

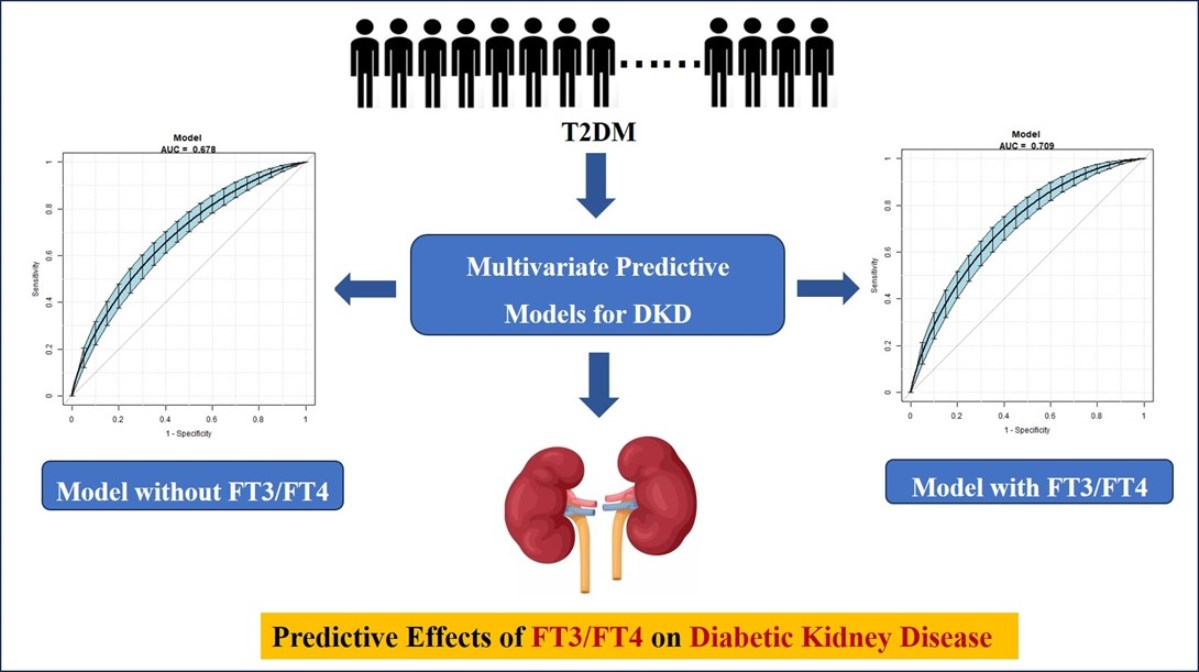
Predictive Effects of FT3/FT4 on Diabetic Kidney Disease: An Exploratory Study on Hospitalized Euthyroid Patients with T2DM in China

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Research Subjects
2.3. Methods
General Conditions and Laboratory Biochemical Indices
2.4. Statistical Analysis
3. Results
3.1. Comparison of General Characteristics and Biochemical Indexes among the Three Groups
3.2. Correlation Analysis between Thyroid Hormone and Renal Function (UACR, eGFR)
3.3. Logistic Regression Analyses of TH and DKD
3.4. Univariate Predictive Model of DKD with TH
3.5. Multivariate Predictive Model for the Risk of DKD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, M.C.; Brownlee, M.; Susztak, K.; Sharma, K.; Jandeleit-Dahm, K.A.M.; Zoungas, S.; Rossing, P.; Groop, P.-H.; Cooper, M.E. Diabetic kidney disease. Nat. Rev. Dis. Prim. 2015, 1, 15018. [Google Scholar] [CrossRef] [PubMed]
- Looker, H.C.; Mauer, M.; Nelson, R.G. Role of Kidney Biopsies for Biomarker Discovery in Diabetic Kidney Disease. Adv. Chronic Kidney Dis. 2018, 25, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Yan, B.; Wang, F.; Wen, F.; Xing, X.; Tang, X.; Shi, Y.; Le, G. Type 1 5′-deiodinase activity is inhibited by oxidative stress and restored by alpha-lipoic acid in HepG2 cells. Biochem. Biophys. Res. Commun. 2016, 472, 496–501. [Google Scholar] [CrossRef]
- Oda, T.; Taneichi, H.; Takahashi, K.; Togashi, H.; Hangai, M.; Nakagawa, R.; Ono, M.; Matsui, M.; Sasai, T.; Nagasawa, K.; et al. Positive association of free triiodothyronine with pancreatic β-cell function in people with prediabetes. Diabet. Med. 2015, 32, 213–219. [Google Scholar] [CrossRef]
- Ruhla, S.; Arafat, A.M.; Weickert, M.O.; Osterhoff, M.; Isken, F.; Spranger, J.; Schöfl, C.; Pfeiffer, A.F.H.; Möhlig, M. T3/rT3-Ratio is Associated with Insulin Resistance Independent of TSH. Horm. Metab. Res. 2011, 43, 130–134. [Google Scholar] [CrossRef]
- Ruhla, S.; Weickert, M.O.; Arafat, A.M.; Osterhoff, M.; Isken, F.; Spranger, J.; Schöfl, C.; Pfeiffer, A.F.H.; Möhlig, M. A high normal TSH is associated with the metabolic syndrome. Clin. Endocrinol. 2010, 72, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Topsakal, S.; Yerlikaya, E.; Akin, F.; Kaptanoglu, B.; Erürker, T. Relation with HOMA-IR and thyroid hormones in obese Turkish women with metabolic syndrome. Eat. Weight. Disord. Stud. Anorexia, Bulim. Obes. 2012, 17, e57–e61. [Google Scholar] [CrossRef] [PubMed]
- Amouzegar, A.; Kazemian, E.; Gharibzadeh, S.; Mehran, L.; Tohidi, M.; Azizi, F. Association between thyroid hormones, thyroid antibodies and insulin resistance in euthyroid individuals: A population-based cohort. Diabetes Metab. 2015, 41, 480–488. [Google Scholar] [CrossRef]
