
Serum Urate Levels and Ultrasound Characteristics of Carotid Atherosclerosis across Obesity Phenotypes
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Physical Evaluation
2.3. Laboratory Examination
2.4. Ultrasound Assessment
2.5. Statistical Analysis
3. Results
3.1. General Characteristics
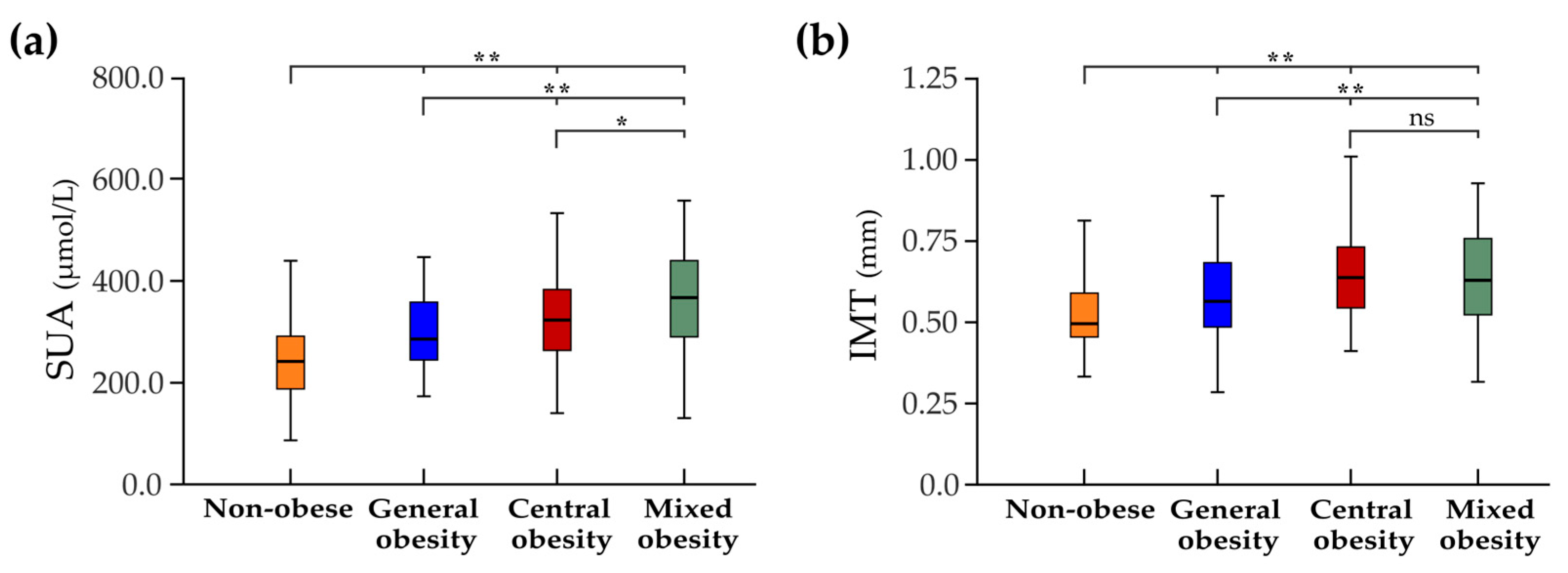
3.2. Serum Urate Levels
3.3. Ultrasound Characteristics
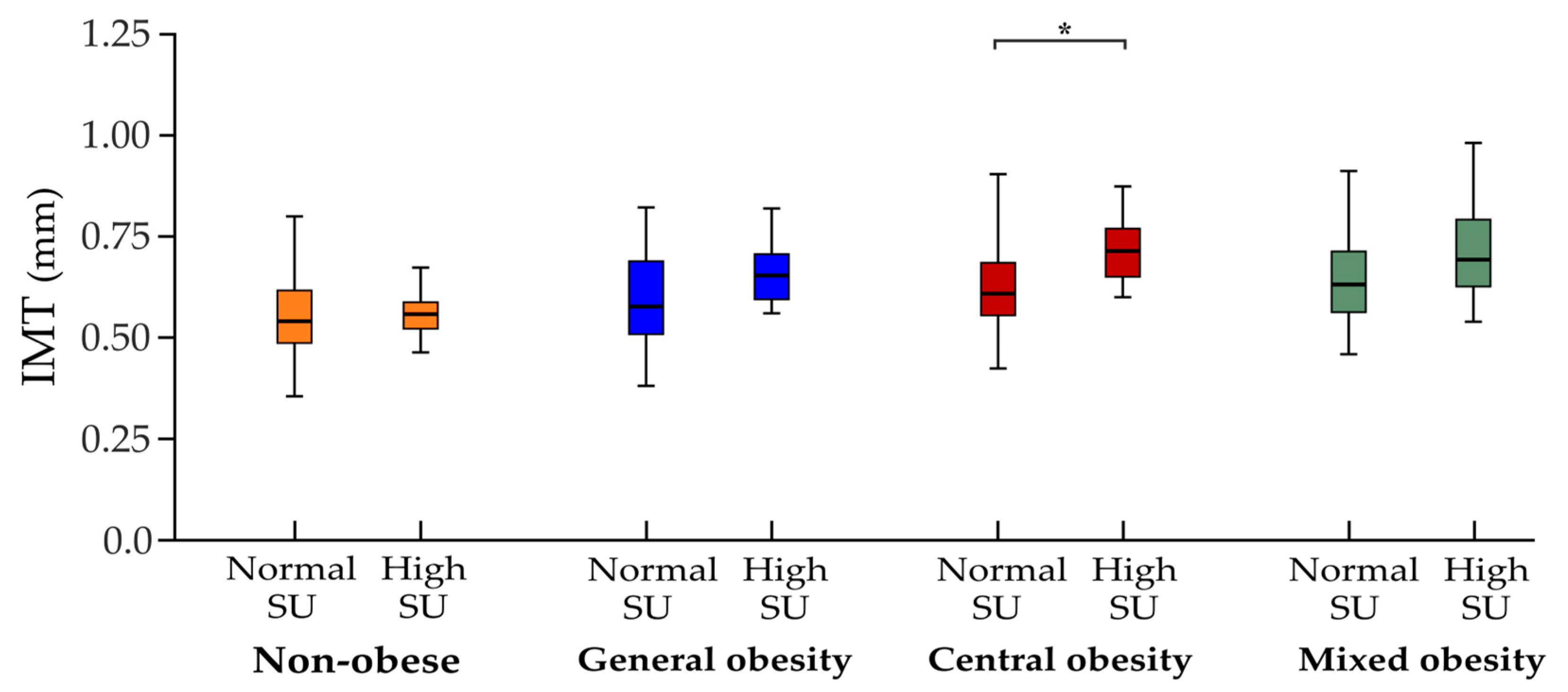
3.4. Serum Urate Levels and Carotid Atherosclerosis
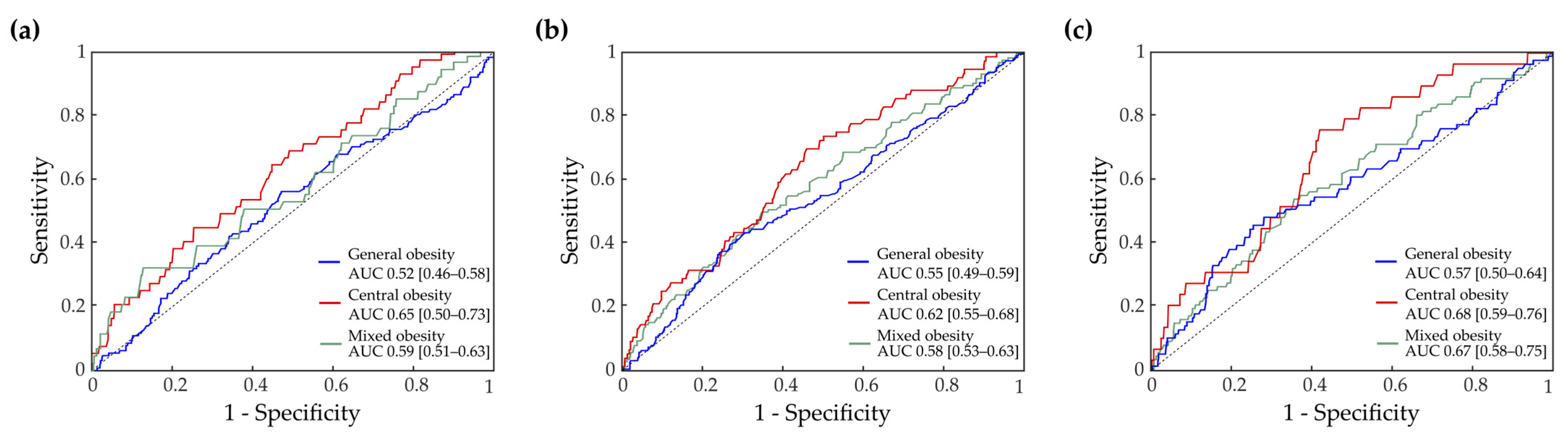
3.5. ROC Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yusuf, S.; Joseph, P.; Rangarajan, S.; Islam, S.; Mente, A.; Hystad, P.; Brauer, M.; Kutty, V.R.; Gupta, R.; Wielgosz, A. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): A prospective cohort study. Lancet 2020, 395, 795–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bos, M.J.; Koudstaal, P.J.; Hofman, A.; Witteman, J.C.; Breteler, M.M. Uric acid is a risk factor for myocardial infarction and stroke: The Rotterdam study. Stroke 2006, 37, 1503–1507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borghi, C.; Rosei, E.A.; Bardin, T.; Dawson, J.; Dominiczak, A.; Kielstein, J.T.; Manolis, A.J.; Perez-Ruiz, F.; Mancia, G. Serum uric acid and the risk of cardiovascular and renal disease. J. Hypertens. 2015, 33, 1729–1741. [Google Scholar] [CrossRef]
- Stack, A.; Hanley, A.; Casserly, L.; Cronin, C.; Abdalla, A.; Kiernan, T.; Murthy, B.; Hegarty, A.; Hannigan, A.; Nguyen, H. Independent and conjoint associations of gout and hyperuricaemia with total and cardiovascular mortality. QJM Int. J. Med. 2013, 106, 647–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagliardi, A.C.; Miname, M.H.; Santos, R.D. Uric acid: A marker of increased cardiovascular risk. Atherosclerosis 2009, 202, 11–17. [Google Scholar] [CrossRef]
- Mandviwala, T.; Khalid, U.; Deswal, A. Obesity and cardiovascular disease: A risk factor or a risk marker? Curr. Atheroscler. Rep. 2016, 18, 21. [Google Scholar] [CrossRef]
- Kernan, W.N.; Inzucchi, S.E.; Sawan, C.; Macko, R.F.; Furie, K.L. Obesity: A stubbornly obvious target for stroke prevention. Stroke 2013, 44, 278–286. [Google Scholar] [CrossRef]
- Yue, J.-R.; Huang, C.-Q.; Dong, B.-R. Association of serum uric acid with body mass index among long-lived Chinese. Exp. Gerontol. 2012, 47, 595–600. [Google Scholar] [CrossRef]
