
Prevalence and Factors Associated with Metabolic Syndrome among Non-Diabetic Saudi Adults: A Cross-Sectional Study

 ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
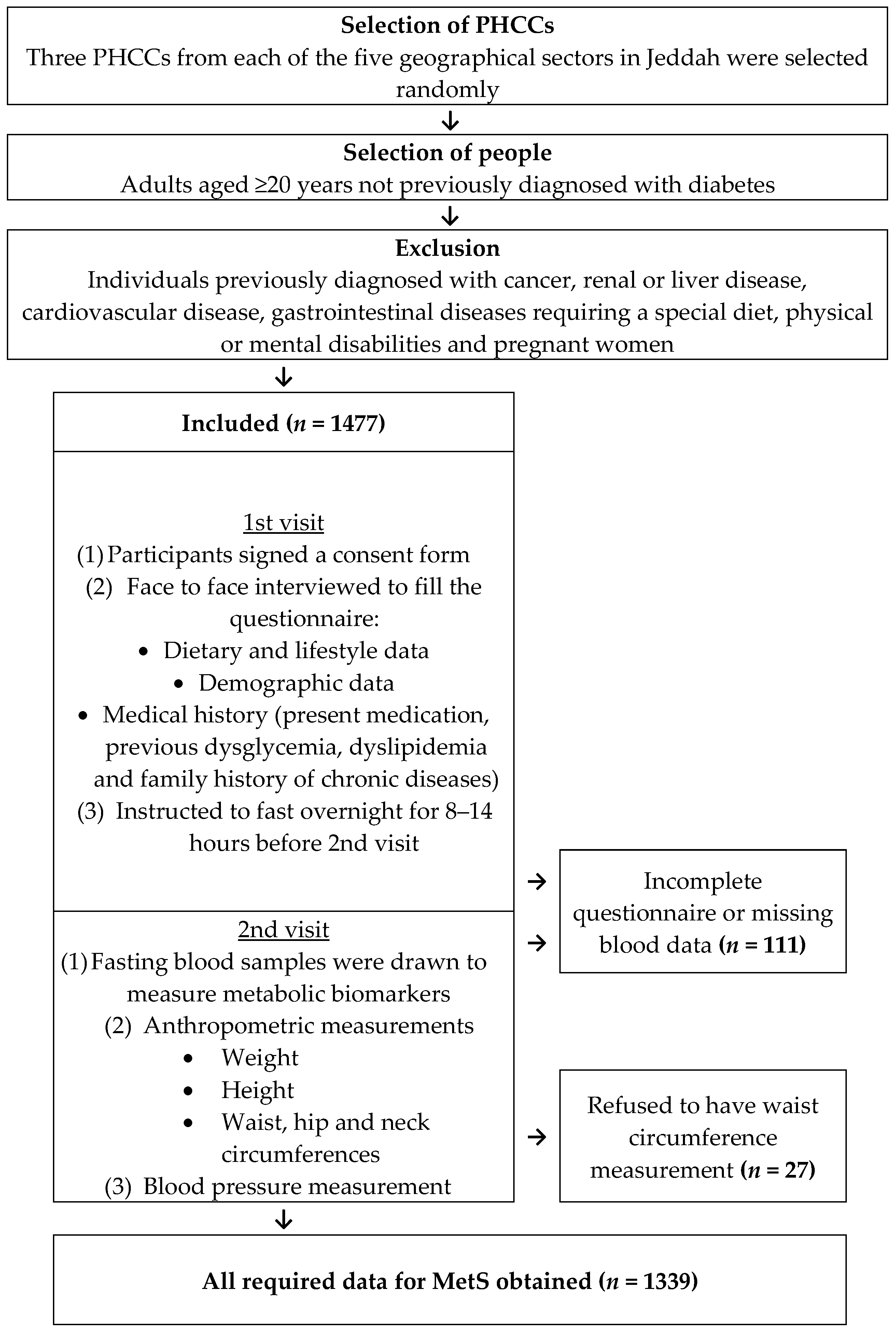
2.1. Study Design and Data Collection
2.2. Anthropometric Indices
2.3. Biochemical Assays
2.4. Definition of MetS
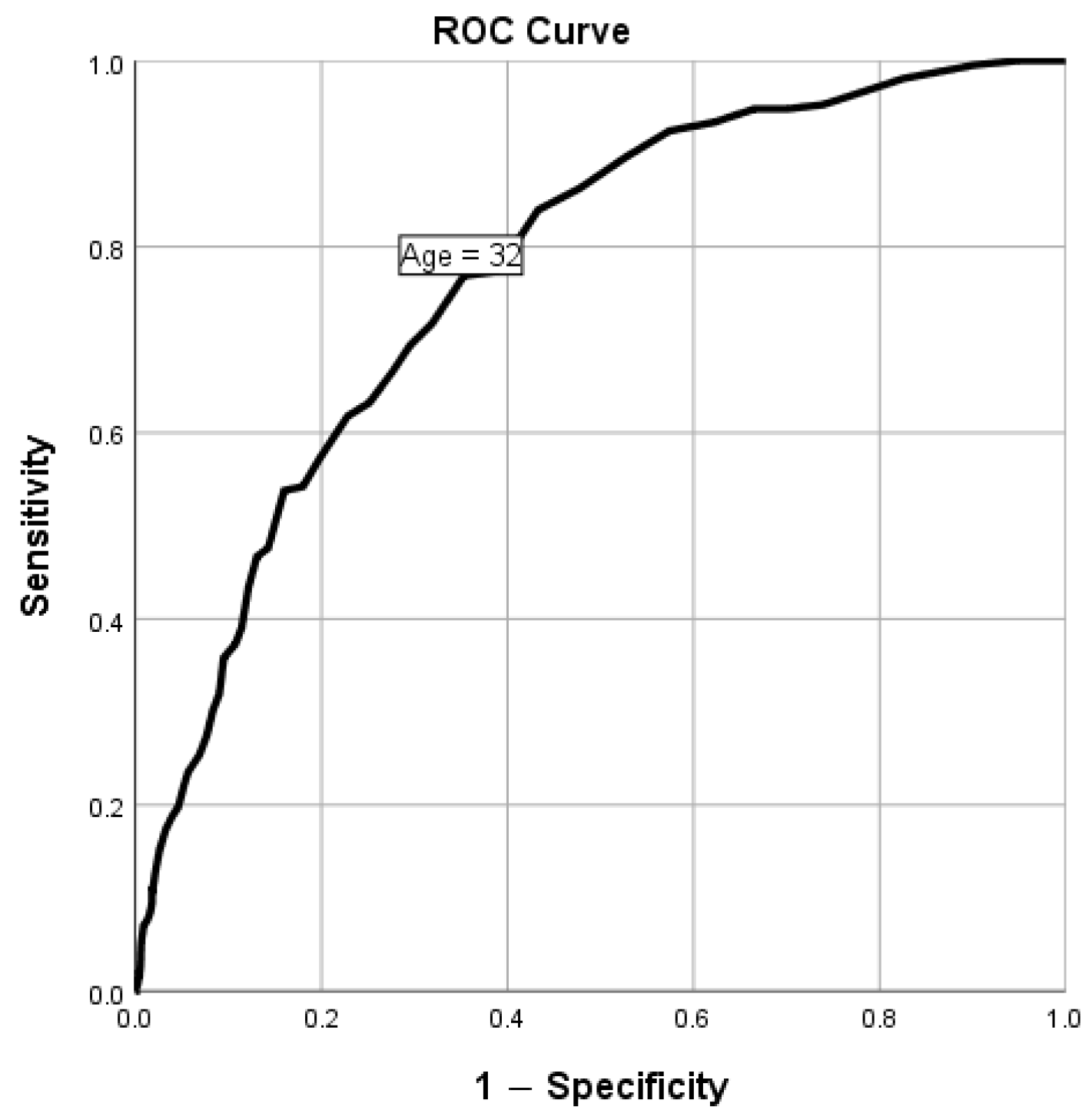
2.5. Statistical Analysis
3. Results
3.1. Association between MetS and Anthropometric Measurements
3.2. Prevalence of MetS and Its Components in Age and Sex Groups
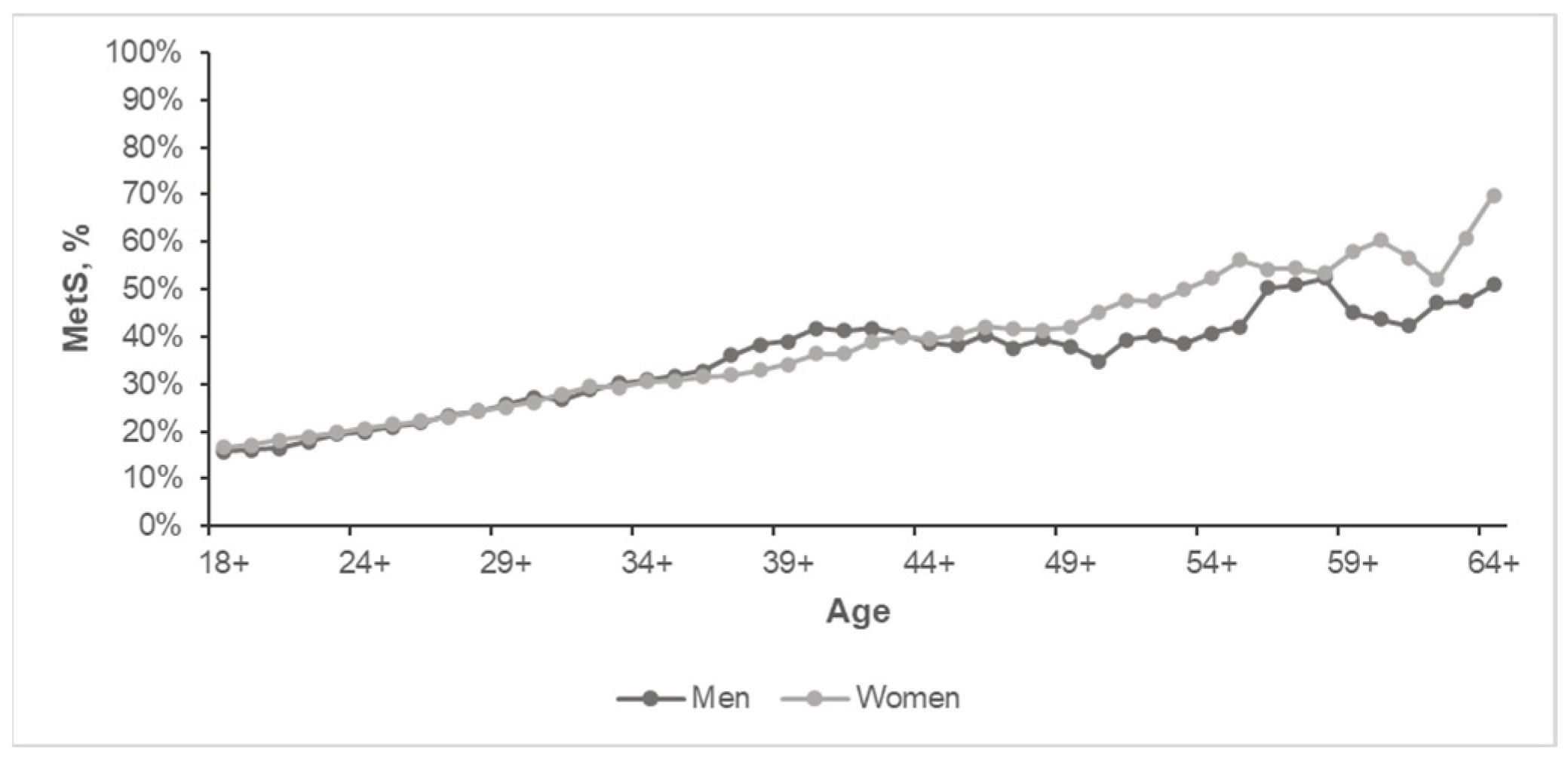
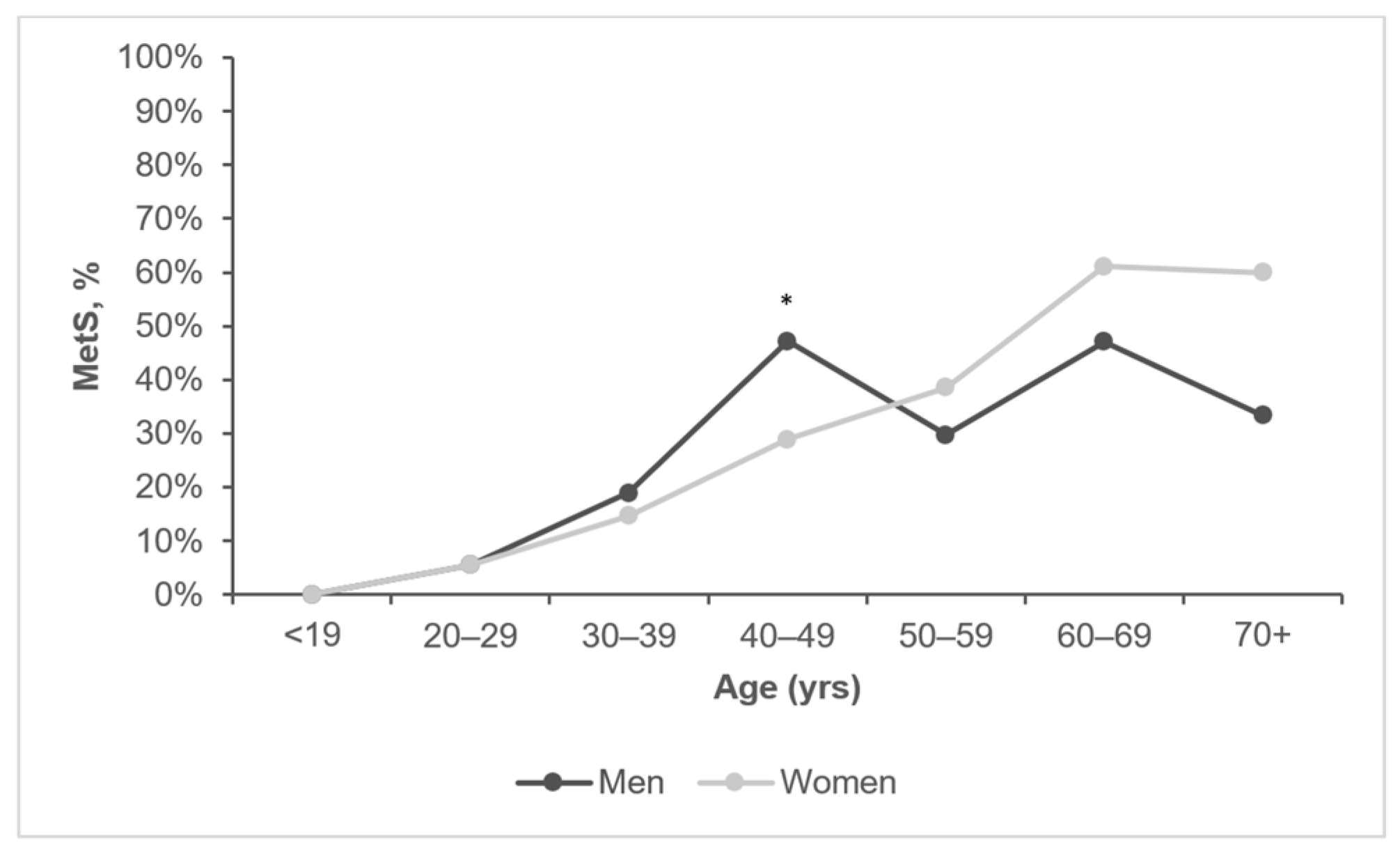
3.2.1. The Overall Prevalence of MetS by Age and Sex
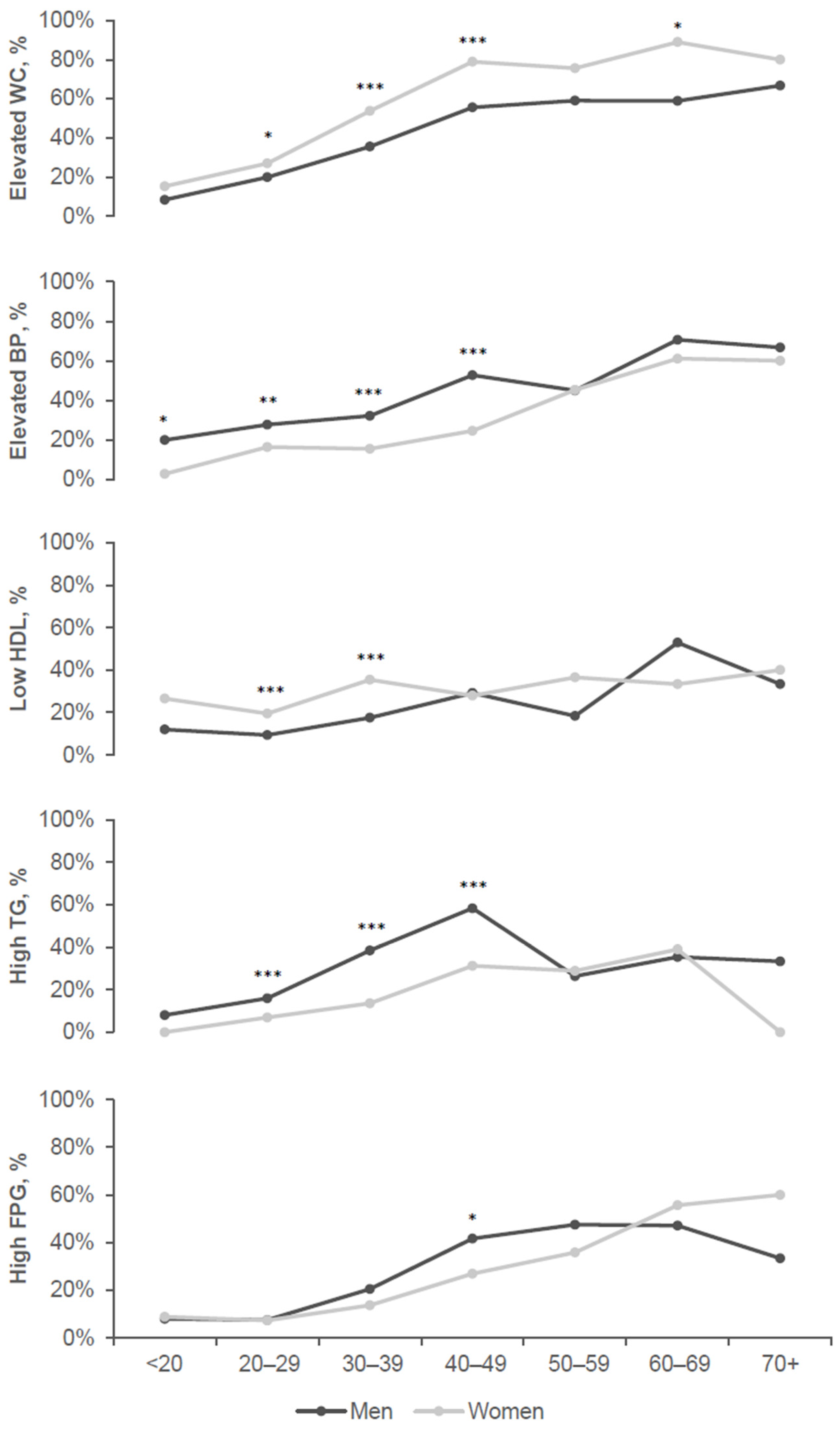
3.2.2. Prevalence of MetS Components by Age and Sex
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Isomaa, B. A major health hazard: The metabolic syndrome. Life Sci. 2003, 73, 2395–2411. [Google Scholar] [CrossRef] [PubMed]
- Scott, C.L. Diagnosis, prevention, and intervention for the metabolic syndrome. Am. J. Cardiol. 2003, 92, 35i–42i. [Google Scholar] [CrossRef] [PubMed]
- Lakka, H.M.; Laaksonen, D.E.; Lakka, T.A.; Niskanen, L.K.; Kumpusalo, E.; Tuomilehto, J.; Salonen, J.T. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA 2002, 288, 2709–2716. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: A summary of the evidence. Diabetes Care 2005, 28, 1769–1778. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Q.; The, D.S.G. Comparison of different definitions of the metabolic syndrome in relation to cardiovascular mortality in European men and women. Diabetologia 2006, 49, 2837–2846. [Google Scholar] [CrossRef] [PubMed]
- Akbar, D. Metabolic syndrome is common in Saudi type 2 diabetic patients. Hypertension 2002, 12, 47–49. [Google Scholar]
