
Antifungal Drug Resistance: An Emergent Health Threat

 ,
,  ,
,  ,
,  , ,
, , 
Abstract
:1. Fungal Infections
2. Systemic Mycosis and Pharmacological Therapy
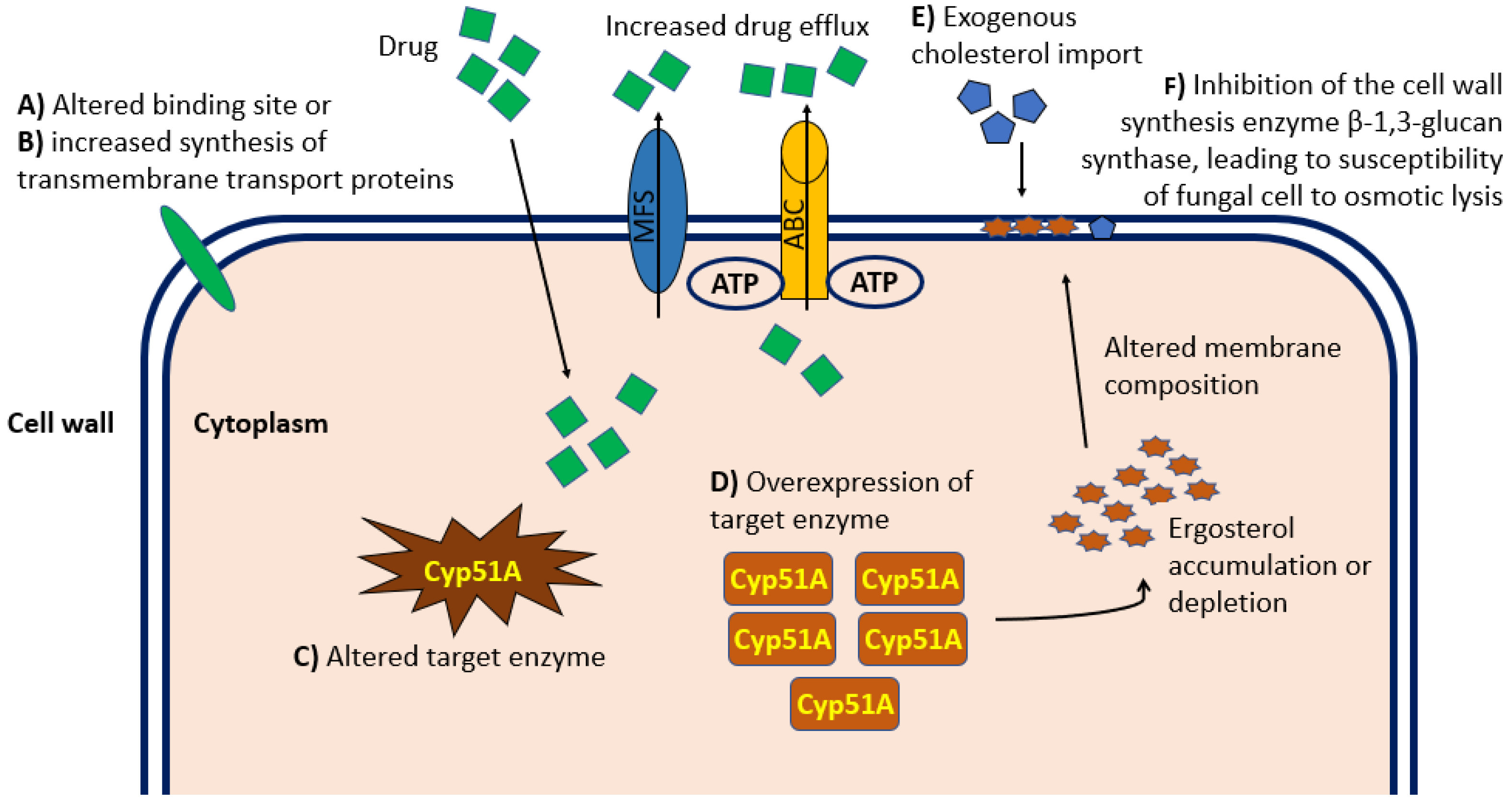
3. Antifungal Resistance Mechanisms
4. New Antifungal Agents
5. Discussion
5.1. The Non-Negligible Burden of Invasive Fungal Infections
5.2. Drug-Resistant Fungal Infections
5.3. Overall Efforts in the Fight of Severe Fungal Infections
5.4. Limits of Our Study
6. Future Perspectives
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Brown, G.D.; Denning, D.W.; Gow, N.A.; Levitz, S.M.; Netea, M.G.; White, T.C. Hidden killers: Human fungal infections. Sci. Transl. Med. 2012, 4, 165rv13. [Google Scholar] [CrossRef] [Green Version]
- Kainz, K.; Bauer, M.A.; Carmona-Gutierrez, C. Fungal infections in humans: The silent crisis. Microb. Cell 2020, 7, 143–145. [Google Scholar] [CrossRef]
- Rogawansamy, S.; Gaskin, S.; Taylor, M.; Pisaniello, D. An Evaluation of Antifungal Agents for the Treatment of Fungal Contamination in Indoor Air Environments. Int. J. Environ. Res. Public Health 2015, 12, 6319–6332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suhail Ahmad, S.; Asadzadeh, M. Strategies to Prevent Transmission of Candida auris in Healthcare Settings. Curr. Fungal Infect. Rep. 2023, 17, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Chandley, P.; Subba, P.; Rohatgi, S. COVID-19-Associated Mucormycosis: A Matter of Concern Amid the SARS-CoV-2 Pandemic. Vaccines 2022, 10, 1266. [Google Scholar] [CrossRef] [PubMed]
- Corrêa-Junior, D.; Andrade, I.B.; Alves, V.; de Araújo, S.G.R.; Frasest, S. Clinical Challenges of Emerging and Re-Emerging Yeast Infections in the Context of the COVID-19 Pandemic. Microorganisms 2022, 10, 2223. [Google Scholar] [CrossRef] [PubMed]
- Kapitan, M.; Niemiec, M.J.; Steimle, A.; Frick, J.S.; Jacobsen, I.D. Fungi as Part of the Microbiota and Interactions with Intestinal Bacteria. Curr. Top Microbiol. Immunol. 2019, 422, 265–301. [Google Scholar]
- Vitiello, A.; Ferrara, F.; Zovi, A. The direct correlation between microbiota and SARS-CoV-2 infectious disease. Inflammopharmacology 2023, 1, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Enoch, D.A.; Yang, H.; Aliyu, S.H.; Micallef, C. The Changing Epidemiology of Invasive Fungal Infections. Methods Mol. Biol. 2017, 1508, 17–65. [Google Scholar] [PubMed]
- Liao, Y.; Lu, X.; Yang, S.; Luo, Y.; Chen, Q.; Yang, R. Epidemiology and outcome of trichosporon fungemia: A review of 185 reported cases from 1975 to 2014. Open Forum Infect. Dis. 2015, 2, ofv141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin-Loeches, I.; Antonelli, M.; Cuenca-Estrella, M.; Dimopoulos, G.; Einav, S.; De Waele, J.J.; Garnacho-Montero, J.; Kanj, S.S.; Machado, F.R.; Montravers, P.; et al. ESICM/ESCMID task force on practical management of invasive candidiasis in critically ill patients. Intensive Care Med. 2019, 45, 789–805. [Google Scholar] [CrossRef] [PubMed]