- Tanaka, K.; Ogata, S.; Tanaka, H.; Omura, K.; Honda, C.; Group, O.T.R.; Hayakawa, K. The relationship between body mass index and uric acid: A study on Japanese adult twins. Environ. Health Prev. Med. 2015, 20, 347–353. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.-m.; Gan, L.; Su, Y.; Li, F. Association between serum uric acid level and body mass index in sex-and age-specific groups in southwestern China. Endocr. Pract. 2019, 25, 438–445. [Google Scholar] [CrossRef]
- Ishizaka, N.; Ishizaka, Y.; Toda, A.; Tani, M.; Koike, K.; Yamakado, M.; Nagai, R. Changes in waist circumference and body mass index in relation to changes in serum uric acid in Japanese individuals. J. Rheumatol. 2010, 37, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Biradar, M.I.; Chiang, K.-M.; Yang, H.-C.; Huang, Y.-T.; Pan, W.-H. The causal role of elevated uric acid and waist circumference on the risk of metabolic syndrome components. Int. J. Obes. 2020, 44, 865–874. [Google Scholar] [CrossRef]
- Onat, A.; Uyarel, H.; Hergenc, G.; Karabulut, A.; Albayrak, S.; Sarı, I.; Yazıcı, M.; Keleş, I. Serum uric acid is a determinant of metabolic syndrome in a population-based study. Am. J. Hypertens. 2006, 19, 1055–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groppa, S. Accidentul Vascular Cerebral: Epidemiologie, Factori de Risc, Prevenție; Î. S. Firma Editorial-Poligrafică “Tipografia Centrală”: Chişinău, Moldova, 2020; 212p. [Google Scholar]
- Groppa, S.; Zota, E.; Efremova, D.; Chiforişina, V. Profilaxia secundară a accidentului vascular cerebral ischemic şi factorii de risc modificabili în populaţia Republicii Moldova. Bul. Acad. Ştiinţe Moldovei Ştiinţe Med. 2015, 49, 130–133. [Google Scholar]
- Bots, M.L.; Hoes, A.W.; Koudstaal, P.J.; Hofman, A.; Grobbee, D.E. Common carotid intima-media thickness and risk of stroke and myocardial infarction: The Rotterdam Study. Circulation 1997, 96, 1432–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsivgoulis, G.; Vemmos, K.; Papamichael, C.; Spengos, K.; Manios, E.; Stamatelopoulos, K.; Vassilopoulos, D.; Zakopoulos, N. Common carotid artery intima-media thickness and the risk of stroke recurrence. Stroke 2006, 37, 1913–1916. [Google Scholar] [CrossRef] [PubMed]
- Parish, S.; Arnold, M.; Clarke, R.; Du, H.; Wan, E.; Kurmi, O.; Chen, Y.; Guo, Y.; Bian, Z.; Collins, R. Assessment of the role of carotid atherosclerosis in the association between major cardiovascular risk factors and ischemic stroke subtypes. JAMA Netw. Open 2019, 2, e194873. [Google Scholar] [CrossRef]
