

An Investigation of Metabolic Risk Factors and Gut Microbiota in Unexplained Syncope
 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Assessment of Clinical and Metabolic Parameters
2.3. Instrumental Exams
2.4. Collection of Fecal Samples and Pre-Processing of Fastq Files with QIIME2
2.5. Statistical Analysis
2.6. Fecal Microbiota Analysis
3. Results
3.1. Anthropometric, Clinical, and Metabolic Characteristics
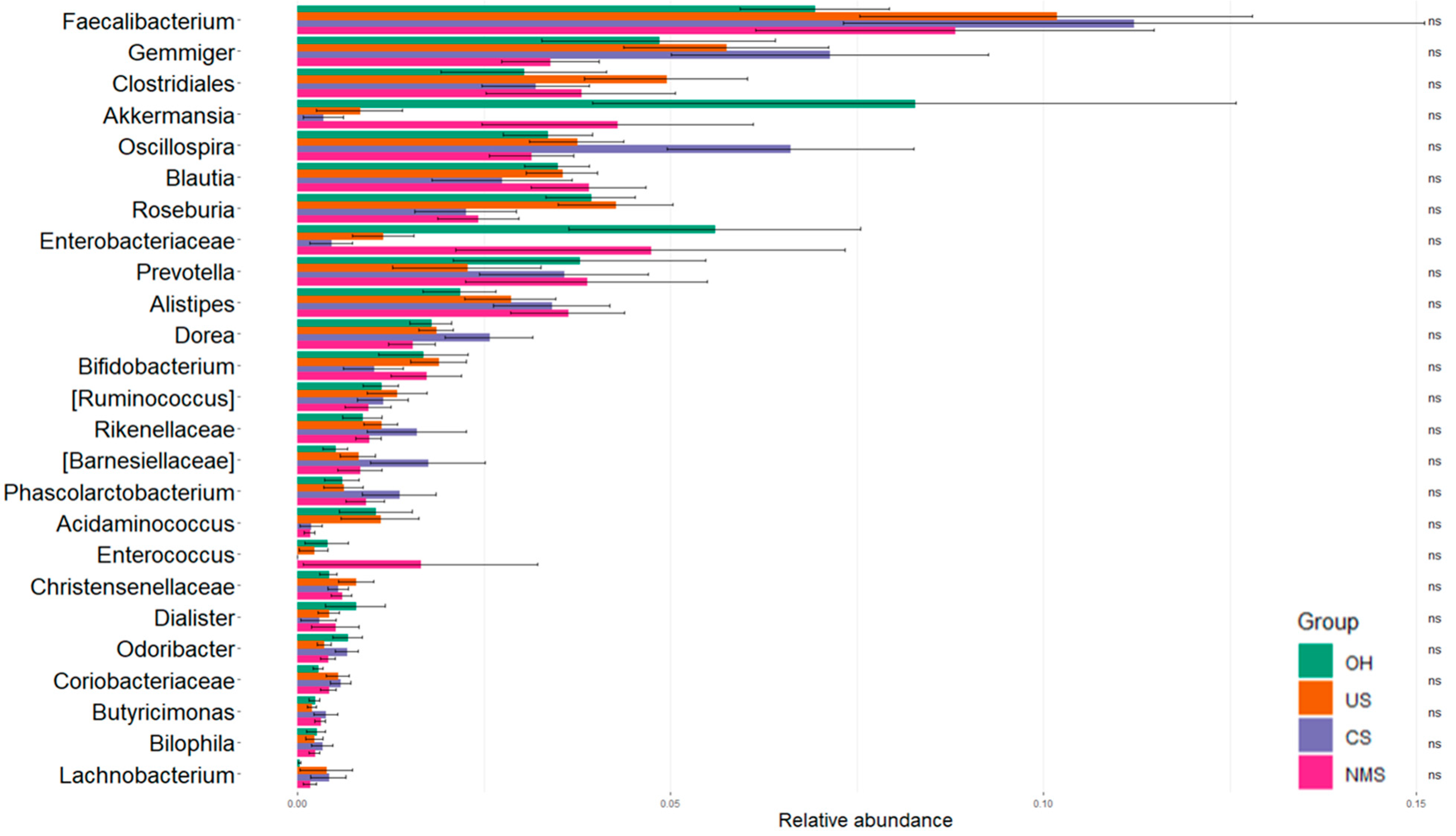
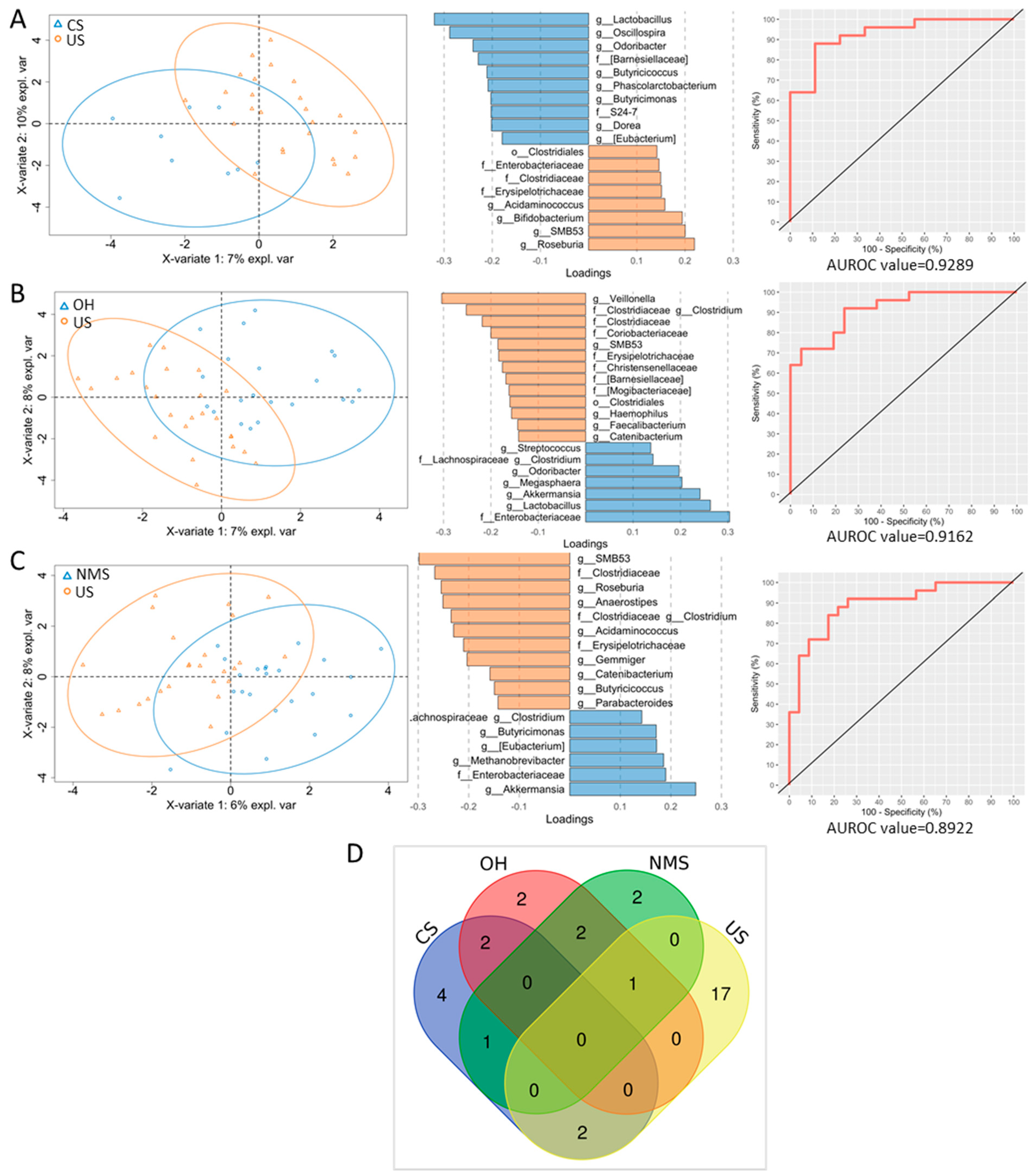
3.2. Characterization of Fecal Microbiota
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Longo, S.; Legramante, J.M.; Rizza, S.; Federici, M. Vasovagal syncope: An overview of pathophysiological mechanisms. Eur. J. Intern. Med. 2023, 112, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Moya, A.; De Lange, F.J.; Deharo, J.C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martìn, A.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef] [PubMed]
- Soteriades, E.S.; Evans, J.C.; Larson, M.G.; Chen, M.H.; Chen, L.; Benjamin, E.J.; Levy, D. Incidence and prognosis of syncope. N. Engl. J. Med. 2002, 19, 347, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.; Su, W.W.; Li, X. Risk factors of sudden cardiac death in hypertrophic cardiomyopathy. Curr. Opin. Cardiol. 2022, 37, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, Z.D.; Petek, B.J.; Brignole, M.; Shen, W.K.; Sheldon, R.S.; Solbiati, M.; Deharo, J.C.; Moya, A.; Hamdan, M.H. ACC/AHA/HRS Versus ESC Guidelines for the Diagnosis and Management of Syncope: JACC Guideline Comparison. J. Am. Coll. Cardiol. 2019, 74, 2410–2423. [Google Scholar] [CrossRef]
- Bai, W.; Chen, S.; Tang, C.S.; Qi, J.G.; Cui, Q.H.; Xu, M.; Du, J.B.; Jin, H.F. Gut microbiota analysis and its significance in vasovagal syncope in children. Chin. Med. J. 2019, 132, 411–419. [Google Scholar] [CrossRef]
- Longo, S.; Rizza, S.; Federici, M. Microbiota-gut-brain axis: Relationships among the vagus nerve, gut microbiota, obesity, and diabetes. Acta Diabetol. 2023, 60, 1007–1017. [Google Scholar] [CrossRef]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.; Holmes, S.P. DADA2: High-resolution sample inference from Illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef]