- Al-Nozha, M.; Al-Khadra, A.; Arafah, M.R.; Al-Maatouq, M.A.; Khalil, M.Z.; Khan, N.B.; Al-Mazrou, Y.Y.; Al-Marzouki, K.; Al-Harthi, S.S.; Abdullah, M.; et al. Metabolic syndrome in Saudi Arabia. Saudi Med. J. 2005, 26, 1918. [Google Scholar]
- Al-Qahtani, D.A.; Imtiaz, M.L. Prevalence of metabolic syndrome in Saudi adult soldiers. Saudi Med. J. 2005, 26, 1360–1366. [Google Scholar]
- Al-Qahtani, D.A.; Imtiaz, M.L.; Saad, O.S.; Hussein, N.M. AComparison of the Prevalence of Metabolic Syndrome in Saudi Adult Females Using Two Definitions. Metab. Syndr. Relat. Disord. 2006, 4, 204–214. [Google Scholar] [CrossRef]
- Barrimah, I.E.; Mohaimeed, A.R.; Midhat, F.; Al-Shobili, H.A. Prevalence of metabolic syndrome among qassim university personnel in saudi arabia. Int. J. Health Sci. 2009, 3, 133–142. [Google Scholar]
- Al-Daghri, N.M.; Al-Attas, O.S.; Alokail, M.S.; Alkharfy, K.M.; Sabico, S.L.B.; Chrousos, G.P. Decreasing Prevalence of the Full Metabolic Syndrome but a Persistently High Prevalence of Dyslipidemia among Adult Arabs. PLoS ONE 2010, 5, e12159. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, A.M.; Karawagh, A.M.; Alshahrani, F.M.; Naser, T.A.; Ahmed, A.A.; Alsharef, E.H. Prevalence and predictors of metabolic syndrome among healthy Saudi Adults. Br. J. Diabetes Vasc. Dis. 2012, 12, 78–80. [Google Scholar] [CrossRef]
- Bahijri, S.M.; Al Raddadi, R.M. The importance of local criteria in the diagnosis of metabolic syndrome in Saudi Arabia. Ther. Adv. Endocrinol. Metab. 2013, 4, 51–59. [Google Scholar] [CrossRef]
- Alberti, G.; Zimmet, P.; Shaw, J.; Grundy, S.M. The IDF consensus worldwide definition of the metabolic syndrome. Bruss. Int. Diabetes Fed. 2006, 23, 469–480. [Google Scholar]
