
A Pharmacovigilance Study on the Safety of Axicabtagene Ciloleucel Based on Spontaneous Reports from the EudraVigilance Database

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. ICSRs Selection
2.3. Descriptive Analysis
2.4. Disproportionality Analysis
2.5. Ethical Consideration
3. Results
3.1. Demography and General Characteristics of the ICSRs with Axi-cel as Suspected Drug
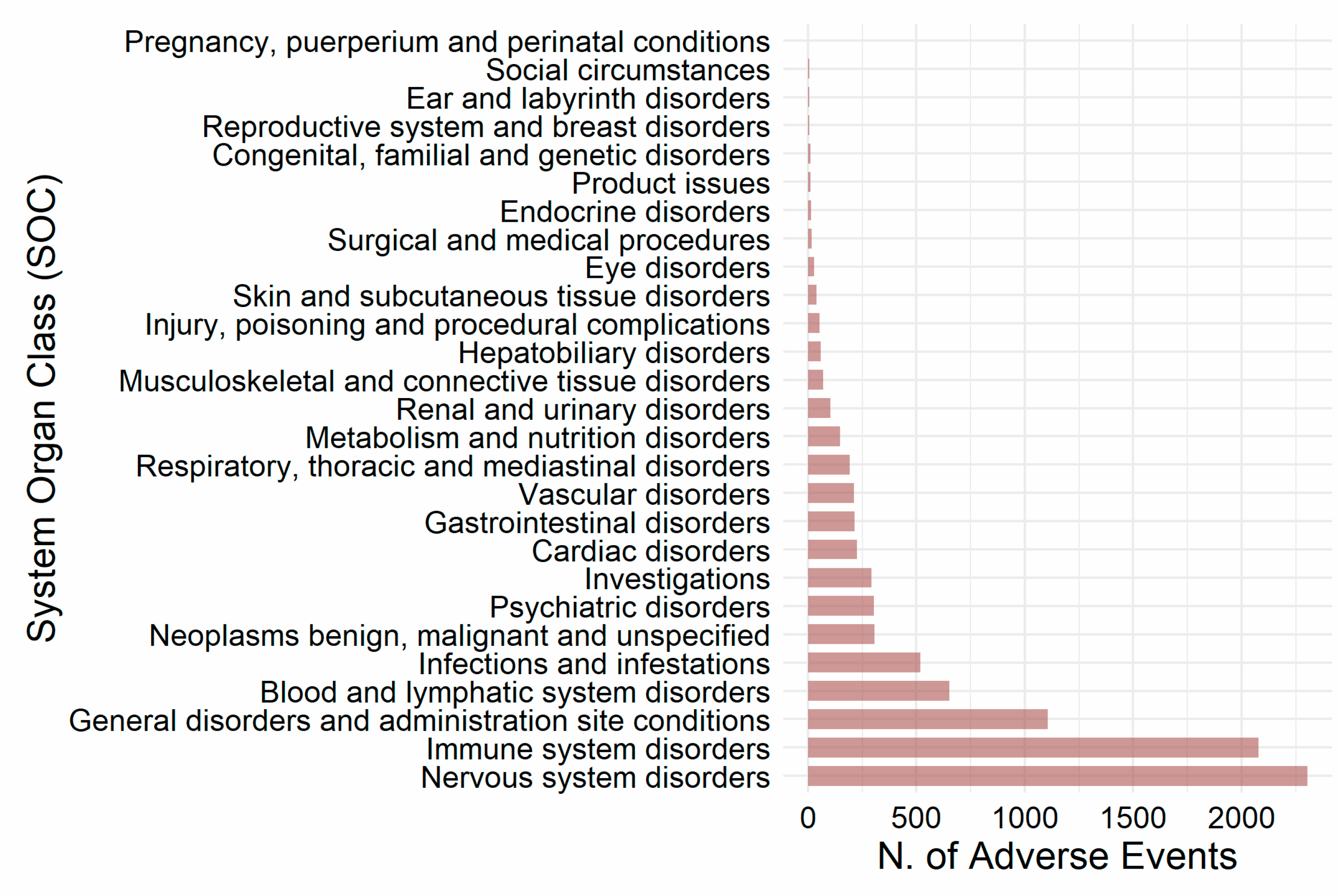
3.2. Reported Suspected Adverse Reactions
3.3. Concomitant Medicinal Products
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- El-Kadiry, A.E.; Rafei, M.; Shammaa, R. Cell Therapy: Types, Regulation, and Clinical Benefits. Front. Med. 2021, 8, 756029. [Google Scholar] [CrossRef] [PubMed]
- Sterner, R.C.; Sterner, R.M. CAR-T cell therapy: Current limitations and potential strategies. Blood Cancer J. 2021, 11, 69. [Google Scholar] [CrossRef] [PubMed]
- Brentjens, R.J.; Curran, K.J. Novel cellular therapies for leukemia: CAR-modified T cells targeted to the CD19 antigen. Hematol. Am. Soc. Hematol. Educ. Program 2012, 2012, 143–151. [Google Scholar] [CrossRef] [Green Version]
- Campbell, A.; Brieva, T.; Raviv, L.; Rowley, J.; Niss, K.; Brandwein, H.; Oh, S.; Karnieli, O. Concise Review: Process Development Considerations for Cell Therapy. Stem Cells Transl. Med. 2015, 4, 1155–1163. [Google Scholar] [CrossRef]
- Regulation (EC) No 1394/2007 of the European Parliament and of the Council of 13 November 2007 on Advanced Therapy Medicinal Products and Amending Directive 2001/83/EC and Regulation (EC) No 726/2004. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2007:324:0121:0137:en:PDF (accessed on 27 December 2002).
- EMA-Committee for Medicinal Products for Human Use (CHMP). Guideline on Safety and Efficacy Follow-Up and Risk Management of Advanced Therapy Medicinal Products. 25 January 2018 EMEA/149995/2008 rev.1 3. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/draft-guideline-safety-efficacy-follow-risk-management-advanced-therapy-medicinal-products-revision_en.pdf (accessed on 27 December 2022).
