
Prognostic Value of Plasma Biomarkers S100B and Osteopontin in Pediatric TBI: A Prospective Analysis Evaluating Acute and 6-Month Outcomes after Mild to Severe TBI

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
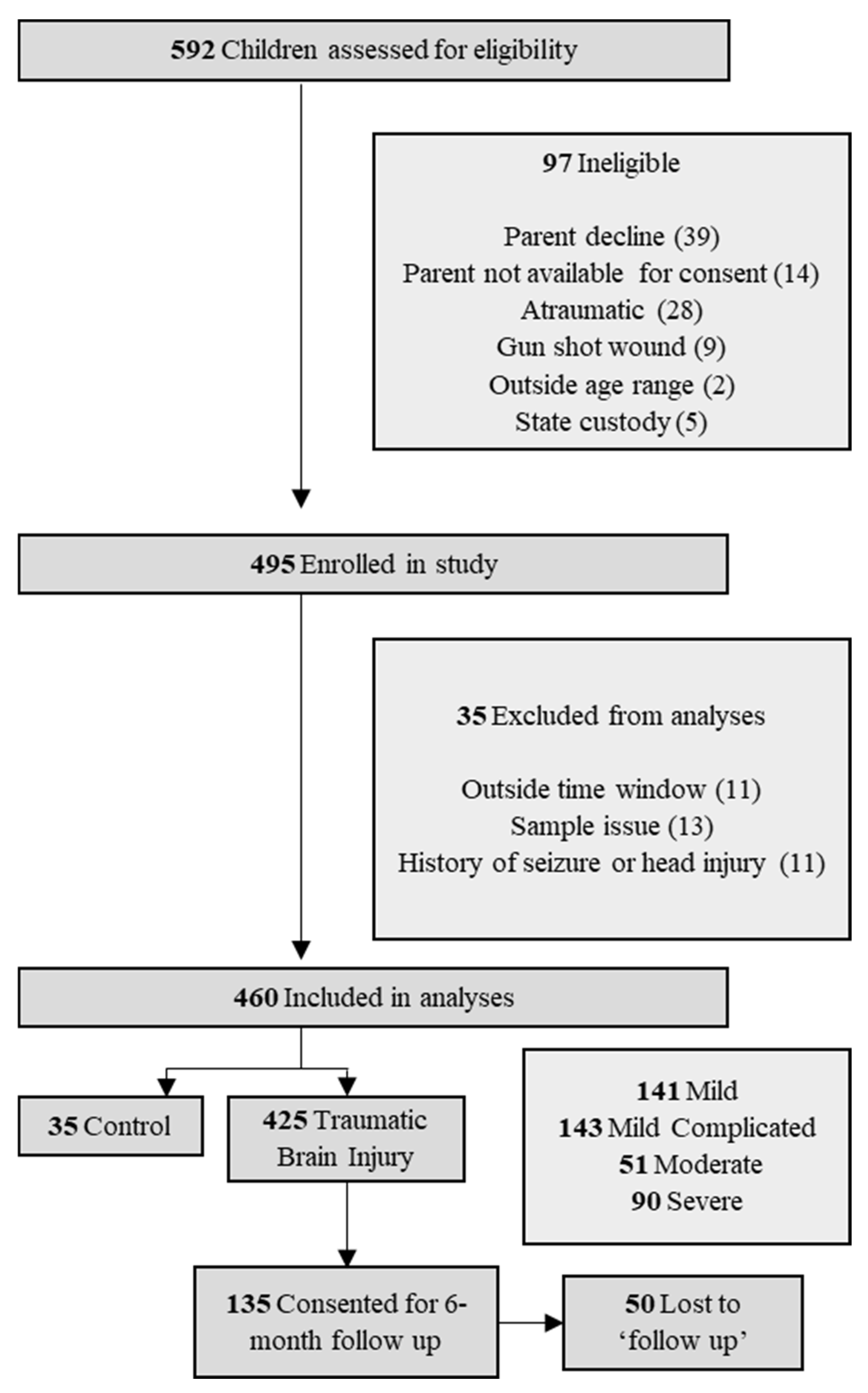
2.1. Participants and Study Design
2.2. Plasma Sample Collection
2.3. Clinical Outcomes
2.4. Statistical Analyses
3. Results
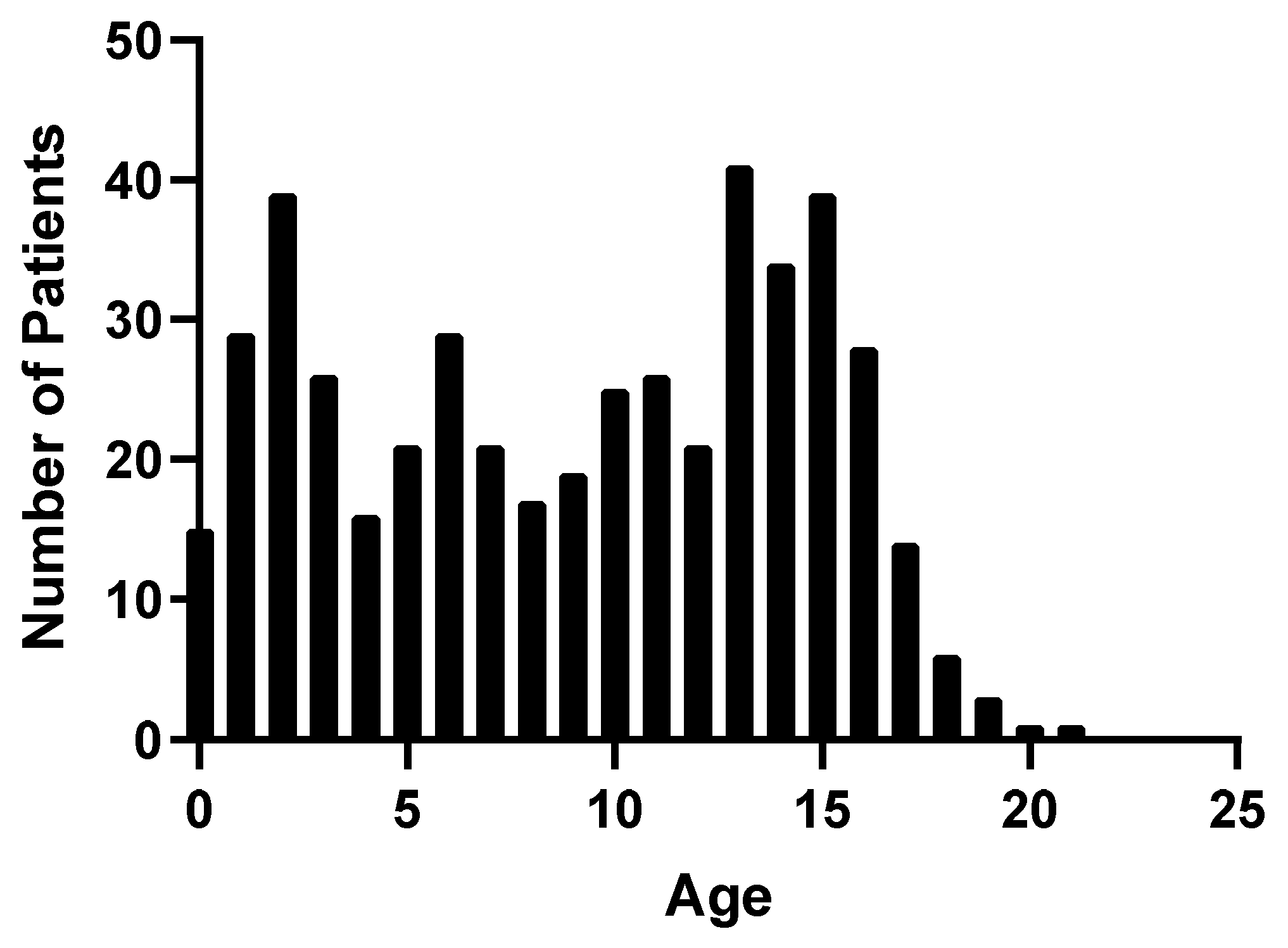
3.1. Patient Demographics
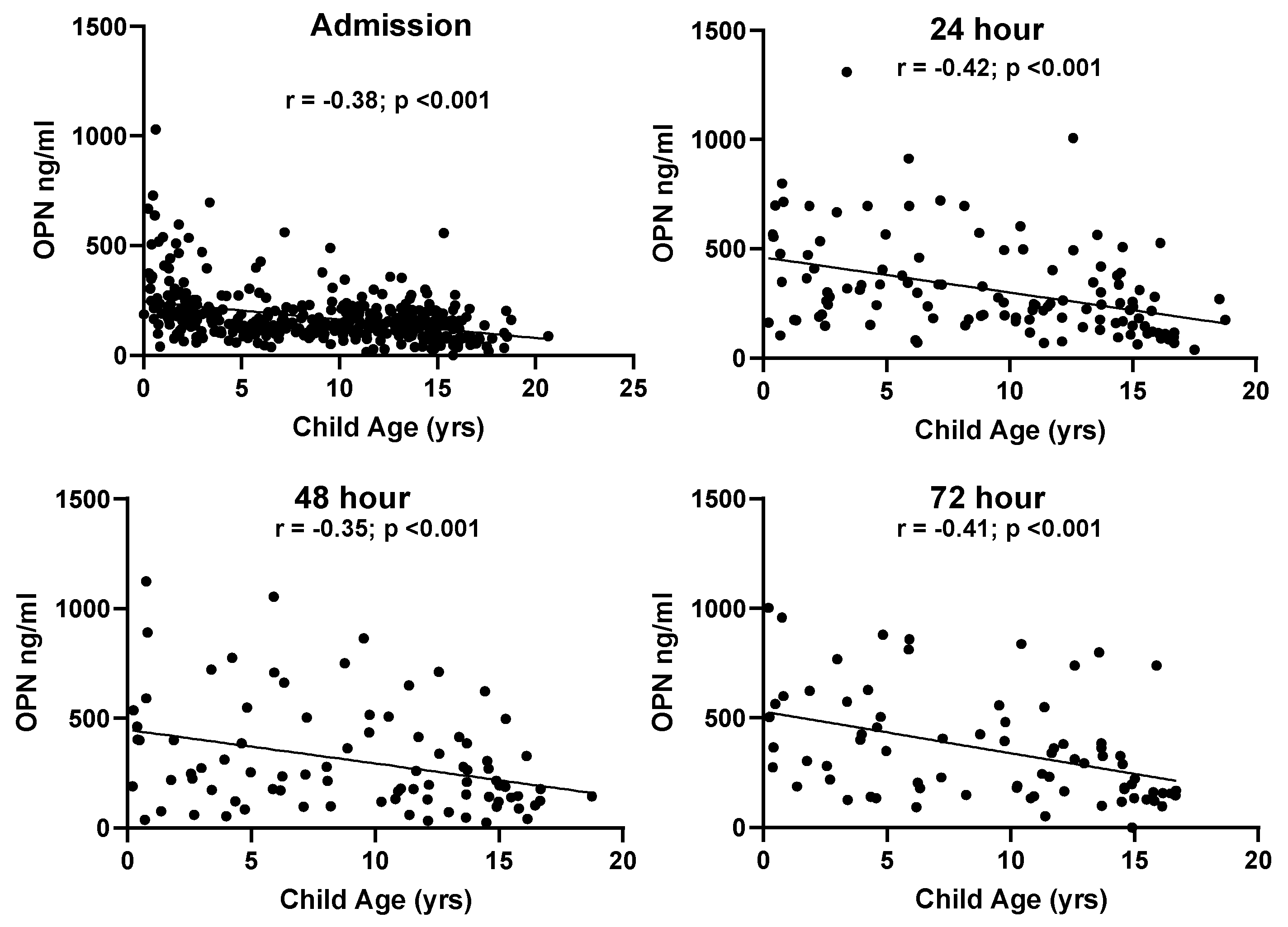
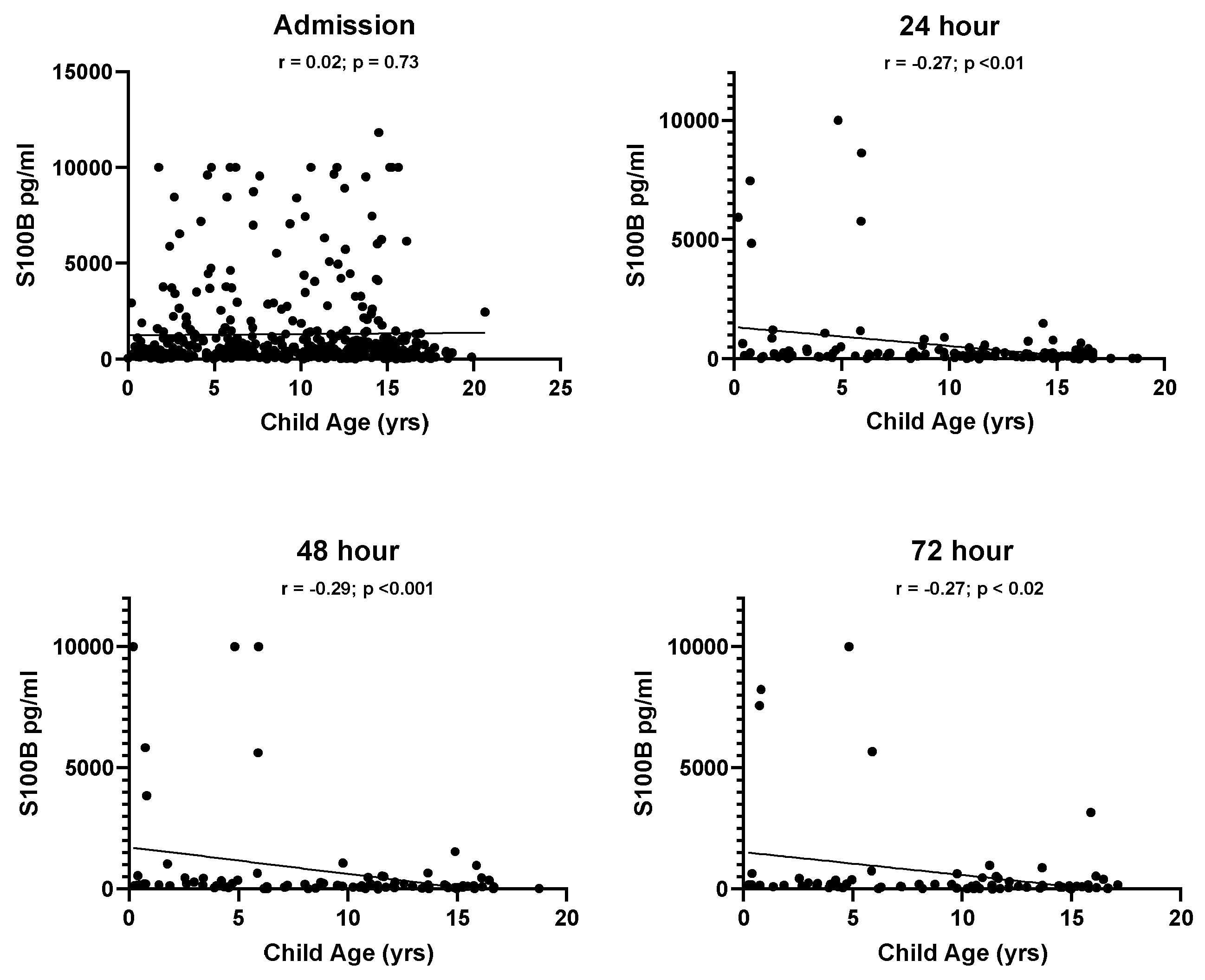
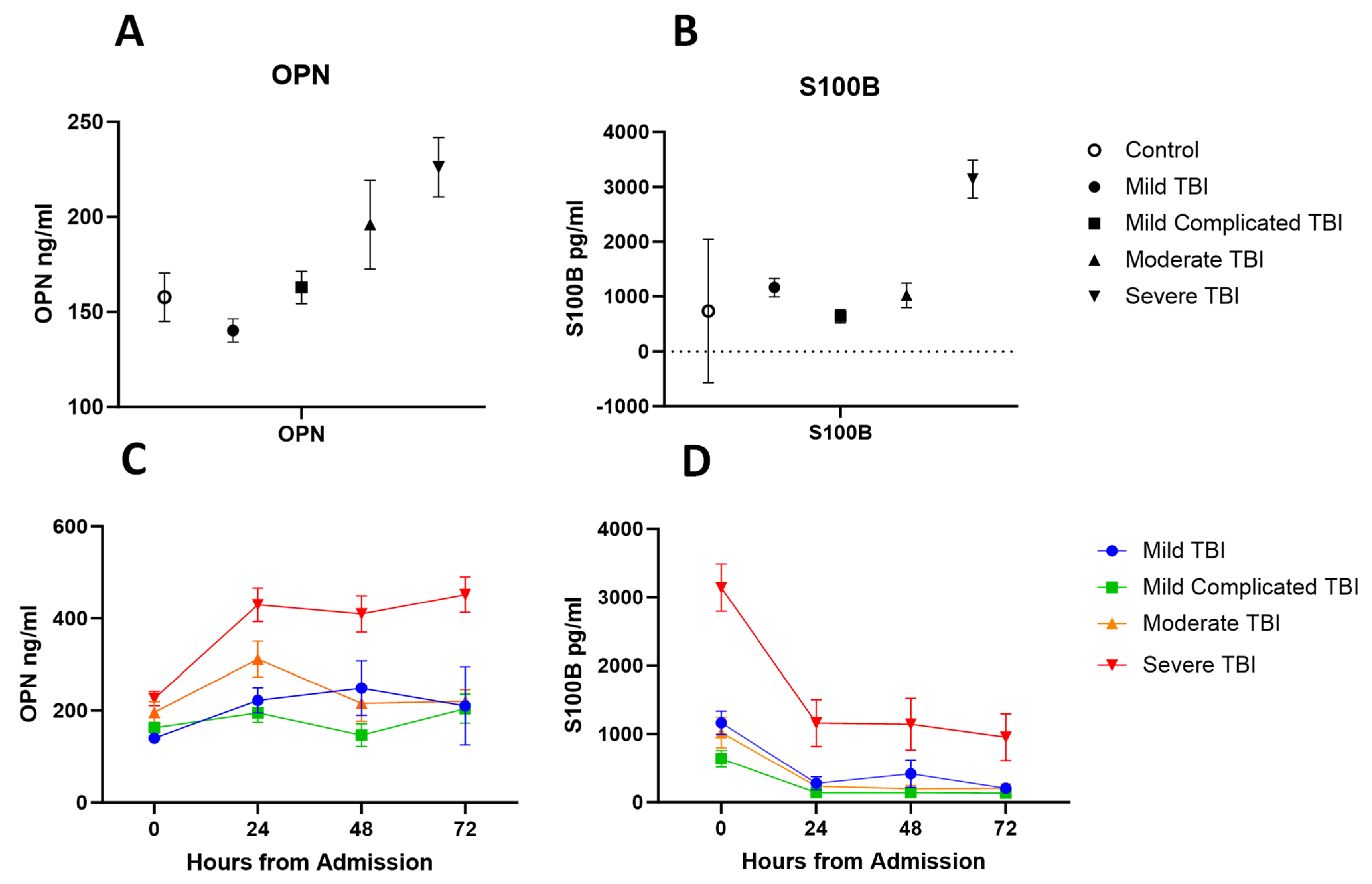
3.2. Plasma Concentrations and Demographic Variables
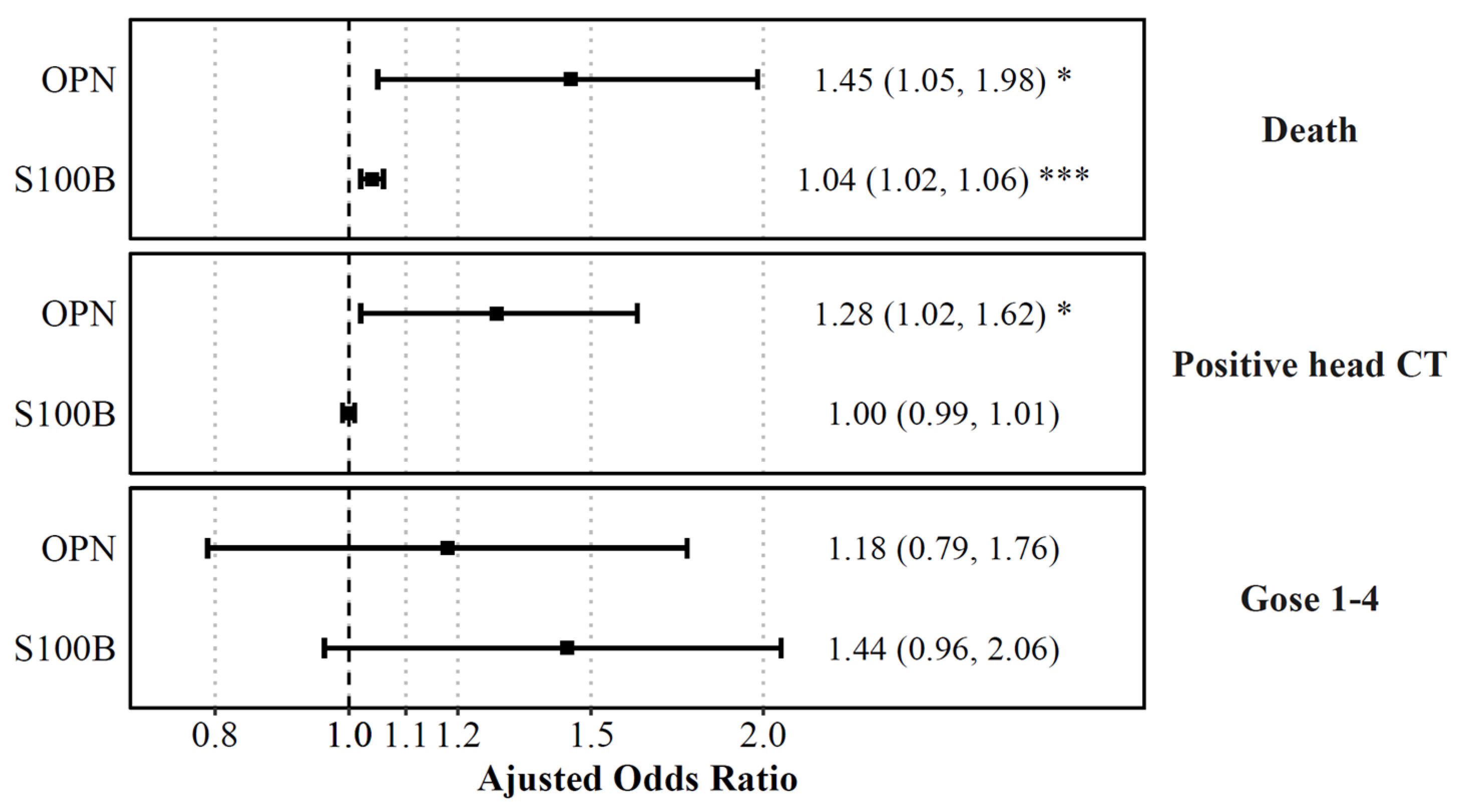
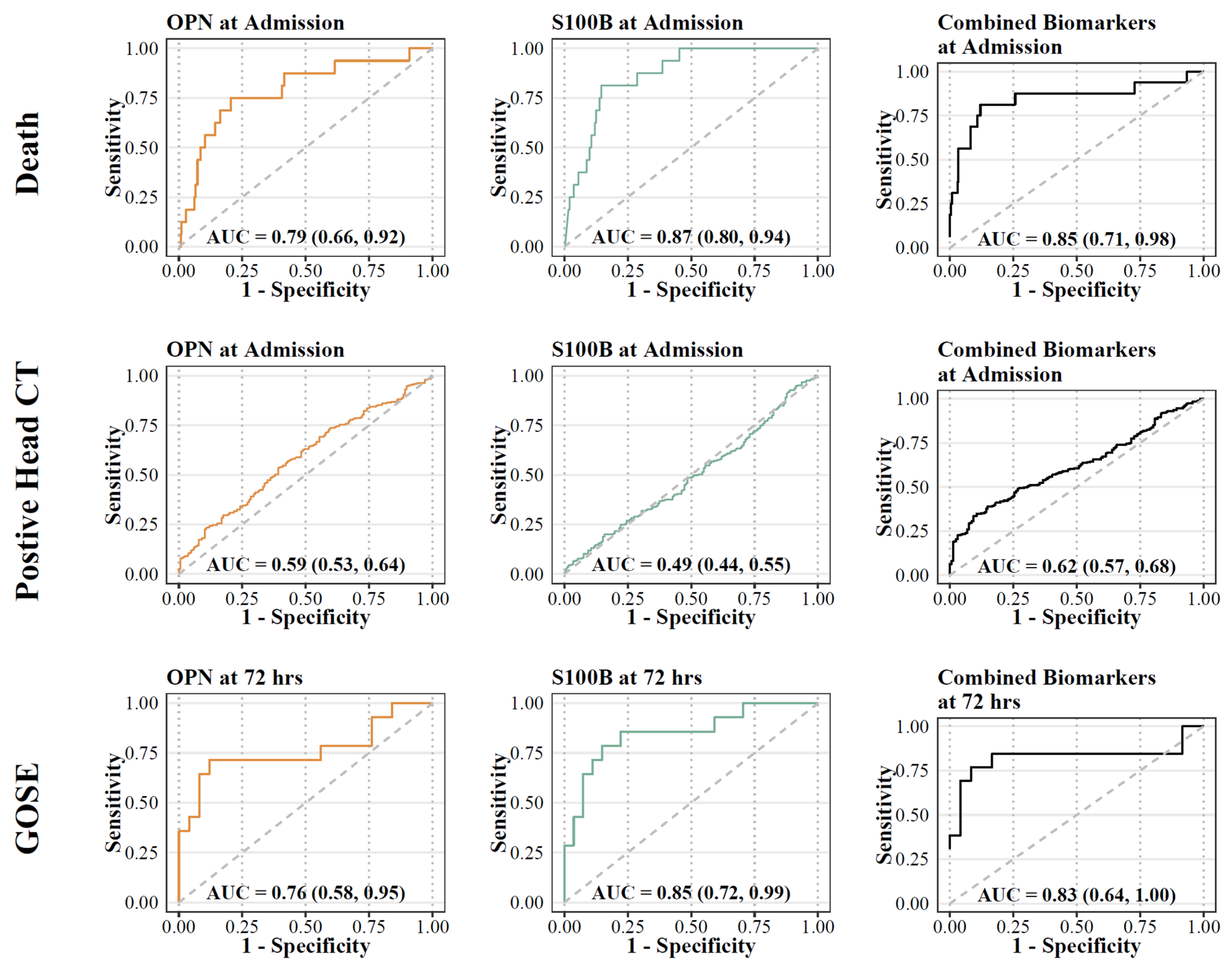
3.3. Plasma Concentrations at Admission and Acute Outcomes
3.4. Plasma Concentrations of Biomarkers and GOSE-Peds at 6 Months
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maas, A.I.R.; Menon, D.K.; Manley, G.T.; Abrams, M.; Åkerlund, C.; Andelic, N.; Aries, M.; Bashford, T.; Bell, M.J.; Bodien, Y.G.; et al. Traumatic brain injury: Progress and challenges in prevention, clinical care, and research. Lancet Neurol. 2022, 21, 1004–1060. [Google Scholar] [CrossRef]
- Taylor, C.; Bell, J.; Breiding, M.; Xy, L. Traumatic Brain Injury–Related Emergency Department Visits, Hospitalizations, and Deaths—United States, 2007 and 2013. MMWR Surveill. Summ. 2017, 66, 1–16. [Google Scholar] [CrossRef]
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2018, 130, 1080–1097. [Google Scholar] [CrossRef] [Green Version]
- Maas, A.I.R.; Fitzgerald, M.; Gao, G.; Gupta, D.; Hutchinson, P.; Manley, G.T.; Menon, D.K. Traumatic brain injury over the past 20 years: Research and clinical progress. Lancet Neurol. 2022, 21, 768–770. [Google Scholar] [CrossRef]