- Tortorano, A.M.; Richardson, M.; Roilides, E.; van Diepeningen, A.; Caira, M.; Munoz, P.; Johnson, E.; Meletiadis, J.; Pana, Z.D.; Lackner, M.; et al. ESCMID and ECMM joint guidelines on diagnosis and management of hyalohyphomycosis: Fusarium spp, Scedosporium spp. and others. Clin. Microbiol. Infect. 2014, 20 (Suppl. S3), 27–46. [Google Scholar] [CrossRef] [Green Version]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24 (Suppl. S1), e1–e38. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Fungal Priority Pathogens List to guide Research, Development and Public Health Action; World Health Organization: Geneva, Switzerland, 2022; Licence: CC BY-NC-SA 3.0 IGO. [updated 2022, October 25]. [Google Scholar]
- Robbins, N.; Wright, G.D.; Cowen, L.E. Antifungal Drugs: The Current Armamentarium and Development of New Agents. Microbiol. Spectr. 2016, 4, 5. [Google Scholar] [CrossRef]
- Hamill, R.J. Amphotericin B formulations: A comparative review of efficacy and toxicity. Drugs 2013, 73, 919–934. [Google Scholar] [CrossRef]
- Zhong, X.; Yang, J.; Liu, H.; Liu, H.; Yang, Z.; Luo, P. Potential lipid-based strategies of amphotericin B designed for oral ad-ministration in clinical application. Drug Deliv. 2023, 30, 2161671. [Google Scholar] [CrossRef]
- Peyton, L.R.; Gallagher, S.; Hashemzadeh, M. Triazole antifungals: A review. Drugs Today 2015, 51, 705–718. [Google Scholar]
- Murray, M.; Hine, P. Treating progressive disseminated histoplasmosis in people living with HIV. Cochrane Database Syst. Rev. 2020, 4, CD013594. [Google Scholar] [PubMed]
- Govindarajan, A.; Bistas, K.G.; Ingold, C.J.; Aboeed, A. Fluconazole; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Ellsworth, M.; Ostrosky-Zeichner, L. Isavuconazole: Mechanism of Action, Clinical Efficacy, and Resistance. J. Fungi 2020, 6, 324. [Google Scholar] [CrossRef]
- Meena, D.S.; Kumar, D.; Bohra, G.K. Combination therapy in Mucormycosis: Current evidence from the world literature, a mini review. J. Mycol. Med. 2023, 33, 101332. [Google Scholar] [CrossRef]
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.A.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagrou, K.; Lewis, R.E.; et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Ogawa, R. Itraconazole and Voriconazole: The Complexity of Dose Adjustments. Clin. Infect. Dis. 2022, 75, 552. [Google Scholar] [CrossRef]