- Ahlqvist, E.; van Zuydam, N.R.; Groop, L.C.; McCarthy, M.I. The genetics of diabetic complications. Nat. Rev. Nephrol. 2015, 11, 277–287. [Google Scholar] [CrossRef]
- Ilera, V.; Delfino, L.C.; Zunino, A.; Glikman, P.; Drnovsek, M.; Reyes, A.; Dios, A.; Toibaro, J.; Pachioli, V.; Lannes, N.; et al. Correlation between inflammatory parameters and pituitary–thyroid axis in patients with COVID-19. Endocrine 2021, 74, 455–460. [Google Scholar] [CrossRef]
- Chaker, L.; Ligthart, S.; Korevaar, T.I.M.; Hofman, A.; Franco, O.H.; Peeters, R.P.; Dehghan, A. Thyroid function and risk of type 2 diabetes: A population-based prospective cohort study. BMC Med. 2016, 14, 150. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Definition, Diagnosis and Classification of Diabetes Mellitus and its Complications. Report of a WHO Consultation. Part 1: Diagnosis and Classification of Diabetes Mellitus; WHO: Geneva, Switzerland, 1999; pp. 4–7. [Google Scholar]
- Microvascular Complications Group of Diabetes Credit Association of Chinese Medical Association. Guidelines for the prevention and treatment of diabetes and kidney disease in China. Chin. J. Diabetes Mellit. 2021, 13, 762–784. [Google Scholar]
- Chuang, T.-J.; Lin, J.-D.; Wu, C.-Z.; Ku, H.-C.; Liao, C.-C.; Yeh, C.-J.; Pei, D.; Chen, Y.-L. The relationships between thyroid-stimulating hormone level and insulin resistance, glucose effectiveness, first- and second-phase insulin secretion in Chinese populations. Medicine 2021, 100, e25707. [Google Scholar] [CrossRef]
- Aguayo-Mazzucato, C.; Zavacki, A.M.; Marinelarena, A.; Hollister-Lock, J.; El Khattabi, I.; Marsili, A.; Weir, G.C.; Sharma, A.; Larsen, P.R.; Bonner-Weir, S. Thyroid Hormone Promotes Postnatal Rat Pancreatic β-Cell Development and Glucose-Responsive Insulin Secretion Through MAFA. Diabetes 2013, 62, 1569–1580. [Google Scholar] [CrossRef] [Green Version]
- Siddiqi, F.S.; Advani, A. Endothelial-Podocyte Crosstalk: The Missing Link Between Endothelial Dysfunction and Albuminuria in Diabetes. Diabetes 2013, 62, 3647–3655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, Y.; Yamagishi, S.-I.; Mizukami, H.; Yabe-Nishimura, C.; Lim, S.W.; Kwon, H.M.; Yagihashi, S. Polyol pathway and diabetic nephropathy revisited: Early tubular cell changes and glomerulopathy in diabetic mice overexpressing human aldose reductase. J. Diabetes Investig. 2011, 2, 111–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.-C.; Li, J.-L.; Wang, Y.-F.; Meng, Y.; Cai, Z.; Shen, C.; Wang, M.-D.; Zhao, W.-J.; Niu, W.-Q. Association between thyroid hormones and diabetic kidney disease in Chinese adults. BMC Endocr. Disord. 2023, 23, 56. [Google Scholar] [CrossRef]
