
Microbiological and Cytokine Profiling of Menstrual Blood for the Assessment of Endometrial Receptivity: A Pilot Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. General Information
2.2. Biomaterial Collection and Processing
2.3. Analysis of Immune Mediators
2.4. Microbiological Analysis
2.5. Statistical Analysis
3. Results
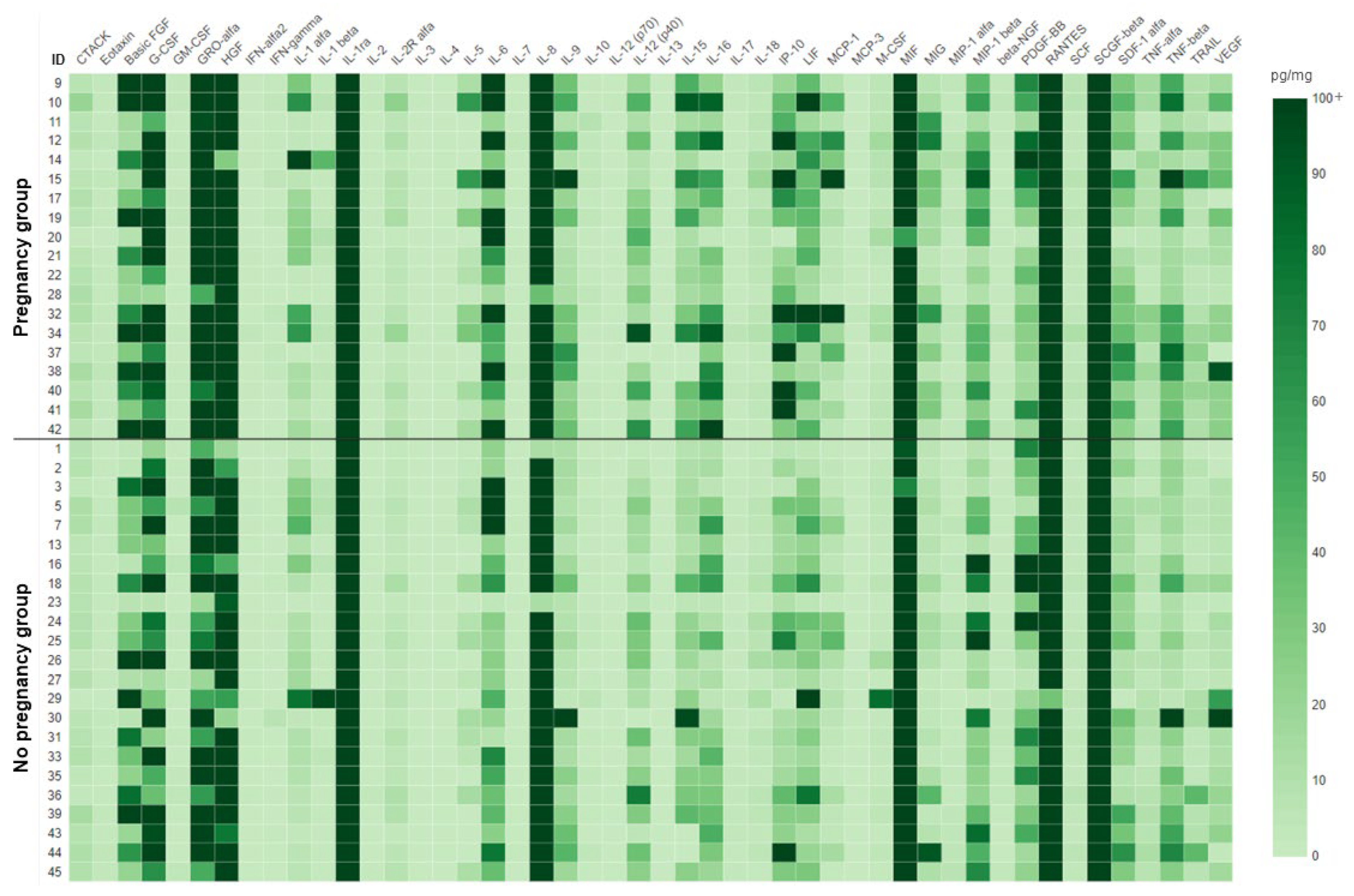
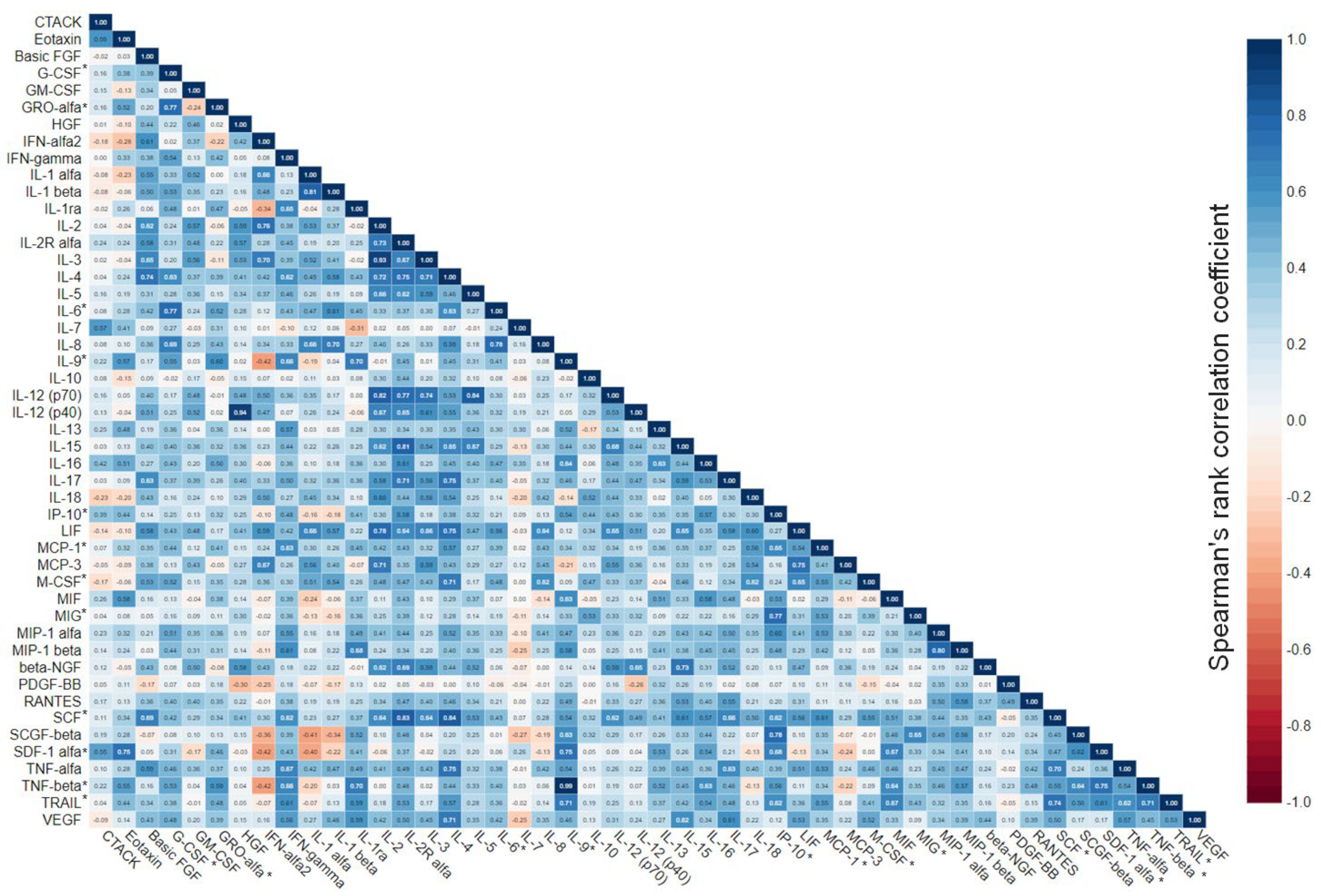
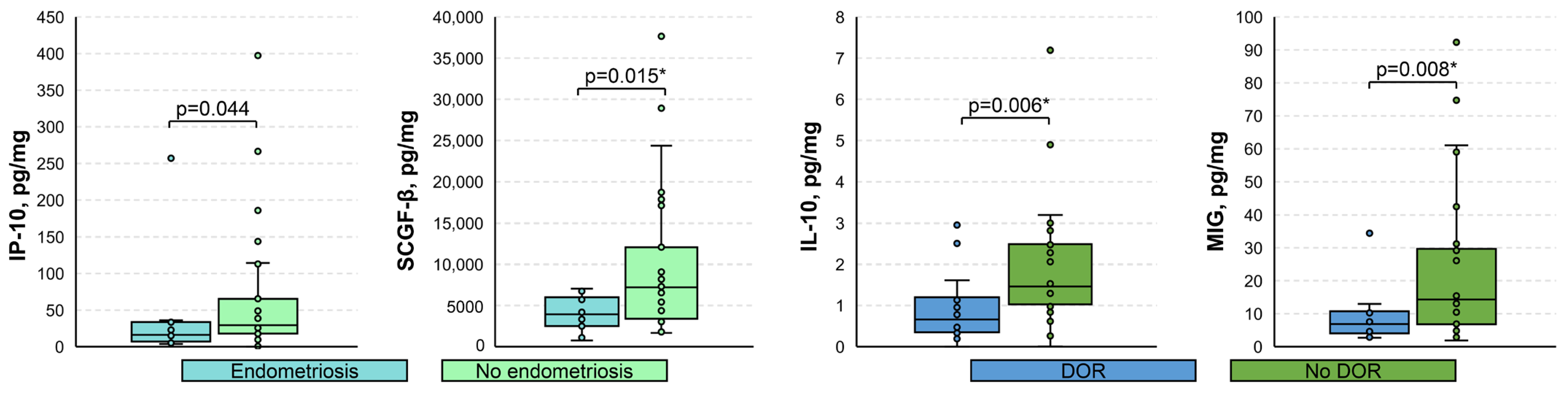
3.1. Cytokine Profiling