- Kochanek, P.M.; Tasker, R.C.; Carney, N.; Totten, A.M.; Adelson, P.D.; Selden, N.R.; Davis-O’Reilly, C.; Hart, E.L.; Bell, M.J.; Bratton, S.; et al. Guidelines for the Management of Pediatric Severe Traumatic Brain Injury, Third Edition: Update of the Brain Trauma Foundation Guidelines, Executive Summary. Clin. Neurosurg. 2019, 84, 1169–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babikian, T.; Asarnow, R. Neurocognitive Outcomes and Recovery After Pediatric TBI: Meta-Analytic Review of the Literature. Neuropsychology 2009, 23, 283–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurowski, B.; Martin, L.J.; Wade, S.L. Genetics and outcomes after traumatic brain injury (TBI): What do we know about pediatric TBI? J. Pediatr. Rehabil. Med. 2012, 5, 217–231. [Google Scholar] [CrossRef] [Green Version]
- Lesko, L.J.; Atkinson, J. Use of biomarkers and surrogate endpoints in drug development and regulatory decision making: Criteria, validation, strategies. Annu. Rev. Pharmacol. Toxicol. 2001, 41, 347–366. [Google Scholar] [CrossRef]
- Munoz Pareja, J.C.; Li, X.; Gandham, N.; Wang, K.K.; The Pediatric TBI Workgroup. Biomarkers in Moderate to Severe Pediatric Traumatic Brain Injury: A Review of the Literature. Pediatr. Neurol. 2022, 130, 60–68. [Google Scholar] [CrossRef]
- Yokobori, S.; Hosein, K.; Burks, S.; Sharma, I.; Gajavelli, S.; Bullock, R. Biomarkers for the Clinical Differential Diagnosis in Traumatic Brain Injury—A Systematic Review. CNS Neurosci. Ther. 2013, 19, 556–565. [Google Scholar] [CrossRef]
- Wang, K.K.; Yang, Z.; Zhu, T.; Shi, Y.; Rubenstein, R.; Tyndall, J.A.; Manley, G.T. An update on diagnostic and prognostic biomarkers for traumatic brain injury. Expert Rev. Mol. Diagn. 2018, 18, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.K.; Pareja, J.C.M.; Mondello, S.; Diaz-Arrastia, R.; Wellington, C.; Kenney, K.; Puccio, A.M.; Hutchison, J.; McKinnon, N.; Okonkwo, D.O.; et al. Blood-based traumatic brain injury biomarkers—Clinical utilities and regulatory pathways in the United States, Europe and Canada. Expert Rev. Mol. Diagn. 2021, 21, 1303–1321. [Google Scholar] [CrossRef] [PubMed]