- Zhang, Y.; Chang, Y.; Ryu, S.; Cho, J.; Lee, W.-Y.; Rhee, E.-J.; Kwon, M.-J.; Pastor-Barriuso, R.; Rampal, S.; Han, W.K.; et al. Thyroid hormone levels and incident chronic kidney disease in euthyroid individuals: The Kangbuk Samsung Health Study. Int. J. Epidemiol. 2014, 43, 1624–1632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Ye, L.; Wang, T.; Hong, J.; Bi, Y.; Zhang, J.; Xu, B.; Sun, J.; Huang, X.; Xu, M. Free Triiodothyronine Concentrations Are Inversely Associated with Microalbuminuria. Int. J. Endocrinol. 2014, 2014, 959781. [Google Scholar] [CrossRef] [Green Version]
- Darras, V.M. Deiodinases: How Nonmammalian Research Helped Shape Our Present View. Endocrinology 2021, 162, bqab039. [Google Scholar] [CrossRef]
- Zhang, Z.; Boelen, A.; Bisschop, P.H.; Kalsbeek, A.; Fliers, E. Hypothalamic effects of thyroid hormone. Mol. Cell. Endocrinol. 2017, 458, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Mooradian, A.D. Age-Related Resistance to Thyroid Hormone Action. Drugs Aging 2019, 36, 1007–1014. [Google Scholar] [CrossRef]
- Zhang, L.; Long, J.; Jiang, W.; Shi, Y.; He, X.; Zhou, Z.; Li, Y.; Yeung, R.O.; Wang, J.; Matsushita, K.; et al. Trends in Chronic Kidney Disease in China. N. Engl. J. Med. 2016, 375, 905–906. [Google Scholar] [CrossRef] [PubMed]
- Duntas, L.H.; Orgiazzi, J.; Brabant, G. The interface between thyroid and diabetes mellitus. Clin. Endocrinol. 2011, 75, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Okada, J.; Isoda, A.; Hoshi, H.; Watanabe, T.; Yamada, E.; Saito, T.; Okada, K.; Nakajima, Y.; Ozawa, A.; Ohshima, K.; et al. Free triiodothyronine /free thyroxine ratio as an index of deiodinase type 1 and 2 activities negatively correlates with casual serum insulin levels in patients with type 2 diabetes mellitus. Endocr. J. 2021, 68, 1237–1240. [Google Scholar] [CrossRef] [PubMed]
- Martinez, B.; Ortiz, R.M. Thyroid Hormone Regulation and Insulin Resistance: Insights From Animals Naturally Adapted to Fasting. Physiology 2017, 32, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Štěpánek, L.; Horáková, D.; Štěpánek, L.; Janout, V.; Janoutová, J.; Bouchalová, K.; Martiník, K. Free triiodothyronine/free thyroxine (FT3/FT4) ratio is strongly associated with insulin resistance in euthyroid and hypothyroid adults: A cross-sectional study. Endokrynol. Polska 2021, 72, 8–13. [Google Scholar] [CrossRef]
- Wang, J.; Li, H.; Tan, M.; Gao, G.; Zhang, Y.; Ding, B.; Su, X.; Kong, X.; Ma, J. Association between thyroid function and diabetic nephropathy in euthyroid subjects with type 2 diabetes mellitus: A cross-sectional study in China. Oncotarget 2019, 10, 88–97. [Google Scholar] [CrossRef] [Green Version]