- Douglas, A.P.; Smibert, O.C.; Bajel, A.; Halliday, C.L.; Lavee, O.; McMullan, B.; Yong, M.K.; van Hal, S.J.; Chen, S. Australasian Antifungal Guidelines Steering Committee. Consensus guidelines for the diagnosis and management of invasive aspergillosis. Intern. Med. J. 2021, 7, 143–176. [Google Scholar] [CrossRef]
- Takesue, Y.; Hanai, Y.; Oda, K.; Hamada, Y.; Ueda, T.; Mayumi, T.; Matsumoto, K.; Fujii, S.; Takahashi, Y.; Miyazaki, Y.; et al. Clinical Practice Guideline for the Therapeutic Drug Monitoring of Voriconazole in Non-Asian and Asian Adult Patients: Consensus Review by the Japanese Society of Chemotherapy and the Japanese Society of Therapeutic Drug Monitoring. Clin. Ther. 2022, 44, 1604–1623. [Google Scholar] [CrossRef]
- Hanai, Y.; Hamada, Y.; Kimura, T.; Matsumoto, K.; Takahashi, Y.; Fujii, S.; Nishizawa, K.; Miyazaki, Y.; Takesue, Y. Favorable Effects of Voriconazole Trough Concentrations Exceeding 1 μg/mL on Treatment Success and All-Cause Mortality: A Systematic Review and Meta-Analysis. J. Fungi 2021, 7, 306. [Google Scholar] [CrossRef] [PubMed]
- Biagi, M.J.; Wiederhold, N.P.; Gibas, C.; Wickes, B.L.; Lozano, V.; Bleasdale, S.C.; Danziger, L. Development of high-level echinocandin resistance in a patient with recurrent Candida auris candidemia secondary to chronic candiduria. Open Forum Infect. Dis. 2019, 6, ofz262. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Giacobbe, D.; Berruti, M.; Del Puente, F.; Vena, V. Adequate duration of therapy in severe fungal infections. Curr. Opin. Crit. Care 2020, 26, 466–472. [Google Scholar] [CrossRef]
- Ben-Ami, R.; Kontoyiannis, D.P. Resistance to Antifungal Drugs. Infect. Dis. Clin. North Am. 2021, 35, 279–311. [Google Scholar] [CrossRef] [PubMed]
- Pathadka, S.; Yan, V.K.C.; Neoh, C.F.; Al-Badriyeh, D.; Kong, D.C.M.; Slavin, M.A.; Cowling, B.J.; Hung, I.F.N.; Wong, I.C.K.; Chanet, E.W. Global Consumption Trend of Antifungal Agents in Humans From 2008 to 2018: Data From 65 Middle- and High-Income Countries. Drugs 2022, 82, 1193–1205. [Google Scholar] [CrossRef]
- Rabaan, A.A.; Eljaaly, K.; Alfouzan, W.A.; Al Mutair, A.; Alhumaid, S.; Alfaraj, A.H.; Aldawood, Y.; Alsaleh, A.A.; Albayat, H.; Al Azmi, R.; et al. Psychogenetic, genetic and epigenetic mechanisms in Candida auris: Role in drug resistance. J. Infect. Public Health 2023, 16, 257–263. [Google Scholar] [CrossRef]
- Kaur, J.; Nobile, C.J. Antifungal drug-resistance mechanisms in Candida biofilms. Curr. Opin. Microbiol. 2023, 71, 102237. [Google Scholar] [CrossRef] [PubMed]
- Rybak, J.M.; Munoz, J.F.; Barker, K.S.; Parker, J.E.; Esquivel, B.D.; Berkow, E.L.; Lockhart, S.H.; Gade, L.; Palmer, G.E.; White, T.C.; et al. Mutations in TAC1B: A novel genetic determinant of clinical fluconazole resistance in Candida auris. mBio 2020, 11, e00365-20. [Google Scholar] [CrossRef] [PubMed]