- Petranovich, C.L.; Smith-Paine, J.; Wade, S.L.; Yeates, K.O.; Taylor, H.G.; Stancin, T.; Kurowski, B.G. From early childhood to adolescence: Lessons about traumatic brain injury (TBI) from the Ohio Head Injury Outcomes Study HHS Public Access. J. Head Trauma Rehabil. 2020, 35, 226–239. [Google Scholar] [CrossRef] [PubMed]
- Papa, L.; Ramia, M.M.; Edwards, D.; Johnson, B.D.; Slobounov, S.M. Systematic Review of Clinical Studies Examining Biomarkers of Brain Injury in Athletes after Sports-Related Concussion. J. Neurotrauma. 2015, 32, 661–673. [Google Scholar] [CrossRef] [Green Version]
- Bazarian, J.J.; Welch, R.D.; Caudle, K.; Jeffrey, C.A.; Chen, J.Y.; Chandran, R.; McCaw, T.; Datwyler, S.A.; Zhang, H.; McQuiston, B. Accuracy of a rapid glial fibrillary acidic protein/ubiquitin carboxyl-terminal hydrolase L1 test for the prediction of intracranial injuries on head computed tomography after mild traumatic brain injury. Acad. Emerg. Med. 2021, 28, 1308–1317. [Google Scholar] [CrossRef] [PubMed]
- Biberthaler, P.; Musaelyan, K.; Krieg, S.; Meyer, B.; Stimmer, H.; Zapf, J.; von Matthey, F.; Chandran, R.; Marino, J.A.; Beligere, G.; et al. Evaluation of Acute Glial Fibrillary Acidic Protein and Ubiquitin C-Terminal Hydrolase-L1 Plasma Levels in Traumatic Brain Injury Patients with and without Intracranial Lesions. Neurotrauma Rep. 2021, 2, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Korley, F.K.; Datwyler, S.A.; Jain, S.; Sun, X.; Beligere, G.; Chandran, R.; Marino, J.A.; McQuiston, B.; Zhang, H.; Caudle, K.L.; et al. Comparison of GFAP and UCH-L1 Measurements from Two Prototype Assays: The Abbott i-STAT and ARCHITECT Assays. Neurotrauma Rep. 2021, 2, 193–199. [Google Scholar] [CrossRef]
- Korley, F.K.; Jain, S.; Sun, X.; Puccio, A.M.; Yue, J.K.; Gardner, R.C.; Okonkwo, D.O.; Mukherjee, P.; Nelson, L.D.; Taylor, S.R.; et al. Prognostic value of day-of-injury plasma GFAP and UCH-L1 concentrations for predicting functional recovery after traumatic brain injury in patients from the US TRACK-TBI cohort: An observational cohort study. Artic. Lancet Neurol. 2022, 21, 803–816. [Google Scholar] [CrossRef]
