
Comparative Analysis of Clinical and CT Findings in Patients with SARS-CoV-2 Original Strain, Delta and Omicron Variants
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
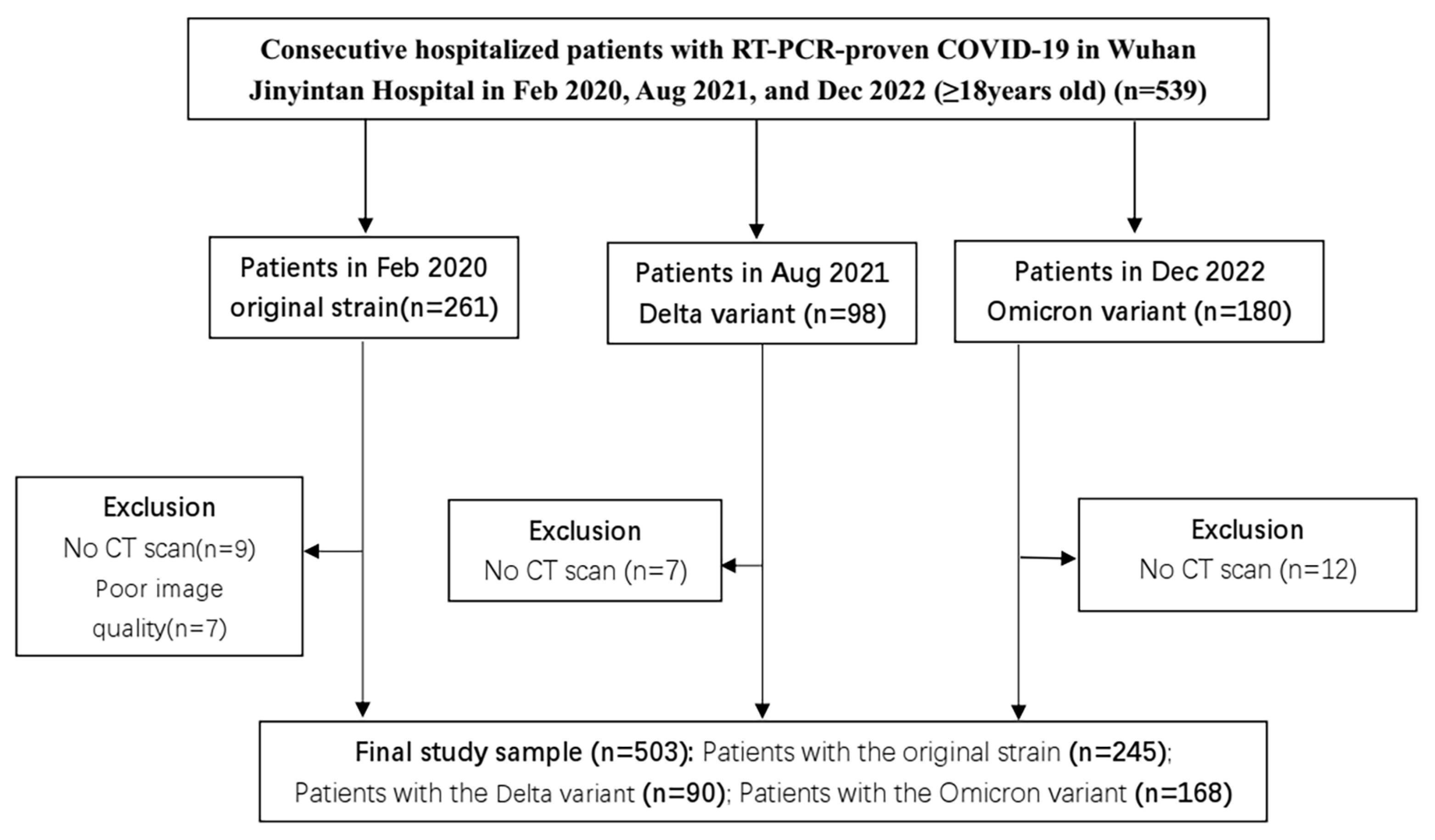
2.1. Patients and Clinical Characteristics
2.2. CT Imaging Acquisition
2.3. Imaging Interpretation
2.4. Quantitative CT Analysis by Artificial Intelligence
2.5. Statistical Analysis
3. Results
3.1. Demographics and Clinical Characteristics on Admission
3.2. Laboratory Findings
3.3. Chest CT Score and Features
3.4. Patient Clinical Characteristics by Vaccination
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Fontanet, A.; Autran, B.; Lina, B.; Kieny, M.P.; Karim, S.S.A.; Sridhar, D. SARS-CoV-2 variants and ending the COVID-19 pandemic. Lancet 2021, 397, 952–954. [Google Scholar] [CrossRef] [PubMed]
- Harvey, W.T.; Carabelli, A.M.; Jackson, B.; Gupta, R.K.; Thomson, E.C.; Harrison, E.M.; Ludden, C.; Reeve, R.; Rambaut, A.; Peacock, S.J.; et al. SARS-CoV-2 variants, spike mutations and immune escape. Nat. Rev. Microbiol. 2021, 19, 409–424. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Tsakok, M.T.; Watson, R.A.; Saujani, S.J.; Kong, M.; Xie, C.; Peschl, H.; Wing, L.; MacLeod, F.K.; Shine, B.; Talbot, N.P.; et al. Chest CT and Hospital Outcomes in Patients with Omicron Compared with Delta Variant SARS-CoV-2 Infection. Radiology 2023, 306, 261–269. [Google Scholar] [CrossRef]
- Yoon, S.H.; Lee, J.H.; Kim, B.N. Chest CT Findings in Hospitalized Patients with SARS-CoV-2: Delta versus Omicron Variants. Radiology 2022, 305, E66. [Google Scholar] [CrossRef]
- Jin, C.; Chen, W.; Cao, Y.; Xu, Z.; Tan, Z.; Zhang, X.; Deng, L.; Zheng, C.; Zhou, J.; Shi, H.; et al. Development and evaluation of an artificial intelligence system for COVID-19 diagnosis. Nat. Commun. 2020, 11, 5088. [Google Scholar] [CrossRef]
- Kang, H.; Xia, L.; Yan, F.; Wan, Z.; Shi, F.; Yuan, H.; Jiang, H.; Wu, D.; Sui, H.; Zhang, C.; et al. Diagnosis of Coronavirus Disease 2019 (COVID-19) With Structured Latent Multi-View Representation Learning. IEEE Trans. Med. Imaging 2020, 39, 2606–2614. [Google Scholar] [CrossRef]
- Bai, H.X.; Hsieh, B.; Xiong, Z.; Halsey, K.; Choi, J.W.; Tran, T.M.L.; Pan, I.; Shi, L.B.; Wang, D.C.; Mei, J.; et al. Performance of Radiologists in Differentiating COVID-19 from Non-COVID-19 Viral Pneumonia at Chest CT. Radiology 2020, 296, E46–E54. [Google Scholar] [CrossRef] [Green Version]