- DeSantis, T.Z.; Hugenholtz, P.; Larsen, N.; Rojas, M.; Brodie, E.L.; Keller, K.; Huber, T.; Dalevi, D.; Hu, P.; Andersen, G.L. Greengenes, a chimera-checked 16S rRNA gene database and workbench compatible with ARB. Appl. Environ. Microbiol. 2006, 72, 5069–5072. [Google Scholar] [CrossRef]
- Janssen, S.; McDonald, D.; Gonzalez, A.; Navas-Molina, J.A.; Jiang, L.; Xu, Z.Z.; Winker, K.; Kado, D.M.; Orwoll, E.; Manary, M.; et al. Phylogenetic Placement of Exact Amplicon Sequences Improves Associations with Clinical Information. mSystems 2018, 3, e00021-18. [Google Scholar] [CrossRef] [PubMed]
- McMurdie, P.J.; Holmes, S. phyloseq: An R package for reproducible interactive analysis and graphics of microbiome census data. PLoS ONE 2013, 8, e61217. [Google Scholar] [CrossRef] [PubMed]
- Paulson, J.N.; Stine, O.C.; Bravo, H.C.; Pop, M. Differential abundance analysis for microbial marker-gene surveys. Nat. Methods 2013, 10, 1200–1202. [Google Scholar] [CrossRef]
- Fernandez, G.; Lee, J.A.; Liu, L.C.; Gassler, J.P. The Baroreflex in Hypertension. Curr. Hypertens. Rep. 2015, 17, 19. [Google Scholar] [CrossRef] [PubMed]
- McCubbin, J.W.; Green, J.H.; Page, I.H. Baroceptor function in chronic renal hypertension. Circ. Res. 1956, 4, 205–210. [Google Scholar] [CrossRef]
- Matton, G. Carotid sinus and neurogenic and renal hypertension. J. Physiol. 1954, 29, 13–14P. [Google Scholar]
- Bishop, V.S.; Haywood, J.R.; Shade, R.E.; Siegel, M.; Hamm, C. Aortic baroreceptor deafferentation in the baboon. J. Appl. Physiol. 1986, 60, 798–801. [Google Scholar] [CrossRef]
- Viggiano, J.; Coutinho, D.; Clark-Cutaia, M.N.; Martinez, D. Effects of a high salt diet on blood pressure dipping and the implications on hypertension. Front. Neurosci. 2023, 17, 1212208. [Google Scholar] [CrossRef]
- Yasa, E.; Ricci, F.; Magnusson, M.; Sutton, R.; Gallina, S.; Caterina, R.; Melander, O.; Fedorowski, A. Cardiovascular risk after zhospitalization for unexplained syncope and orthostatic hypotension. Heart 2018, 104, 487–493. [Google Scholar] [CrossRef]
- da Silva, R.M.F.L.; Brugada, J. Cardiac and Vascular Causes of Syncope and Atherosclerosis. Curr. Cardiol. Rep. 2022, 24, 1241–1249. [Google Scholar] [CrossRef]