- Locke, F.L.; Go, W.Y.; Neelapu, S.S. Development and Use of the Anti-CD19 Chimeric Antigen Receptor T-Cell Therapy Axicabtagene Ciloleucel in Large B-Cell Lymphoma: A Review. JAMA Oncol. 2020, 6, 281–290. [Google Scholar] [CrossRef]
- Shah, N.; Chari, A.; Scott, E.; Mezzi, K.; Usmani, S.Z. B-cell maturation antigen (BCMA) in multiple myeloma: Rationale for targeting and current therapeutic approaches. Leukemia 2020, 34, 985–1005. [Google Scholar] [CrossRef] [Green Version]
- Jacobson, C.A.; Farooq, U.; Ghobadi, A. Axicabtagene Ciloleucel, an Anti-CD19 Chimeric Antigen Receptor T-Cell Therapy for Relapsed or Refractory Large B-Cell Lymphoma: Practical Implications for the Community Oncologist. Oncologist 2020, 25, e138–e146. [Google Scholar] [CrossRef] [Green Version]
- Locke, F.L.; Neelapu, S.S.; Bartlett, N.L.; Siddiqi, T.; Chavez, J.C.; Hosing, C.M.; Ghobadi, A.; Budde, L.E.; Bot, A.; Rossi, J.M.; et al. Phase 1 Results of ZUMA-1: A Multicenter Study of KTE-C19 Anti-CD19 CAR T Cell Therapy in Refractory Aggressive Lymphoma. Mol. Ther. 2017, 25, 285–295. [Google Scholar] [CrossRef] [Green Version]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y.; et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N. Engl. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef]
- Jacobson, C.A.; Chavez, J.C.; Sehgal, A.R.; William, B.M.; Munoz, J.; Salles, G.; Munshi, P.N.; Casulo, C.; Maloney, D.G.; de Vos, S.; et al. Axicabtagene ciloleucel in relapsed or refractory indolent non-Hodgkin lymphoma (ZUMA-5): A single-arm, multicentre, phase 2 trial. Lancet Oncol. 2022, 23, 91–103. [Google Scholar] [CrossRef]
- Locke, F.L.; Miklos, D.B.; Jacobson, C.A.; Perales, M.A.; Kersten, M.J.; Oluwole, O.O.; Ghobadi, A.; Rapoport, A.P.; McGuirk, J.; Pagel, J.M.; et al. Axicabtagene Ciloleucel as Second-Line Therapy for Large B-Cell Lymphoma. N. Engl. J. Med. 2022, 386, 640–654. [Google Scholar] [CrossRef]
- EMA. Summary of Product Characteristics for Yescarta (Axicabtagene Ciloleucel). Available online: https://www.ema.europa.eu/en/documents/product-information/yescarta-epar-product-information_en.pdf (accessed on 10 April 2023).