- Yek, C.; Warner, S.; Wiltz, J.L.; Sun, J.; Adjei, S.; Mancera, A.; Silk, B.J.; Gundlapalli, A.V.; Harris, A.M.; Boehmer, T.K.; et al. Risk Factors for Severe COVID-19 Outcomes Among Persons Aged ≥18 Years Who Completed a Primary COVID-19 Vaccination Series–465 Health Care Facilities, United States, December 2020-October 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Deng, A.; Li, K.; Hu, Y.; Li, Z.; Shi, Y.; Xiong, Q.; Liu, Z.; Guo, Q.; Zou, L.; et al. Viral infection and transmission in a large, well-traced outbreak caused by the SARS-CoV-2 Delta variant. Nat. Commun. 2022, 13, 460. [Google Scholar] [CrossRef] [PubMed]
- Ai, J.; Zhang, H.; Zhang, Y.; Lin, K.; Zhang, Y.; Wu, J.; Wan, Y.; Huang, Y.; Song, J.; Fu, Z.; et al. Omicron variant showed lower neutralizing sensitivity than other SARS-CoV-2 variants to immune sera elicited by vaccines after boost. Emerg. Microbes Infect. 2022, 11, 337–343. [Google Scholar] [CrossRef]
- CDC. Pneumonia Diagnosis and Treatment Plan for New Coronavirus Infection, 9th ed.; CDC: Atlanta, GA, USA, 2022. [Google Scholar]
- Force, A.D.T.; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Simpson, S.; Kay, F.U.; Abbara, S.; Bhalla, S.; Chung, J.H.; Chung, M.; Henry, T.S.; Kanne, J.P.; Kligerman, S.; Ko, J.P.; et al. Radiological Society of North America Expert Consensus Document on Reporting Chest CT Findings Related to COVID-19: Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA. Radiol. Cardiothorac. Imaging 2020, 2, e200152. [Google Scholar] [CrossRef] [Green Version]
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; Müller, N.L.; Remy, J. Fleischner Society: Glossary of terms for thoracic imaging. Radiology 2008, 246, 697–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.-C.; Yu, C.-J.; Chang, S.-C.; Galvin, J.R.; Liu, H.-M.; Hsiao, C.-H.; Kuo, P.-H.; Chen, K.-Y.; Franks, T.J.; Huang, K.-M.; et al. Pulmonary Sequelae in Convalescent Patients after Severe Acute Respiratory Syndrome: Evaluation with Thin-Section CT. Radiology 2005, 236, 1067–1075. [Google Scholar] [CrossRef]
- Wang, M.; Xia, C.; Huang, L.; Xu, S.; Qin, C.; Liu, J.; Cao, Y.; Yu, P.; Zhu, T.; Zhu, H.; et al. Deep learning-based triage and analysis of lesion burden for COVID-19: A retrospective study with external validation. Lancet Digit. Health 2020, 2, e506–e515. [Google Scholar] [CrossRef]