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgözoğlu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Primers 2019, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Xian, X.; Wang, Z.; Bi, Y.; Chen, Q.; Han, X.; Tang, D.; Chen, R. Research Progress on the Relationship between Atherosclerosis and Inflammation. Biomolecules 2018, 8, 80. [Google Scholar] [CrossRef]
- Wong, N.D.; Budoff, M.J.; Ferdinand, K.; Graham, I.M.; Michos, E.D.; Reddy, T.; Shapiro, M.D.; Toth, P.P. Atherosclerotic cardiovascular disease risk assessment: An American Society for Preventive Cardiology clinical practice statement. Am. J. Prev. Cardiol. 2022, 10, 100335. [Google Scholar] [CrossRef] [PubMed]
- Rizza, S.; Longo, S.; Piciucchi, G.; Romanello, D.; Mavilio, M.; Montagna, M.; Coppeta, L.; Martelli, E.; Magrini, A.; Federici, M. Carotid intimal medial thickness in rotating night shift is related to IL1β/IL6 axis. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1826–1832. [Google Scholar] [CrossRef] [PubMed]
- Zoto, E.; Cenko, F.; Doci, P.; Rizza, S. Effect of night shift work on risk of diabetes in healthy nurses in Albania. Acta Diabetol. 2019, 56, 811–813. [Google Scholar] [CrossRef]
- Stein, J.H.; Korcarz, C.E.; Hurst, R.T.; Lonn, E.; Kendall, C.B.; Mohler, E.R.; Najjar, S.S.; Rembold, C.M.; Post, W.S.; American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J. Am. Soc. Echocardiogr. 2008, 21, 93–111. [Google Scholar] [CrossRef]
- Poredos, P.; Jezovnik, M.K. Preclinical carotid atherosclerosis as an indicator of polyvascular disease: A narrative review. Ann. Transl. Med. 2021, 9, 1204. [Google Scholar] [CrossRef]
- Salonen, J.T.; Salonen, R. Ultrasonographically assessed carotid morphology and the risk of coronary heart disease. Arterioscler. Thromb. 1991, 11, 1245–1249. [Google Scholar] [CrossRef]
- Novo, S.; Diana, D.; Tomasino, C.; Zambelli, G.; Mignano, A.; Scalmato, A.; Maniscalco, L.; Galassi, A.R.; Matranga, D.; Novo, G. Electrocardiographic abnormalities, preclinical carotid atherosclerosis and cardiovascular risk in an apparently healthy real-world population. Data from the “No Stroke, No Infarction” project of the Rotary International—District 2110 (Sicily and Malta). Int Angiol. 2021, 40, 470–477. [Google Scholar] [CrossRef]