- Expert Panel on Detection, E., and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Grundy, S.M. Metabolic syndrome: A multiplex cardiovascular risk factor. J. Clin. Endocrinol. Metab. 2007, 92, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Després, J.P.; Lemieux, I. Abdominal obesity and metabolic syndrome. Nature 2006, 444, 881–887. [Google Scholar] [CrossRef]
- Gami, A.S.; Witt, B.J.; Howard, D.E.; Erwin, P.J.; Gami, L.A.; Somers, V.K.; Montori, V.M. Metabolic syndrome and risk of incident cardiovascular events and death: A systematic review and meta-analysis of longitudinal studies. J. Am. Coll. Cardiol. 2007, 49, 403–414. [Google Scholar] [CrossRef]
- Mehta, S.; Ghosh, S.; Sander, S.; Kuti, E.; Mountford, W.K. Differences in All-Cause Health Care Utilization and Costs in a Type 2 Diabetes Mellitus Population with and Without a History of Cardiovascular Disease. J. Manag. Care Spec. Pharm. 2018, 24, 280–290. [Google Scholar] [CrossRef]
- Einarson, T.R.; Acs, A.; Ludwig, C.; Panton, U.H. Economic Burden of Cardiovascular Disease in Type 2 Diabetes: A Systematic Review. Value Health 2018, 21, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Al-Nozha, M.M.; Al-Maatouq, M.A.; Al-Mazrou, Y.Y.; Al-Harthi, S.S.; Arafah, M.R.; Khalil, M.Z.; Khan, N.B.; Al-Khadra, A.; Al-Marzouki, K.; Nouh, M.S.; et al. Diabetes mellitus in Saudi Arabia. Saudi Med. J. 2004, 25, 1603. [Google Scholar] [PubMed]
- Bahijri, S.M.; Jambi, H.A.; Al Raddadi, R.M.; Ferns, G.; Tuomilehto, J. The Prevalence of Diabetes and Prediabetes in the Adult Population of Jeddah, Saudi Arabia—A Community-Based Survey. PLoS ONE 2016, 11, e0152559. [Google Scholar] [CrossRef]
- NHS. Metabolic Syndrome. Available online: https://www.nhs.uk/conditions/metabolic-syndrome/ (accessed on 21 February 2023).
