
Platelet Adhesion Mediated by von Willebrand Factor at High Shear Rates Is Associated with Premature Coronary Artery Disease
 ,
,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Measurement of VWF Plasma Levels
2.3. Blood Sample Collection
2.4. Materials for Platelet Adhesion Measurements
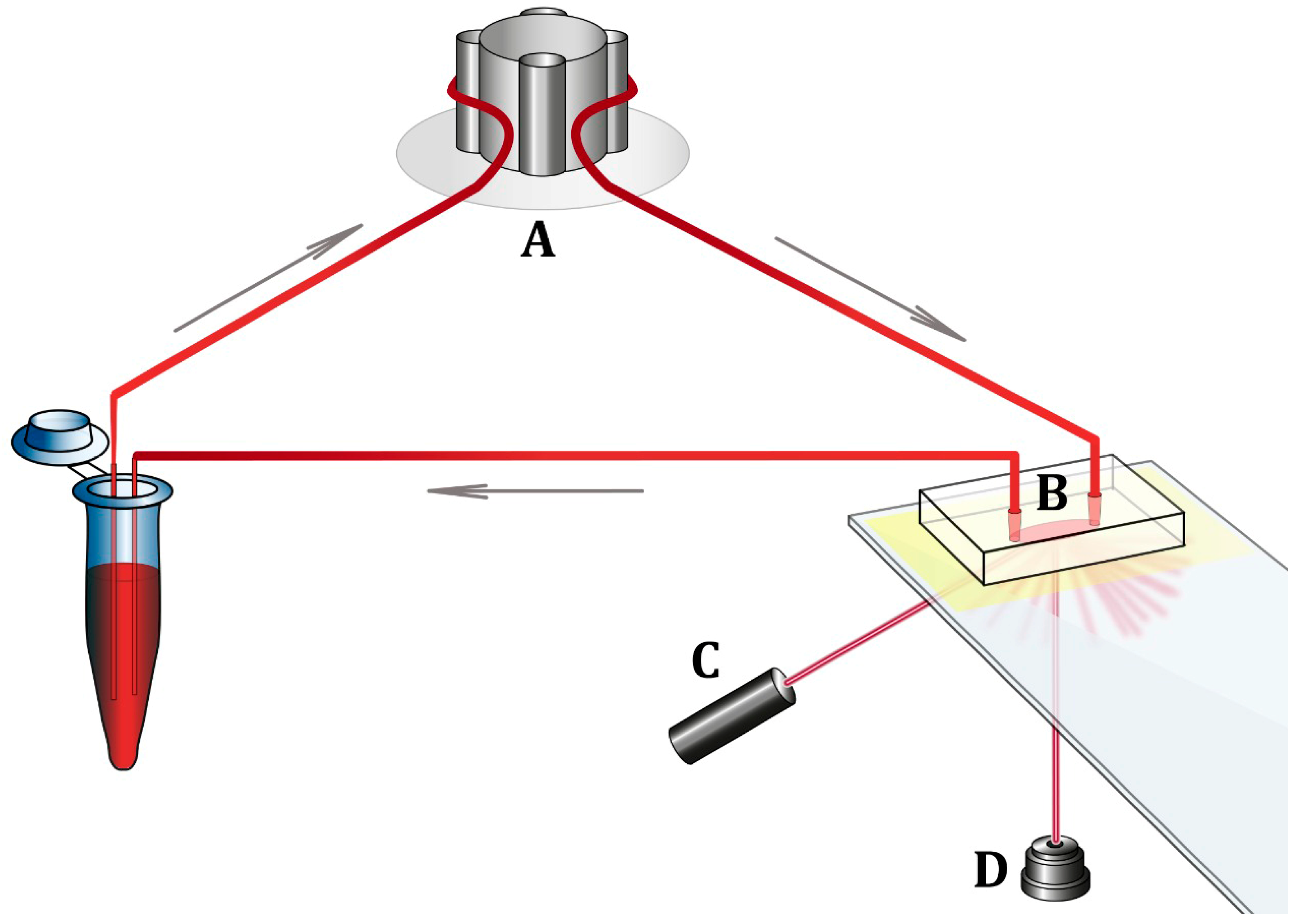
2.5. Measurement of Platelet Adhesion to the Collagen Surface
2.6. Statistical Analysis
2.7. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the Diagnosis and Management of Chronic Coronary Syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [Green Version]
- Casa, L.D.C.; Deaton, D.H.; Ku, D.N. Role of High Shear Rate in Thrombosis. J. Vasc. Surg. 2015, 61, 1068–1080. [Google Scholar] [CrossRef] [Green Version]
- Springer, T.A. Von Willebrand Factor, Jedi Knight of the Bloodstream. Blood 2014, 124, 1412–1425. [Google Scholar] [CrossRef] [Green Version]
- Zeitouni, M.; Clare, R.M.; Chiswell, K.; Abdulrahim, J.; Shah, N.; Pagidipati, N.P.; Shah, S.H.; Roe, M.T.; Patel, M.R.; Jones, W.S. Risk Factor Burden and Long-Term Prognosis of Patients with Premature Coronary Artery Disease. J. Am. Heart Assoc. 2020, 9, e017712. [Google Scholar] [CrossRef]
- Awad-Elkarim, A.A. A Prospective Study of Long Term Prognosis in Young Myocardial Infarction Survivors: The Prognostic Value of Angiography and Exercise Testing. Heart 2003, 89, 843–847. [Google Scholar] [CrossRef]
- Rana, A.; Westein, E.; Niego, B.; Hagemeyer, C.E. Shear-Dependent Platelet Aggregation: Mechanisms and Therapeutic Opportunities. Front. Cardiovasc. Med. 2019, 6, 141. [Google Scholar] [CrossRef]
- Gabbasov, Z.A.; Avtaeva, Y.N.; Melnikov, I.S.; Okhota, S.D.; Caprnda, M.; Mozos, I.; Prosecky, R.; Rodrigo, L.; Kruzliak, P.; Zozulya, N.I. Kinetics of Platelet Adhesion to a Fibrinogen-coated Surface in Whole Blood under Flow Conditions. J. Clin. Lab. Anal. 2021, 35, e23939. [Google Scholar] [CrossRef]