- Lee, D.W.; Santomasso, B.D.; Locke, F.L.; Ghobadi, A.; Turtle, C.J.; Brudno, J.N.; Maus, M.V.; Park, J.H.; Mead, E.; Pavletic, S.; et al. ASTCT Consensus Grading for Cytokine Release Syndrome and Neurologic Toxicity Associated with Immune Effector Cells. Biol. Blood Marrow Transplant. 2019, 25, 625–638. [Google Scholar] [CrossRef] [Green Version]
- Miao, L.; Zhang, Z.; Ren, Z.; Li, Y. Reactions Related to CAR-T Cell Therapy. Front. Immunol. 2021, 12, 663201. [Google Scholar] [CrossRef]
- Xiao, X.; Huang, S.; Chen, S.; Wang, Y.; Sun, Q.; Xu, X.; Li, Y. Mechanisms of cytokine release syndrome and neurotoxicity of CAR T-cell therapy and associated prevention and management strategies. J. Exp. Clin. Cancer Res. 2021, 40, 367. [Google Scholar] [CrossRef]
- Santomasso, B.D.; Nastoupil, L.J.; Adkins, S.; Lacchetti, C.; Schneider, B.J.; Anadkat, M.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; et al. Management of Immune-Related Adverse Events in Patients Treated With Chimeric Antigen Receptor T-Cell Therapy: ASCO Guideline J. Clin. Oncol. 2021, 39, 3978–3992. [Google Scholar] [CrossRef]
- Gust, J.; Hay, K.A.; Hanafi, L.A.; Li, D.; Myerson, D.; Gonzalez-Cuyar, L.F.; Yeung, C.; Liles, W.C.; Wurfel, M.; Lopez, J.A.; et al. Endothelial activation and blood-brain barrier disruption in neurotoxicity after adoptive immunotherapy with CD19 CAR-T cells. Cancer Discov. 2017, 7, 1404–1419. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.; Reagan, P.M.; Liesveld, J.L. Cytopenia after CAR-T Cell Therapy—A Brief Review of a Complex Problem. Cancers 2022, 14, 1501. [Google Scholar] [CrossRef]
- Si, X.; Gu, T.; Liu, L.; Huang, Y.; Han, Y.; Qian, P.; Huang, H. Hematologic cytopenia post CAR T cell therapy: Etiology, potential mechanisms and perspective. Cancer Lett. 2022, 550, 215920. [Google Scholar] [CrossRef]
- Haidar, G.; Garner, W.; Hill, J.A. Infections after anti-CD19 chimeric antigen receptor T-cell therapy for hematologic malignancies: Timeline, prevention, and uncertainties. Curr. Opin. Infect. Dis. 2020, 33, 449–457. [Google Scholar] [CrossRef]
- Postigo, R.; Brosch, S.; Slattery, J.; van Haren, A.; Dogné, J.M.; Kurz, X.; Candore, G.; Domergue, F.; Arlett, P. EudraVigilance Medicines Safety Database: Publicly Accessible Data for Research and Public Health Protection. Drug Saf. 2018, 41, 665–675. [Google Scholar] [CrossRef] [Green Version]
- EMA. EudraVigilance—European Database of Suspected Adverse Reactions Related to Medicines: User Manual for Online Access via the Adrreports.eu Portal. Available online: https://www.ema.europa.eu/en/documents/regulatory-procedural-guideline/eudravigilance-european-database-suspected-adverse-reactions-related-medicines-user-manual-online_en.pdf (accessed on 13 February 2023).