- Vickers, M.; Sloboda, D. Strategies for Reversing the Effects of Metabolic Disorders Induced as a Consequence of Developmental Programming. Front. Physiol. 2012, 3, 242. [Google Scholar] [CrossRef]
- Lindström, J.; Ilanne-Parikka, P.; Peltonen, M.; Aunola, S.; Eriksson, J.G.; Hemiö, K.; Hämäläinen, H.; Härkönen, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; et al. Sustained reduction in the incidence of type 2 diabetes by lifestyle intervention: Follow-up of the Finnish Diabetes Prevention Study. Lancet 2006, 368, 1673–1679. [Google Scholar] [CrossRef]
- Tuomilehto, J.; Lindström, J.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Prevention of Type 2 Diabetes Mellitus by Changes in Lifestyle among Subjects with Impaired Glucose Tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, J.; Louheranta, A.; Mannelin, M.; Rastas, M.; Salminen, V.; Eriksson, J.; Uusitupa, M.; Tuomilehto, J.; Finnish Diabetes Prevention Study Group. The Finnish Diabetes Prevention Study (DPS): Lifestyle intervention and 3-year results on diet and physical activity. Diabetes Care 2003, 26, 3230–3236. [Google Scholar] [CrossRef]
- Bahijri, S.; Al-Raddadi, R.; Ajabnoor, G.; Jambi, H.; Al Ahmadi, J.; Borai, A.; Barengo, N.C.; Tuomilehto, J. Dysglycemia risk score in Saudi Arabia: A tool to identify people at high future risk of developing type 2 diabetes. J. Diabetes Investig. 2020, 11, 844–855. [Google Scholar] [CrossRef]
- Sedgwick, P. Stratified cluster sampling. BMJ 2013, 347, f7016. [Google Scholar] [CrossRef]
- Eriksson, K.F.; Lindgärde, F. Prevention of Type 2 (non-insulin-dependent) diabetes mellitus by diet and physical exercise The 6-year Malm feasibility study. Diabetologia 1991, 34, 891–898. [Google Scholar] [CrossRef]
- Al-Lawati, J.A.; Tuomilehto, J. Diabetes risk score in Oman: A tool to identify prevalent type 2 diabetes among Arabs of the Middle East. Diabetes Res. Clin. Pract. 2007, 77, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.R.; Li, G.W.; Hu, Y.H.; Wang, J.X.; Yang, W.Y.; An, Z.X.; Hu, Z.X.; Lin, J.; Xiao, J.Z.; Cao, H.B.; et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance: The Da Qing IGT and Diabetes Study. Diabetes Care 1997, 20, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Kaczorowski, J.; Robinson, C.; Nerenberg, K.A. Development of the CANRISK questionnaire to screen for prediabetes and undiagnosed type 2 diabetes. Can. J. Diabetes 2009, 33, 381–385. [Google Scholar] [CrossRef]
- Makrilakis, K.; Liatis, S.; Grammatikou, S.; Perrea, D.; Stathi, C.; Tsiligros, P.; Katsilambros, N. Validation of the Finnish diabetes risk score (FINDRISC) questionnaire for screening for undiagnosed type 2 diabetes, dysglycaemia and the metabolic syndrome in Greece. Diabetes Metab. 2011, 37, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Phillips, L.S.; Ziemer, D.C.; Kolm, P.; Weintraub, W.S.; Vaccarino, V.; Rhee, M.K.; Chatterjee, R.; Narayan, K.M.; Koch, D.D. Glucose challenge test screening for prediabetes and undiagnosed diabetes. Diabetologia 2009, 52, 1798–1807. [Google Scholar] [CrossRef]
- Pareek, M.; Bhatt, D.L.; Nielsen, M.L.; Jagannathan, R.; Eriksson, K.F.; Nilsson, P.M.; Bergman, M.; Olsen, M.H. Enhanced Predictive Capability of a 1-Hour Oral Glucose Tolerance Test: A Prospective Population-Based Cohort Study. Diabetes Care 2018, 41, 171–177. [Google Scholar] [CrossRef]
- Orchard, T.J.; Temprosa, M.; Goldberg, R.; Haffner, S.; Ratner, R.; Marcovina, S.; Fowler, S. The effect of metformin and intensive lifestyle intervention on the metabolic syndrome: The Diabetes Prevention Program randomized trial. Ann. Intern. Med. 2005, 142, 611–619. [Google Scholar] [CrossRef]
- Kaur, G.; Mukundan, S.; Wani, V.; Kumar, M.S. Nutraceuticals in the management and prevention of metabolic syndrome. Austin J. Pharmacol. Ther. 2015, 3, 1063. [Google Scholar]
- Yamaoka, K.; Tango, T. Effects of lifestyle modification on metabolic syndrome: A systematic review and meta-analysis. BMC Med. 2012, 10, 138. [Google Scholar] [CrossRef]
- Ilanne-Parikka, P.; Eriksson, J.G.; Lindstrom, J.; Peltonen, M.; Aunola, S.; Hamalainen, H.; Keinanen-Kiukaanniemi, S.; Laakso, M.; Valle, T.T.; Lahtela, J.; et al. Effect of Lifestyle Intervention on the Occurrence of Metabolic Syndrome and its Components in the Finnish Diabetes Prevention Study. Diabetes Care 2008, 31, 805–807. [Google Scholar] [CrossRef]
- Al-Rubeaan, K.; Bawazeer, N.; Al Farsi, Y.; Youssef, A.M.; Al-Yahya, A.A.; AlQumaidi, H.; Al-Malki, B.M.; Naji, K.A.; Al-Shehri, K.; Al Rumaih, F.I. Prevalence of metabolic syndrome in Saudi Arabia—A cross sectional study. BMC Endocr. Disord. 2018, 18, 16. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S. Prevalence of the metabolic syndrome defined by the International Diabetes Federation among adults in the U.S. Diabetes Care 2005, 28, 2745–2749. [Google Scholar] [CrossRef] [PubMed]
- Balkau, B.; Vernay, M.; Mhamdi, L.; Novak, M.; Arondel, D.; Vol, S.; Tichet, J.; Eschwège, E. The incidence and persistence of the NCEP (National Cholesterol Education Program) metabolic syndrome. The French D.E.S.I.R. study. Diabetes Metab. 2003, 29, 526–532. [Google Scholar] [CrossRef]
- Cameron, A.J.; Shaw, J.E.; Zimmet, P.Z. The metabolic syndrome: Prevalence in worldwide populations. Endocrinol. Metab. Clin. N. Am. 2004, 33, 351–375, table of contents. [Google Scholar] [CrossRef] [PubMed]
- Fiuza, M.; Cortez-Dias, N.; Martins, S.; Belo, A. Metabolic syndrome in Portugal: Prevalence and implications for cardiovascular risk--results from the VALSIM Study. Rev. Port Cardiol. 2008, 27, 1495–1529. [Google Scholar]
- Cheung, B.M.; Ong, K.L.; Man, Y.B.; Wong, L.Y.; Lau, C.P.; Lam, K.S. Prevalence of the metabolic syndrome in the United States National Health and Nutrition Examination Survey 1999-2002 according to different defining criteria. J. Clin. Hypertens. 2006, 8, 562–570. [Google Scholar] [CrossRef]