- Geroulakos, G.; Domjan, J.; Nicolaides, A.; Stevens, J.; Labropoulos, N.; Ramaswami, G.; Belcaro, G.; Mansfield, A. Ultrasonic carotid artery plaque structure and the risk of cerebral infarction on computed tomography. J. Vasc. Surg. 1994, 20, 263–266. [Google Scholar] [CrossRef] [Green Version]
- Kitamura, A.; Iso, H.; Imano, H.; Ohira, T.; Okada, T.; Sato, S.; Kiyama, M.; Tanigawa, T.; Yamagishi, K.; Shimamoto, T. Carotid intima-media thickness and plaque characteristics as a risk factor for stroke in Japanese elderly men. Stroke 2004, 35, 2788–2794. [Google Scholar] [CrossRef] [Green Version]
- Ma, M.; Wang, L.; Huang, W.; Zhong, X.; Li, L.; Wang, H.; Peng, B.; Mao, M. Meta-analysis of the correlation between serum uric acid level and carotid intima-media thickness. PLoS ONE 2021, 16, e0246416. [Google Scholar] [CrossRef]
- Neogi, T.; Ellison, R.C.; Hunt, S.; Terkeltaub, R.; Felson, D.T.; Zhang, Y. Serum uric acid is associated with carotid plaques: The National Heart, Lung, and Blood Institute Family Heart Study. J. Rheumatol. 2009, 36, 378–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Zhou, Y.; Dong, K.; Wang, A.; Yang, X.; Zhang, C.; Zhu, Y.; Wu, S.; Zhao, X. The association between serum uric acid levels and the prevalence of vulnerable atherosclerotic carotid plaque: A cross-sectional study. Sci. Rep. 2015, 5, 10003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Efremova, D.; Ciolac, D.; Zota, E.; Glavan, D.; Ciobanu, N.; Aulitzky, W.; Nics, A.M.; Trinka, E.; Yamada, C.; Movila, A. Dissecting the Spectrum of Stroke Risk Factors in an Apparently Healthy Population: Paving the Roadmap to Primary Stroke Prevention. J. Cardiovasc. Dev. Dis. 2023, 10, 35. [Google Scholar] [CrossRef]
- Efremova, D.; Groppa, S. Factorii de risc ai accidentului vascular cerebral la adulţii tineri în populaţia Republicii Moldova: Studiu descriptiv. Rev. Ştiinţe Ale Sănătăţii Mold. 2020, 25, 31–39. [Google Scholar]
- World Health Organization. Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation, Geneva, 8–11 December 2008; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; LeFevre, M.L.; MacKenzie, T.D.; Ogedegbe, O. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fodor, G. Primary prevention of CVD: Treating dyslipidemia. Am. Fam. Physician 2011, 83, 1207–1208. [Google Scholar]