- Izadi, A.; Gharehbolagh, A.S.; Sadeghi, F.; Talebi, M.; Darmiani, K.; Zarrinnia, A.; Zarei, F.; Peymaeei, F.; Khojasteh, S.; Borman, A.M.; et al. Drug repurposing against Candida auris: A systematic review. Mycoses 2022, 65, 784–793. [Google Scholar] [CrossRef] [PubMed]
- Khojasteh, S.; Abastabar, M.; Haghani, I.; Valadan, R.; Ghazanfari, S.; Abbasi, K.; Ahangarkani, F.; Zarrinfar, H.; Khodavaisy, S.; Badali, H.; et al. Five-year surveillance study of clinical and environmental Triazole-Resistant Aspergillus fumigatus isolates in Iran. Mycoses 2023, 66, 98–105. [Google Scholar] [CrossRef]
- Sen, P.; Vijay, M.; Singh, S.; Hameed, S.; Vijayaraghavan, P. Understanding the environmental drivers of clinical azole resistance in Aspergillus species. Drug Target Insights. 2022, 16, 25–35. [Google Scholar] [CrossRef]
- Cruz, R.; Wuest, W.M. Beyond Ergosterol: Strategies for Combatting Antifungal Resistance in Aspergillus fumigatus and Candida auris. Tetrahedron 2023, 133, 133268. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Devarajan, P.V. Enhancing safety and efficacy by altering the toxic aggregated state of amphotericin B in lipidic nanoformulations. Mol. Pharm. 2020, 17, 2186–2195. [Google Scholar] [CrossRef]
- Huang, T.; Li, X.; Maier, M.; O’Brien-Simpson, N.M.; Heath, D.E.; O’Connor, A.J. Using inorganic nanoparticles to fight fungal infections in the antimicrobial resistant era. Acta Biomater. 2023, 158, 56–79. [Google Scholar] [CrossRef]
- Lian, X.; Scott-Thomas, A.; Lewis, J.G.; Bhatia, M.; MacPherson, S.A.; Zeng, Y.; Chambers, S.T. Monoclonal Antibodies and Invasive Aspergillosis: Diagnostic and Therapeutic Perspectives. Int. J. Mol. Sci. 2022, 23, 5563. [Google Scholar] [CrossRef]
- Ulrich, S.; Ebel, F. Monoclonal antibodies as tools to combat fungal infections. J. Fungi 2020, 6, 22. [Google Scholar] [CrossRef] [Green Version]
- Thompson, G.R.; Soriano, A.; Cornely, A.O.; Kullberg, B.J.; Kollef, M.; Vazquez, J.; Honore, P.M.; Bassetti, M.; Pullman, J.; Chayakulkeeree, M.; et al. Rezafungin versus caspofungin for treatment of candidaemia and invasive candidiasis (ReSTORE): A multicentre, double-blind, dou-ble-dummy, randomised phase 3 trial. Lancet 2023, 401, 49–59. [Google Scholar] [CrossRef]
- Lamoth, F. Novel Therapeutic Approaches to Invasive Candidiasis: Considerations for the Clinician. Infect. Drug Resist. 2023, 16, 1087–1097. [Google Scholar] [CrossRef]
- Global Prevalence of Fungal Infections. Available online: http://en.fungaleducation.org/prevalence-of-fungal-infections/ (accessed on 24 March 2023).