- Huang, L.; Han, R.; Ai, T.; Yu, P.; Kang, H.; Tao, Q.; Xia, L. Serial Quantitative Chest CT Assessment of COVID-19: A Deep Learning Approach. Radiol. Cardiothorac. Imaging 2020, 2, e200075. [Google Scholar] [CrossRef] [Green Version]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D.G.; Everatt, J.; Bhiman, J.N.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Ulloa, A.C.; Buchan, S.A.; Daneman, N.; Brown, K.A. Estimates of SARS-CoV-2 Omicron Variant Severity in Ontario, Canada. JAMA 2022, 327, 1286–1288. [Google Scholar] [CrossRef]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- Twohig, K.A.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, M.A.; Aliabadi, S.; Seaman, S.R.; Harris, R.J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern: A cohort study. Lancet Infect. Dis. 2022, 22, 35–42. [Google Scholar] [CrossRef]
- Fisman, D.N.; Tuite, A.R. Evaluation of the relative virulence of novel SARS-CoV-2 variants: A retrospective cohort study in Ontario, Canada. CMAJ Can. Med. Assoc. J. 2021, 193, E1619–E1625. [Google Scholar] [CrossRef]
- Monteil, V.; Kwon, H.; Prado, P.; Hagelkrüys, A.; Wimmer, R.A.; Stahl, M.; Leopoldi, A.; Garreta, E.; Hurtado Del Pozo, C.; Prosper, F.; et al. Inhibition of SARS-CoV-2 Infections in Engineered Human Tissues Using Clinical-Grade Soluble Human ACE2. Cell 2020, 181, 905–913.e907. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Han, X.; Gu, J.; Li, Y.; Liu, J.; Alwalid, O.; Cui, Y.; Zhang, X.; Zheng, C.; Fan, Y.; et al. Prognostic value of baseline clinical and HRCT findings in 101 patients with severe COVID-19 in Wuhan, China. Sci. Rep. 2020, 10, 17543. [Google Scholar] [CrossRef]
- Del Rio, C.; Omer, S.B.; Malani, P.N. Winter of Omicron-The Evolving COVID-19 Pandemic. JAMA 2022, 327, 319–320. [Google Scholar] [CrossRef] [PubMed]
- Christie, B. Covid-19: Early studies give hope omicron is milder than other variants. BMJ 2021, 375, n3144. [Google Scholar] [CrossRef]
- Hammer, M.M. Real-World Diagnostic Performance of RSNA Consensus Reporting Guidelines for Findings Related to COVID-19 on Chest CT. Am. J. Roentgenol. 2021, 218, 75–76. [Google Scholar] [CrossRef] [PubMed]
- Hammer, M.M.; Zhao, A.H.; Hunsaker, A.R.; Mendicuti, A.D.; Sodickson, A.D.; Boland, G.W.; Khorasani, R. Radiologist Reporting and Operational Management for Patients with Suspected COVID-19. J. Am. Coll. Radiol. JACR 2020, 17, 1056–1060. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- Zheng, H.; Cao, Y.; Chen, X.; Wang, F.; Hu, Y.; Song, W.; Chai, Y.; Gu, Q.; Shi, Y.; Feng, Y.; et al. Disease profile and plasma neutralizing activity of post-vaccination Omicron BA.1 infection in Tianjin, China: A retrospective study. Cell Res. 2022, 32, 781–784. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Fusco, R.; Villanacci, A.; Magliocchetti, S.; Urraro, F.; Tetaj, N.; Marchioni, L.; Albarello, F.; Campioni, P.; Cristofaro, M.; et al. Imaging Severity COVID-19 Assessment in Vaccinated and Unvaccinated Patients: Comparison of the Different Variants in a High Volume Italian Reference Center. J. Pers. Med. 2022, 12, 955. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Characteristic | Original Strain (n = 245) | Delta Variant (n = 90) | Omicron Variant (n = 168) | p Value |
|---|---|---|---|---|
| Sex | 134 (54.7%) a | 58 (64%) | 102 (61%) | 0.211 |
| Age | 58.1 ± 13.2 a,b | 39.1 ± 16.4 c | 45 ± 20 | <0.001 |
| Comorbidities | 146 (59.6%) a,b | 18 (20%) | 49 (29%) | <0.001 |
| Diabetes | 41 (16.8%) a,b | 1 (1.1%) | 11 (6.6%) | <0.001 |
| Hypertension | 92 (37.7%) a,b | 7 (7.8%) | 33 (20%) | <0.001 |
| Cardiovascular and cerebrovascular disease | 18 (7.4%) a,b | 0 | 17 (10%) | 0.009 |
| Chronic pulmonary disease | 19 (7.8%) b | 2 (2.2%) | 7 (4.2%) | 0.094 |
| Hepatopathy | 9 (3.7%) | 3 (3.3%) | 6 (3.6%) | 0.987 |
| Nephropathy | 10 (4.1%) | 3 (3.3%) | 4 (2.4%) | 0.657 |
| Received vaccination | -- | 68 (75.6%) | 147 (88%) | 0.014 |
| Number of vaccination | <0.001 | |||
| One dose | -- | 14 (15.6%) | 6 (3.6%) | |
| Two doses | -- | 54 (60%) | 33 (20%) | |
| Three doses | -- | 0 | 107 (64%) | |
| Clinical severity | <0.001 | |||
| Mild type | 10 (4.1%) a,b | 17 (19%) | 95 (57%) | |
| moderate type | 170 (69.4%) | 64 (71%) | 65 (39%) | |
| Severe or critical type | 65 (26.5%) a,b | 9 (10%) | 8 (4.8%) | |
| Clinical symptoms | ||||
| Fever | 214 (88%)a,b | 58 (64%)c | 123 (75%) | <0.001 |
| Maximum temperature | 38 ± 1.6 | 37.4 ± 1.0c | 38.2 ± 1.2 | 0.069 |
| Cough | 185 (75.5%) a,b | 41 (45.6%) | 42 (25%) | <0.001 |
| Sputum | 79 (32.2%) a,b | 11 (12.2%) | 34 (21%) | <0.001 |
| Rhinorrhea | 0 a,b | 4 (4.4%) | 8 (4.9%) | 0.006 |
| Asthma | 132 (53.9%) a,b | 5 (5.6%) | 11 (6.5%) | <0.001 |
| Throat pain | 16 (6.6%) a,b | 21 (23.3%) | 51 (31%) | <0.001 |
| Diarrhoea | 13 (5.3%) | 10 (11.1%) c | 3 (1.8%) | 0.006 |
| Hyposmia | 1 (0.4%) a | 5 (5.6%) | 6 (3.6%) | 0.008 |
| Ophthalmia | 0 | 3 (3.3%) | 0 | 0.003 |
| Weakness | 73 (29.8%) a,b | 6 (6.7%) | 52 (31%) | <0.001 |
| Heart rate | 94 ± 14 b | 87 ± 14 | 86 ± 12 | <0.001 |
| Respiratory rate | 23 ± 5 a,b | 20 ± 1 | 21 ± 6 | <0.001 |
| Oxygen saturation | 91 ± 10 a,b | 97.5 ± 1.3 | 98 ± 1.9 | <0.001 |
| SBP (mmHg) | 132 ± 20 a,b | 126 ± 14 | 124 ± 12 | <0.001 |