- Bergau, L.; Sohns, C.; Sommer, P. Unexplained syncope in a young athlete: The diagnostic process to find the diagnosis a case report. Eur. Heart J. Case Rep. 2022, 6, ytac018. [Google Scholar] [CrossRef]
- Runser, L.A.; Gauer, R.L.; Houser, A. Syncope: Evaluation and Differential Diagnosis. Am. Fam. Physician 2017, 95, 303–312. [Google Scholar] [PubMed]
- Davis, S.; Westby, M.; Pitcher, D.; Petkar, S. Implantable loop recorders are cost-effective when used to investigate transient loss of consciousness which is either suspected to be arrhythmic or remains unexplained. Europace 2012, 14, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Krahn, A.D.; Klein, G.J.; Yee, R.; Hoch, J.S.; Skanes, A.C. Cost implications of testing strategy in patients with syncope: Randomized assessment of syncope trial. J. Am. Coll. Cardiol. 2003, 42, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Tavora, M.Z.; Morillo, C.A. Explaining the unexplained causes of syncope: Are we there yet? J. Am. Coll. Cardiol. 2011, 58, 174–176. [Google Scholar] [CrossRef] [PubMed]
- Doundoulakis, I.; Gatzoulis, K.A.; Arsenos, P.; Dilaveris, P.; Skiadas, I.; Tsiachris, D.; Antoniou, C.K.; Soulaidopoulos, S.; Karystinos, G.; Pylarinou, V.; et al. Permanent pacemaker implantation in unexplained syncope patients with borderline sinus bradycardia and electrophysiology study-proven sinus node disease. J. Arrhythm. 2020, 37, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Menozzi, C.; Moya, A.; Garcia-Civera, R.; Mont, L.; Alvarez, M.; Errazquin, F.; Beiras, J.; Bottoni, N.; Donateo, P.; et al. Mechanism of syncope in patients with bundle branch block and negative electrophysiological test. Circulation 2001, 104, 2045–2050. [Google Scholar] [CrossRef]
- Moya, A.; Brignole, M.; Menozzi, C.; Garcia-Civera, R.; Tognarini, S.; Mont, L.; Botto, G.; Giada, F.; Cornacchia, D.; International Study on Syncope of Uncertain Etiology (ISSUE) Investigators. Mechanism of syncope in patients with isolated syncope and in patients with tilt-positive syncope. Circulation 2001, 104, 1261–1267. [Google Scholar] [CrossRef]