- Díez, J.J.; Iglesias, P. Relationship between serum thyrotropin concentrations and metformin therapy in euthyroid patients with type 2 diabetes. Clin. Endocrinol. 2013, 78, 505–511. [Google Scholar] [CrossRef]
- Dimic, D.; Golubovic, M.V.; Radenkovic, S.; Radojkovic, D.; Pesic, M. The effect of metformin on TSH levels in euthyroid and hypothyroid newly diagnosed diabetes mellitus type 2 patients. Bratisl. LekListy 2016, 117, 433–435. [Google Scholar] [CrossRef] [Green Version]
- Radcliffe, N.J.; Seah, J.-M.; Clarke, M.; MacIsaac, R.J.; Jerums, G.; Ekinci, E.I. Clinical predictive factors in diabetic kidney disease progression. J. Diabetes Investig. 2017, 8, 6–18. [Google Scholar] [CrossRef] [PubMed]
- Alicic, R.Z.; Rooney, M.T.; Tuttle, K.R. Diabetic Kidney Disease: Challenges, Progress, and Possibilities. Clin. J. Am. Soc. Nephrol. 2017, 12, 2032–2045. [Google Scholar] [CrossRef] [PubMed]
- Kourtidou, C.; Stangou, M.; Marinaki, S.; Tziomalos, K. Novel Cardiovascular Risk Factors in Patients with Diabetic Kidney Disease. Int. J. Mol. Sci. 2021, 22, 11196. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Index | Low FT3/FT4 | Medium FT3/FT4 | High FT3/FT4 | F (χ2) | p |
|---|---|---|---|---|---|
| (n = 575) | (n = 577) | (n = 577) | |||
| Age (years) | 57.51 ± 13.83 | 54.53 ± 13.80 a | 51.96 ± 12.85 a,b | 24.32 | <0.01 |
| Sex (male%) | 309 (53.74%) | 354 (61.35%) | 411 (71.23%) | 41.06 | <0.01 |
| BMI (kg/m2) | 25.35 ± 3.73 | 26.18 ± 3.80 a | 26.75 ± 3.86 a,b | 17.05 | <0.01 |
| Diabetic duration (years) | 10.30 ± 9.22 | 9.50 ± 8.14 | 7.90 ± 6.83 a,b | 11.69 | <0.01 |
| SBP (mmHg) | 132.60 ± 18.68 | 132.10 ± 17.96 | 132.02 ± 15.55 | 0.18 | 0.83 |
| DBP (mmHg) | 78.93 ± 11.07 | 79.05 ± 11.35 | 79.70 ± 10.82 | 0.81 | 0.44 |
| WHR | 0.94 ± 0.08 | 0.95 ± 0.07 | 0.96 ± 0.06 a | 5.13 | 0.02 |
| TC (mmol/L) | 4.35 ± 1.17 | 4.40 ± 1.12 | 4.40 ± 1.10 | 0.21 | 0.81 |
| TG (mmol/L) | 1.95 ± 1.62 | 2.06 ± 1.42 | 2.06 ± 1.79 | 1.39 | 0.20 |
| LDL-C (mmol/L) | 2.55 ± 0.93 | 2.62 ± 0.93 | 2.60 ± 0.90 | 0.74 | 0.48 |
| HDL-C (mmol/L) | 1.02 ± 0.28 | 1.01 ± 0.28 | 0.99 ± 0.29 | 2.07 | 0.13 |
| UA (umol/L) | 339.82 ± 98.78 | 348.50 ± 93.42 | 348.51 ± 84.59 | 1.57 | 0.21 |
| eGFR | 93.35 ± 22.30 | 98.95 ± 18.86 a | 101.63 ± 17.26 a | 24.73 | <0.01 |
| UACR (mg/g) | 119.53 ± 440.90 | 61.08 ± 291.11 a | 57.96 ± 259.18 a | 5.39 | 0.02 |
| HbA1c (%) | 9.11 ± 2.12 | 8.38 ± 1.94 a | 8.02 ± 1.76 a,b | 39.39 | <0.01 |
| FBG (mmol/L) | 9.41 ± 3.60 | 8.64 ± 3.06 a | 8.00 ± 2.58 a,b | 27.04 | <0.01 |
| PBG (mmol/L) | 12.97 ± 4.74 | 12.62 ± 4.26 | 12.03 ± 4.03 a,b | 5.76 | 0.03 |
| FT4 (pmol/L) | 17.79 ± 1.85 | 16.58 ± 1.77 a | 15.22 ± 1.66 a,b | 306.65 | <0.01 |