- Neilson, J.; Bonnon, A.; Dickson, A.; Roddy, E. Gout: Diagnosis and management—Summary of NICE guidance. BMJ 2022, 378, o1754. [Google Scholar] [CrossRef]
- Maloberti, A.; Giannattasio, C.; Bombelli, M.; Desideri, G.; Cicero, A.; Muiesan, M.; Rosei, E.; Salvetti, M.; Ungar, A.; Rivasi, G. Hyperuricemia and risk of cardiovascular outcomes: The experience of the URRAH (uric acid right for heart health) project. High Blood Press. Cardiovasc. Prev. 2020, 27, 121–128. [Google Scholar] [CrossRef]
- Groppa, S.; Zota, E.; Chiforişina, V.; Efremova, D. Importanţa caracteristicilor ultrasonografice a plăcilor aterosclerotice carotidiene ca factor predictor a accidentului vascular cerebral ischemic. Bul. Acad. Ştiinţe Moldovei Ştiinţe Med. 2015, 49, 134–137. [Google Scholar]
- Touboul, P.-J.; Hennerici, M.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Fatar, M. Mannheim carotid intima-media thickness consensus (2004–2006). Cerebrovasc. Dis. 2007, 23, 75–80. [Google Scholar] [CrossRef]
- Csiba, L.; Baracchini, C. Manual of Neurosonology; Cambridge University Press: Cambridge, UK, 2016. [Google Scholar]
- Spence, J.D. Technology insight: Ultrasound measurement of carotid plaque—Patient management, genetic research, and therapy evaluation. Nat. Clin. Pract. Neurol. 2006, 2, 611–619. [Google Scholar] [CrossRef]
- Geroulakos, G.; Ramaswami, G.; Nicolaides, A.; James, K.; Labropoulos, N.; Belcaro, G.; Holloway, M. Characterization of symptomatic and asymptomatic carotid plaques using high-resolution real-time ultrasonography. J. Br. Surg. 1993, 80, 1274–1277. [Google Scholar] [CrossRef]
- Topakian, R.; King, A.; Kwon, S.; Schaafsma, A.; Shipley, M.; Markus, H.; Investigators, A. Ultrasonic plaque echolucency and emboli signals predict stroke in asymptomatic carotid stenosis. Neurology 2011, 77, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.; Wang, L.; Zhong, X.; Zhong, L.; Chen, R.; Li, L.; Mao, M. Age and gender differences between carotid intima-media thickness and serum uric acid. Am. J. Cardiol. 2022, 172, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Recio-Rodriguez, J.I.; Gomez-Marcos, M.A.; Patino-Alonso, M.C.; Agudo-Conde, C.; Rodriguez-Sanchez, E.; Garcia-Ortiz, L.; Group, V. Abdominal obesity vs general obesity for identifying arterial stiffness, subclinical atherosclerosis and wave reflection in healthy, diabetics and hypertensive. BMC Cardiovasc. Disord. 2012, 12, 3. [Google Scholar] [CrossRef] [Green Version]