- Prevalence of the metabolic syndrome in populations of Asian origin. Comparison of the IDF definition with the NCEP definition. Diabetes Res. Clin. Pract. 2007, 76, 57–67. [CrossRef]
- Santos, A.C.; Barros, H. Impact of metabolic syndrome definitions on prevalence estimates: A study in a Portuguese community. Diabetes Vasc. Dis. Res. 2007, 4, 320–327. [Google Scholar] [CrossRef]
- Park, D.; Shin, M.J.; Després, J.P.; Eckel, R.H.; Tuomilehto, J.; Lim, S. 20-Year Trends in Metabolic Syndrome Among Korean Adults From 2001 to 2020. JACC Asia 2023, 3, 491–502. [Google Scholar] [CrossRef]
- Hirode, G.; Wong, R.J. Trends in the Prevalence of Metabolic Syndrome in the United States, 2011–2016. JAMA 2020, 323, 2526–2528. [Google Scholar] [CrossRef] [PubMed]
- Sirdah, M.M.; Al Laham, N.A.; Abu Ghali, A.S. Prevalence of metabolic syndrome and associated socioeconomic and demographic factors among Palestinian adults (20–65 years) at the Gaza Strip. Diabetes Metab. Syndr. 2011, 5, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Delavar, M.A.; Lye, M.S.; Khor, G.L.; Hanachi, P.; Hassan, S.T. Prevalence of metabolic syndrome among middle aged women in Babol, Iran. Southeast Asian J. Trop. Med. Public Health 2009, 40, 612–628. [Google Scholar] [PubMed]
- Rguibi, M.; Belahsen, R. Overweight and obesity among urban Sahraoui women of South Morocco. Ethn. Dis. 2004, 14, 542–547. [Google Scholar]
- Al-Daghri, N.M.; Alkharfy, K.M.; Al-Attas, O.S.; Khan, N.; Alfawaz, H.A.; Alghanim, S.A.; Al-Yousef, M.A.; Al-Ajlan, A.S.; Alokail, M.S. Gender-dependent associations between socioeconomic status and metabolic syndrome: A cross-sectional study in the adult Saudi population. BMC Cardiovasc. Disord. 2014, 14, 51. [Google Scholar] [CrossRef]
- Santos, A.C.; Ebrahim, S.; Barros, H. Gender, socioeconomic status and metabolic syndrome in middle-aged and old adults. BMC Public Health 2008, 8, 62. [Google Scholar] [CrossRef]
- Ferguson, T.S.; Younger, N.; Tulloch-Reid, M.K.; Forrester, T.E.; Cooper, R.S.; Van den Broeck, J.; Wilks, R.J. Prevalence of the metabolic syndrome in Jamaican adults and its relationship to income and education levels. West Indian Med. J. 2010, 59, 265–273. [Google Scholar]
- Park, S.J.; Kang, H.T.; Nam, C.M.; Park, B.J.; Linton, J.A.; Lee, Y.J. Sex differences in the relationship between socioeconomic status and metabolic syndrome: The Korean National Health and Nutrition Examination Survey. Diabetes Res. Clin. Pract. 2012, 96, 400–406. [Google Scholar] [CrossRef]
- Allal-Elasmi, M.; Haj Taieb, S.; Hsairi, M.; Zayani, Y.; Omar, S.; Sanhaji, H.; Jemaa, R.; Feki, M.; Elati, J.; Mebazaa, A.; et al. The metabolic syndrome: Prevalence, main characteristics and association with socioeconomic status in adults living in Great Tunis. Diabetes Metab. 2010, 36, 204–208. [Google Scholar] [CrossRef]
- Cena, H.; Fonte, M.L.; Turconi, G. Relationship between smoking and metabolic syndrome. Nutr. Rev. 2011, 69, 745–753. [Google Scholar] [CrossRef]
- Miyatake, N.; Wada, J.; Kawasaki, Y.; Nishii, K.; Makino, H.; Numata, T. Relationship between metabolic syndrome and cigarette smoking in the Japanese population. Intern. Med. 2006, 45, 1039–1043. [Google Scholar] [CrossRef]
- Kim, S.W.; Kim, H.J.; Min, K.; Lee, H.; Lee, S.H.; Kim, S.; Kim, J.S.; Oh, B. The relationship between smoking cigarettes and metabolic syndrome: A cross-sectional study with non-single residents of Seoul under 40 years old. PLoS ONE 2021, 16, e0256257. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Liu, J.; Ning, G. Active smoking and risk of metabolic syndrome: A meta-analysis of prospective studies. PLoS ONE 2012, 7, e47791. [Google Scholar] [CrossRef]
- O’Neill, S.; O’Driscoll, L. Metabolic syndrome: A closer look at the growing epidemic and its associated pathologies. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2015, 16, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Zappalà, G.; Bernardini, S.; Giambini, I.; Bes-Rastrollo, M.; Martinez-Gonzalez, M. Adherence to the Mediterranean diet is inversely associated with metabolic syndrome occurrence: A meta-analysis of observational studies. Int. J. Food Sci. Nutr. 2017, 68, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Enani, S.; Bahijri, S.; Malibary, M.; Jambi, H.; Eldakhakhny, B.; Al-Ahmadi, J.; Al Raddadi, R.; Ajabnoor, G.; Boraie, A.; Tuomilehto, J. The Association between Dyslipidemia, Dietary Habits and Other Lifestyle Indicators among Non-Diabetic Attendees of Primary Health Care Centers in Jeddah, Saudi Arabia. Nutrients 2020, 12, 2441. [Google Scholar] [CrossRef]
- Hong, S.; Song, Y.; Lee, K.H.; Lee, H.S.; Lee, M.; Jee, S.H.; Joung, H. A fruit and dairy dietary pattern is associated with a reduced risk of metabolic syndrome. Metab. Clin. Exp. 2012, 61, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Viscogliosi, G.; Cipriani, E.; Liguori, M.L.; Marigliano, B.; Saliola, M.; Ettorre, E.; Andreozzi, P. Mediterranean dietary pattern adherence: Associations with prediabetes, metabolic syndrome, and related microinflammation. Metab. Syndr. Relat. Disord. 2013, 11, 210–216. [Google Scholar] [CrossRef]
- Fallah, Z.; Darand, M.; Salehi-Abargouei, A.; Mirzaei, M.; Ferns, G.A.; Khayyatzadeh, S.S. The association between dietary habits and metabolic syndrome: Findings from the Shahedieh-cohort study. BMC Nutr. 2022, 8, 117. [Google Scholar] [CrossRef]
- Lorzadeh, E.; Sangsefidi, Z.S.; Mirzaei, M.; Hosseinzadeh, M. Dietary Habits and their Association with Metabolic Syndrome in a sample of Iranian adults: A population-based study. Food Sci. Nutr. 2020, 8, 6217–6225. [Google Scholar] [CrossRef]