- Bonaldo, G.; Montanaro, N.; Vaccheri, A.; Motola, D. Safety profile of chimeric antigen receptor T-cell immunotherapies (CAR-T) in clinical practice. Eur. J. Clin. Pharmacol. 2021, 77, 1225–1234. [Google Scholar] [CrossRef] [PubMed]
- Fusaroli, M.; Isgrò, V.; Cutroneo, P.M.; Ferrajolo, C.; Cirillo, V.; Del Bufalo, F.; Raschi, E.; Poluzzi, E.; Trifirò, G. Post-Marketing Surveillance of CAR-T-Cell Therapies: Analysis of the FDA Adverse Event Reporting System (FAERS) Database. Drug Saf. 2022, 45, 891–908. [Google Scholar] [CrossRef] [PubMed]
- Inácio, P.; Cavaco, A.; Airaksinen, M. The value of patient reporting to the pharmacovigilance system: A systematic review. Br. J. Clin. Pharmacol. 2017, 83, 227–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Güner, M.D.; Ekmekci, P.E. Healthcare professionals’ pharmacovigilance knowledge and adverse drug reaction reporting behavior and factors determining the reporting rates. J. Drug Assess. 2019, 8, 13–20. [Google Scholar] [CrossRef]
- Kc, S.; Tragulpiankit, P.; Gorsanan, S.; Edwards, I.R. Attitudes among healthcare professionals to the reporting of adverse drug reactions in Nepal. BMC Pharmacol. Toxicol. 2013, 14, 16. [Google Scholar] [CrossRef] [Green Version]
- Acharya, U.H.; Dhawale, T.; Yun, S.; Jacobson, C.A.; Chavez, J.C.; Ramos, J.D.; Appelbaum, J.; Maloney, D.G. Management of cytokine release syndrome and neurotoxicity in chimeric antigen receptor (CAR) T cell therapy. Expert Rev. Hematol. 2019, 12, 195–205. [Google Scholar] [CrossRef]
- Kotch, C.; Barrett, D.; Teachey, D.T. Tocilizumab for the treatment of chimeric antigen receptor T cell-induced cytokine release syndrome. Expert Rev. Clin. Immunol. 2019, 15, 813–822. [Google Scholar] [CrossRef]
- Sterner, R.C.; Sterner, R.M. Immune effector cell associated neurotoxicity syndrome in chimeric antigen receptor-T cell therapy. Front. Immunol. 2022, 13, 879608. [Google Scholar] [CrossRef]
- Abramson, J.S.; Siddiqi, T.; Palomba, M.L.; Gordon, L.I.; Lunning, M.A.; Arnason, J.E.; Wang, M.; Forero-Torres, A.; Albertson, T.; Dehner, C.; et al. High durable CR rates and preliminary safety profile for JCAR017 in R/R aggressive B-NHL (TRANSCEND NHL 001 study): A defined composition CD19-directed CAR T cell product with potential for outpatient administration. Biol. Blood Marrow Transplant. 2018, 24, S20–S24. [Google Scholar] [CrossRef] [Green Version]
- Locke, F.L.; Ghobadi, A.; Jacobson, C.A.; Miklos, D.B.; Lekakis, L.J.; Oluwole, O.O.; Lin, Y.; Braunschweig, I.; Hill, B.T.; Timmerman, J.; et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): A single-arm, multicentre, phase 1-2 trial. Lancet Oncol. 2019, 20, 31–42. [Google Scholar] [CrossRef]
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; Waller, E.K.; Borchmann, P.; McGuirk, J.P.; Jäger, U.; Jaglowski, S.; Andreadis, C.; Westin, J.R.; et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2019, 380, 45–56. [Google Scholar] [CrossRef]
- EMA. Assessment Report for Breyanzi (Lisocabtagene Maraleucel). Available online: https://www.ema.europa.eu/en/documents/assessment-report/breyanzi-epar-public-assessment-report_en.pdf (accessed on 10 April 2023).
- EMA. Assessment Report for Yescarta (Axicabtagene Ciloleucel). Available online: https://www.ema.europa.eu/en/documents/assessment-report/yescarta-epar-public-assessment-report_en.pdf (accessed on 10 April 2023).
- EMA. Assessment Report for Kymriah (Tisagenlecleucel). Available online: https://www.ema.europa.eu/en/documents/variation-report/kymriah-h-c-4090-ii-56-epar-assessment-report-variation_en.pdf (accessed on 10 April 2023).