- Oikonen, M.; Wendelin-Saarenhovi, M.; Lyytikäinen, L.P.; Siitonen, N.; Loo, B.M.; Jula, A.; Seppälä, I.; Saarikoski, L.; Lehtimäki, T.; Hutri-Kähönen, N.; et al. Associations between serum uric acid and markers of subclinical atherosclerosis in young adults. The cardiovascular risk in Young Finns study. Atherosclerosis 2012, 223, 497–503. [Google Scholar] [CrossRef]
- Ishizaka, N.; Ishizaka, Y.; Toda, E.-I.; Nagai, R.; Yamakado, M. Association between serum uric acid, metabolic syndrome, and carotid atherosclerosis in Japanese individuals. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1038–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugiura, T.; Dohi, Y.; Takagi, Y.; Yokochi, T.; Yoshikane, N.; Suzuki, K.; Tomiishi, T.; Nagami, T.; Iwase, M.; Takase, H. Increased impact of serum uric acid on arterial stiffness and atherosclerosis in females. J. Atheroscler. Thromb. 2022, 29, 1672–1691. [Google Scholar] [CrossRef]
- Nardi, V.; Franchi, F.; Prasad, M.; Fatica, E.M.; Alexander, M.P.; Bois, M.C.; Lam, J.; Singh, R.J.; Meyer, F.B.; Lanzino, G. Uric acid expression in carotid atherosclerotic plaque and serum uric acid are associated with cerebrovascular events. Hypertension 2022, 79, 1814–1823. [Google Scholar] [CrossRef]
- Puddu, P.; Puddu, G.M.; Cravero, E.; Vizioli, L.; Muscari, A. The relationships among hyperuricemia, endothelial dysfunction, and cardiovascular diseases: Molecular mechanisms and clinical implications. J. Cardiol. 2012, 59, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Gherghina, M.-E.; Peride, I.; Tiglis, M.; Neagu, T.P.; Niculae, A.; Checherita, I.A. Uric Acid and Oxidative Stress—Relationship with Cardiovascular, Metabolic, and Renal Impairment. Int. J. Mol. Sci. 2022, 23, 3188. [Google Scholar] [CrossRef]
- Feig, D.I.; Kang, D.-H.; Johnson, R.J. Uric acid and cardiovascular risk. N. Engl. J. Med. 2008, 359, 1811–1821. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pujia, R.; Tarsitano, M.G.; Arturi, F.; De Lorenzo, A.; Lenzi, A.; Pujia, A.; Montalcini, T. Advances in phenotyping obesity and in its dietary and pharmacological treatment: A narrative review. Front. Nutr. 2022, 9, 804719. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Non-Obese (n = 686) | General Obesity (n = 59) | Central Obesity (n = 616) | Mixed Obesity (n = 715) | p-Value |