- Sarebanhassanabadi, M.; Mirhosseini, S.J.; Mirzaei, M.; Namayandeh, S.M.; Soltani, M.H.; Pakseresht, M.; Pedarzadeh, A.; Baramesipour, Z.; Faraji, R.; Salehi-Abargouei, A. Effect of dietary habits on the risk of metabolic syndrome: Yazd Healthy Heart Project. Public Health Nutr. 2018, 21, 1139–1146. [Google Scholar] [CrossRef] [PubMed]
- Shin, A.; Lim, S.Y.; Sung, J.; Shin, H.R.; Kim, J. Dietary intake, eating habits, and metabolic syndrome in Korean men. J. Am. Diet. Assoc. 2009, 109, 633–640. [Google Scholar] [CrossRef] [PubMed]
- McKeown, N.M.; Meigs, J.B.; Liu, S.; Wilson, P.W.; Jacques, P.F. Whole-grain intake is favorably associated with metabolic risk factors for type 2 diabetes and cardiovascular disease in the Framingham Offspring Study. Am. J. Clin. Nutr. 2002, 76, 390–398. [Google Scholar] [CrossRef]
- Tian, Y.; Su, L.-J.; Wang, J.; Duan, X.; Jiang, X. Fruit and vegetable consumption and risk of the metabolic syndrome: A meta-analysis. Public Health Nutr. 2017, 21, 756–765. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, D.Z. Associations of vegetable and fruit consumption with metabolic syndrome. A meta-analysis of observational studies. Public Health Nutr. 2018, 21, 1693–1703. [Google Scholar] [CrossRef]
- Lee, M.; Lim, M.; Kim, J. Fruit and vegetable consumption and the metabolic syndrome: A systematic review and dose-response meta-analysis. Br. J. Nutr. 2019, 122, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Jambi, H.; Enani, S.; Malibary, M.; Bahijri, S.; Eldakhakhny, B.; Al-Ahmadi, J.; Al Raddadi, R.; Ajabnoor, G.; Boraie, A.; Tuomilehto, J. The Association Between Dietary Habits and Other Lifestyle Indicators and Dysglycemia in Saudi Adults Free of Previous Diagnosis of Diabetes. Nutr. Metab. Insights 2020, 13, 1178638820965258. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Je, Y. Meat Consumption and Risk of Metabolic Syndrome: Results from the Korean Population and a Meta-Analysis of Observational Studies. Nutrients 2018, 10, 390. [Google Scholar] [CrossRef]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.P.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: A meta-analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef]
- Khosravi-Boroujeni, H.; Sarrafzadegan, N.; Mohammadifard, N.; Alikhasi, H.; Sajjadi, F.; Asgari, S.; Esmaillzadeh, A. Consumption of sugar-sweetened beverages in relation to the metabolic syndrome among Iranian adults. Obes. Facts 2012, 5, 527–537. [Google Scholar] [CrossRef]
- Ali, B.H.; Al Wabel, N.; Blunden, G. Phytochemical, pharmacological and toxicological aspects of Hibiscus sabdariffa L.: A review. Phytother. Res. PTR 2005, 19, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Ellis, L.R.; Zulfiqar, S.; Holmes, M.; Marshall, L.; Dye, L.; Boesch, C. A systematic review and meta-analysis of the effects of Hibiscus sabdariffa on blood pressure and cardiometabolic markers. Nutr. Rev. 2022, 80, 1723–1737. [Google Scholar] [CrossRef] [PubMed]
- Parichatikanond, W.; Pinthong, D.; Mangmool, S. Blockade of the renin-angiotensin system with delphinidin, cyanin, and quercetin. Planta Med. 2012, 78, 1626–1632. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.W.; Ikeda, K.; Yamori, Y. Upregulation of endothelial nitric oxide synthase by cyanidin-3-glucoside, a typical anthocyanin pigment. Hypertension 2004, 44, 217–222. [Google Scholar] [CrossRef]
- Lin, T.-L.; Lin, H.-H.; Chen, C.-C.; Lin, M.-C.; Chou, M.-C.; Wang, C.-J. Hibiscus sabdariffa extract reduces serum cholesterol in men and women. Nutr. Res. 2007, 27, 140–145. [Google Scholar] [CrossRef]
- Jeffery, T.D.; Richardson, M.L. A review of the effectiveness of hibiscus for treatment of metabolic syndrome. J. Ethnopharmacol. 2021, 270, 113762. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves Bortolini, D.; Windson Isidoro Haminiuk, C.; Cristina Pedro, A.; de Andrade Arruda Fernandes, I.; Maria Maciel, G. Processing, chemical signature and food industry applications of Camellia sinensis teas: An overview. Food Chem. X 2021, 12, 100160. [Google Scholar] [CrossRef] [PubMed]
- Sirotkin, A.V.; Kolesárová, A. The anti-obesity and health-promoting effects of tea and coffee. Physiol. Res. 2021, 70, 161–168. [Google Scholar] [CrossRef]
- Mahdavi-Roshan, M.; Salari, A.; Ghorbani, Z.; Ashouri, A. The effects of regular consumption of green or black tea beverage on blood pressure in those with elevated blood pressure or hypertension: A systematic review and meta-analysis. Complement. Ther. Med. 2020, 51, 102430. [Google Scholar] [CrossRef]
- Kondo, Y.; Goto, A.; Noma, H.; Iso, H.; Hayashi, K.; Noda, M. Effects of Coffee and Tea Consumption on Glucose Metabolism: A Systematic Review and Network Meta-Analysis. Nutrients 2018, 11, 48. [Google Scholar] [CrossRef]
- Grosso, G.; Stepaniak, U.; Micek, A.; Topor-Mądry, R.; Pikhart, H.; Szafraniec, K.; Pająk, A. Association of daily coffee and tea consumption and metabolic syndrome: Results from the Polish arm of the HAPIEE study. Eur. J. Nutr. 2015, 54, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.S.; Chang, Y.F.; Liu, P.Y.; Chen, C.Y.; Tsai, Y.S.; Wu, C.H. Smoking, habitual tea drinking and metabolic syndrome in elderly men living in rural community: The Tianliao old people (TOP) study 02. PLoS ONE 2012, 7, e38874. [Google Scholar] [CrossRef] [PubMed]
- Hayat, K.; Iqbal, H.; Malik, U.; Bilal, U.; Mushtaq, S. Tea and its consumption: Benefits and risks. Crit. Rev. Food Sci. Nutr. 2015, 55, 939–954. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.L.; Jeong, G.H.; Yang, J.W.; Lee, K.H.; Kronbichler, A.; van der Vliet, H.J.; Grosso, G.; Galvano, F.; Aune, D.; Kim, J.Y.; et al. Tea Consumption and Risk of Cancer: An Umbrella Review and Meta-Analysis of Observational Studies. Adv. Nutr. 2020, 11, 1437–1452. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Guo, X.; Yang, H.; Zheng, L.; Sun, Y. An update on the prevalence of metabolic syndrome and its associated factors in rural northeast China. BMC Public Health 2014, 14, 877. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.-X.; Wang, R.-R.; Liu, J.-Y.; Ma, Q.-H.; Pan, C.-W. Habitual tea consumption and 5-year incident metabolic syndrome among older adults: A community-based cohort study. BMC Geriatr. 2021, 21, 728. [Google Scholar] [CrossRef] [PubMed]