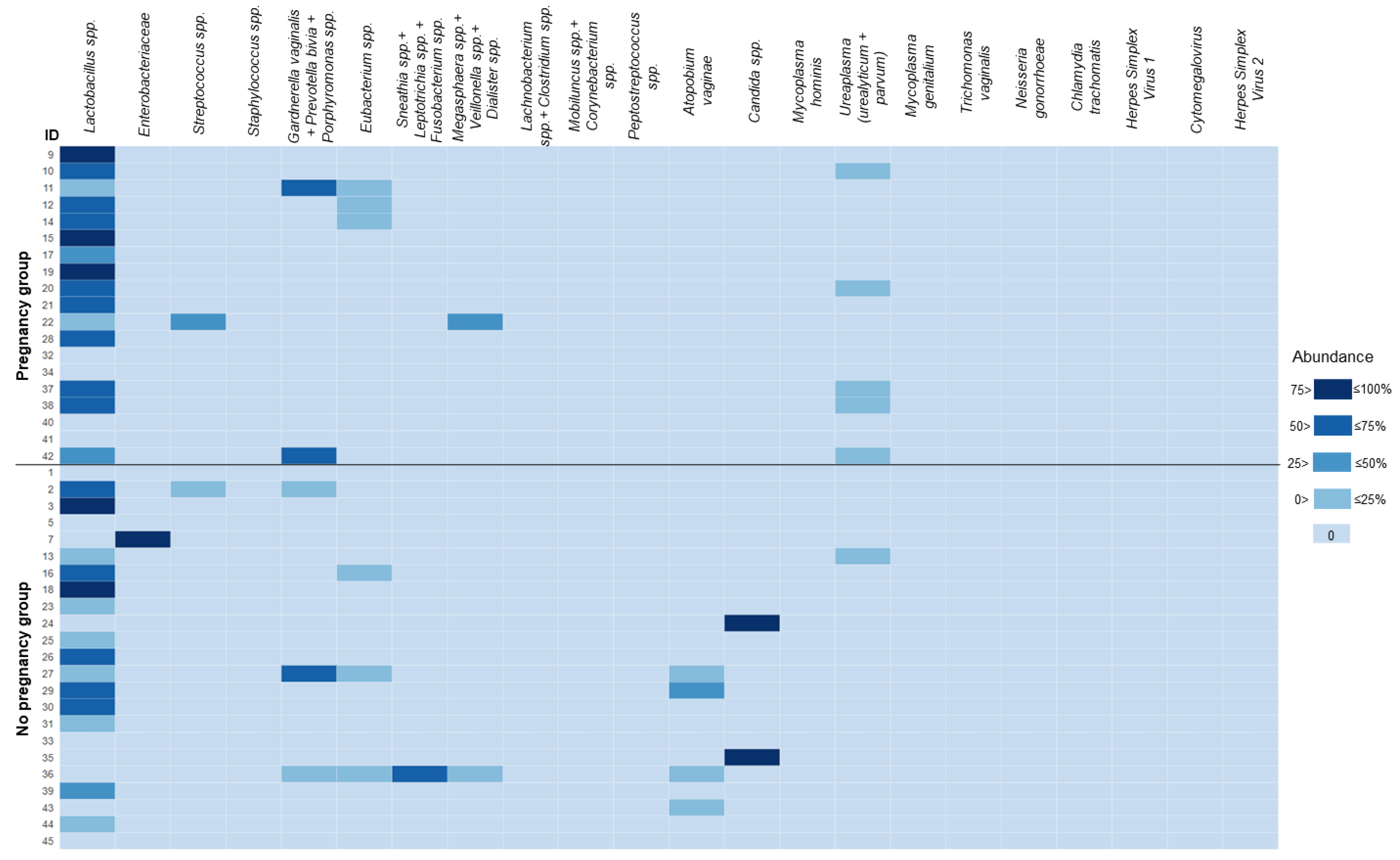
3.2. Microbiological Profiling
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO International Classification of Diseases, 11th Revision (ICD-11). Available online: https://icd.who.int/ (accessed on 15 February 2023).