- Brignole, M.; Deharo, J.C.; De Roy, L.; Menozzi, C.; Blommaert, D.; Dabiri, L.; Ruf, J.; Guieu, R. Syncope due to idiopathic paroxysmal atrioventricular block: Long-term follow-up of a distinct form of atrioventricular block. J. Am. Coll. Cardiol. 2011, 58, 167–173. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions, and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content. |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | TLC Groups | p-Value | |||||
|---|---|---|---|---|---|---|---|
| CS (n = 9) | OH (n = 24) | NMS (n = 26) | US (n = 27) | US vs. CS | US vs. OH | US vs. NMS | |
| Age | 68.9 ± 16.0 * | 57.2 ± 16.2 * | 53.9 ± 13.7 * | 62.5 ± 14.5 * | 0.270 | 0.225 | 0.031 |
| Sex (M/F) | 5 (5.8%)/4 (4.7%) | 11 (12.8%)/13 (15.1%) | 12 (14.0%)/14 (16.3%) | 13 (15.1%)/14 (16.3%) | 0.700 | 0.869 | 0.884 |
| Altered sleep quality (n/y) | 4 (4.8%)/5 (6.0%) | 8 (9.6%)/16 (19.3%) | 5 (6.0%)/19 (22.9%) | 6 (7.2%)/20 (24.1%) | 0.221 | 0.420 | 0.848 |
| Alcohol (n/y) | 6 (7.1%)/3 (3.5%) | 19 (22.4%)/5 (5.9%) | 21 (24.7%)/4 (4.7%) | 19 (22.4%)/8 (9.4%) | 0.835 | 0.472 | 0.244 |
| Smoke (n/y) | 4 (4.7%)/5 (5.8%) | 21 (24.4%)/3 (3.5%) | 15 (17.4%)/11 (12.8%) | 14 (16.3%)/13 (15.1%) | 0.700 | 0.006 | 0.669 |
| Exercise (n/y) | 4 (4.8%)/5 (6.0%) | 16 (19.0%)/8 (9.5%) | 16 (19.0%)/9 (10.7%) | 20 (23.8%)/6 (7.1%) | 0.070 | 0.420 | 0.311 |
| History of hypertension (n/y) | 5 (5.8%)/4 (4.7%) | 14 (16.3%)/10 (11.6%) | 21 (24.4%)/5 (5.8%) | 13 (15.1%)/14 (16.3%) | 0.700 | 0.467 | 0.013 |
| History of diabetes (n/y) | 7 (8.1%)/2 (2.3%) | 21 (24.4%)/3 (3.5%) | 25 (29.1%)/1 (1.2%) | 22 (25.6%)/5 (5.8%) | 0.808 | 0.555 | 0.092 |
| Cardiovascular diseases (n/y) | 7 (8.1%)/2 (2.3%) | 21 (24.4%)/3 (3.5%) | 24 (27.9%)/2 (2.3%) | 23 (26.7%)/4 (4.7%) | 0.606 | 0.811 | 0.413 |
| History of syncope (n/y) | 4 (4.8%)/4 (4.8%) | 9 (10.8%)/14 (16.9%) | 6 (7.2%)/20 (24.1%) | 9 (10.8%)/17 (20.5%) | 0.434 | 0.744 | 0.358 |
| Weight | 70.0 ± 13.4 ** | 70.0 ± 20.2 ** | 65.5 ± 17.2 ** | 78.0 ± 12.5 ** | 0.241 | 0.91 | 0.029 |
| Height | 168 ± 9.3 ** | 165 ± 34.7 ** | 170 ± 9.7 ** | 167 ± 9.3 ** | 0.783 | 0.520 | 0.852 |
| BMI | 24.6 ± 2.9 ** | 25.7 ± 3.4 ** | 24.1 ± 4.6 ** | 26.7 ± 4.3 ** | 0.125 | 0.385 | 0.014 |
| Waist | 91.5 ± 8.0 ** | 94.5 ± 11.5 ** | 87.0 ± 16.3 ** | 98.0 ± 12.3 ** | 0.215 | 0.437 | 0.082 |
| SBP | 145 ± 12.1 * | 134 ± 14.3 * | 125 ± 13.5 * | 129 ± 15.7 * | 0.010 | 0.303 | 0.340 |