- EMA. Assessment Report for Carvykti (Ciltacabtagene Autoleucel). Available online: https://www.ema.europa.eu/en/documents/assessment-report/carvykti-epar-public-assessment-report_en.pdf (accessed on 10 April 2023).
- EMA. Assessment Report for Abecma (Idecabtagene Vicleucel). Available online: https://www.ema.europa.eu/en/documents/assessment-report/abecma-epar-public-assessment-report_en.pdf (accessed on 10 April 2023).
- Parker, K.R.; Migliorini, D.; Perkey, E.; Yost, K.E.; Bhaduri, A.; Bagga, P.; Haris, M.; Wilson, N.E.; Liu, F.; Gabunia, K.; et al. Single-Cell Analyses Identify Brain Mural Cells Expressing CD19 as Potential Off-Tumor Targets for CAR-T Immunotherapies. Cell 2020, 183, 126–142.e17. [Google Scholar] [CrossRef]
- Kawalekar, O.U.; O’Connor, R.S.; Fraietta, J.A.; Guo, L.; McGettigan, S.E.; Posey, A.D., Jr.; Patel, P.R.; Guedan, S.; Scholler, J.; Keith, B.; et al. Distinct Signaling of Coreceptors Regulates Specific Metabolism Pathways and Impacts Memory Development in CAR T Cells. Immunity 2016, 44, 380–90. [Google Scholar] [CrossRef] [Green Version]
- Salter, A.I.; Ivey, R.G.; Kennedy, J.J.; Voillet, V.; Rajan, A.; Alderman, E.J.; Voytovich, U.J.; Lin, C.; Sommermeyer, D.; Liu, L.; et al. Phosphoproteomic analysis of chimeric antigen receptor signaling reveals kinetic and quantitative differences that affect cell function. Sci. Signal. 2018, 11, eaat6753. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, J.C.; Weiss, S.L.; Maude, S.L.; Barrett, D.M.; Lacey, S.F.; Melenhorst, J.J.; Shaw, P.; Berg, R.A.; June, C.H.; Porter, D.L.; et al. Cytokine release syndrome after chimeric antigen receptor T cell therapy for acute lymphoblastic leukemia. Crit. Care Med. 2017, 45, e124–e131. [Google Scholar] [CrossRef]
- Frey, N.; Porter, D. Cytokine Release Syndrome with Chimeric Antigen Receptor T Cell Therapy. Biol. Blood Marrow Transplant. 2019, 25, e123–e127. [Google Scholar] [CrossRef] [Green Version]
- Teachey, D.T.; Lacey, S.F.; Shaw, P.A.; Melenhorst, J.J.; Maude, S.L.; Frey, N.; Pequignot, E.; Gonzalez, V.E.; Chen, F.; Finklestein, J.; et al. Identification of Predictive Biomarkers for Cytokine Release Syndrome after Chimeric Antigen Receptor T-Cell Therapy for Acute Lymphoblastic Leukemia. Cancer Discov. 2016, 6, 664–679. [Google Scholar] [CrossRef] [Green Version]
- Winter, S.F.; Martinez-Lage, M.; Clement, N.F.; Hochberg, E.P.; Dietrich, J. Fatal neurotoxicity after chimeric antigen receptor T-cell therapy: An unexpected case of fludarabine-associated progressive leukoencephalopathy. Eur. J. Cancer 2021, 144, 178–181. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ICSRs n (% of Total) | ||
|---|---|---|
| Gender | Female (%) | 927 (31.9) |
| Male (%) | 1331 (45.8) | |
| Not Reported (%) | 647 (22.3) | |
| TOTAL | 2905 (100.0) | |
| Age | 12–17 Years (%) | 1 (<0.1) |
| 18–64 Years (%) | 1225 (42.1) | |
| 65–85 Years | 657 (22.6) | |
| More than 85 Years | 6 (0.2) | |
| Not Specified | 1016 (35.0) | |
| TOTAL | 2905 (100.0) | |
| Reporter Groups | Health Care Professional | 2803 (96.5) |