- Perlin, D.S.; Rautemaa-Richardson, R.; Alastruey-Izquierdo, A. The global problem of antifungal resistance: Prevalence, mechanisms, and management. Lancet Infect. Dis. 2017, 17, e383–e392. [Google Scholar] [CrossRef]
- Benedict, K.; Molinari, N.A.; Jackson, B.R. Public Awareness of Invasive Fungal Diseases—United States, 2019. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 1343–1346. [Google Scholar] [CrossRef]
- Rodrigues, M.L.; Nosanchuk, J.D. Fungal Diseases as Neglected Pathogens: A Wake-up Call to Public Health Officials. PLoS Negl. Trop. Dis. 2020, 14, e0007964. [Google Scholar] [CrossRef] [Green Version]
- Ain Wan Ismail, W.N.; Jasmi, N.; Khan, T.M.; Hong, Y.H.; Neoh, C.F. The Economic Burden of Candidemia and Invasive Candidiasis: A Systematic Review. Value Health Reg. Issues. 2020, 21, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Benedict, K.; Jackson, B.R.; Chiller, T.; Beer, K.D. Estimation of Direct Healthcare Costs of Fungal Diseases in the United States. Clin. Infect. Dis. 2019, 68, 1791–1797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad Khan, M.S.; Alshehrei, F.; Al-Ghamdi, S.B.; Bamaga, M.A.; Al-Thubiani, A.S.; Alam, M.Z. Virulence and biofilms as promising targets in developing antipathogenic drugs against candidiasis. Future Sci. OA 2020, 6, FSO440. [Google Scholar] [CrossRef] [Green Version]
- Yadav, A.; Jain, K.; Wang, Y.; Pawar, K.; Kaur, H.; Sharma, H.K.; Tripathy, V.; Singh, A.; Xu, J.; Chowdhary, A. Candida auris on Apples: Diversity and Clinical Significance. mBio 2022, 13, e0051822. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Tong, J.; Li, Y.; Zhu, J.; Zhang, W.; Niu, L.; Zhang, H. Bacterial and fungal assemblages and functions associated with biofilms differ between diverse types of plastic debris in a freshwater system. Environ. Res. 2022, 15, 2388. [Google Scholar] [CrossRef] [PubMed]
- Houšť, J.; Spížek, J.; Havlíček, V. Antifungal Drugs. Metabolites 2020, 10, 106. [Google Scholar] [CrossRef] [Green Version]
- Muhaj, F.F.; George, S.J.; Nguyen, C.D.; Tyring, S.K. Antimicrobials and resistance part II: Antifungals, antivirals, and antiparasitics. J. Am. Acad. Dermatol. 2022, 86, 1207–1226. [Google Scholar] [CrossRef]
- Holmes, A.R.; Cardno, T.S.; Strouse, J.J.; Ivnitski-Steele, I.; Keniya, M.V.; Lackovic, K.; Monk, B.C.; Sklar, L.A.; Cannon, R.D. Targeting efflux pumps to overcome antifungal drug resistance. Future Med. Chem. 2016, 8, 1485–1501. [Google Scholar] [CrossRef] [Green Version]
- Global Action Fund for Fungal Infections (GAFFI). Available online: https://gaffi.org/ (accessed on 30 March 2023).
- Global AMR R&D Hub. Available online: https://dashboard.globalamrhub.org/ (accessed on 30 March 2023).
- Koehler, P.; Arendrup, M.C.; Arikan-Akdagli, S.; Bassetti, M.; Bretagne, S.; Klingspor, L.; Lagrou, K.; Meis, J.F.; Rautemaa-Richardson, R.; Schelenz, S.; et al. ECMM CandiReg—A ready to use platform for outbreaks and epidemiological studies. Multicent. Study Mycoses 2019, 62, 920–927. [Google Scholar] [CrossRef] [PubMed]
- The Global Antimicrobial Resistance and Use Surveillance System (GLASS)-FUNGI. WHO. Available online: https://www.who.int/initiatives/glass/glass-modules-5 (accessed on 30 March 2023).