- Diaz-Arrastia, R.; Wang, K.K.W.; Papa, L.; Sorani, M.D.; Yue, J.K.; Puccio, A.M.; McMahon, P.J.; Inoue, T.; Yuh, E.L.; Lingsma, H.F.; et al. Acute Biomarkers of Traumatic Brain Injury: Relationship between Plasma Levels of Ubiquitin C-Terminal Hydrolase-L1 and Glial Fibrillary Acidic Protein. J. Neurotrauma 2014, 31, 19–25. [Google Scholar] [CrossRef]
- Okonkwo, D.O.; Yue, J.K.; Puccio, A.M.; Panczykowski, D.M.; Inoue, T.; McMahon, P.J.; Sorani, M.D.; Yuh, E.L.; Lingsma, H.F.; Maas, A.I.R.; et al. GFAP-BDP as an Acute Diagnostic Marker in Traumatic Brain Injury: Results from the Prospective Transforming Research and Clinical Knowledge in Traumatic Brain Injury Study. J. Neurotrauma 2013, 30, 1490–1497. [Google Scholar] [CrossRef] [Green Version]
- Thelin, E.P.; Nelson, D.W.; Bellander, B.M. A review of the clinical utility of serum S100B protein levels in the assessment of traumatic brain injury. Acta. Neurochir. 2017, 159, 209–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiani, M.; Chaparian, A. Evaluation of image quality, organ doses, effective dose, and cancer risk from pediatric brain CT scans. Eur. J. Radiol. 2022, 158, 110657. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.; Gao, G.; Feng, J.; Jin, Y.; Wang, C.; Mao, Q. Glial fibrillary acidic protein as a biomarker in severe traumatic brain injury patients: A prospective cohort study. Crit. Care 2015, 19, 362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, F.; Wang, X.; Wu, H.; Wu, Q.; Zhang, J. Microglia and Neuroinflammation: Crucial Pathological Mechanisms in Traumatic Brain Injury-Induced Neurodegeneration. Front. Aging Neurosci. 2022, 14, 825086. [Google Scholar] [CrossRef]
- Hernandez-Ontiveros, D.G.; Tajiri, N.; Acosta, S.; Giunta, B.; Tan, J.; Borlongan, C.V. Microglia activation as a biomarker for traumatic brain injury. Front. Neurol. 2013, 4, 30. [Google Scholar] [CrossRef] [Green Version]
- Lanteri, P.; Lombardi, G.; Colombini, A.; Grasso, D.; Banfi, G. Stability of osteopontin in plasma and serum. Clin. Chem. Lab. Med. 2012, 50, 1979–1984. [Google Scholar] [CrossRef]