- Cox, C.M.; Thoma, M.E.; Tchangalova, N.; Mburu, G.; Bornstein, M.J.; Johnson, C.L.; Kiarie, J. Infertility prevalence and the methods of estimation from 1990 to 2021: A systematic review and meta-analysis. Hum. Reprod. Open 2022, 2022, hoac051. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Gong, T.T.; Jiang, Y.T.; Zhang, S.; Zhao, Y.H.; Wu, Q.J. Global, Regional, and National Prevalence and Disability-Adjusted Life-Years for Infertility in 195 Countries and Territories, 1990–2017: Results from a Global Burden of Disease Study, 2017. Aging 2019, 11, 10952–10991. [Google Scholar] [CrossRef] [PubMed]
- De Mouzon, J.; Chambers, G.M.; Zegers-Hochschild, F.; Mansour, R.; Ishihara, O.; Banker, M.; Dyer, S.; Kupka, M.; David Adamson, G. International committee for monitoring assisted reproductive technologies world report: Assisted reproductive technology 2012. Hum. Reprod. 2020, 35, 1900–1913. [Google Scholar] [CrossRef] [PubMed]
- Graham, M.E.; Jelin, A.; Hoon, A.H.J.; Wilms Floet, A.M.; Levey, E.; Graham, E.M. Assisted reproductive technology: Short- and long-term outcomes. Dev. Med. Child Neurol. 2023, 65, 38–49. [Google Scholar] [CrossRef]
- Oron, G.; Son, W.Y.; Buckett, W.; Tulandi, T.; Holzer, H. The association between embryo quality and perinatal outcome of singletons born after single embryo transfers: A pilot study. Hum. Reprod. 2014, 29, 1444–1451. [Google Scholar] [CrossRef]
- Zhu, J.; Lian, Y.; Li, M.; Chen, L.; Liu, P.; Qiao, J. Does IVF cleavage stage embryo quality affect pregnancy complications and neonatal outcomes in singleton gestations after double embryo transfers? J. Assist. Reprod. Genet. 2014, 31, 1635–1641. [Google Scholar] [CrossRef]
- Greco, E.; Litwicka, K.; Minasi, M.G.; Cursio, E.; Greco, P.F.; Barillari, P. Preimplantation Genetic Testing: Where We Are Today. Int. J. Mol. Sci. 2020, 21, 4381. [Google Scholar] [CrossRef]
- Ji, H.; Zhou, Y.; Cao, S.; Zhang, J.; Ling, X.; Zhao, C.; Shen, R. Effect of Embryo Developmental Stage, Morphological Grading, and Ploidy Status on Live Birth Rate in Frozen Cycles of Single Blastocyst Transfer. Reprod. Sci. 2021, 28, 1079–1091. [Google Scholar] [CrossRef]
- Lessey, B.A.; Young, S.L. What exactly is endometrial receptivity? Fertil. Steril. 2019, 111, 611–617. [Google Scholar] [CrossRef]
- Jain, M.; Samokhodskaya, L.; Mladova, E.; Panina, O. Mucosal biomarkers for endometrial receptivity: A promising yet underexplored aspect of reproductive medicine. Syst. Biol. Reprod. Med. 2022, 68, 13–24. [Google Scholar] [CrossRef]
- Diaz-Martínez, M.D.C.; Bernabeu, A.; Lledó, B.; Carratalá-Munuera, C.; Quesada, J.A.; Lozano, F.M.; Ruiz, V.; Morales, R.; Llácer, J.; Ten, J.; et al. Impact of the Vaginal and Endometrial Microbiome Pattern on Assisted Reproduction Outcomes. J. Clin. Med. 2021, 10, 4063. [Google Scholar] [CrossRef]
- Moreno, I.; Garcia-Grau, I.; Perez-Villaroya, D.; Gonzalez-Monfort, M.; Bahçeci, M.; Barrionuevo, M.J.; Taguchi, S.; Puente, E.; Dimattina, M.; Lim, M.W.; et al. Endometrial microbiota composition is associated with reproductive outcome in infertile patients. Microbiome 2022, 10, 1. [Google Scholar] [CrossRef]