- Takami, H.; Nakamoto, M.; Uemura, H.; Katsuura, S.; Yamaguchi, M.; Hiyoshi, M.; Sawachika, F.; Juta, T.; Arisawa, K. Inverse correlation between coffee consumption and prevalence of metabolic syndrome: Baseline survey of the Japan Multi-Institutional Collaborative Cohort (J-MICC) Study in Tokushima, Japan. J. Epidemiol. 2013, 23, 12–20. [Google Scholar] [CrossRef]
- Micek, A.; Grosso, G.; Polak, M.; Kozakiewicz, K.; Tykarski, A.; Puch Walczak, A.; Drygas, W.; Kwaśniewska, M.; Pająk, A. Association between tea and coffee consumption and prevalence of metabolic syndrome in Poland—Results from the WOBASZ II study (2013–2014). Int. J. Food Sci. Nutr. 2018, 69, 358–368. [Google Scholar] [CrossRef]
- Bahijri, S.; Al-Fares, A.; Al-Khateeb, T.; Mufti, A. Hyperparathyroidism and Hypothyroidism in Individuals Consuming High Fluoride Intake in Jeddah-Saudi Arabia. In Proceedings of the 12th International Congress of Endocrinology, Lisbon, Portugal, 31 August–4 September 2004. [Google Scholar]
- Natella, F.; Scaccini, C. Role of coffee in modulation of diabetes risk. Nutr. Rev. 2012, 70, 207–217. [Google Scholar] [CrossRef]
- Tuomilehto, J.; Hu, G.; Bidel, S.; Lindström, J.; Jousilahti, P. Coffee consumption and risk of type 2 diabetes mellitus among middle-aged Finnish men and women. JAMA 2004, 291, 1213–1219. [Google Scholar] [CrossRef]
- Ding, M.; Bhupathiraju, S.N.; Satija, A.; van Dam, R.M.; Hu, F.B. Long-term coffee consumption and risk of cardiovascular disease: A systematic review and a dose-response meta-analysis of prospective cohort studies. Circulation 2014, 129, 643–659. [Google Scholar] [CrossRef]
- Marventano, S.; Salomone, F.; Godos, J.; Pluchinotta, F.; Del Rio, D.; Mistretta, A.; Grosso, G. Coffee and tea consumption in relation with non-alcoholic fatty liver and metabolic syndrome: A systematic review and meta-analysis of observational studies. Clin. Nutr. 2016, 35, 1269–1281. [Google Scholar] [CrossRef]
- Shang, F.; Li, X.; Jiang, X. Coffee consumption and risk of the metabolic syndrome: A meta-analysis. Diabetes Metab. 2016, 42, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Godos, J.; Galvano, F.; Giovannucci, E.L. Coffee, Caffeine, and Health Outcomes: An Umbrella Review. Annu. Rev. Nutr. 2017, 37, 131–156. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, M.C. Toward systems epidemiology of coffee and health. Curr. Opin. Lipidol. 2015, 26, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Ratnayake, W.M.; Hollywood, R.; O’Grady, E.; Stavric, B. Lipid content and composition of coffee brews prepared by different methods. Food Chem. Toxicol. 1993, 31, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Dórea, J.G.; da Costa, T.H. Is coffee a functional food? Br. J. Nutr. 2005, 93, 773–782. [Google Scholar] [CrossRef]
- Aro, A.; Tuomilehto, J.; Kostiainen, E.; Uusitalo, U.; Pietinen, P. Boiled coffee increases serum low density lipoprotein concentration. Metab. Clin. Exp. 1987, 36, 1027–1030. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-MetS n = 1127 | MetS n = 212 | p-Value | |
|---|---|---|---|
| Demographical characteristics | |||
| Age (years) mean ± SD | 30.5 ± 10.2 | 41.7 ± 12.4 | <0.001 a |
| Sex n (n%) | |||
| Men | 642 (84.5%) | 118 (15.5%) | 0.725 b |
| Women | 485 (83.8%) | 94 (16.2%) | |
| Parents consanguinity n (n%) | |||
| No | 838 (83.8%) | 162 (16.2%) | 0.527 b |
| Yes | 289 (85.3%) | 50 (14.7%) | |
| Marital status n (n%) | |||
| Single | 570 (93%) | 43 (7%) | <0.001 b |
| Married | 557 (76.7%) | 169 (23.3%) | |
| Have children n (n%) | |||
| No | 304 (89.4%) | 36 (10.6%) | 0.002 b |
| Yes | 823 (82.4%) | 176 (17.6%) | |
| Number of children mean ± SD | 4 ± 3 | 5 ± 2 | 0.228 a |
| Educational level n (n%) | |||
| Lower education or illiteracy | 428 (77%) | 128 (23%) | <0.001 b |
| Higher education | 699 (89.3%) | 84 (10.7%) | |
| Job type n (n%) | |||
| None | 529 (85.2%) | 92 (14.8%) | 0.584 b |
| Office job | 210 (82.4%) | 45 (17.6%) | |
| Job with some physical activity | 288 (84.7%) | 52 (15.3%) | |
| Job with considerable physical activity | 100 (81.3%) | 23 (18.7%) | |
| Income n (n%) | |||
| 3000 or less | 179 (74.6%) | 61 (25.4%) | <0.001 b |
| >3000–5000 | 188 (83.2%) | 38 (16.8%) | |
| >5000–10,000 | 280 (82.8%) | 58 (17.2%) | |
| >10,000–20,000 | 298 (88.4%) | 39 (11.6%) | |
| >20,000 | 182 (91.9%) | 16 (8.1%) | |
| Anthropometric measurements (mean ± SD) | |||
| Weight (kg) | |||
| Men | 78.7 ± 17 | 97 ± 19.4 | <0.001 a |
| Women | 65.8 ± 15.1 | 82.5 ± 16.3 | <0.001 a |
| BMI | 26.6 ± 5.7 | 32.8 ± 5.9 | <0.001 a |
| Fat (%) | |||
| Men | 25.9 ± 9 | 33.6 ± 7 | <0.001 a |
| Women | 38.6 ± 11.3 | 46 ± 9.6 | <0.001 a |
| NC (cm) | |||
| Men | 39 ± 4.1 | 42.5 ± 3.5 | <0.001 a |
| Women | 33.1 ± 3.9 | 36.4 ± 4.3 | <0.001 a |
| WC (cm) | |||
| Men | 94.3 ± 14.1 | 112.4 ± 14 | <0.001 a |
| Women | 85.7 ± 15.3 | 102.4 ± 12.6 | <0.001 a |
| HC (cm) | |||
| Men | 105.3 ± 12.9 | 117.4 ± 13.3 | <0.001 a |
| Women | 103.3 ± 12.9 | 115.8 ± 13.1 | <0.001 a |
| WC to HC ratio | |||
| Men | 0.89 ± 0.08 | 0.96 ± 0.06 | <0.001 a |
| Women | 0.83 ± 0.09 | 0.89 ± 0.08 | <0.001 a |
| WC to height ratio | 0.55 ± 0.09 | 0.65 ± 0.08 | <0.001 a |
| Clinical measurements mean ± SD | |||
| BP-Systolic | 115.7 ± 13.1 | 129.2 ± 19.5 | <0.001 a |
| BP-Diastolic | 71.8 ± 11.1 | 80.6 ± 12.3 | <0.001 a |
| Biochemical measurements mean ± SD | |||
| Serum TC (mmol/L) | 4.8 ± 0.9 | 5.1 ± 1 | <0.001 a |