| DBP | 81.9 ± 10.5 * | 77.9 ± 9.2 * | 78.6 ± 8.7 * | 77.2 ± 10.8 * | 0.226 | 0.807 | 0.608 |
| Orthostatic hypotension (n/Y) | 7 (8.5%)/2 (2.4%) | 18 (22.0%)/5 (6.1%) | 24 (29.3%)/2 (2.4%) | 20 (24.4%)/4 (4.9%) | 0.712 | 0.659 | 0.329 |
| Diurnal BH (n/y) | 2 (2.4%)/7 (8.5%) | 15 (18.3%)/8 (9.8%) | 17 (20.7%)/8 (9.8%) | 15 (18.3%)/10 (12.2%) | 0.052 | 0.709 | 0.515 |
| Nocturnal BH (n/y) | 2 (2.4%)/7 (8.5%) | 16 (19.5%)/7 (8.5%) | 19 (23.2%)/6 (7.3%) | 18 (22.0%)/7 (8.5%) | 0.009 | 0.853 | 0.581 |
| Circadian rhythm of blood pressure (normal/altered) | 7 (8.8%)/2 (2.5%) | 13 (16.3%)/9 (11.3%) | 23 (28.7%)/2 (2.5%) | 13 (16.3%)/11 (13.8) | 0.216 | 0.736 | 0.003 |
| Circadian rhythm of heart rate (normal/altered) | 4 (6.3%)/2 (3.1%) | 12 (18.8%)/5 (7.8%) | 12 (18.8%)/6 (9.4%) | 17 (26.6%)/6 (9.4%) | 0.724 | 0.816 | 0.613 |
| EF | 60.0 ± 3.3 ** | 62.0 ± 3.1 ** | 65.0 ± 2.9 ** | 64.0 ± 4.0 ** | 0.027 | 0.495 | 0.551 |
| Carotid plaques (n/y) | 1 (1.2%)/8 (9.4%) | 16 (18.8%)/8 (9.4%) | 14 (16.5%)/11 (12.9%) | 10 (11.8%)/17 (20.0%) | 0.144 | 0.035 | 0.171 |
| IMT | 676 ± 128 ** | 595 ± 114 ** | 555 ± 134 ** | 648 ± 138 ** | 0.689 | 0.075 | 0.008 |
| Hemoglobin | 14.2 ± 1.5 ** | 14.2 ± 2.1 ** | 14.1 ± 1.6 ** | 14.0 ± 1.0 ** | 0.216 | 0.953 | 0.805 |
| White blood cells | 6.4 ± 2.3 ** | 6.0 v 1.6 ** | 6.1 ± 2.2 ** | 6.9 ± 1.8 ** | 0.576 | 0.070 | 0.252 |
| Glycemia | 91.0 ± 23.4 ** | 97.0 ± 13.2 ** | 88.0 ± 11.2 ** | 94.5 ± 16.6 ** | 1.000 | 0.638 | 0.161 |
| eGFR | 80.9 ± 18.4 * | 91.3 ± 15.3 * | 89.3 ± 19.3 * | 83.6 ± 18.6 * | 0.703 | 0.123 | 0.281 |
| Total cholesterol | 192 ± 32.1 * | 193 ± 33.3 * | 195 ± 33.3 * | 201 ± 41.7 * | 0.566 | 0.495 | 0.603 |
| HDL cholesterol | 47.0 ± 21.0 ** | 49.5 ± 12.1 ** | 53.5 ± 13.1 ** | 52.5 ± 20.5 ** | 0.865 | 0.627 | 0.389 |
| LDL cholesterol | 116 ± 22.6 * | 127 ± 31.0 * | 124 ± 37.2 * | 127 ± 44.0 * | 0.510 | 0.993 | 0.815 |
| Triglycerides | 89.5 ± 43.6 ** | 84.0 ± 53.6 ** | 76.0 ± 47.2 ** | 102.0 ± 65.2 ** | 0.834 | 0.856 | 0.510 |
| TLC Groups | N of ASVs | ASVs | Phylum |
|---|---|---|---|
| NMS, OH, US | 1 | Enterobacteriaceae | Pseudomonadota |
| CS, NMS | 1 | Odoribacter | Bacteroidota |
| CS, OH | 2 | Lactobacillus | Bacillota |
| Eubacterium | Bacillota | ||