|---|---|---|---|---|---|
| Age, mean ± SD | 42.8 ± 13.3 | 51.5 ± 10.4 | 48.9 ± 13.0 | 52.4 ± 10.9 | <0.001 a |
| Sex (female/male), n (%) | 602 (88)/84 (12) | 58 (98)/1 (2) | 169 (27)/447 (73) | 478 (67)/237 (33) | <0.001 b |
| Systolic BP, mean ± SD, mmHg | 125.8 ± 17.2 | 139.1 ± 19.1 | 137.0 ± 20.2 | 145.7 ± 21.3 | <0.001 c |
| Diastolic BP, mean ± SD, mmHg | 79.0 ± 10.0 | 84.5 ± 10.2 | 83.5 ± 10.6 | 88.3 ± 10.8 | <0.001 c |
| BMI, mean ± SD, kg/m2 | 23.8 ± 3.0 | 31.9 ± 1.7 | 26.3 ± 2.4 | 34.9 ± 4.1 | NA |
| Abdominal circumference, mean ± SD, cm | 80.9 ± 7.8 | 89.1 ± 5.8 | 96.1 ± 7.9 | 109.6 ± 9.5 | NA |
| Arterial hypertension, n (%) | 113 (16) | 26 (44) | 164 (27) | 373 (52) | <0.001 b |
| Diabetes mellitus, n (%) | 12 (7) | 5 (8) | 25 (4) | 80 (11) | <0.001 b |
| Dyslipidemia, n (%) | 377 (55) | 45 (76) | 411 (66) | 544 (76) | <0.001 b |
| Smoking, n (%) | 49 (7) | 1 (2) | 159 (25) | 60 (8) | <0.001 b |
| Serum urate, mean ± SD, μmol/L | 234.2 ± 59.8 | 272.9 ± 61.8 | 301.2 ± 73.1 | 309.4 ± 82.2 | <0.001 d |
| Increased serum urate, n (%) | 12 (2) | 6 (10) | 48 (8) | 126 (17) | <0.001 b |
| FBG, mean ± SD, mmol/L | 4.7 ± 0.7 | 4.8 ± 0.6 | 5.0 ± 1.2 | 5.5 ± 1.8 | <0.001 d |
| Creatinine, mean ± SD, mmol/L | 68.6 ± 14.4 | 72.9 ± 10.8 | 76.5 ± 16.5 | 73.4 ± 16.1 | <0.01 e |
| Triglycerides, mean ± SD, mmol/L | 1.0 ± 0.6 | 1.4 ± 0.6 | 1.3 ± 0.7 | 1.5 ± 0.9 | <0.001 e |
| Total-C, mean ± SD, mmol/L | 5.0 ± 0.9 | 5.4 ± 1.0 | 5.3 ± 1.1 | 5.5 ± 1.0 | <0.001 e |
| LDL-C, mean ± SD, mmol/L | 3.1 ± 0.9 | 3.5 ± 1.1 | 3.7 ± 0.9 | 3.7 ± 0.9 | <0.001 e |
| HDL-C, mean ± SD, mmol/L | 1.6 ± 0.4 | 1.5 ± 0.4 | 1.4 ± 0.4 | 1.3 ± 0.3 | <0.001 e |
| Concomitant medication (aspirin), n (%) | 54 (8) | 16 (27) | 93 (15) | 227 (32) | <0.001 b |
| Parameter | Non-Obese (n = 686) | General Obesity (n = 59) | Central Obesity (n = 616) | Mixed Obesity (n = 715) | p-Value |
|---|---|---|---|---|---|
| IMT, mean ± SD, mm | 0.57 ± 0.13 | 0.62 ± 0.14 | 0.67 ± 0.16 | 0.68 ± 0.16 | <0.001 a |
| Increased IMT, n (%) | 17 (2) | 6 (10) | 44 (7) | 70 (10) | <0.001 b |
| Presence of plaques, n (%) | 76 (11) | 15 (25) | 138 (22) | 189 (26) | <0.001 b |
| Number of plaques, mean ± SD | 0.21 ± 0.03 | 0.33 ± 0.11 | 0.45 ± 0.04 | 0.49 ± 0.03 | <0.001 a |
| Area of plaques (mm2), mean ± SD | 4.4 ± 15.7 | 5.6 ± 11.3 | 10.9 ± 27.3 | 11.0 ± 24.5 | <0.001 a |