- Neeland, I.J.; Patel, R.S.; Eshtehardi, P.; Dhawan, S.; McDaniel, M.C.; Rab, S.T.; Vaccarino, V.; Zafari, A.M.; Samady, H.; Quyyumi, A.A. Coronary Angiographic Scoring Systems: An Evaluation of Their Equivalence and Validity. Am. Heart J. 2012, 164, 547–552.e1. [Google Scholar] [CrossRef] [Green Version]
- Sakariassen, K.S. Thrombus Formation on Apex of Arterial Stenoses: The Need for a Fluid High Shear Stenosis Diagnostic Device. Future Cardiol. 2007, 3, 193–201. [Google Scholar] [CrossRef]
- Panteleev, M.A.; Korin, N.; Reesink, K.D.; Bark, D.L.; Cosemans, J.M.E.M.; Gardiner, E.E.; Mangin, P.H. Wall Shear Rates in Human and Mouse Arteries: Standardization of Hemodynamics for in Vitro Blood Flow Assays: Communication from the ISTH SSC Subcommittee on Biorheology. J. Thromb. Haemost. 2021, 19, 588–595. [Google Scholar] [CrossRef]
- Borgdorff, P.; Tangelder, G.J.; Paulus, W.J. Cyclooxygenase-2 Inhibitors Enhance Shear Stress-Induced Platelet Aggregation. J. Am. Coll. Cardiol. 2006, 48, 817–823. [Google Scholar] [CrossRef] [Green Version]
- Rutten, B.; Maseri, A.; Cianflone, D.; Laricchia, A.; Cristell, N.; Durante, A.; Spartera, M.; Ancona, F.; Limite, L.; Hu, D.; et al. Plasma Levels of Active Von Willebrand Factor Are Increased in Patients with First ST-Segment Elevation Myocardial Infarction: A Multicenter and Multiethnic Study. Eur. Heart J. Acute Cardiovasc. Care 2015, 4, 64–74. [Google Scholar] [CrossRef]
- Chion, C.K.N.K.; Doggen, C.J.M.; Crawley, J.T.B.; Lane, D.A.; Rosendaal, F.R. ADAMTS13 and von Willebrand Factor and the Risk of Myocardial Infarction in Men. Blood 2007, 109, 1998–2000. [Google Scholar] [CrossRef] [Green Version]