| CS, US | 2 | Butyricicoccus | Bacillota |
| Barnesiellaceae | Bacteroidota | ||
| NMS, OH | 2 | Clostridium (Lachnospiraceae) | Bacillota |
| Akkermansia | Verrucomicrobiota | ||
| OH | 2 | Streptococcus | Bacillota |
| Maegasphaera | Bacillota | ||
| NMS | 2 | Butyricimonas | Bacteroidota |
| Methanobrevibacter | Euryarchaeota | ||
| CS | 4 | Dorea | Bacillota |
| Oscillospira | Bacillota | ||
| Phascolarbacterium | Bacillota | ||
| S24-7 | Bacteroidota | ||
| US | 17 | Bifidobacterium | Actinomycetota |
| Coriobacteriaceae | Actinomycetota | ||
| Acidaminococcus | Bacillota | ||
| Anaerostipes | Bacillota | ||
| Catenibacterium | Bacillota | ||
| Christensenellaceae | Bacillota | ||
| Clostridiaceae | Bacillota | ||
| Clostridiales | Bacillota | ||
| Clostridium (Clostridiaceae) | Bacillota | ||
| Erysipelotrichaceae | Bacillota | ||
| Faecalibacterium | Bacillota | ||
| Gemmiger | Bacillota | ||
| Roseburia | Bacillota | ||
| SMB53 | Bacillota | ||
| Veillonella | Bacillota | ||
| Parabacteroides | Bacteroidota | ||
| Haemophilus | Pseudomonadota |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longo, S.; Del Chierico, F.; Scanu, M.; Toto, F.; Legramante, J.M.; Rizza, S.; Putignani, L.; Federici, M. An Investigation of Metabolic Risk Factors and Gut Microbiota in Unexplained Syncope. Biomedicines 2024, 12, 264. https://doi.org/10.3390/biomedicines12020264
Longo S, Del Chierico F, Scanu M, Toto F, Legramante JM, Rizza S, Putignani L, Federici M. An Investigation of Metabolic Risk Factors and Gut Microbiota in Unexplained Syncope. Biomedicines. 2024; 12(2):264. https://doi.org/10.3390/biomedicines12020264
Chicago/Turabian StyleLongo, Susanna, Federica Del Chierico, Matteo Scanu, Francesca Toto, Jacopo M. Legramante, Stefano Rizza, Lorenza Putignani, and Massimo Federici. 2024. "An Investigation of Metabolic Risk Factors and Gut Microbiota in Unexplained Syncope" Biomedicines 12, no. 2: 264. https://doi.org/10.3390/biomedicines12020264
APA StyleLongo, S., Del Chierico, F., Scanu, M., Toto, F., Legramante, J. M., Rizza, S., Putignani, L., & Federici, M. (2024). An Investigation of Metabolic Risk Factors and Gut Microbiota in Unexplained Syncope. Biomedicines, 12(2), 264. https://doi.org/10.3390/biomedicines12020264