| FT3 (pmol/L) | 4.03 ± 0.46 | 4.51 ± 0.49 a | 4.86 ± 0.54 a,b | 412.15 | <0.01 |
| TSH (uIU/mL) | 1.89 ± 0.88 | 1.97 ± 0.88 | 2.00 ± 0.89 | 2.66 | 0.07 |
| DKD (%) | 172 (29.9%) | 118 (20.45%) a | 94 (16.29%) a,b | 25.83 | <0.01 |
| Index | UACR | eGFR | ||
|---|---|---|---|---|
| r | p | r | p | |
| FT4 | −0.06 | 0.03 | 0.06 | 0.01 |
| FT3 | −0.13 | <0.01 | 0.20 | <0.01 |
| FT3/FT4 | −0.07 | <0.01 | 0.19 | <0.01 |
| Index | Crude OR | 95% CI | p | Adjust OR | 95% CI | p |
|---|---|---|---|---|---|---|
| FT3 (pmol/L) | ||||||
| High (>4.68) | 1.00 | 1.00 | ||||
| Medium (4.20–4.68) | 1.81 | 1.39, 2.36 | 0.02 | 1.74 | 1.21, 2.49 | 0.02 |
| Low (<4.20) | 2.20 | 1.68, 2.87 | 0.01 | 1.96 | 1.33, 2.90 | 0.03 |
| FT4 (pmol/L) | ||||||
| High (>17.39) | 1.00 | 1.00 | ||||
| Medium (15.66–17.39) | 0.94 | 0.73, 1.20 | 0.61 | 0.93 | 0.67, 1.30 | 0.68 |
| Low (<15.66) | 0.71 | 0.55, 0.93 | 0.02 | 0.85 | 0.60, 1.19 | 0.34 |
| FT3/FT4 | ||||||
| High (>0.29) | 1.00 | 1.00 | ||||
| Medium (0.25–0.29) | 3.13 | 2.32, 4.22 | <0.01 | 1.72 | 1.19, 2.49 | 0.02 |
| Low (<0.25) | 3.96 | 2.95, 5.32 | <0.01 | 2.36 | 1.63, 3.42 | 0.01 |
| TSH (uIU/mL) | ||||||
| High (>2.29) | 1.00 | 1.00 | ||||
| Medium (1.45–2.29) | 1.00 | 0.77, 1.30 | 0.99 | 1.02 | 0.73, 1.43 | 0.89 |
| Low (<1.45) | 0.95 | 0.74, 1.24 | 0.72 | 0.84 | 0.60, 1.17 | 0.30 |
| Index | AUC (95% CI) | Specificity | Sensitivity | Cut-Off |
|---|---|---|---|---|
| FT4 | 0.57 (0.54, 0.60) | 0.44 | 0.68 | 15.95 |
| FT3 | 0.61 (0.58, 0.64) | 0.54 | 0.64 | 4.85 |
| FT3/FT4 | 0.65 (0.62, 0.68) | 0.41 | 0.84 | 0.29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, X.; Sun, J.; Xin, S.; Zhang, X. Predictive Effects of FT3/FT4 on Diabetic Kidney Disease: An Exploratory Study on Hospitalized Euthyroid Patients with T2DM in China. Biomedicines 2023, 11, 2211. https://doi.org/10.3390/biomedicines11082211
Zhao X, Sun J, Xin S, Zhang X. Predictive Effects of FT3/FT4 on Diabetic Kidney Disease: An Exploratory Study on Hospitalized Euthyroid Patients with T2DM in China. Biomedicines. 2023; 11(8):2211. https://doi.org/10.3390/biomedicines11082211
Chicago/Turabian StyleZhao, Xin, Jianbin Sun, Sixu Xin, and Xiaomei Zhang. 2023. "Predictive Effects of FT3/FT4 on Diabetic Kidney Disease: An Exploratory Study on Hospitalized Euthyroid Patients with T2DM in China" Biomedicines 11, no. 8: 2211. https://doi.org/10.3390/biomedicines11082211
APA StyleZhao, X., Sun, J., Xin, S., & Zhang, X. (2023). Predictive Effects of FT3/FT4 on Diabetic Kidney Disease: An Exploratory Study on Hospitalized Euthyroid Patients with T2DM in China. Biomedicines, 11(8), 2211. https://doi.org/10.3390/biomedicines11082211