- Willeit, P.; Thompson, A.; Aspelund, T.; Rumley, A.; Eiriksdottir, G.; Lowe, G.; Gudnason, V.; Di Angelantonio, E. Hemostatic Factors and Risk of Coronary Heart Disease in General Populations: New Prospective Study and Updated Meta-Analyses. PLoS ONE 2013, 8, e55175. [Google Scholar] [CrossRef] [Green Version]
- Ray, K.K.; Morrow, D.A.; Gibson, C.M.; Murphy, S.; Antman, E.M.; Braunwald, E. Predictors of the Rise in VWF after ST Elevation Myocardial Infarction: Implications for Treatment Strategies and Clinical Outcome. Eur. Heart J. 2005, 26, 440–446. [Google Scholar] [CrossRef]
- Jansson, J.H.; Nilsson, T.K.; Johnson, O. Von Willebrand Factor in Plasma: A Novel Risk Factor for Recurrent Myocardial Infarction and Death. Heart 1991, 66, 351–355. [Google Scholar] [CrossRef]
- Rumley, A.; Lowe, G.D.; Sweetnam, P.M.; Yarnell, J.W.; Ford, R.P. Factor VIII, von Willebrand Factor and the Risk of Major Ischaemic Heart Disease in the Caerphilly Heart Study. Br. J. Haematol. 1999, 105, 110–116. [Google Scholar] [CrossRef]
- Thompson, S.G.; Kienast, J.; Pyke, S.D.M.; Haverkate, F.; van de Loo, J.C.W. Hemostatic Factors and the Risk of Myocardial Infarction or Sudden Death in Patients with Angina Pectoris. N. Engl. J. Med. 1995, 332, 635–641. [Google Scholar] [CrossRef]
- Vischer, U.M. Von Willebrand Factor, Endothelial Dysfunction, and Cardiovascular Disease. J. Thromb. Haemost. 2006, 4, 1186–1193. [Google Scholar] [CrossRef]
- Roberts, J.C.; Flood, V.H. Laboratory Diagnosis of von Willebrand Disease. Int. J. Lab. Hematol. 2015, 37, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Xu, A.-G.; Xu, R.-M.; Lu, C.-Q.; Yao, M.-Y.; Zhao, W.; Fu, X.; Guo, J.; Xu, Q.-F.; Li, D.-D. Correlation of von Willebrand Factor Gene Polymorphism and Coronary Heart Disease. Mol. Med. Rep. 2012, 6, 1107–1110. [Google Scholar] [CrossRef] [Green Version]
