283.696 | 232.052 | 329.424 | 314.157 | 191.962 |
| Fatigue | 206.240 | 0.0000 | 189.356 | 185.192 | 286.871 | 259.451 | 173.276 |
| Sleep | 283.696 | 189.356 | 0.0000 | 182.618 | 352.678 | 324.184 | 207.396 |
| Stiffness | 232.052 | 185.192 | 182.618 | 0.0000 | 312.836 | 279.140 | 182.064 |
| Anxiety | 329.424 | 286.871 | 352.678 | 312.836 | 0.0000 | 173.849 | 233.890 |
| Depression | 314.157 | 259.451 | 324.184 | 279.140 | 173.849 | 0.0000 | 227.812 |
| Difficulty at work | 191.962 | 173.276 | 207.396 | 182.064 | 233.890 | 227.812 | 0.0000 |
| Stage | Cluster * 1 | Cluster * 2 | Coefficients | Cluster ** 1 | Cluster ** 2 | Next Stage |
|---|---|---|---|---|---|---|
| 1 | 2 | 7 | 173.276 | 0 | 0 | 4 |
| 2 | 5 | 6 | 173.849 | 0 | 0 | 6 |
| 3 | 3 | 4 | 182.618 | 0 | 0 | 4 |
| 4 | 2 | 3 | 191.002 | 1 | 3 | 5 |
| 5 | 1 | 2 | 228.488 | 0 | 4 | 6 |
| 6 | 1 | 5 | 292.044 | 5 | 2 | 0 |
| Variables | Catastrophizing | Surrender | Mindfulness | Acceptance | Injustice | Positive Affect | Negative Affect |
|---|---|---|---|---|---|---|---|
| Catastrophizing | 0.0000 | 155.560 | 169.251 | 813.405 | 706.444 | 733.237 | 211.856 |
| Surrender | 155.560 | 0.0000 | 137.812 | 790.621 | 763.422 | 741.268 | 205.045 |
| Mindfulness | 169.251 | 137.812 | 0.0000 | 787.965 | 704.242 | 721.446 | 219.548 |
| Acceptance | 813.405 | 790.621 | 787.965 | 0.0000 | 298.573 | 192.085 | 742.781 |
| Injustice | 706.444 | 763.422 | 704.242 | 298.573 | 0.0000 | 278.596 | 703.264 |
| Positive affect | 733.237 | 741.268 | 721.446 | 192.085 | 278.596 | 0.0000 | 723.220 |
| Negative affect | 211.856 | 205.045 | 219.548 | 742.781 | 703.264 | 723.220 | 0.0000 |
| Stage | Cluster * 1 | Cluster * 2 | Coefficients | Cluster ** 1 | Cluster ** 2 | Next Stage |
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 137.812 | 0 | 0 | 2 |
| 2 | 1 | 2 | 162.406 | 0 | 1 | 4 |
| 3 | 4 | 6 | 192.085 | 0 | 0 | 5 |
| 4 | 1 | 7 | 212.150 | 2 | 0 | 6 |
| 5 | 4 | 5 | 288.584 | 3 | 0 | 6 |
| 6 | 1 | 4 | 744.276 | 4 | 5 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maurel, S.; Giménez-Llort, L.; Alegre-Martin, J.; Castro-Marrero, J. Hierarchical Cluster Analysis Based on Clinical and Neuropsychological Symptoms Reveals Distinct Subgroups in Fibromyalgia: A Population-Based Cohort Study. Biomedicines 2023, 11, 2867. https://doi.org/10.3390/biomedicines11102867
Maurel S, Giménez-Llort L, Alegre-Martin J, Castro-Marrero J. Hierarchical Cluster Analysis Based on Clinical and Neuropsychological Symptoms Reveals Distinct Subgroups in Fibromyalgia: A Population-Based Cohort Study. Biomedicines. 2023; 11(10):2867. https://doi.org/10.3390/biomedicines11102867
Chicago/Turabian StyleMaurel, Sara, Lydia Giménez-Llort, Jose Alegre-Martin, and Jesús Castro-Marrero. 2023. "Hierarchical Cluster Analysis Based on Clinical and Neuropsychological Symptoms Reveals Distinct Subgroups in Fibromyalgia: A Population-Based Cohort Study" Biomedicines 11, no. 10: 2867. https://doi.org/10.3390/biomedicines11102867
APA StyleMaurel, S., Giménez-Llort, L., Alegre-Martin, J., & Castro-Marrero, J. (2023). Hierarchical Cluster Analysis Based on Clinical and Neuropsychological Symptoms Reveals Distinct Subgroups in Fibromyalgia: A Population-Based Cohort Study. Biomedicines, 11(10), 2867. https://doi.org/10.3390/biomedicines11102867