- Rubin, D.M.; Christian, C.W.; Bilaniuk, L.T.; Zazyczny, K.A.; Durbin, D.R. Occult head injury in high-risk abused children. Pediatrics 2003, 111 Pt 1, 1382–1386. [Google Scholar] [CrossRef]
- Sarkar, K.; Keachie, K.; Nguyen, U.; Muizelaar, J.P.; Zwienenberg-Lee, M.; Shahlaie, K. Computed tomography characteristics in pediatric versus adult traumatic brain injury. J. Neurosurg. Pediatr. 2014, 13, 307–314. [Google Scholar] [CrossRef] [Green Version]
- Yue, J.K.; Kobeissy, F.H.; Jain, S.; Sun, X.; Phelps, R.R.L.; Korley, F.K.; Gardner, R.C.; Ferguson, A.R.; Huie, J.R.; Schneider, A.L.C.; et al. Neuroinflammatory Biomarkers for Traumatic Brain Injury Diagnosis and Prognosis: A TRACK-TBI Pilot Study. Neurotrauma Rep. 2023, 4, 171. [Google Scholar] [CrossRef]
- Asgari, S.; Higgins, V.; McCudden, C.; Adeli, K. Continuous reference intervals for 38 biochemical markers in healthy children and adolescents: Comparisons to traditionally partitioned reference intervals. Clin. Biochem. 2019, 73, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Ozarda, Y.; Sikaris, K.; Streichert, T.; Macri, J. Distinguishing reference intervals and clinical decision limits—A review by the IFCC Committee on Reference Intervals and Decision Limits. Crit. Rev. Clin. Lab. Sci. 2018, 55, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Adelson, P.D.; Pineda, J.; Bell, M.J.; Abend, N.S.; Berger, R.P.; Giza, C.C.; Hotz, G.; Wainwright, M.S. Common data elements for pediatric traumatic brain injury: Recommendations from the working group on demographics and clinical assessment. J. Neurotrauma 2012, 29, 639–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dikmen, S.; Machamer, J.; Manley, G.T.; Yuh, E.L.; Nelson, L.D.; Temkin, N.R. Functional Status Examination versus Glasgow Outcome Scale Extended as Outcome Measures in Traumatic Brain Injuries: How Do They Compare? J. Neurotrauma 2019, 36, 2423–2429. [Google Scholar] [CrossRef] [PubMed]