| Non-Health Care Professional | 102 (3.5) | |
| TOTAL | 2905 (100.0) | |
| Primary Source Country | Non-EU Economic Area | 1849 (63.6) |
| EU Economic Area | 1056 (36.4) | |
| TOTAL | 2905 (100.0) |
| Therapeutic Indication | ICSRs n (% of Total) |
|---|---|
| Diffuse large B-cell lymphoma | 1369 (46.5) |
| B-cell lymphoma | 272 (9.2) |
| Non-Hodgkin’s lymphoma | 111 (3.8) |
| Primary mediastinal large B-cell lymphoma | 92 (3.1) |
| Lymphoma | 85 (2.9) |
| Follicular lymphoma | 65 (2.2) |
| TOTAL | 2945 (100.0) * |
| AEs n (%) | ||
|---|---|---|
| Seriousness | Serious (%) | 7104 (79.1) |
| Not Serious (%) | 1878 (20.9) | |
| TOTAL | 8982 (100.0%) | |
| Outcome | Recovered/Resolved | 3194 (35.6) |
| Recovering/Resolving | 410 (4.6) | |
| Recovered with Sequelae | 31 (0.3) | |
| Not Recovered/Not Resolved | 852 (9.5) | |
| Fatal | 765 (8.5) | |
| Unknown | 3730 (41.5) | |
| TOTAL | 8982 (100.0%) |
| AEs n (%) | |
|---|---|
| Nervous system disorders | 2304 (100.0) |
| Neurotoxicity | 723 (31.4) |
| ICANS | 616 (26.7) |
| Encephalopathy | 154 (6.7) |
| Tremor | 105 (4.6) |
| Aphasia | 92 (4.0) |
| Headache | 84 (3.6) |
| Somnolence | 53 (2.3) |
| Dysgraphia | 41 (1.8) |
| Seizure | 34 (1.5) |
| Memory impairment | 29 (1.3) |
| Depressed level of consciousness | 23 (1.0) |
| Immune system disorders | 2078 (100.0) |
| Cytokine release syndrome | 1929 (92.8) |
| Hypogammaglobulinemia | 54 (2.6) |
| Hemophagocytic lymphohistiocytosis | 45 (2.2) |
| Cytokine storm | 30 (1.4) |
| General disorders and administration site conditions | 1105 (100.0) |
| Pyrexia | 368 (33.3) |
| Disease progression | 155 (14.0) |
| Death | 141 (12.8) |
| Fatigue | 116 (10.5) |
| Malaise | 36 (3.3) |
| Drug ineffective | 36 (3.3) |
| Chills | 36 (3.3) |
| Disease recurrence | 20 (1.8) |
| Multiple organ dysfunction syndrome | 19 (1.7) |
| Asthenia | 18 (1.6) |
| Gait disturbance | 13 (1.2) |
| Hyperthermia | 12 (1.1) |
| Blood and lymphatic system disorders | 652 (100.0) |
| Neutropenia | 176 (27.0) |
| Pancytopenia | 97 (14.9) |
| Thrombocytopenia | 87 (13.3) |
| Cytopenia | 70 (10.7) |
| Febrile neutropenia | 44 (6.7) |
| Bone marrow failure | 34 (5.2) |
| Anemia | 30 (4.6) |
| Leukopenia | 17 (2.6) |
| Myelosuppression | 14 (2.1) |
| Disseminated intravascular coagulation | 14 (2.1) |
| B-cell aplasia | 14 (2.1) |
| Coagulopathy | 13 (2.0) |
| Lymphopenia | 7 (1.1) |
| Agranulocytosis | 7 (1.1) |
| Infections and infestations | 517 (100.0) |
| Sepsis | 39 (7.5) |
| Septic shock | 36 (7.0) |
| Infection | 35 (6.8) |
| Pneumonia | 32 (6.2) |
| COVID-19 | 24 (4.6) |
| Bacteremia | 17 (3.3) |
| Cytomegalovirus infection reactivation | 11 (2.1) |
| Clostridium difficile colitis | 10 (1.9) |
| Aspergillus infection | 10 (1.9) |
| Urinary tract infection | 9 (1.7) |
| Systemic candida | 9 (1.7) |
| Clostridium difficile infection | 9 (1.7) |
| Systemic mycosis | 7 (1.4) |
| Bronchopulmonary aspergillosis | 7 (1.4) |
| Pneumonia bacterial | 6 (1.2) |
| Human herpesvirus 6 encephalitis | 6 (1.2) |
| BK virus infection | 6 (1.2) |
| Staphylococcal infection | 5 (1.0) |