- Craciunas, L.; Gallos, I.; Chu, J.; Bourne, T.; Quenby, S.; Brosens, J.J.; Coomarasamy, A. Conventional and modern markers of endometrial receptivity: A systematic review and meta-analysis. Hum. Reprod. Update 2019, 25, 202–223. [Google Scholar] [CrossRef] [PubMed]
- Camargo-Díaz, F.; García, V.; Ocampo-Bárcenas, A.; González-Marquez, H.; López-Bayghen, E. Colony stimulating factor-1 and leukemia inhibitor factor expression from current-cycle cannula isolated endometrial cells are associated with increased endometrial receptivity and pregnancy. BMC Women’s Health 2017, 17, 63. [Google Scholar] [CrossRef] [PubMed]
- Boomsma, C.M.; Kavelaars, A.; Eijkemans, M.J.C.; Lentjes, E.G.; Fauser, B.C.J.M.; Heijnen, C.J.; MacKlon, N.S. Endometrial secretion analysis identifies a cytokine profile predictive of pregnancy in IVF. Hum. Reprod. 2009, 24, 1427–1435. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of Russian Federation Clinical Recommendations (Treatment Protocol) № 15-4/N/2-1908. Assisted Reproductive Technologies and Artificial Insemination. Available online: https://rahr.ru/d_pech_mat_metod/BPT1.pdf (accessed on 15 February 2023).
- Armstrong, R.A. When to use the Bonferroni correction. Ophthalmic Physiol. Opt. J. Br. Coll. Ophthalmic Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Lee, D.K. What is the proper way to apply the multiple comparison test? Korean J. Anesthesiol. 2018, 71, 353–360. [Google Scholar] [CrossRef]
- Sanchez-Mata, A.; Gonzalez-Muñoz, E. Understanding menstrual blood-derived stromal/stem cells: Definition and properties. Are we rushing into their therapeutic applications? iScience 2021, 24, 103501. [Google Scholar] [CrossRef]
- Crona Guterstam, Y.; Strunz, B.; Ivarsson, M.A.; Zimmer, C.; Melin, A.-S.; Jonasson, A.F.; Björkström, N.K.; Gidlöf, S.B. The cytokine profile of menstrual blood. Acta Obstet. Gynecol. Scand. 2021, 100, 339–346. [Google Scholar] [CrossRef]
- Tortorella, C.; Piazzolla, G.; Matteo, M.; Pinto, V.; Tinelli, R.; Sabbà, C.; Fanelli, M.; Cicinelli, E. Interleukin-6, interleukin-1β, and tumor necrosis factor α in menstrual effluents as biomarkers of chronic endometritis. Fertil. Steril. 2014, 101, 242–247. [Google Scholar] [CrossRef]
- Vitagliano, A.; Laganà, A.S.; De Ziegler, D.; Cicinelli, R.; Santarsiero, C.M.; Buzzaccarini, G.; Chiantera, V.; Cicinelli, E.; Marinaccio, M. Chronic Endometritis in Infertile Women: Impact of Untreated Disease, Plasma Cell Count and Antibiotic Therapy on IVF Outcome—A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 2250. [Google Scholar] [CrossRef]
- Granot, I.; Gnainsky, Y.; Dekel, N. Endometrial inflammation and effect on implantation improvement and pregnancy outcome. Reproduction 2012, 144, 661–668. [Google Scholar] [CrossRef]
- Jin, X.H.; Li, Y.; Li, D. Intrauterine interventions for women with two or more implantation failures: A systematic review and network meta-analysis. Front. Endocrinol. 2022, 13, 959121. [Google Scholar] [CrossRef] [PubMed]
- Rahiminejad, M.E.; Moaddab, A.; Ebrahimi, M.; Rabiee, S.; Zamani, A.; Ezzati, M.; Shamshirsaz, A.A. The relationship between some endometrial secretion cytokines and in vitro fertilization. Iran. J. Reprod. Med. 2015, 13, 557–562. [Google Scholar] [PubMed]