- McMillan, T.; Wilson, L.; Ponsford, J.; Levin, H.; Teasdale, G.; Bond, M. The Glasgow Outcome Scale—40 years of application and refinement. Nat. Rev. Neurol. 2016, 12, 477–485. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | Control | Mild | Mild-Complicated | Moderate | Severe | p | SMD b,c | |
|---|---|---|---|---|---|---|---|---|
| n = 460 | n = 35 | n = 141 | n = 143 | n = 51 | n = 90 | |||
| Patient demographics | ||||||||
| Age | 9.69 [3.92, 13.71] | 12.62 [8.20, 14.66] | 12.31 [7.58, 14.65] | 6.88 [2.05, 13.01] | 6.78 [2.25, 13.23] | 7.83 [4.07, 11.87] | <0.001 | 0.43 |
| Sex (M) | 302 (65.7%) | 24 (68.6%) | 89 (63.1%) | 96 (67.1%) | 36 (70.6%) | 57 (63.3%) | 0.838 | 0.086 |
| Ethnicity | ||||||||
| African American or Black | 151 (32.8%) | 7 (20.0%) | 47 (33.3%) | 31 (21.7%) | 21 (41.2%) | 45 (50.0%) | <0.001 | 0.537 |
| Asian | 15 (3.3%) | 0 (0.0%) | 5 (3.5%) | 6 (4.2%) | 3 (5.9%) | 1 (1.1%) | ||
| Hispanic/ Latino | 51 (11.1%) | 4 (11.4%) | 13 (9.2%) | 15 (10.5%) | 6 (11.8%) | 13 (14.4%) | ||
| Other | 9 (2.0%) | 0 (0.0%) | 1 (0.7%) | 3 (2.1%) | 3 (5.9%) | 2 (2.2%) | ||
| White | 234 (50.9%) | 24 (68.6%) | 75 (53.2%) | 88 (61.5%) | 18 (35.3%) | 29 (32.2%) | ||
| Clinical variables | ||||||||
| Mechanism of Injury | ||||||||
| Fall | 147 (32.0%) | 10 (28.6%) | 42 (29.8%) | 71 (49.7%) | 16 (31.4%) | 8 (8.9%) | <0.001 | 0.967 |
| MVC | 124 (27.0%) | 10 (28.6%) | 43 (30.5%) | 16 (11.2%) | 13 (25.5%) | 42 (46.7%) | ||
| Peds vs. motor vehicle | 42 (9.1%) | 1 (2.9%) | 14 (9.9%) | 9 (6.3%) | 2 (3.9%) | 16 (17.8%) | ||
| Bike | 22 (4.8%) | 4 (11.4%) | 8 (5.7%) | 9 (6.3%) | 1 (2.0%) | 0 (0.0%) | ||
| Struck by/against | 44 (9.6%) | 2 (5.7%) | 15 (10.6%) | 18 (12.6%) | 6 (11.8%) | 3 (3.3%) | ||
| Confirmed abuse | 8 (1.7%) | 0 (0.0%) | 0 (0.0%) | 3 (2.1%) | 2 (3.9%) | 3 (3.3%) | ||
| Suspected abuse | 24 (5.2%) | 0 (0.0%) | 1 (0.7%) | 8 (5.6%) | 6 (11.8%) | 9 (10.0%) | ||
| ATV | 32 (7.0%) | 1 (2.9%) | 15 (10.6%) | 8 (5.6%) | 4 (7.8%) | 4 (4.4%) | ||