| Pneumonia fungal | 5 (1.0) |
| Comparisons | ROR | 95% CI | p-Value |
|---|---|---|---|
| axi-cel vs. all | 2.34 | 2.13–2.58 | <<0.05 |
| axi-cel vs. tisa-cel | 3.03 | 2.70–3.39 | <<0.05 |
| axi-cel vs. brexu-cel | 0.91 | 0.77–1.08 | 0.26 |
| axi-cel vs. ide-cel | 2.29 | 1.68–3.19 | <<0.05 |
| axi-cel vs. liso-cel | 1.76 | 1.17–2.74 | <0.05 |
| axi-cel vs. cilta-cel | 3.27 | 1.92–5.99 | <<0.05 |
| 2nd Level ATC Drug Classes | n (%) | |
|---|---|---|
| Antineoplastic agents | (L01) | 1009 (16.4) |
| Antibacterials for systemic use | (J01) | 598 (9.7) |
| Ophthalmic drugs | (S01) | 502 (8.2) |
| Analgesic | (N02) | 309 (5.0) |
| Antiepileptic drugs | (N03) | 306 (5.0) |
| Drugs for acid related disorders | (A02) | 292 (4.7) |
| Psycholeptics | (N05) | 230 (3.7) |
| Blood substitutes and perfusion solutions | (B05) | 196 (3.2) |
| Antithrombotic agents | (B01) | 179 (2.9) |
| Antifungals for dermatological use | (D01) | 171 (2.8) |
| Drugs for constipation | (A06) | 161 (2.6) |
| Antivirals for systemic use | (J05) | 154 (2.5) |
| Musculo-skeletal system | (M04) | 147 (2.4) |
| Antiemetics and antinauseants | (A04) | 128 (2.1) |
| Antihistamines for systemic use | (R06) | 121 (2.0) |
| Corticosteroids, dermatological preparations | (D07) | 117 (1.9) |
| Antimycotics for systemic use | (J02) | 106 (1.7) |
| Beta blocking agents | (C07) | 99 (1.6) |
| Psychoanaleptics | (N06) | 98 (1.6) |
| Drugs used in diabetes | (A10) | 95 (1.5) |
| Immunosuppressants | (L04) | 92 (1.5) |
| Mineral supplements | (A12) | 88 (1.4) |
| Diuretics | (C03) | 70 (1.1) |
| Antineoplastic agents | (L01) | 1009 (16.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rafaniello, C.; Liguori, V.; Zinzi, A.; Gaio, M.; Falco, A.; Di Costanzo, L.; Gargano, F.; Trimarco, V.; Cataldi, M.; Capuano, A. A Pharmacovigilance Study on the Safety of Axicabtagene Ciloleucel Based on Spontaneous Reports from the EudraVigilance Database. Biomedicines 2023, 11, 2162. https://doi.org/10.3390/biomedicines11082162
Rafaniello C, Liguori V, Zinzi A, Gaio M, Falco A, Di Costanzo L, Gargano F, Trimarco V, Cataldi M, Capuano A. A Pharmacovigilance Study on the Safety of Axicabtagene Ciloleucel Based on Spontaneous Reports from the EudraVigilance Database. Biomedicines. 2023; 11(8):2162. https://doi.org/10.3390/biomedicines11082162
Chicago/Turabian StyleRafaniello, Concetta, Valerio Liguori, Alessia Zinzi, Mario Gaio, Angela Falco, Luigi Di Costanzo, Francesca Gargano, Valentina Trimarco, Mauro Cataldi, and Annalisa Capuano. 2023. "A Pharmacovigilance Study on the Safety of Axicabtagene Ciloleucel Based on Spontaneous Reports from the EudraVigilance Database" Biomedicines 11, no. 8: 2162. https://doi.org/10.3390/biomedicines11082162
APA StyleRafaniello, C., Liguori, V., Zinzi, A., Gaio, M., Falco, A., Di Costanzo, L., Gargano, F., Trimarco, V., Cataldi, M., & Capuano, A. (2023). A Pharmacovigilance Study on the Safety of Axicabtagene Ciloleucel Based on Spontaneous Reports from the EudraVigilance Database. Biomedicines, 11(8), 2162. https://doi.org/10.3390/biomedicines11082162