- Khadem, N.; Mansoori, M.; Attaran, M.; Attaranzadeh, A.; Zohdi, E. Association of il-1 and tnf-α levels in endometrial secretion and success of embryo transfer in ivf/icsi cycles. Int. J. Fertil. Steril. 2019, 13, 236–239. [Google Scholar] [CrossRef]
- Yoshino, O.; Osuga, Y.; Koga, K.; Hirota, Y.; Tsutsumi, O.; Yano, T.; Morita, Y.; Momoeda, M.; Fujiwara, T.; Kugu, K.; et al. Concentrations of interferon-gamma-induced protein-10 (IP-10), an antiangiogenic substance, are decreased in peritoneal fluid of women with advanced endometriosis. Am. J. Reprod. Immunol. 2003, 50, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, H.; Fedorcsak, P.; Isaacson, K.; Tevonian, E.; Xiao, A.; Beste, M.; Qvigstad, E.; Lauffenburger, D.; Griffith, L. Endometrial cytokines in patients with and without endometriosis evaluated for infertility. Fertil. Steril. 2022, 117, 629–640. [Google Scholar] [CrossRef] [PubMed]
- Tissier, H. Recherches sur la Flore Intestinale des Nourrissons:(état Normal et Pathologique). 1900. Available online: https://www.biusante.parisdescartes.fr/histoire/medica/resultats/index.php?do=page&cote=TPAR1900x529&p=195 (accessed on 15 February 2023).
- Butler, B. Value of endometrial cultures in sterility investigation. Fertil. Steril. 1958, 9, 269–273. [Google Scholar] [CrossRef]
- Toson, B.; Simon, C.; Moreno, I. The Endometrial Microbiome and Its Impact on Human Conception. Int. J. Mol. Sci. 2022, 23, 485. [Google Scholar] [CrossRef]
- Winters, A.D.; Romero, R.; Gervasi, M.T.; Gomez-Lopez, N.; Tran, M.R.; Garcia-Flores, V.; Pacora, P.; Jung, E.; Hassan, S.S.; Hsu, C.-D.; et al. Does the endometrial cavity have a molecular microbial signature? Sci. Rep. 2019, 9, 9905. [Google Scholar] [CrossRef]
- Miles, S.M.; Hardy, B.L.; Merrell, D.S. Investigation of the microbiota of the reproductive tract in women undergoing a total hysterectomy and bilateral salpingo-oopherectomy. Fertil. Steril. 2017, 107, 813.e1–820.e1. [Google Scholar] [CrossRef] [PubMed]
- Walther-António, M.R.S.; Chen, J.; Multinu, F.; Hokenstad, A.; Distad, T.J.; Cheek, E.H.; Keeney, G.L.; Creedon, D.J.; Nelson, H.; Mariani, A.; et al. Potential contribution of the uterine microbiome in the development of endometrial cancer. Genome Med. 2016, 8, 122. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Song, X.; Wei, W.; Zhong, H.; Dai, J.; Lan, Z.; Li, F.; Yu, X.; Feng, Q.; Wang, Z.; et al. The microbiota continuum along the female reproductive tract and its relation to uterine-related diseases. Nat. Commun. 2017, 8, 875. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.M.; Haick, A.; Nkwopara, E.; Garcia, R.; Rendi, M.; Agnew, K.; Fredricks, D.N.; Eschenbach, D. Colonization of the upper genital tract by vaginal bacterial species in nonpregnant women. Am. J. Obstet. Gynecol. 2015, 212, 611.e1–611.e9. [Google Scholar] [CrossRef]
- Franasiak, J.M.; Werner, M.D.; Juneau, C.R.; Tao, X.; Landis, J.; Zhan, Y.; Treff, N.R.; Scott, R.T. Endometrial microbiome at the time of embryo transfer: Next-generation sequencing of the 16S ribosomal subunit. J. Assist. Reprod. Genet. 2016, 33, 129–136. [Google Scholar] [CrossRef]