| DBP (mmHg) | 82 ± 11 b | 82 ± 11 c | 83 ± 9 | 0.009 |
| Secondary infection | 30 (12.2%) b | 5 (5.6%) | 1 (0.6%) | |
| ICU | 42 (17.1%) a,b | 2 (2.2%) | 6 (3.6%) | <0.001 |
| ARDS | 65 (26.5%) a,b | 1 (1.1%) | 0 | <0.001 |
| Hospital stay duration (days) | 15 (11–23) a | 26.5 (19.6–34) c | 14 (10–17) | <0.001 |
| Treatment | ||||
| Oxygen therapy | 116 (47.3%) a,b | 10 (11.1%) c | 9 (5.4%) | <0.001 |
| Endotracheal intubation | 16 (6.6%) a,b | 0 | 0 | 0.001 |
| Antiviral therapy | 232 (94.7%) b | 86 (95.6%) c | 80 (48%) | <0.001 |
| Antibiotic therapy | 218 (89.0%) a,b | 7 (7.8%) | 11 (6.5%) | <0.001 |
| Hormone | 163 (66.5%) a,b | 14 (15.7%) c | 3 (1.8%) | <0.001 |
| Intravenous immunoglobulin | 51 (20.9%) a,b | 2 (2.2%) | 3 (1.8%) | <0.001 |
| Mortality | 35 (14.3%) a,b | 0 | 0 | <0.001 |
| CT Characteristics | Original Strain (n = 245) | Delta Variant (n = 90) | Omicron Variant (n = 168) | p Value |
|---|---|---|---|---|
| CT scan thickness | <0.001 | |||
| 1.25 mm | 140 (57.1%) | 90 (100%) | 168 (100%) | |
| 5 mm | 105 (42.8%) a | 0 | 0 | |
| Abnormal CT | 235 (95.9%) a,b | 73 (81%) c | 73 (44%) | <0.001 |
| COVID-19 pneumonia imaging classification | <0.001 | |||
| Typical appearance | 228 (97%) | 55 (75%) | 48 (66%) | |
| Indeterminate appearance | 3 (1.3%) | 8 (11%) | 13 (18%) | |
| Atypical appearance | 4 (1.7%) | 10 (14%) | 12 (16%) | |
| Lesions involvement | <0.001 | |||
| Unilateral | 9 (3.8%) a | 17 (23%) | 9 (12%) | |
| Bilateral | 226 (96.2%) a | 56 (77%) | 64 (88%) | |
| CT score of total lesions | 14 (9.0–20.0) a,b | 6.0 (3.0, 8.5) | 5.0 (3.0, 10) | <0.001 |
| superior lobe of left lung | 3.0 (2.0–4.0) a,b | 1.0 (0, 1.5) c | 1 (0, 1.0) | <0.001 |
| inferior lobe of left lung | 3.0 (2.0–4.0) a,b | 1.0 (0, 2.0) | 1.0 (1.0, 2.0) | <0.001 |
| superior lobe of right lung | 3.0 (2.0–4.0) a,b | 0 (0, 1.0) | 1.0 (1.0, 2.0) | <0.001 |
| middle lobe of right lung | 2.0 (1.0–3.5) a,b | 0 (0, 1.0) | 0 (0, 1.0) | <0.001 |
| inferior lobe of right lung | 3.0 (2.0–4.0) a,b | 2 (1.0, 2.5) | 2 (1.0, 2.5) | <0.001 |
| CT score of GGO | 11.0 (6.0–16.5) a,b | 4.0 (2.0, 7.0) c | 4 (1.5, 7.0) | |
| superior lobe of left lung | 2.0 (1.0–3.0) a,b | 1.0 (0, 1.0) | 1.0 (0, 2.0) | <0.001 |
| inferior lobe of left lung | 2.0 (1.0–4.0) a,b | 1.0 (0, 2.0) | 1.0 (0, 2.0) | <0.001 |
| superior lobe of right lung | 2.0 (1.0–4.0) a,b | 0 (0, 1.0) | 1 (0, 1.5) | <0.001 |
| middle lobe of right lung | 2.0 (1.0–3.0) a,b | 0 (0, 1.0) | 0 (0, 1.0) | <0.001 |