- Kohlenberg, A.; Monnet, D.L.; Plachouras, D. Increasing number of cases and outbreaks caused by Candida auris in the EU/EEA, 2020 to 2021. Euro Surveill. 2022, 27, 2200846. [Google Scholar] [CrossRef]
- Sticchi, C.; Raso, R.; Ferrara, L.; Vecchi, E.; Ferrero, L.; Filippi, D.; Finotto, G.; Frassinelli, E.; Silvestre, C.; Zozzoli, S.; et al. Increasing number of cases due to Candida auris in north Italy, July 2019–December 2022. J. Clin. Med. 2023, 12, 1912. [Google Scholar] [CrossRef] [PubMed]
- Bongomin, F.; Gago, S.; Oladele, R.O.; Denning, D.W. Global and Multi-National Prevalence of Fungal Diseases—Estimate Precision. J. Fungi 2017, 3, 57. [Google Scholar] [CrossRef] [PubMed]
- Casadevall, A.; Kontoyiannis, D.P.; Robert, V. Environmental Candida auris and the Global Warming Emergence Hypothesis. mBio 2021, 12, e00360-21. [Google Scholar] [CrossRef]
- Robertson, E.; Abera, C.; Wood, K.; Deressa, K.; Mesfin, S.; Scantlebury, C. Striving towards access to essential medicines for human and animal health; a situational analysis of access to and use of antifungal medications for histoplasmosis in Ethiopia. PLoS ONE 2023, 18, e0278964. [Google Scholar] [CrossRef]


{kind=link}
| Main Fungal Forms in the Clinical Practice | Sensitivity to Main Antifungal Treatments | ||||||
|---|---|---|---|---|---|---|---|
| Polyene | Triazoles | Echinocandin | |||||
| Amphotericin B | Itraconazole | Voriconazole | Posaconazole | Isavuconazole | Fluconazole | Anidulafungin Caspofungin Micafungin | |
| Aspergillus fumigatus | low | low | high | medium | medium | low | high |
| Aspergillus hiratsukae | high | high | high | high | medium | Low | high |
| Aspergillus lentulus | low | low | low | medium | medium | low | high |
| Candida spp. | medium (not against C. krusei, C. lusitania) | medium/high | species-dependent | medium | species-dependent | species-dependent | medium/high |
| Fusarium spp. | medium | no activity/low | species-dependent | medium | low | low | low |
| Fusarium solani | medium | low | low | low | low | low | low |
| Lamentospora prolificans | low | low | low/medium | low | low | low | low |
| Mucorales | medium | no activity/low | no activity/low | species-dependent | species-dependent | low | low |
| Antifungal Compound/Agent | Study Outcome | Reference |
|---|---|---|
| Nanoparticles/nanoformulations | High efficacy and selectivity index indicated the superiority of the amphotericin nanoformulations. | [39] |
| Surface charge, hydrophobicity, and stabilizing agents of nanoparticles can affect the antifungal activities. Long-term use may lead to accumulation in the host’s organs and cause harm. Biodistribution studies are needed before clinical use could be deemed safe. Synergistic fungicidal effects of antifungal drugs with inorganic nanoparticles could reduce dosage of both these agents, thereby reducing toxicity. | [40] | |
| Monoclonal antibodies | Passive immunization with mAbs against Aspergillus spp. improved survival in mouse models of invasive aspergillosis. | [41] |
| Effectiveness depends by several variables: type of pathogen, antifungal mechanism of action, biological properties of immunoglobulins, routes of experimental infections, prophylactic rather than therapeutic use, optimal immunoglobulin dosage. | [42] | |
| Rezafungin | Rezafungin was non-inferior to caspofungin for the primary endpoints of day-14 global cure and 30-day all-cause mortality. Phase 3 results show the efficacy and safety of rezafungin and support its ongoing development. | [43] |
| Ibrexafunge, Fosmanogepix | Ibrexafungerp and fosmanogepix are first-in-class molecules and display extended antifungal spectrum, in particular against echinocandin-resistant Candida spp. (including C. auris). | [44] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitiello, A.; Ferrara, F.; Boccellino, M.; Ponzo, A.; Cimmino, C.; Comberiati, E.; Zovi, A.; Clemente, S.; Sabbatucci, M. Antifungal Drug Resistance: An Emergent Health Threat. Biomedicines 2023, 11, 1063. https://doi.org/10.3390/biomedicines11041063
Vitiello A, Ferrara F, Boccellino M, Ponzo A, Cimmino C, Comberiati E, Zovi A, Clemente S, Sabbatucci M. Antifungal Drug Resistance: An Emergent Health Threat. Biomedicines. 2023; 11(4):1063. https://doi.org/10.3390/biomedicines11041063
Chicago/Turabian StyleVitiello, Antonio, Francesco Ferrara, Mariarosaria Boccellino, Annarita Ponzo, Carla Cimmino, Emilio Comberiati, Andrea Zovi, Salvatore Clemente, and Michela Sabbatucci. 2023. "Antifungal Drug Resistance: An Emergent Health Threat" Biomedicines 11, no. 4: 1063. https://doi.org/10.3390/biomedicines11041063
APA StyleVitiello, A., Ferrara, F., Boccellino, M., Ponzo, A., Cimmino, C., Comberiati, E., Zovi, A., Clemente, S., & Sabbatucci, M. (2023). Antifungal Drug Resistance: An Emergent Health Threat. Biomedicines, 11(4), 1063. https://doi.org/10.3390/biomedicines11041063