- Kyono, K.; Hashimoto, T.; Kikuchi, S.; Nagai, Y.; Sakuraba, Y. A pilot study and case reports on endometrial microbiota and pregnancy outcome: An analysis using 16S rRNA gene sequencing among IVF patients, and trial therapeutic intervention for dysbiotic endometrium. Reprod. Med. Biol. 2019, 18, 72–82. [Google Scholar] [CrossRef]
- Rocha, M.N.D.C.; Florêncio, R.D.S.; Alves, R.R.F. The role played by granulocyte colony stimulating factor (G-CSF) on women submitted to in vitro fertilization associated with thin endometrium: Systematic review. JBRA Assist. Reprod. 2020, 24, 278–282. [Google Scholar] [CrossRef]
- Jindal, P.C.; Singh, R.; Singh, M. O-026 RCT of INTRA-Uterine administration of granulocyte colony-stimulating factor (G-CSF) before embryo-transfer in resistant thin endometrium in IVF-ICSI cycles. Hum. Reprod. 2022, 37, deac104.026. [Google Scholar] [CrossRef]
- Budrys, N.M.; Nair, H.B.; Liu, Y.-G.; Kirma, N.B.; Binkley, P.A.; Kumar, S.; Schenken, R.S.; Tekmal, R.R. Increased expression of macrophage colony-stimulating factor and its receptor in patients with endometriosis. Fertil. Steril. 2012, 97, 1129.e1–1135.e1. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Pregnancy Group (n = 19) | No Pregnancy Group (n = 23) |
|---|---|---|
| Age, years | 34.7 (19.0–50.0) | 38.3 (31.0–51.0) |
| Body mass index, kg/m2 | 21.7 (17.3–30.5) | 21.9 (17.3–27.9) |
| ART details: - IVF - IVF/ICSI - cryo-ET - stimulated cycle - natural cycle - PGT | 12/19 7/19 19/19 18/19 1/19 6/19 | 9/23 14/23 23/23 23/23 0/23 13/23 |
| Infertility factors: - tubo-peritoneal factor - endometriosis - DOR - uterine factor - endocrinologic factor - male factor - unknown factor | 5/19 3/19 4/19 1/19 1/19 6/19 2/19 | 3/23 8/23 12/23 1/23 0/23 5/23 3/23 |
| Uterine adhesions | 0/19 | 1/23 |
| Uterine fibroids | 0/19 | 2/23 |
| RIF | 1/19 | 5/23 |
| RPL | 0/19 | 1/23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jain, M.; Mladova, E.; Shichanina, A.; Kirillova, K.; Povarova, A.; Scherbakova, L.; Samokhodskaya, L.; Panina, O. Microbiological and Cytokine Profiling of Menstrual Blood for the Assessment of Endometrial Receptivity: A Pilot Study. Biomedicines 2023, 11, 1284. https://doi.org/10.3390/biomedicines11051284
Jain M, Mladova E, Shichanina A, Kirillova K, Povarova A, Scherbakova L, Samokhodskaya L, Panina O. Microbiological and Cytokine Profiling of Menstrual Blood for the Assessment of Endometrial Receptivity: A Pilot Study. Biomedicines. 2023; 11(5):1284. https://doi.org/10.3390/biomedicines11051284
Chicago/Turabian StyleJain, Mark, Elena Mladova, Anna Shichanina, Karina Kirillova, Anna Povarova, Liya Scherbakova, Larisa Samokhodskaya, and Olga Panina. 2023. "Microbiological and Cytokine Profiling of Menstrual Blood for the Assessment of Endometrial Receptivity: A Pilot Study" Biomedicines 11, no. 5: 1284. https://doi.org/10.3390/biomedicines11051284
APA StyleJain, M., Mladova, E., Shichanina, A., Kirillova, K., Povarova, A., Scherbakova, L., Samokhodskaya, L., & Panina, O. (2023). Microbiological and Cytokine Profiling of Menstrual Blood for the Assessment of Endometrial Receptivity: A Pilot Study. Biomedicines, 11(5), 1284. https://doi.org/10.3390/biomedicines11051284