| inferior lobe of right lung | 3.0 (2.0–4.0) a,b | 1.0 (1.0, 2.0) c | 1.0 (0, 2.0) | <0.001 |
| CT score of consolidation | 3.0 (0–8.5) a | 1.0 (0, 4.0) c | 2.0 (0, 5) | 0.001 |
| superior lobe of left lung | 0 (0–2.0) a,b | 0 (0, 1.0) | 0 (0, 0.25) | 0.004 |
| inferior lobe of left lung | 1.0 (0–2.0) a,b | 0 (0, 1.0) | 0 (0, 1.3) | <0.001 |
| superior lobe of right lung | 0 (0–2.0) a, | 0 (0, 0) c | 0 (0, 1.0) | 0.003 |
| middle lobe of right lung | 0 (0–1.0) a,b | 0 (0, 0) | 0 (0, 0.25) | <0.001 |
| inferior lobe of right lung | 1.0 (0–2.0) a | 0 (0, 1.0) | 1.0 (0, 2.0) | 0.008 |
| CT score of linear opacities | 3.0 (0–7.0) a,b | 0 (0, 2.0) | 0 (0, 2.0) | <0.001 |
| superior lobe of left lung | 0 (0–1.0) a,b | 0 (0, 0) | 0 (0, 0) | <0.001 |
| inferior lobe of left lung | 1.0 (0–2.0) a,b | 0 (0, 1.0) | 0 (0, 1.0) | <0.001 |
| superior lobe of right lung | 0 (0–1.0) a,b | 0 (0, 0) | 0 (0, 0) | <0.001 |
| middle lobe of right lung | 0 (0–1.0) a,b | 0 (0, 0) | 0 (0, 0) | <0.001 |
| inferior lobe of right lung | 1.0 (0–2.0) a,b | 0 (0, 1.0) | 0 (0, 1.0) | <0.001 |
| Lung involvement | ||||
| superior lobe of bilateral lung | 25 (10.2%) a,b | 16 (22%) | 17 (23%) | 0.007 |
| inferior lobe of bilateral lung | 220 (89.8%) | 57 (78%) | 56 (77%) | |
| Peripheral or subpleural | 236 (96.3%) a,b | 62 (85%) | 57 (78%) | |
| Degree of lesions involvement | <0.001 | |||
| focal | 9 (3.8%) a,b | 11 (15%) | 19 (26%) | |
| Multiple | 53 (22.6%) | 34 (47%) | 30 (41%) | |
| Diffused | 173 (73.6%) | 28 (38%) | 24 (33%) | |
| Predominant CT pattern | 0.093 | |||
| GGO | 176 (74.9%) a,b | 45 (62%) | 48 (66%) | |
| Consolidation | 44 (18.7%) | 18 (25%) | 20 (27%) | |
| Linear and reticulation | 15 (6.4%) | 10 (14%) | 5 (6.8%) | |
| Crazy paving | 79 (33.6%) a,b | 14 (19%) | 10 (14%) | |
| Thickening of the bronchial wall | 51 (21.8%) | 7 (9.6%) | 20 (28%) | 0.009 |
| Nodule or mass | 8 (3.4%) a,b | 6 (8.2%)c | 17 (23%) | <0.001 |
| Tree-in-bud sign | 0 a,b | 4 (5.5%) | 6 (8.2%) | <0.001 |
| Halo sign | 4 (1.6%) a,b | 5 (6.8%) | 10 (14%) | <0.001 |
| pleural effusion | 37 (15.7%) a | 8 (11%) | 4 (5.5%) | 0.063 |
| Virus Type | Delta Variant (n = 90) | p Value | Omicron Variant (n = 168) | p Value | ||
|---|---|---|---|---|---|---|
| Vaccination Status | Unvaccinated (n = 22) | Vaccinated (n = 68) | Less Than Three Doses (n = 61) | Three Doses (n = 107) | ||
| Age | 39.5 ± 22 | 38.8 ± 14.1 | 0.856 | 49 ± 24 | 42 ± 17 | 0.037 |
| Sex | 0.131 | 0.185 | ||||