| Other | 17 (3.7%) | 7 (20.0%) | 3 (2.1%) | 1 (0.7%) | 1 (2.0%) | 5 (5.6%) | ||
| Clinical outcomes | ||||||||
| Death | 16 (3.5%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 16 (17.8%) | <0.001 | 0.263 |
| Positive head CT | 252 (58.9%) | 0 (0.0%) | 11 (9.4%) | 132 (92.3%) | 34 (68.0%) | 75 (83.3%) | <0.001 | 1.854 |
| ICU Admission | 184 (40.0%) | 2 (5.7%) | 10 (7.1%) | 46 (32.2%) | 38 (74.5%) | 88 (97.8%) | <0.001 | 1.791 |
| ≥Cut-Off | <Cut-Off | Odds Ratio (95% CI) | AUC (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | |
|---|---|---|---|---|---|---|
| OPN at admission | ||||||
| Death | ≥218.63 | <218.63 | ||||
| Yes | 11 (12.5%) | 5 (1.4%) | 9.91 (3.35, 29.36) | 0.75 (0.63, 0.87) | 0.69 (0.46, 0.91) | 0.82 (0.78, 0.86) |
| No | 77 (87.5%) | 347 (98.6%) | Ref. | |||
| Positive head CT | ≥144.75 | <144.75 | ||||
| Yes | 141 (65.0%) | 102 (53.1%) | 1.64 (1.10, 2.44) | 0.56 (0.51, 0.61) | 0.58 (0.52, 0.64) | 0.54 (0.47, 0.62) |
| No | 76 (35.0%) | 90 (46.9%) | Ref. | |||
| OPN at 72 h | ||||||
| Gose | ≥497.89 | <497.89 | ||||
| 1–4 | 9 (75.0%) | 5 (18.5%) | 13.2 (2.59, 67.23) | 0.76 (0.62, 0.91) | 0.64 (0.39, 0.89) | 0.88 (0.75, 1) |
| 5–8 | 3 (25.0%) | 22 (81.5%) | Ref. | |||
| S100B at admission | ||||||
| Death | ≥1951.35 | <1951.35 | ||||
| Yes | 12 (16.0%) | 4 (1.1%) | 17.57 (5.49, 56.2) | 0.8 (0.69, 0.91) | 0.75 (0.54, 0.96) | 0.85 (0.82, 0.89) |
| No | 63 (84%) | 369 (98.9%) | Ref. | |||
| Positive head CT | ≥492.90 | <492.90 | ||||
| Yes | 117 (58.5%) | 128 (59.3%) | 0.97 (0.66, 1.43) | 0.5 (0.45, 0.55) | 0.48 (0.42, 0.54) | 0.51 (0.44, 0.59) |
| No | 83 (41.5%) | 88 (40.7%) | Ref. | |||
| S100B at 72 h | ||||||
| Gose | ≥179.65 | <179.65 | ||||
| 1–4 | 10 (71.4%) | 4 (14.8%) | 14.37 (2.98, 69.25) | 0.78 (0.64, 0.92) | 0.71 (0.48, 0.95) | 0.85 (0.72, 0.99) |
| 5–8 | 4 (28.6%) | 23 (85.2%) | Ref. | |||
| OPN | S100B | |
|---|---|---|
| Death | ||
| Univariable Analysis | ||
| OR (95% CI) | 1.65 (1.27, 2.16) *** | 1.03 (1.02, 1.05) *** |
| AUC | 0.79 (0.66, 0.92) | 0.87 (0.80, 0.94) |