- Gonzales, J.U.; Thistlethwaite, J.R.; Thompson, B.C.; Scheuermann, B.W. Exercise-Induced Shear Stress Is Associated with Changes in Plasma von Willebrand Factor in Older Humans. Eur. J. Appl. Physiol. 2009, 106, 779–784. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with Premature CAD (n = 84) | Control Group (n = 64) | p | |
|---|---|---|---|
| Age, years | 54 (49; 55) | 50.5 (44.5; 58) | 0.19 |
| Men/women | 61 (73%)/ 23 (27%) | 26 (42%)/ 38 (58%) | <0.001 |
| Family history of CAD | 23 (28%) | 10 (16%) | 0.11 |
| LDL cholesterol >3 mmol/L | 64 (76%) | 40 (62%) | 0.004 |
| HDL cholesterol <1.0 mmol/L for men and <1.2 mmol/L for women | 41 (50%) | 14 (25%) | 0.004 |
| Smoking Active smoker Former smoker Smoking index Heavy smoker | 53 (63%) 33 (62%) 20 (38%) 33 (25; 44) 38 (72%) | 24 (38%) 14 (58%) 10 (42%) 17 (8; 22) 5 (21%) | 0.003 0.03 0.3 <0.001 <0.001 |
| Obesity | 44 (52%) | 26 (41%) | 0.31 |
| Diabetes mellitus | 18 (21%) | 5 (8%) | 0.03 |
| Arterial hypertension | 75 (89%) | 52 (81%) | 0.23 |
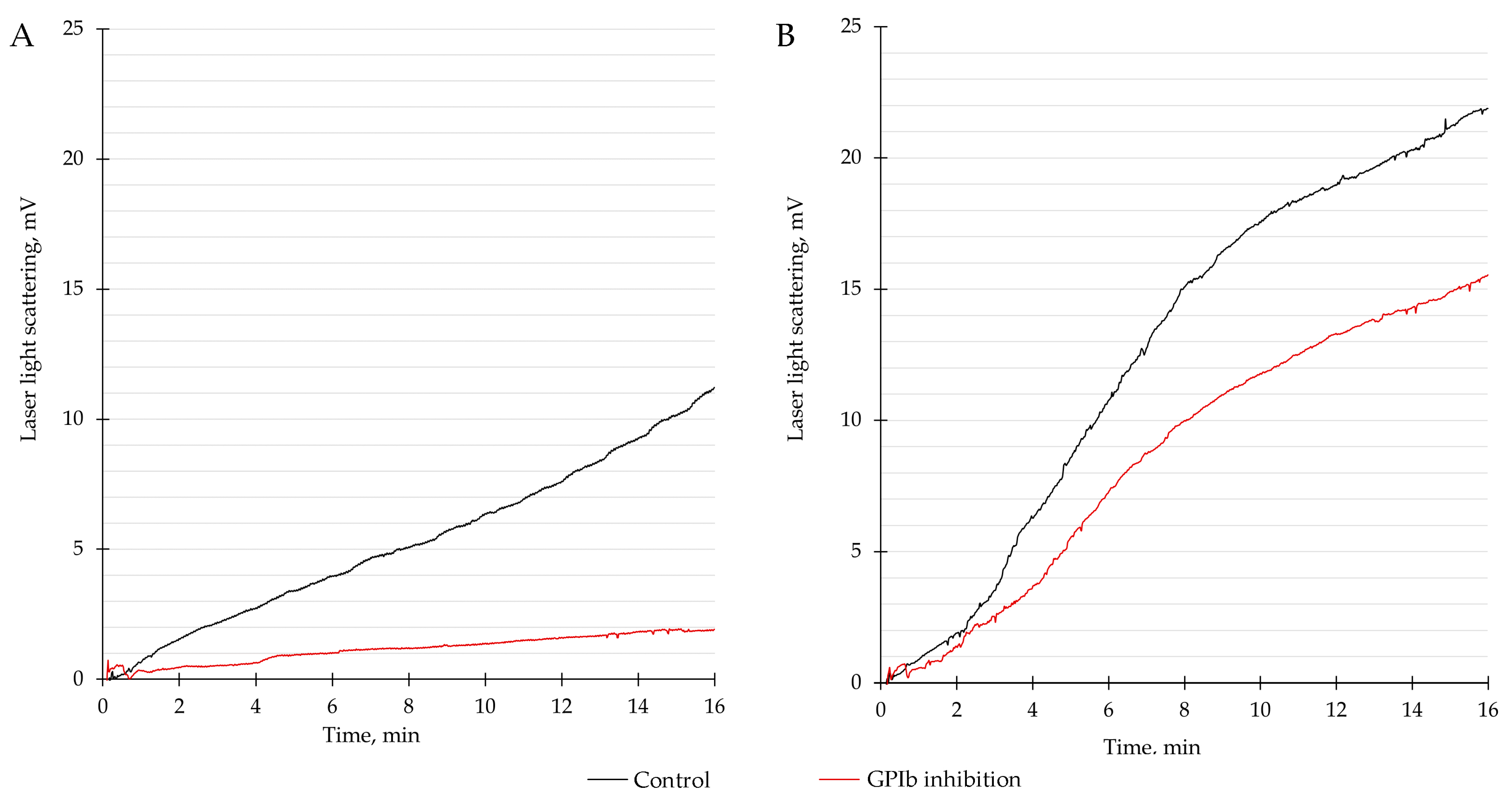
| Platelet Adhesion at Baseline, mV | Platelet Adhesion after GPIb Inhibition, mV | Relative Decrease in Platelet Adhesion after GPIb Inhibition (Δ), % | p | |
|---|---|---|---|---|
| Patients with premature CAD (n = 84) | 8.3 (5.2; 13.5) | 1.7 (1.3; 3.3) | 77.0 (57.2; 84.6) | <0.001 |
| Control group (n = 64) | 12.6 (9.2; 17.0) | 10.3 (4.3; 14.9) | 29.6 (0.0; 59.7) | <0.001 |
| Coefficient (β) | OR (95% CI) | p | |
|---|---|---|---|
| A relative decrease in platelet adhesion after GPIb receptor inhibition, per 1% | 0.41 | 1.04 (1.03–1.06) | <0.001 |
| Male sex | 1.36 | 3.88 (1.94–7.74) | <0.001 |
| Diabetes mellitus | 1.17 | 3.22 (1.13–9.21) | 0.029 |
| HDL cholesterol <1.0 mmol/L for men and <1.2 mmol/L for women | 1.10 | 3.00 (1.43–6.31) | 0.004 |
| Smoking | 1.05 | 2.85 (1.45– 5.58) | 0.002 |
| Age | 0.04 | 1.04 (1.00– 1.08) | 0.045 |
| Family history of CAD | 0.73 | 2.07 (0.90– 4.74) | 0.085 |