| Male | 12 (54.5%) | 46 (68%) | 33 (54%) | 69 (65%) | ||
| Female | 10 (45.5%) | 22 (32%) | 28 (46%) | 38 (36%) | ||
| Comorbidities | 7 (31.8%) | 11 (16.2%) | 0.111 | 24 (39%) | 25 (23%) | 0.028 |
| Clinical type | 0.04 | 0.015 | ||||
| Mild type | 3 (13.6%) | 19 (27.9%) | 26 (43%) | 69 (65%) | ||
| moderate type | 12 (54.5%) | 37 (54.4%) | 30 (49%) | 35 (33%) | ||
| Severe or critical type | 5 (22.7%) | 1 (1.5%) | 5 (8.2%) | 3 (2.8%) | ||
| Fever | 15 (68%) | 43 (63%) | 0.674 | 41 (67%) | 63 (59%) | 0.176 |
| Maximum temperature | 37.7 ± 1.1 | 37.2 ± 0.9 | 0.037 | 38 ± 1.3 | 38 ± 1.1 | 0.750 |
| Hospital stay duration (days) | 31 (24, 41) | 25.5 (19, 32.8) | 0.02 | 14 (10, 16) | 13 (7, 18) | 0.701 |
| Abnormal CT | 19 (86%) | 54 (79%) | 0.469 | 35 (57%) | 38 (36%) | 0.009 |
| Lung involvement | ||||||
| CT score of total lesions | 5 (2, 10) | 5.5 (3, 9.3) | 0.891 | 5.5 (3, 9.3) | 4 (3, 11) | 0.673 |
| CT score of GGOs | 4.0 (1, 5.0) | 4 (2, 7.0) | 0.861 | 4 (2, 7) | 3 (1, 8) | 0.920 |
| CT score of consolidation | 1 (0, 3) | 2 (0, 5.3) | 0.229 | 2 (0, 5.3) | 0 (0, 2) | 0.825 |
| CT score of linear opacities | 0 (0, 2.0) | 0 (0, 2) | 0.723 | 0 (0, 2) | 2 (0, 5) | 0.274 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, X.; Chen, J.; Chen, L.; Jia, X.; Fan, Y.; Zheng, Y.; Alwalid, O.; Liu, J.; Li, Y.; Li, N.; et al. Comparative Analysis of Clinical and CT Findings in Patients with SARS-CoV-2 Original Strain, Delta and Omicron Variants. Biomedicines 2023, 11, 901. https://doi.org/10.3390/biomedicines11030901
Han X, Chen J, Chen L, Jia X, Fan Y, Zheng Y, Alwalid O, Liu J, Li Y, Li N, et al. Comparative Analysis of Clinical and CT Findings in Patients with SARS-CoV-2 Original Strain, Delta and Omicron Variants. Biomedicines. 2023; 11(3):901. https://doi.org/10.3390/biomedicines11030901
Chicago/Turabian StyleHan, Xiaoyu, Jingze Chen, Lu Chen, Xi Jia, Yanqing Fan, Yuting Zheng, Osamah Alwalid, Jie Liu, Yumin Li, Na Li, and et al. 2023. "Comparative Analysis of Clinical and CT Findings in Patients with SARS-CoV-2 Original Strain, Delta and Omicron Variants" Biomedicines 11, no. 3: 901. https://doi.org/10.3390/biomedicines11030901
APA StyleHan, X., Chen, J., Chen, L., Jia, X., Fan, Y., Zheng, Y., Alwalid, O., Liu, J., Li, Y., Li, N., Gu, J., Wang, J., & Shi, H. (2023). Comparative Analysis of Clinical and CT Findings in Patients with SARS-CoV-2 Original Strain, Delta and Omicron Variants. Biomedicines, 11(3), 901. https://doi.org/10.3390/biomedicines11030901