| Serum HDL-C (mmol/L) | |||
| Men | 1.3 ± 0.2 | 1.1 ± 0.2 | <0.001 a |
| Women | 1.5 ± 0.3 | 1.3 ± 0.2 | <0.001 a |
| Serum LDL-C (mmol/L) | 3.2 ± 0.8 | 3.5 ± 0.9 | <0.001 a |
| Serum TG (mmol/L) | 1.1 ± 0.7 | 2.1 ± 1.1 | <0.001 a |
| HbA1c % | 5.2 ± 0.5 | 5.7 ± 1 | <0.001 a |
| Plasma glucose (0 h) | 4.3 ± 0.9 | 5.2 ± 1.7 | <0.001 a |
| Plasma glucose (1 h) | 6.4 ± 2.1 | 8.4 ± 3 | <0.001 a |
| Lifestyle factors | |||
| Physical activity of at least 30 min per day for at least 5 days per week n (n%) | |||
| No | 618 (82.4%) | 132 (17.6%) | 0.046 b |
| Yes | 509 (86.4%) | 80 (13.6%) | |
| Sitting h/day n (n%) | |||
| <4 | 207 (82.8%) | 43 (17.2%) | 0.868 b |
| 4–5 | 348 (84.9%) | 62 (15.1%) | |
| 6–8 | 350 (83.7%) | 68 (16.3%) | |
| 8+ | 222 (85.1%) | 39 (14.9%) | |
| Sleep duration n (n%) | |||
| <6 h | 432 (83.1%) | 88 (16.9%) | 0.657 b |
| 6–8 h | 590 (85%) | 104 (15%) | |
| >8 h | 105 (84%) | 20 (16%) | |
| Smoking habits n (n%) | |||
| Non-smoker | 858 (85%) | 152 (15%) | 0.243 b |
| Smoker | 230 (81%) | 54 (19%) | |
| Previous smoker | 39 (86.7%) | 6 (13.3%) | |
| Dietary items (portion/day) mean ± SD | |||
| Fruits | 0.66 ± 0.81 | 0.7 ± 0.78 | 0.524 a |
| Raw vegetables | 0.79 ± 0.83 | 0.82 ± 0.77 | 0.63 a |
| Cooked vegetables | 0.65 ± 0.77 | 0.73 ± 0.75 | 0.135 a |
| Whole grains | 1.17 ± 1.05 | 1.23 ± 1.12 | 0.467 a |
| Red meat | 0.57 ± 0.71 | 0.57 ± 0.71 | 0.979 a |
| Fresh juice | 0.47 ± 0.72 | 0.49 ± 0.65 | 0.769 a |
| Fruit drinks | 0.57 ± 0.83 | 0.51 ± 0.75 | 0.344 a |
| Carbonated drinks | 0.62 ± 0.91 | 0.51 ± 0.85 | 0.127 a |
| Red tea | 0.96 ± 1.1 | 1.04 ± 1.12 | 0.3 a |
| Green tea | 0.37 ± 0.72 | 0.49 ± 0.83 | 0.063 a |
| Arabic coffee | 0.63 ± 0.99 | 0.63 ± 0.97 | 0.99 a |
| Turkish coffee | 0.24 ± 0.62 | 0.23 ± 0.6 | 0.82 a |
| American coffee | 0.16 ± 0.55 | 0.17 ± 0.57 | 0.932 a |
| Cappuccino | 0.26 ± 0.59 | 0.19 ± 0.49 | 0.051 a |
| Energy drinks | 0.12 ± 0.43 | 0.04 ± 0.17 | 0.009 a |
| Hibiscus drink | 0.03 ± 0.18 | 0.08 ± 0.29 | 0.033 a |
| Cinnamon drink | 0.08 ± 0.37 | 0.15 ± 0.44 | 0.027 a |
| Age < 32 | Age 32+ | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Men n = 471 | Women n = 307 | p-Value b | Men n = 289 | Women n = 272 | p-Value b | |||||
| n (%) | Mean ± SD | n (%) | Mean ± SD | n (%) | Mean ± SD | n (%) | Mean ± SD | |||
| WC ^ | ||||||||||
| Normal WC | 369 (78.3) | 87.4 ± 9.4 | 225 (73.3) | 75.2 ± 7.4 | <0.001 | 156 (54.2) | 92.7 ± 7.5 | 77 (28.4) | 78.7 ± 7.8 | <0.001 |
| Elevated WC | 102 (21.7) | 115.8 ± 12.1 | 82 (26.7) | 100 ± 10.2 | <0.001 | 132 (45.8) | 115 ± 10 | 194 (71.6) | 103 ± 12 | <0.001 |
| p-value a | 0.105 | <0.001 | ||||||||
| BP ^ | ||||||||||
| Normal BP | 338 (71.8) | SBP: 115.1 ± 8.3 | 261 (85) | SBP: 107 ± 10 | <0.001 | 169 (58.5) | SBP: 116 ± 7 | 192 (70.6) | SBP: 109 ± 10 | <0.001 |
| DBP: 69.8 ± 9.2 | DBP: 66.4 ± 8.4 | <0.001 | DBP: 72.9 ± 8 | DBP:67.4 ± 0.8 | <0.001 | |||||
| Elevated BP | 133 (28.2) | SBP: 131.2 ± 11.3 | 46 (15) | SBP: 127 ± 15 | 0.061 | 120 (41.5) | SBP: 136 ± 17 | 80 (29.4) | SBP: 134 ± 19 | 0.461 |
| DBP: 82.8 ± 11.3 | DBP: 86.2 ± 9.6 | 0.054 | DBP: 85 ± 10.4 | DBP: 83.8 ± 11.8 | 0.462 | |||||
| p-value a | <0.001 | 0.003 | ||||||||
| HDL-C ^ | ||||||||||
| Normal HDL-C | 420 (89.4) | 1.3 ± 0.2 | 235 (76.5) | 1.6 ± 0.2 | <0.001 | 223 (77.2) | 1.3 ± 0.2 | 184 (67.6) | 1.6 ± 0.2 | <0.001 |
| Low HDL-C | 50 (10.6) | 0.9 ± 0.1 | 72 (23.5) | 1.1 ± 0.2 | <0.001 | 66 (22.8) | 1 ± 0.2 | 88 (32.4) | 1.2 ± 0.2 | <0.001 |
| p-value a | <0.001 | 0.012 | ||||||||
| TG ^ | ||||||||||
| Normal TG | 389 (82.8) | 0.94 ± 0.32 | 288 (93.8) | 0.79 ± 0.27 | <0.001 | 162 (56.1) | 1.1 ± 0.33 | 203 (74.6) | 1 ± 0.33 | 0.007 |
| High TG | 81 (17.2) | 2.66 ± 1.24 | 19 (6.2) | 1.98 ± 0.73 | 0.024 | 127 (43.9) | 2.68 ± 1.04 | 69 (25.4) | 2.03 ± 0.88 | <0.001 |
| p-value a | <0.001 | <0.001 | ||||||||
| FPG ^ | ||||||||||
| Normal FPG | 427 (90.7) | 4.2 ± 0.5 | 282 (91.9) | 4.1 ± 0.5 | 0.82 | 198 (68.5) | 4.4 ± 0.6 | 202 (74.3) | 4.3 ± 0.6 | 0.097 |
| High FPG | 44 (9.3) | 5.1 ± 1.3 | 25 (8.1) | 5 ± 0.9 | 0.598 | 91 (31.5) | 6 ± 2.7 | 70 (25.7) | 5.4 ± 2.1 | 0.16 |
| p-value a | 0.565 | 0.132 | ||||||||
| MetS ^ | ||||||||||
| No MetS | 436 (92.6) | 293 (95.4) | 206 (71.3) | 192 (70.6) | ||||||
| MetS | 35 (7.4) | 14 (4.6) | 83 (28.7) | 80 (29.4) | ||||||
| p-value a | 0.107 | 0.857 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eldakhakhny, B.; Enani, S.; Jambi, H.; Ajabnoor, G.; Al-Ahmadi, J.; Al-Raddadi, R.; Alsheikh, L.; Abdulaal, W.H.; Gad, H.; Borai, A.; et al. Prevalence and Factors Associated with Metabolic Syndrome among Non-Diabetic Saudi Adults: A Cross-Sectional Study. Biomedicines 2023, 11, 3242. https://doi.org/10.3390/biomedicines11123242
Eldakhakhny B, Enani S, Jambi H, Ajabnoor G, Al-Ahmadi J, Al-Raddadi R, Alsheikh L, Abdulaal WH, Gad H, Borai A, et al. Prevalence and Factors Associated with Metabolic Syndrome among Non-Diabetic Saudi Adults: A Cross-Sectional Study. Biomedicines. 2023; 11(12):3242. https://doi.org/10.3390/biomedicines11123242
Chicago/Turabian StyleEldakhakhny, Basmah, Sumia Enani, Hanan Jambi, Ghada Ajabnoor, Jawaher Al-Ahmadi, Rajaa Al-Raddadi, Lubna Alsheikh, Wesam H. Abdulaal, Hoda Gad, Anwar Borai, and et al. 2023. "Prevalence and Factors Associated with Metabolic Syndrome among Non-Diabetic Saudi Adults: A Cross-Sectional Study" Biomedicines 11, no. 12: 3242. https://doi.org/10.3390/biomedicines11123242
APA StyleEldakhakhny, B., Enani, S., Jambi, H., Ajabnoor, G., Al-Ahmadi, J., Al-Raddadi, R., Alsheikh, L., Abdulaal, W. H., Gad, H., Borai, A., Bahijri, S., & Tuomilehto, J. (2023). Prevalence and Factors Associated with Metabolic Syndrome among Non-Diabetic Saudi Adults: A Cross-Sectional Study. Biomedicines, 11(12), 3242. https://doi.org/10.3390/biomedicines11123242