| Arterial hypertension | 0.65 | 1.92 (0.76– 4.89) | 0.170 |
| LDL cholesterol >3 mmol/L | 0.44 | 1.55 (0.76–3.18) | 0.230 |
| Obesity | 0.39 | 1.48 (0.76–2.88) | 0.247 |
| Coefficient (β) | aOR (95% CI) | p | |
|---|---|---|---|
| A relative decrease in platelet adhesion after GPIb receptor inhibition, per 1% | 0.03 | 1.03 (1.02–1.05) | <0.001 |
| Male sex | 1.09 | 2.98 (1.13–7.89) | 0.03 |
| Age | 0.10 | 1.11 (1.04–1.18) | 0.001 |
| Smoking | 0.97 | 2.64 (1.09–6.36) | 0.03 |
| Intercept | −5.6 | 0.004 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okhota, S.; Kozlov, S.; Avtaeva, Y.; Melnikov, I.; Saburova, O.; Guria, K.; Matroze, E.; Gabbasov, Z. Platelet Adhesion Mediated by von Willebrand Factor at High Shear Rates Is Associated with Premature Coronary Artery Disease. Biomedicines 2023, 11, 1916. https://doi.org/10.3390/biomedicines11071916
Okhota S, Kozlov S, Avtaeva Y, Melnikov I, Saburova O, Guria K, Matroze E, Gabbasov Z. Platelet Adhesion Mediated by von Willebrand Factor at High Shear Rates Is Associated with Premature Coronary Artery Disease. Biomedicines. 2023; 11(7):1916. https://doi.org/10.3390/biomedicines11071916
Chicago/Turabian StyleOkhota, Sergey, Sergey Kozlov, Yuliya Avtaeva, Ivan Melnikov, Olga Saburova, Konstantin Guria, Evgeny Matroze, and Zufar Gabbasov. 2023. "Platelet Adhesion Mediated by von Willebrand Factor at High Shear Rates Is Associated with Premature Coronary Artery Disease" Biomedicines 11, no. 7: 1916. https://doi.org/10.3390/biomedicines11071916
APA StyleOkhota, S., Kozlov, S., Avtaeva, Y., Melnikov, I., Saburova, O., Guria, K., Matroze, E., & Gabbasov, Z. (2023). Platelet Adhesion Mediated by von Willebrand Factor at High Shear Rates Is Associated with Premature Coronary Artery Disease. Biomedicines, 11(7), 1916. https://doi.org/10.3390/biomedicines11071916