| Multivariable Analysis | ||
| OR (95% CI) | 1.45 (1.05, 1.98) * | 1.04 (1.02, 1.06) *** |
| AUC | 0.85 (0.71, 0.98) | |
| Head CT | ||
| Univariable Analysis | ||
| OR (95% CI) | 1.44 (1.16, 1.78) *** | 1 (0.99, 1.01) |
| AUC | 0.59 (0.53, 0.64) | 0.49 (0.44, 0.55) |
| Multivariable Analysis | ||
| OR (95% CI) | 1.28 (1.02, 1.62) * | 1.00 (0.99, 1.01) |
| AUC | 0.62 (0.57, 0.68) | |
| GOSE-Peds | ||
| Univariable Analysis | ||
| OR (95% CI) | 1.56 (1.15, 2.11) ** | 1.46 (1.01, 2.11) * |
| AUC | 0.76 (0.58, 0.95) | 0.85 (0.72, 0.99) |
| Multivariable Analysis | ||
| OR (95% CI) | 1.18 (0.79, 1.76) | 1.44 (0.96, 2.06) |
| AUC | 0.83 (0.64, 1.00) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blackwell, L.S.; Wali, B.; Xiang, Y.; Alawieh, A.; Sayeed, I.; Reisner, A. Prognostic Value of Plasma Biomarkers S100B and Osteopontin in Pediatric TBI: A Prospective Analysis Evaluating Acute and 6-Month Outcomes after Mild to Severe TBI. Biomedicines 2023, 11, 2167. https://doi.org/10.3390/biomedicines11082167
Blackwell LS, Wali B, Xiang Y, Alawieh A, Sayeed I, Reisner A. Prognostic Value of Plasma Biomarkers S100B and Osteopontin in Pediatric TBI: A Prospective Analysis Evaluating Acute and 6-Month Outcomes after Mild to Severe TBI. Biomedicines. 2023; 11(8):2167. https://doi.org/10.3390/biomedicines11082167
Chicago/Turabian StyleBlackwell, Laura S., Bushra Wali, Yijin Xiang, Ali Alawieh, Iqbal Sayeed, and Andrew Reisner. 2023. "Prognostic Value of Plasma Biomarkers S100B and Osteopontin in Pediatric TBI: A Prospective Analysis Evaluating Acute and 6-Month Outcomes after Mild to Severe TBI" Biomedicines 11, no. 8: 2167. https://doi.org/10.3390/biomedicines11082167
APA StyleBlackwell, L. S., Wali, B., Xiang, Y., Alawieh, A., Sayeed, I., & Reisner, A. (2023). Prognostic Value of Plasma Biomarkers S100B and Osteopontin in Pediatric TBI: A Prospective Analysis Evaluating Acute and 6-Month Outcomes after Mild to Severe TBI. Biomedicines, 11(8), 2167. https://doi.org/10.3390/biomedicines11082167