| Type of plaques: | 0.77 b | ||||
| vulnerable (types 1, 2) | 29 (38) | 7 (47) | 51 (37) | 79 (42) | |
| stable (types 3, 4, 5) | 47 (62) | 8 (53) | 87 (63) | 110 (58) |
| Subject Group | OR | 95% CI | p-Value |
|---|---|---|---|
| Presence of increased IMT a | |||
| Non-obese | 0.992 | 0.985–1.001 | 0.06 |
| General obesity | 1.001 | 0.987–1.015 | 0.91 |
| Central obesity | 1.027 | 1.021–1.038 | <0.01 |
| Mixed obesity | 1.001 | 0.984–1.019 | 0.89 |
| Presence of carotid plaques a | |||
| Non-obese | 0.992 | 0.988–0.996 | <0.001 |
| General obesity | 1.002 | 0.992–1.011 | 0.74 |
| Central obesity | 1.005 | 0.993–1.009 | 0.70 |
| Mixed obesity | 1.008 | 0.996–1.014 | 0.88 |
| Presence of vulnerable carotid plaques a | |||
| Non-obese | 1.001 | 0.978–1.063 | 0.71 |
| General obesity | 1.004 | 0.995–1.015 | 0.90 |
| Central obesity | 0.997 | 0.990–1.005 | 0.11 |
| Mixed obesity | 0.999 | 0.997–1.001 | 0.41 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Efremova, D.; Ciobanu, N.; Glavan, D.; Leahu, P.; Racila, R.; Bălănuță, T.; Matei, A.; Vasilieva, M.; Cheptea, C.; Bîtcă, P.; et al. Serum Urate Levels and Ultrasound Characteristics of Carotid Atherosclerosis across Obesity Phenotypes. Biomedicines 2023, 11, 1897. https://doi.org/10.3390/biomedicines11071897
Efremova D, Ciobanu N, Glavan D, Leahu P, Racila R, Bălănuță T, Matei A, Vasilieva M, Cheptea C, Bîtcă P, et al. Serum Urate Levels and Ultrasound Characteristics of Carotid Atherosclerosis across Obesity Phenotypes. Biomedicines. 2023; 11(7):1897. https://doi.org/10.3390/biomedicines11071897
Chicago/Turabian StyleEfremova, Daniela, Natalia Ciobanu, Danu Glavan, Pavel Leahu, Renata Racila, Tatiana Bălănuță, Alexandru Matei, Maria Vasilieva, Cristina Cheptea, Paula Bîtcă, and et al. 2023. "Serum Urate Levels and Ultrasound Characteristics of Carotid Atherosclerosis across Obesity Phenotypes" Biomedicines 11, no. 7: 1897. https://doi.org/10.3390/biomedicines11071897
APA StyleEfremova, D., Ciobanu, N., Glavan, D., Leahu, P., Racila, R., Bălănuță, T., Matei, A., Vasilieva, M., Cheptea, C., Bîtcă, P., Damian, C., Bondarciuc, A., Bejenari, I., Cojocaru, A., Manea, D., Ciocanu, M., Zota, E., Ciolac, D., & Groppa, S. A. (2023). Serum Urate Levels and Ultrasound Characteristics of Carotid Atherosclerosis across Obesity Phenotypes. Biomedicines, 11(7), 1897. https://doi.org/10.3390/biomedicines11071897